reconsideration request form - TRICARE Overseas
reconsideration request form - TRICARE Overseas
reconsideration request form - TRICARE Overseas

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
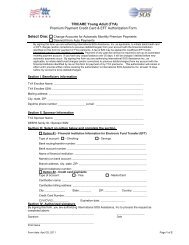
<strong>TRICARE</strong> Young Adult (TYA)Request for <strong>TRICARE</strong> Regional Office Reconsideration of Involuntary Disenrollment,Late Initial Enrollment and Late Changes to CoverageSection I. Sponsor / Beneficiary in<strong>form</strong>ationTYA Sponsor Name: _________________________________________________________DEERS Family ID / SSN: _________________________________________________________Mailing Address: _________________________________________________________City, State, ZIP: _________________________________________________________Daytime Phone Number: __________________ E-mail: _________________________________Date of Request: ___ / ___ / ___TYA Beneficiary Name: _________________________________________________________DEERS Family ID / SSN: _________________________________________________________Section II. Reconsideration Request DetailsRequest Reconsideration of (Check One):Involuntary DisenrollmentLate Initial EnrollmentLate change to coverage due to qualifying life eventSponsor’s Unit: ___________________________________________________________________Unit Address & Phone Number:_____________________________________________________Unit Administrative Officer/Contact & Phone Number: _________________________________Please provide details regarding your <strong>request</strong> for <strong>reconsideration</strong> (attach additional pages as necessary):___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Section III. Sponsor SignatureBy signing this <strong>form</strong>, you are authorizing International SOS Assistance Inc., to process the <strong>request</strong> as completed above.___________________________________________Signature________________________Date________________________________________Print NameSection IV. TRO Use OnlyApprovedNot Approved – Reason:_________________________________Signature of Approving Authority: _____________________________Date: ___________________(cont.)
<strong>TRICARE</strong> Young Adult (TYA)Request for <strong>TRICARE</strong> Regional Office Reconsideration of Involuntary Disenrollment,Late Initial Enrollment and Late Changes to CoverageForm InstructionsUse this <strong>form</strong> if you would like to <strong>request</strong> re-enrollment into the TYA <strong>Overseas</strong> Program following an involuntarydisenrollment, late initial enrollment, or late change to coverage due to qualifying life event (QLE). Forms will be sent tothe <strong>TRICARE</strong> Regional Office for review within 10 days of receipt. Please see instructions below on how to submit <strong>form</strong>.Section I. – Sponsor / Beneficiary In<strong>form</strong>ationComplete TYA Sponsor and Beneficiary personal in<strong>form</strong>ation. Please do not leave anything blank. Please provide aphone number where we can reach you if we need your assistance in processing the in<strong>form</strong>ation you provided on this<strong>form</strong>.Section II. – Reconsideration Request DetailsIndicate the <strong>request</strong> type (involuntary disenrollment, late initial enrollment or late change to coverage due to QLE) andcomplete all sections with required in<strong>form</strong>ation. Please do not leave anything blank.Section III. Authorized signatureHow to Submit Form:Submit a completed copy of page 1 of this <strong>form</strong> via one of the options below:Mail to:International SOS Assistance, Inc.Attention: TOP TRS/TRR/TYA EnrollmentsPO Box 11689Philadelphia, PA 19116Fax to: +1-215-354-5015PRIVACY ACT STATEMENTAUTHORITY: 10 U.S.C. 1079 and 1086, 32 U.S.C. Chapter 17; 32 CFR 199.17; 45 CFR Parts 160 and 164, HealthInsurance Portability and Accountability Act (HIPAA) Privacy and Security Rules; and E.O. 9397 (SSN), as amended.PRINCIPAL PURPOSE(S): To obtain in<strong>form</strong>ation necessary to permit individuals to be re-enrolled into the TYA<strong>Overseas</strong> Program.ROUTINE USE(S): In addition to those disclosures generally permitted under 5 U.S.C. 552a(b) of the Privacy Act of1974, as amended, these records may specifically be disclosed outside the Department of Defense as a routine usepursuant to 5 U.S.C. 552a(b)(3) as follows: to the Departments of Health and Human Services, Homeland Security, andVeterans Affairs, and to other Federal, State, local, or foreign government agencies, and to private business entities,including entities under contract with the Department of Defense and individual providers of care, on matters relating toeligibility, claims pricing and payment, fraud, program abuse, utilization review, quality assurance, peer review, programintegrity, third-party liability, coordination of benefits, and civil or criminal litigation.DISCLOSURE: Voluntary; however, failure to provide in<strong>form</strong>ation may result in the denial of re-enrollment into theTYA <strong>Overseas</strong> Program and cancellation of coverage.