Community-Associated Staphylococcus aureus ... - SWACM
Community-Associated Staphylococcus aureus ... - SWACM
Community-Associated Staphylococcus aureus ... - SWACM

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Evolution, Epidemiology, andEradication of Contemporary<strong>Staphylococcus</strong> <strong>aureus</strong>Stephanie Fritz, MD, MSCIAssistant Professor of PediatricsWashington University School of MedicineSeptember 6, 2012Case: Family D• 2 week old infant with a buttock pustule– Resolved without medical intervention• 1 week later: Mother developed mastitis, breast abscess,and sepsis– Hospitalized for 6 weeks• 15 month old sister hospitalized with skin abscess andfever• Father also developed fever and boils on his arms, backand buttocks• Over the next 2 years, all family members had recurrentepisodes of fever and boils• Caused by “antibiotic-resistant <strong>Staphylococcus</strong> <strong>aureus</strong>”McKenna M, Superbug 2010Outline• Historical perspective of <strong>Staphylococcus</strong> <strong>aureus</strong>• Emergence and epidemiology of communityassociatedmethicillin-resistant S. <strong>aureus</strong>(CA-MRSA)• Treatment of CA-MRSA infections• Prevention of recurrent disease<strong>Staphylococcus</strong> <strong>aureus</strong>• <strong>Staphylococcus</strong> <strong>aureus</strong> is a commensalbacterium that commonly lives on the skin orin the nose of healthy people• S. <strong>aureus</strong> is also a successful pathogen1946:Penicillinintroduced<strong>Staphylococcus</strong> <strong>aureus</strong> Timeline1947:Penicillin-resistantS. <strong>aureus</strong> detected1957: AMAEMERGENCY SESSION:Conference onStaphylococcic Infectionsin the Hospital and<strong>Community</strong>Newborn Nursery Epidemic: 1950s• Infants discharged homefrom the hospital healthy• Returned ~8 days of life withS. <strong>aureus</strong> infection• Mothers presented ~14 daysafter delivery• Phage Type 80/81Mudd S, JAMA 1958; 166:1177-8Heinz Eichenwald, MDHenry Shinefield, MD1
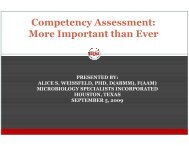
Increase in S. <strong>aureus</strong> InfectionsDiagnosed at St. Louis Children’sHospital: 1999-2007• >1200 childrenpresent with skininfections– 900 require painfuldrainage proceduresClinical Questions• How prevalent is colonization?• What is the significance of colonization?• How can we intervene to reduce infectionsand improve outcomes?• ~50 children aretreated for invasiveS. <strong>aureus</strong> infectionsOrscheln RC et al., Clin Infect Dis 2009; 49:536-542Prevalence and Natural Historyof CA-MRSA Nasal Colonizationin St. Louis ChildrenNasal Colonization StatusParticipants were recruited from 11 pediatric practices fromOctober 2005 to June 20061300 ParticipantsMRSA32 (2.5%)MSSA331 (25.5%)No S. <strong>aureus</strong>937 (72%)Fritz SA et al., Pediatrics 2008; 121:1090-1098Fritz SA et al., Pediatrics 2008; 121:1090-1098Geographic Distribution of ColonizedIndividualsChildren with MRSA Nasal Colonization AreMore Likely To Develop Skin Infections1300 ParticipantsMRSA32 (2.5%)MSSA331 (25.5%)No S. <strong>aureus</strong>937 (72%)Pediatric Population Estimates in St. Louis City and St. Louis County:– MRSA colonization: 8,455– MSSA colonization: 84,5527 Skin or soft tissueinfections(32%)p=0.0322 (69%)responses142 (43%)responses14 Skin or softtissue infections(10%)370 (39%)responses33 Skin or softtissue infections(9%)Fritz SA et al., J Infect 2009; 59: 394-4014
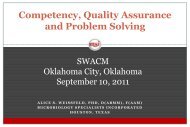
# OF STRAINS TESTEDCEFAZOLIN/OXACILLINCLINDAMYCINERYTHROMYCINLINEZOLIDTETRACYCLINETMP-SMXVANCOMYCINManagement of SSTI in the Era ofCA-MRSA• Cutaneous abscess:– Incision and drainage (I&D) is the primarytreatment– For simple abscesses and boils, I&D aloneis likely to be adequate• Additional data are needed to furtherdefine the role of antibiotics, if any, in thissettingLiu C et al., Clin Infect Dis 2011; 52:285-292TMP-SMXIncision & DrainagePlacebo• No significant difference in cure rates betweenTMP-SMX and placebo• Antibiotic therapy may decrease new lesiondevelopmentDuong M, et al., Ann Emerg Med 2010; 55:401-407Schmitz G et al., Ann Emerg Med 2010; 56:283-287Conditions in which Antibiotics areRecommended after I&D• Severe or extensive disease– Involving multiple sites of infection• Rapid progression in presence of associated cellulitis• Signs and symptoms of systemic illness• <strong>Associated</strong> co-morbidities or immunosuppression– Diabetes mellitus, HIV/AIDS, neoplasm• Extremes of age• Abscess in an area difficult to drain– Face, hand, genitalia• <strong>Associated</strong> septic phlebitis• Lack of response to incision and drainage aloneLiu C et al., Clin Infect Dis 2011; 52:285-292SLCH S. <strong>aureus</strong> AntibiogramOutlineEmergency Dept. AbscessAntibiogram (2009-2010)<strong>Staphylococcus</strong> <strong>aureus</strong> 1712 23 91 15 100 97 99 100MRSA 1314 0 92 9 100 98 100 100MSSA 398 100 89 41 100 94 98 100Cumulative Antibiogram 2010<strong>Staphylococcus</strong> <strong>aureus</strong> 1970 43 78 31 100 97 99 100MRSA 1133 0 79 10 100 97 99 100MSSA 837 100 75 59 100 96 98 100• Historical perspective of <strong>Staphylococcus</strong> <strong>aureus</strong>• Emergence and epidemiology of communityassociatedmethicillin-resistant S. <strong>aureus</strong> (CA-MRSA)• Treatment of CA-MRSA infections• Prevention of recurrent diseaseData indicate percent susceptible for each antimicrobial tested. Data based on first isolate per patient.Courtesy of Carey-Ann Burnham, PhD6
Management of Recurrent SSTI• Emphasize personal hygiene andappropriate wound care– Regular bathing• Shower after exercise and any activity thatinvolves direct skin contact with others– Keep hands clean• Soap and water• Alcohol-based hand sanitizers– Avoid sharing personal hygiene items• Environmental hygiene measures– Cleaning high-touch surfaces that maycontact bare skin or uncovered infectionsLiu C et al., Clin Infect Dis 2011; 52:285-292Decolonization• S. <strong>aureus</strong> colonization is a risk factor for SSTI 1,2• Decolonization– The use of antimicrobial or antiseptic agents to suppressor eliminate S. <strong>aureus</strong> carriage 3– Traditionally used to prevent healthcare-associated MRSA(HA-MRSA) infections– Decolonization is frequently prescribed to patients incommunity settings to prevent recurrent SSTI(1) Fritz SA et al. J Infect 2009; 59:394-401(2) Ellis MW et al. Clin Infect Dis 2004; 39:971-9(3) Liu C et al. Clin Infect Dis 2011; 52:285-292Management of Recurrent SSTI• Decolonization may be considered in selected cases:– A patient develops a recurrent SSTI despite optimizingwound care and hygiene measures– Ongoing transmission is occurring among householdmembers or other close contacts despite optimizing woundcare and hygiene measuresDecolonization Regimens• Mupirocin– Inhibits bacterial isoleucyl-tRNAsynthetase• Protein synthesis inhibition• Chlorhexidine– Biguanide cationic bactericidal agent• Disrupts integrity of cell wall andmembranes• Causes coagulation of intracellular contents• Dilute Bleach (Sodium Hypochlorite)– S. <strong>aureus</strong> antimicrobial activity both invivo and in vitroLiu C et al., Clin Infect Dis 2011; 52:285-292Uncertainty SurroundingDecolonization• Do these measures actually eradicate theorganism?• Does decolonization prevent SSTI?• Who should perform decolonization?StL StaRSSt. Louis<strong>Staphylococcus</strong> <strong>aureus</strong>Reduction StudyRandomized Controlled Trial EvaluatingDecolonization Regimens in Patients with<strong>Community</strong>-<strong>Associated</strong> Skin InfectionsColonized with <strong>Staphylococcus</strong> <strong>aureus</strong>Fritz SA et al., Infect Control Hosp Epidemiol 2011;32:872-8807
Twelve-Month Evaluation of aHousehold vs. Individual Approachto Decolonizing Children with<strong>Community</strong>-<strong>Associated</strong><strong>Staphylococcus</strong> <strong>aureus</strong><strong>Staphylococcus</strong> <strong>aureus</strong>Decolonization Study (SuDS)Study Objectives• To measure S. <strong>aureus</strong> colonization in householdcontacts of children with S. <strong>aureus</strong> skin infections• To identify sites of colonization in index patients• To compare rates of skin infections over 12 monthswhen decolonization measures are performed by theindex patient alone vs. all household membersParticipant Enrollment• Setting:– 9 WU PAARC practices– St. Louis Children’s Hospital• Emergency Department and Wound Center• 183 index patients enrolled– <strong>Community</strong>-onset S. <strong>aureus</strong> skin infection, plus– S. <strong>aureus</strong> colonization in the nose, axilla, and/or inguinal fold• Cultures to evaluate colonization were collected from609 household contacts of index patientsHousehold Contact Colonization128 colonized withMRSA (21%)Colonization SwabsObtained from 609Household Contacts208 colonized withMSSA (34%)Fritz SA, et al. Arch Pediatr Adolesc Med 2012; 166:551-7Baseline Colonization Sites: Index CasesMRSA Colonization SitesMRSA Colonization SitesNose + Axilla +GroinNose OnlyNose + GroinAxilla + GroinNose + AxillaGroin OnlyAxilla OnlyMSSA Colonization SitesNose + GroinAxilla + GroinNose + AxillaNose + Axilla +GroinGroin OnlyAxilla Only• MRSA most frequently colonizes the groin (p=0.03)• MSSA most frequently colonizes the anterior nares (p=0.05)Nose OnlyS. <strong>aureus</strong> Decolonization Protocol• Hygiene curriculum• Mupirocin ointment appliedto the nose twice daily for 5days• Hibiclens® (chlorhexidine)solution used in the showeror bath daily for 5 days++Fritz SA, et al. Arch Pediatr Adolesc Med 2012; 166:551-79
Concordance Among Index CaseInfecting and Colonizing StrainsIndex Cases163Concordance Among Index CaseInfecting and Household ContactColonizing StrainsIndex Cases163Colonizingstrains =Infectingstrains: 109(67%)Colonizingstrains ≠Infectingstrains: 54(33%)HHcolonizingstrain =Infectingstrain: 75(46%)HHcolonizingstrain ≠Infectingstrain: 57(35%)No HHcontactColonization31 (19%)Rodriguez M, et al. 49 th Annual Meeting of the Infectious Diseases Society of America, 2011Rodriguez M, et al. 49 th Annual Meeting of the Infectious Diseases Society of America, 2011Challenges toDecolonizationMupirocin Resistance• Low-level resistance– MIC 8-128 µg/mL– Alteration in the isoleucyl-tRNA synthetase geneileS• High-level mupirocin resistance– MIC ≥256 µg/mL– Conferred by the plasmid-encoded mupA gene• Encodes novel isoleucyl-tRNA synthetase• Plasmids carrying the mupA gene may carry resistancegenes for other systemic antibioticsPatel JB, et al. Clin Infect Dis 2009; 49:935-41Cadilla A, et al. J Clin Microbiol 2011; 49:95-100Clinical and Laboratory Standards InstituteMupirocin Resistance• Widespread use of mupirocin in thecommunity has been associated withincreasing resistance 1• Mupirocin resistance may be related todecolonization failure 2• Up to 12% of S. <strong>aureus</strong> SSTI are caused bymupirocin resistant strains 3(1) Upton A, et al. J Antimicrob Chemother 2003; 51:613-7(2) Lee AS, et al. Clin Infect Dis 2011; 52:1422-30(3) McNeil JC, et al. Antimicrob Agents Chemother 2011; 55:2431-3Mupirocin Resistance and EradicationSuccessBaseline Mup-RPatients with S. <strong>aureus</strong>108923 Mup-R 1066 Mup-SPrescribed Mupirocin408Baseline Mup-SColonized atColonized atOne MonthOne Month4/4 (100%) 144/324 (44%) p=0.041Fritz SA, et al. 49 th Annual Meeting of the Infectious Diseases Society of America, 201111
CA-MRSA Transmission Dynamics• Molecular typing will be performed on all recoveredCA-MRSA isolates– Determine whether infecting strains resemble:• Endogenous colonizing strains• Strains recovered from household contacts• Strains recovered from environmental surfaces– Identify the directionality of transmissionSummary• CA-MRSA is a significant health burden• Colonization is often associated with subsequentinfections• A household decolonization approach reducesthe incidence of SSTI compared to an individualapproach• Decolonization should be applied to specificgroups• Widespread use of decolonization measures maylead to resistance• Fritz Research Team– Patrick Hogan, MPH– Duha Al-Zubeidi, MD– Madeline Martin, RN, BSN– Mary Boyle, RN, MSN– Carol Patrick– Lauren Singh, MPH– Meghan Butler, BS– Ali Ainsworth, BS– Marcela Rodriguez, MDAcknowledgements• Mentorship– Victoria Fraser, MD– Gregory Storch, MD– Alan Schwartz PhD, MD– Jane Garbutt, MB ChB• Collaborators– Carey-Ann Burnham, PhD– David Hunstad, MD– George Weinstock, PhD– Bernard Camins, MD– Robert Kennedy, MD– Sarah Gehlert, PhD– Rachel Orscheln, MD– SLCH Microbiology Laboratory– SLCH PAWS– WU PAARC Clinicians and StaffBaseline Mupirocin Resistance by Participant FactorsParticipant FactorsMupirocin ResistantN=23 (%)Mupirocin SusceptibleN=1066 (%)Female 10/23 (43) 623/1066 (58) 0.20pAfrican-American Race 17/23 (74) 679/1060 (64) 0.60BacterialGeneticFactorsTHEPERFECTSTORMHumanGeneticFactorsInsurance: Government Issued orSelf-Pay15/17 (88) 542/774 (70) 0.18Co-morbid Health Condition 6/9 (67) 254/474 (54) 0.52Skin Disorder 7/15 (47) 273/803 (34) 0.41Antibiotic Use in Past Year 14/15 (93) 452/791 (57) 0.006Emergency Department or UrgentCare Visit in Past Year7/9 (78) 191/474 (40) 0.04Hospitalization in Past Year 6/15 (40) 127/800 (16) 0.02Surgery in the Past Year 1/9 (11) 91/474 (19) 1.00SSTI in Prior Year 9/15 (60) 346/798 (43) 0.29Household Contact SSTI inPrior Year12/15 (80) 336/798 (42) 0.006Healthcare Worker in Household 6/15 (40) 210/802 (26) 0.24Pet in Household 2/15 (13) 349/803 (44) 0.0313
Concordance Among Index CaseInfecting and Colonizing StrainsColonizing strains =Infecting strains: 109(67%)Index cases163Colonizing strains ≠Infecting strains: 54(33%)Intrafamilial Transmission• Definition: an identical strain carried by 2 ormore household members (contacts and/orindex case)• Occurred in 105 of 163 households (64%)HH colonizingstrain =Infectingstrain: 60(55%)HH colonizingstrain ≠Infectingstrain: 29(27%)No HHcontactColonization20 (18%)HH colonizingstrain =Infectingstrain: 15(28%)HH colonizingstrain =Infectingstrain: 28(52%)No HH contactColonization11(20%)Intrafamilial TransmissionNumber of householdmembers, (mean ± SD)Number of people perbedroom, (mean ± SD)MRSA colonization pressure,(mean ± SD)MSSA colonization pressure,(mean ± SD)HouseholdTransmission ofS. <strong>aureus</strong>No HouseholdTransmission ofS. <strong>aureus</strong>P-value5.2 ± 1.9 3.7 ± 1.0
Risk FactorRisk Factors for Nasal MRSAColonizationMRSA vs. Not MRSAOdds Ratio95% CIMedicaid or no insurance 3.3 1.6 - 7.0African-American race 3.5 1.7-7.3Crowded household (>2 people/bedroom) 2.7 1.4-5.3ER or UC visit in past 6 months 2.3 1.3 - 4.0Antibiotic use in past year 2.4 1.3 – 4.7Hospitalization in past year 2.4 1.3 – 4.2Prior systemic infection 5.2 3.0 – 9.0Household member works in healthcare 2.8 1.6 – 5.0CA-MRSA in the Environment• MRSA can survive on some surfaces for hoursto months– Temperature– Humidity– Amount of germs present– Type of surface– Nutrients on surfaces• When surfaces aren’t cleaned and conditions are goodfor bacterial growth, MRSA is more likely to survive forlonger periodsFritz SA et al., Pediatrics 2008; 121:1090-109815