Journal of Dental Hygiene supplement on anti-microbial mouth rinses
Journal of Dental Hygiene supplement on anti-microbial mouth rinses
Journal of Dental Hygiene supplement on anti-microbial mouth rinses

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
2007<str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g><str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>Special Supplementto Access magazine<str<strong>on</strong>g>Journal</str<strong>on</strong>g><str<strong>on</strong>g>of</str<strong>on</strong>g><str<strong>on</strong>g>Dental</str<strong>on</strong>g><str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>T HE A MERICAN D ENTAL H YGIENISTS’ A SSOCIATIONIncorporating Anti<strong>microbial</strong> Mouth<strong>rinses</strong>into Oral <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>: Strategies for ManagingOral Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm and Gingivitis• Changing Perspectives <strong>on</strong> the Use <str<strong>on</strong>g>of</str<strong>on</strong>g>Anti<strong>microbial</strong> Mouth<strong>rinses</strong>• The Role <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Plaque Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmin Oral Health• Safety and Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> Anti<strong>microbial</strong>Mouth<strong>rinses</strong> in Clinical Practice• Strategies for Incorporating Anti<strong>microbial</strong>Mouth<strong>rinses</strong> into Daily Oral Care• Anti<strong>microbial</strong> Mouth<strong>rinses</strong> in C<strong>on</strong>temporary<str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Practice: The Take HomeMessageThis special issue <str<strong>on</strong>g>of</str<strong>on</strong>g> the <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> as a<str<strong>on</strong>g>supplement</str<strong>on</strong>g> to Access was made possible through aneducati<strong>on</strong>al grant from Johns<strong>on</strong> & Johns<strong>on</strong> HealthcareProducts Divisi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> McNEIL-PPC, Inc.
about the authorsGuest Editor■ MICHELE LEONARDI DARBY, RDH, MS, is the graduate program directorin dental hygiene at Old Domini<strong>on</strong> University in Norfolk, Virginia. Shelectures internati<strong>on</strong>ally, is the author <str<strong>on</strong>g>of</str<strong>on</strong>g> over 50 articles, has published 3books, and has served <strong>on</strong> several editorial advisory boards, currentlyserving as associate editor <str<strong>on</strong>g>of</str<strong>on</strong>g> the Internati<strong>on</strong>al <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>and as an editorial review board member <str<strong>on</strong>g>of</str<strong>on</strong>g> the <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>and Dimensi<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>. In 1981, she was a member <str<strong>on</strong>g>of</str<strong>on</strong>g> the firstdelegati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> dental hygienists to visit the People’s Republic <str<strong>on</strong>g>of</str<strong>on</strong>g> China. Shehas received many awards, including the Warner Lambert–American<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’ Associati<strong>on</strong> Award for Excellence in <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> andthe designati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> Eminent Scholar by Old Domini<strong>on</strong> University.Authors■ JOANNA ASADOORIAN, RDH, MSc, is an associate pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essor in theSchool <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> at the University <str<strong>on</strong>g>of</str<strong>on</strong>g> Manitoba and worksprivately as a dental hygienist in period<strong>on</strong>tology. She has published andregularly lectures <strong>on</strong> her research interests, which include qualityassurance, maintaining competence in health care pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als, clinicaldecisi<strong>on</strong> making, and oral health care products for home use. Sheserves <strong>on</strong> the editorial review board for the <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>.■ LOUIS G. DEPAOLA, DDS, MS, is a pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essor in the Department <str<strong>on</strong>g>of</str<strong>on</strong>g>Diagnostic Sciences and Pathology at the University <str<strong>on</strong>g>of</str<strong>on</strong>g> Maryland <str<strong>on</strong>g>Dental</str<strong>on</strong>g>School and the director <str<strong>on</strong>g>of</str<strong>on</strong>g> dental training for the PA/Mid-Atl<strong>anti</strong>c AIDSEducati<strong>on</strong> and Training Center. He is an internati<strong>on</strong>al lecturer; hasauthored and coauthored over 130 journal articles, book chapters, andabstracts; and has been awarded over 75 research and service grants,including <strong>on</strong>es for the study <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>plaque chemotherapeutic agents. Heserves as a c<strong>on</strong>sultant to many pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al organizati<strong>on</strong>s and from2002 to 2005 served <strong>on</strong> the American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> Council <strong>on</strong>Scientific Affairs. He is a diplomate <str<strong>on</strong>g>of</str<strong>on</strong>g> the American Board <str<strong>on</strong>g>of</str<strong>on</strong>g> OralMedicine and the American College <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentists.■ JOANN R. GURENLIAN, RDH, PhD, is a former chair <str<strong>on</strong>g>of</str<strong>on</strong>g> the Department<str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> at Thomas Jeffers<strong>on</strong> University in Philadelphia andpast president <str<strong>on</strong>g>of</str<strong>on</strong>g> the American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’ Associati<strong>on</strong>. Shec<strong>on</strong>tinues to c<strong>on</strong>sult and to <str<strong>on</strong>g>of</str<strong>on</strong>g>fer c<strong>on</strong>tinuing educati<strong>on</strong> services in thehealth care field. She has authored over 100 articles, is the coauthor <str<strong>on</strong>g>of</str<strong>on</strong>g>The Medical History: Clinical Implicati<strong>on</strong>s and Emergency Preventi<strong>on</strong> in<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Settings, and is the recipient <str<strong>on</strong>g>of</str<strong>on</strong>g> numerous awards, including theAmerican <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’ Associati<strong>on</strong> Distinguished Service Award.She is the vice president <str<strong>on</strong>g>of</str<strong>on</strong>g> the Internati<strong>on</strong>al Federati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g>Hygienists and chairs a work group for the Nati<strong>on</strong>al Diabetes Educati<strong>on</strong>Program.This special issue <str<strong>on</strong>g>of</str<strong>on</strong>g> the <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g><str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> was funded by an unrestrictededucati<strong>on</strong>al grant from Johns<strong>on</strong> & Johns<strong>on</strong>Healthcare Products Divisi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> McNEIL-PPC, Inc.C<strong>on</strong>tinuing Educati<strong>on</strong> ProgramTo obtain 2 hours <str<strong>on</strong>g>of</str<strong>on</strong>g> c<strong>on</strong>tinuing educati<strong>on</strong>credit, <strong>on</strong>ce you have thoroughly reviewed this<str<strong>on</strong>g>supplement</str<strong>on</strong>g>, please complete the exam athttp://www.adha.org/CE_courses/course16/.Open to all licensed U.S. dental hygienists,ADHA’s CE Program <str<strong>on</strong>g>of</str<strong>on</strong>g>fers <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g><str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> readers the opportunity toearn CE credit. Your exam will be graded bythe ADHA staff using questi<strong>on</strong>s reviewedand developed in cooperati<strong>on</strong> with theUniversity <str<strong>on</strong>g>of</str<strong>on</strong>g> North Carolina School <str<strong>on</strong>g>of</str<strong>on</strong>g>Dentistry, a recognized provider <str<strong>on</strong>g>of</str<strong>on</strong>g> CEcredit.Credit for this CE program expires <strong>on</strong>e yearfrom the date <str<strong>on</strong>g>of</str<strong>on</strong>g> publicati<strong>on</strong> (both print and<strong>on</strong>line). Duplicate submissi<strong>on</strong>s will bedisregarded. Submit your exam <strong>on</strong>ly <strong>on</strong>ce.C<strong>on</strong>tinuing educati<strong>on</strong> credits issued forparticipati<strong>on</strong> in this CE activity may notapply toward license renewal in all licensingjurisdicti<strong>on</strong>s. It is the resp<strong>on</strong>sibility <str<strong>on</strong>g>of</str<strong>on</strong>g> eachparticipant to verify the licensingrequirements <str<strong>on</strong>g>of</str<strong>on</strong>g> his or her licensing orregulatory agency.Any questi<strong>on</strong>s? C<strong>on</strong>tact ADHACommunicati<strong>on</strong>s Divisi<strong>on</strong>: 312/440-8900.■ ANN ESHENAUR SPOLARICH, RDH, PhD, holds several academicappointments and currently teaches at the Ariz<strong>on</strong>a School <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistryand Oral Health, University <str<strong>on</strong>g>of</str<strong>on</strong>g> Southern California School <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry,and University <str<strong>on</strong>g>of</str<strong>on</strong>g> Maryland <str<strong>on</strong>g>Dental</str<strong>on</strong>g> School in additi<strong>on</strong> to practicing dentalhygiene. An internati<strong>on</strong>al lecturer, she has published over 60 articles and6 chapters in dental hygiene textbooks, has been active in research,serves <strong>on</strong> several editorial review boards, and is a c<strong>on</strong>sultant to theNati<strong>on</strong>al Center for <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Research. She is the current chair <str<strong>on</strong>g>of</str<strong>on</strong>g>the American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’ Associati<strong>on</strong> Council <strong>on</strong> Research. Shehas received several awards, most recently, the University <str<strong>on</strong>g>of</str<strong>on</strong>g>Pennsylvania <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Alumni Achievement Award in 2002.
Inside<str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>Message3 Changing Perspectives <strong>on</strong> the Use <str<strong>on</strong>g>of</str<strong>on</strong>g> Anti<strong>microbial</strong> Mouth<strong>rinses</strong>Michele Le<strong>on</strong>ardi Darby, RDH, MSSupplementIncorporating Anti<strong>microbial</strong> Mouth<strong>rinses</strong> intoOral <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>: Strategies for ManagingOral Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm and Gingivitis4 The Role <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Plaque Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm in Oral HealthJoAnn R. Gurenlian, RDH, PhD13 Safety and Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> Anti<strong>microbial</strong> Mouth<strong>rinses</strong>in Clinical PracticeLouis G. DePaola, DDS, MSAnn Eshenaur Spolarich, RDH, PhD26 Strategies for Incorporating Anti<strong>microbial</strong> Mouth<strong>rinses</strong>into Daily Oral CareJoanna Asadoorian, RDH, MSc32 Anti<strong>microbial</strong> Mouth<strong>rinses</strong> in C<strong>on</strong>temporary<str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Practice: The Take Home MessageMichele Le<strong>on</strong>ardi Darby, RDH, MSSpecial <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 1
<str<strong>on</strong>g>Journal</str<strong>on</strong>g><str<strong>on</strong>g>of</str<strong>on</strong>g><str<strong>on</strong>g>Dental</str<strong>on</strong>g><str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>EXECUTIVE DIRECTORAnn Battrell, RDH, BS, MSDHannb@adha.netDIRECTOR OF COMMUNICATIONSJeff Mitchelljeffm@adha.netEDITOR EMERITUSMary Alice Gast<strong>on</strong>, RDH, MSEDITOR-IN-CHIEFRebecca S. Wilder, RDH, BS, MSrebeccaw@adha.netSTAFF EDITORKatie Bargekatieb@adha.netLAYOUT/DESIGNJean MajeskiPaul R. Palmer■ STATEMENT OF PURPOSEThe <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> is the refereed, scientific publicati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> theAmerican <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’ Associati<strong>on</strong>. It promotes the publicati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>original research related to the pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>, the educati<strong>on</strong>, and the practice <str<strong>on</strong>g>of</str<strong>on</strong>g>dental hygiene. The journal supports the development and disseminati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> adental hygiene body <str<strong>on</strong>g>of</str<strong>on</strong>g> knowledge through scientific inquiry in basic, applied,and clinical research.■ EDITORIAL REVIEW BOARDCeleste M. Abraham, DDS, MSCynthia C. Amyot, BSDH, EdDJoanna Asadoorian, RDH, MScCaren M. Barnes, RDH, BS, MSPhyllis L. Beemsterboer, RDH, MS, EdDStephanie Bossenberger, RDH, MSKimberly S. Bray, RDH, MSLorraine Brockmann, RDH, MSPatricia Regener Campbell, RDH, MSDan Caplan, DDS, PhDBarbara H. C<strong>on</strong>nolly, PT, EdD, FAPTAValerie J. Cooke, RDH, MS, EdDMaryAnn Cugini, RDH, MHPSusan J. Daniel, AAS, BS, MSMichele Le<strong>on</strong>ardi Darby, RDH, MSCatherine Davis, RDH, PhD. FIDSAC<strong>on</strong>nie Drisko, RDH, BS, DDSJacquelyn M. Dylla, DPT, PTDeborah E. Fleming, RDH, MSJane L. Forrest, BSDH, MS, EdDJacquelyn L. Fried, RDH, BA, MSMary George, RDH, BSDH, MEdEllen Grimes, RDH, MA, MPA, EdDJoAnn R. Gurenlian, RDH, PhDLinda L. Hanl<strong>on</strong>, RDH, BS, MEd, PhDKitty Harkleroad, RDH, MSHarold A. Hens<strong>on</strong>, RDH, MEdLaura Jansen Howert<strong>on</strong>, RDH, MSLisa F. Harper Mall<strong>on</strong>ee,BSDH,MPH,RD/LD■ SUBSCRIPTIONSHeather L. Jared, RDH, BS, MSWendy Kerschbaum, RDH, MA, MPHSalme Lavigne, RDH, BA, MSDHJessica Y. Lee, DDS, MPH, PhDDeborah S. Manne,RDH,RN,MSN,OCNAnn L. McCann, RDH, BS, MSStacy McCauley, RDH, MSGayle McCombs, RDH, MSShann<strong>on</strong> Mitchell, RDH, MSTricia Moore, RDH, BSDH, MA, EdDChristine Nathe, RDH, MSKathleen J. Newell, RDH, MA, PhDJohanna Odrich, RDH, MS, DrPhPamela Overman, BSDH, MS, EdDVickie Overman, RDH, BS, MEdFotinos S. Panagakos, DMD, PhD, MEdM. Elaine Parker, RDH, MS, PhDCeib Phillips, MPH, PhDMarjorie Reveal, RDH, MS, MBAKip Rowland, RDH, MSJudith Skelet<strong>on</strong>, RDH, BS, MEd, PhDAnn Eshenaur Spolarich, RDH, PhDSheryl L. Ernest Syme, RDH, MSTerri Tilliss, RDH, BS, MS, MA, PhDNita Wallace, RDH, PhDKaren B. Williams, RDH, PhDCharlotte J. Wyche, RDH, MSPamela Zarkowski, BSDH, MPH, JDThe <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> is published quarterly, <strong>on</strong>line-<strong>on</strong>ly, by the American<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’ Associati<strong>on</strong>, 444 N. Michigan Avenue, Chicago, IL 60611. Copyright2007 by the American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’ Associati<strong>on</strong>. Reproducti<strong>on</strong> in whole orpart without written permissi<strong>on</strong> is prohibited. Subscripti<strong>on</strong> rates for n<strong>on</strong>members are<strong>on</strong>e year, $45; two years, $65; three years, $90; prepaid.■ SUBMISSIONSPlease submit manuscripts for possible publicati<strong>on</strong> in the <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g>to Katie Barge at katieb@adha.net.2 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Introducti<strong>on</strong>Changing Perspectives <strong>on</strong> the Use <str<strong>on</strong>g>of</str<strong>on</strong>g>Anti<strong>microbial</strong> Mouth<strong>rinses</strong>Michele Le<strong>on</strong>ardi Darby, RDH, MSAs oral health care pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als,we need to makeevidence-based recommendati<strong>on</strong>sto our patients.Studies from which we derive our recommendati<strong>on</strong>sneed to have beenc<strong>on</strong>ducted with scientific rigor andneed to be c<strong>on</strong>firmed with other welldesignedstudies. Given the numerous,l<strong>on</strong>g-term, peer-reviewed publishedstudies <strong>on</strong> <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> with c<strong>on</strong>sistent statisticallyand clinically significant outcomes,it is time to change our pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>althinking and practices.When c<strong>on</strong>sidering the oral envir<strong>on</strong>ment,about 20% is occupied bytooth surfaces, that is, those areas targetedfor toothbrushing and flossing. 1<str<strong>on</strong>g>Dental</str<strong>on</strong>g> plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm is not limited totooth surfaces. About 80% <str<strong>on</strong>g>of</str<strong>on</strong>g> theremaining surfaces include the oralmucosa and specialized mucosa <str<strong>on</strong>g>of</str<strong>on</strong>g> thet<strong>on</strong>gue. 1 Saliva, the t<strong>on</strong>gue, and oralmucosa serve as reservoirs <str<strong>on</strong>g>of</str<strong>on</strong>g> pathogenicbacteria able to relocate and col<strong>on</strong>ize<strong>on</strong> the teeth and in sulci. Usingan <strong>anti</strong>septic <strong>mouth</strong>rinse produces an<strong>anti</strong><strong>microbial</strong> effect throughout theentire <strong>mouth</strong>, including areas easilymissed during toothbrushing andinterdental cleaning. Therefore, it isnot surprising that in May 2007, theAmerican <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> Council<strong>on</strong> Scientific Affairs issued newadvice highlighting the oral healthbenefits <str<strong>on</strong>g>of</str<strong>on</strong>g> ADA-Accepted <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> that help preventand reduce plaque and gingivitis. 2This special Supplement to the<str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> focuses <strong>on</strong>our changing beliefs about <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> and their value inmaintaining oral health. The paperswithin c<strong>on</strong>tain extensive informati<strong>on</strong>about dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms, the effectiveness<str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong>,and how to incorporate these agentsinto patients’oral self-care. Within thisSupplement, dental hygienists will findbest practices regarding <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> so they can c<strong>on</strong>fidentlyrecommend their use to patients based<strong>on</strong> the evidence. Patients look to dentalhygienists for trustworthy informati<strong>on</strong>that can make a difference in theiroral and systemic health. In this Supplement,dental hygienists have evidence-basedinformati<strong>on</strong> about <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> from oral healthexperts.Dr. Gurenlian provides a primer <strong>on</strong>dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm and the perpetualchallenges facing its management.Drs. DePaola and Spolarich reviewthe safety and efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> the major<strong>mouth</strong><strong>rinses</strong> <strong>on</strong> the market and provideclear guidance <strong>on</strong> which productscan be c<strong>on</strong>fidently recommendedto yield predictable clinical healthoutcomes. New bodies <str<strong>on</strong>g>of</str<strong>on</strong>g> researchevidence encourage the replacement<str<strong>on</strong>g>of</str<strong>on</strong>g> old beliefs and practices with moreeffective therapies; but embracingchange is arduous, even with str<strong>on</strong>gevidence to support the change.Joanna Asadoorian tackles the challenge<str<strong>on</strong>g>of</str<strong>on</strong>g> promptly translating evidence-basedinformati<strong>on</strong> into practice,particularly when it meanschange <strong>on</strong> the part <str<strong>on</strong>g>of</str<strong>on</strong>g> both the practiti<strong>on</strong>erand the patient. From her paper,dental hygienists will better understandresistance to change, the process<str<strong>on</strong>g>of</str<strong>on</strong>g> change, and how to use change theoryto help themselves and patientsincorporate health-promoting behaviorssuch as twice-daily use <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse. Asadoorian’sapproach is also useful in motivatingpatients to adopt other beneficial oralhygiene measures.Clinically relevant and easilyapplied informati<strong>on</strong> can be foundwithin these pages. Through this newknowledge, dental hygienists will beequipped to better c<strong>on</strong>trol plaque andgingivitis in patients who historicallymay have been excluded from <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse recommendati<strong>on</strong>s.I encourage you to read this issuefrom cover to cover because theknowledge within will make a differencein the way you practice dentalhygiene. Share the issue with yourcolleagues, and keep an issue in yourrecepti<strong>on</strong> area for patients to read.Patients will know that you are a valuablesource for oral health care recommendati<strong>on</strong>sthat improve and promotetheir health status.References1. Mager DL, Ximenez-Fyvie LA, HaffajeeAD, Socransky SS. Distributi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>selected bacterial species <strong>on</strong> intraoralsurfaces. J Clin Period<strong>on</strong>tol. 2003;30:644-654.2. ADA affirms benefits <str<strong>on</strong>g>of</str<strong>on</strong>g> ADA-Accepted<strong>anti</strong><strong>microbial</strong> <strong>mouth</strong> <strong>rinses</strong> and toothpastes,fluoride <strong>mouth</strong> <strong>rinses</strong> [newsrelease].Chicago, IL: American <str<strong>on</strong>g>Dental</str<strong>on</strong>g>Associati<strong>on</strong>; May 23, 2007. http://ada.org/public/media/releases/0705_release03.asp. Accessed July 27,2007.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 3
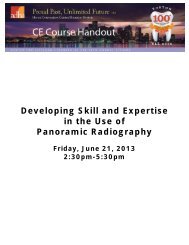
SupplementThe Role <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Plaque Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm in Oral HealthJoAnn R. Gurenlian, RDH, PhDIntroducti<strong>on</strong>In c<strong>on</strong>trast to an accumulati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>individual bacteria, a bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm is acomplex, communal, 3-dimensi<strong>on</strong>alarrangement <str<strong>on</strong>g>of</str<strong>on</strong>g> bacteria. Bacterialbi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms are ubiquitous and are potentiallyfound in a variety <str<strong>on</strong>g>of</str<strong>on</strong>g> sites withinthe human body. For example, theycan grow <strong>on</strong> indwelling catheters,ports, and implants; external surfaces<str<strong>on</strong>g>of</str<strong>on</strong>g> the eye; artificial heart valves;endotracheal tubes; and c<strong>on</strong>taminatedprosthetic joints. A bacterial bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm is<str<strong>on</strong>g>of</str<strong>on</strong>g>ten the cause <str<strong>on</strong>g>of</str<strong>on</strong>g> persistent infecti<strong>on</strong>sand has been associated withosteomyelitis, pneum<strong>on</strong>ia in patientswith cystic fibrosis, and prostatitis. 1In areas related to oral health care,bacterial bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms are found in dentalunit water lines, <strong>on</strong> tooth surfaces anddental prosthetic appliances, and <strong>on</strong>oral mucous membranes. Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm inthe form <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingival and subgingivalplaque is the etiologic agentin dental caries and period<strong>on</strong>tal diseases(Figure 1). 2-5 The pathogenicity<str<strong>on</strong>g>of</str<strong>on</strong>g> the dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm isenhanced by the fact that in bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmform, the comp<strong>on</strong>ent bacteria haveincreased resistance to <strong>anti</strong>biotics andother chemotherapeutic agents andare less able to be phagocytized byhost inflammatory cells. Therefore,c<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g> the dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm isa major objective <str<strong>on</strong>g>of</str<strong>on</strong>g> dental pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>alsand critical to the maintenance<str<strong>on</strong>g>of</str<strong>on</strong>g> optimal oral health. This articlereviews the characteristics <str<strong>on</strong>g>of</str<strong>on</strong>g> dentalbi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm, its role in the etiology <str<strong>on</strong>g>of</str<strong>on</strong>g>period<strong>on</strong>tal diseases, and strategiesfor c<strong>on</strong>trolling the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm to promotehealth.AbstractOverview. Microbial bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms are complex communities <str<strong>on</strong>g>of</str<strong>on</strong>g> bacteria andare comm<strong>on</strong> in the human body and in the envir<strong>on</strong>ment. In recent years,dental plaque has been identified as a bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm, and the structure, microbiology,and pathophysiology <str<strong>on</strong>g>of</str<strong>on</strong>g> dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms have been described. Thenature <str<strong>on</strong>g>of</str<strong>on</strong>g> the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm enhances the comp<strong>on</strong>ent bacteria’s resistance toboth the host’s defense system and <strong>anti</strong><strong>microbial</strong>s. If not removed regularly,the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm undergoes maturati<strong>on</strong>, and the resulting pathogenic bacterialcomplex can lead to dental caries, gingivitis, and period<strong>on</strong>titis. In additi<strong>on</strong>,dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm, especially subgingival plaque in patients with period<strong>on</strong>titis,has been associated with various systemic diseases and disorders, includingcardiovascular disease, diabetes mellitus, respiratory disease, andadverse pregnancy outcomes.Clinical Implicati<strong>on</strong>s. An understanding <str<strong>on</strong>g>of</str<strong>on</strong>g> the nature and pathophysiology<str<strong>on</strong>g>of</str<strong>on</strong>g> the dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm is important to implementing proper managementstrategies. Although dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm cannot be eliminated, it can be reducedand c<strong>on</strong>trolled through daily oral care. A daily regimen <str<strong>on</strong>g>of</str<strong>on</strong>g> thorough mechanicaloral hygiene procedures, including toothbrushing and interdental cleaning,is key to c<strong>on</strong>trolling bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm accumulati<strong>on</strong>. Because teeth comprise<strong>on</strong>ly 20% <str<strong>on</strong>g>of</str<strong>on</strong>g> the <strong>mouth</strong>’s surfaces, for optimal oral health, the use <str<strong>on</strong>g>of</str<strong>on</strong>g> an<strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse helps to c<strong>on</strong>trol bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm not reached by brushingand flossing as well as bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm bacteria c<strong>on</strong>tained in oral mucosal reservoirs.Key words: Anti<strong>microbial</strong> <strong>mouth</strong>rinse, bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm, dental plaque, oral health,period<strong>on</strong>tal diseaseChanging Views <str<strong>on</strong>g>of</str<strong>on</strong>g><str<strong>on</strong>g>Dental</str<strong>on</strong>g> PlaqueOver the past 50 years, the understandingand characterizati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> dentalplaque have underg<strong>on</strong>e significant evoluti<strong>on</strong>.Loesche 6 proposed both a n<strong>on</strong>specificand a specific plaque hypothesisfor period<strong>on</strong>tal disease initiati<strong>on</strong>and progressi<strong>on</strong>.The n<strong>on</strong>specific plaque hypothesisproposed that the entire <strong>microbial</strong> community<str<strong>on</strong>g>of</str<strong>on</strong>g> plaque that accumulated <strong>on</strong>tooth surfaces and in the gingivalcrevice c<strong>on</strong>tributed to the development<str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal disease. Plaque bacteriaproduced virulence factors and noxiousproducts that initiated inflammati<strong>on</strong>,challenged the host defense system, andresulted in the destructi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>taltissues. Under this hypothesis, thequ<strong>anti</strong>ty <str<strong>on</strong>g>of</str<strong>on</strong>g> plaque was c<strong>on</strong>sidered tobe the critical factor in the development<str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal disease. Thus, increasesin the amount <str<strong>on</strong>g>of</str<strong>on</strong>g> plaque (qu<strong>anti</strong>ty), asopposed to specific pathogenicmicroorganisms (quality) found in theplaque, were viewed as being primarilyresp<strong>on</strong>sible for inducing diseaseand disease progressi<strong>on</strong>. 7,8Studies <strong>on</strong> the <strong>microbial</strong> etiology<str<strong>on</strong>g>of</str<strong>on</strong>g> various forms <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>titis sup-4 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Figure 1. Scanning electr<strong>on</strong> micrograph <str<strong>on</strong>g>of</str<strong>on</strong>g> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm grown from thesubgingival plaque <str<strong>on</strong>g>of</str<strong>on</strong>g> a healthy subject for 10 days anaerobically <strong>on</strong>saliva-coated hydroxyapatite discs. (Grown by Michael Sedlacek, PhD,and Clay Walker, PhD, at the University <str<strong>on</strong>g>of</str<strong>on</strong>g> Florida College <str<strong>on</strong>g>of</str<strong>on</strong>g> DentistryPeriod<strong>on</strong>tal Disease Research Center. Image taken by the University<str<strong>on</strong>g>of</str<strong>on</strong>g> Florida Electr<strong>on</strong> Microscopy Core Facility.)A naeslundii 2(A viscosus)S mitisS oralisS sanguisStreptococcus sp.S gord<strong>on</strong>iiS intermediusE corrodensC gingivalisC sputigenaC ochraceaC c<strong>on</strong>cisusA actino. aV parvulaA od<strong>on</strong>tolyticusS c<strong>on</strong>stellatusA actino b.C gracilisP intermediaP nigrescensP microsF nuc vincentiiF nuc nucleatumF nuc polymorphumF period<strong>on</strong>ticumC showaeC rectusE nodatumS noxiaP gingivalisT forsythensisT denticolaport the specific plaque hypothesis,which proposes that <strong>on</strong>ly certainmicroorganisms within the plaquecomplex are pathogenic. Despite thepresence <str<strong>on</strong>g>of</str<strong>on</strong>g> hundreds <str<strong>on</strong>g>of</str<strong>on</strong>g> species <str<strong>on</strong>g>of</str<strong>on</strong>g>microorganisms in period<strong>on</strong>tal pockets,fewer than 20 are routinely foundin increased proporti<strong>on</strong>s at period<strong>on</strong>tallydiseased sites. These specific virulentbacterial species activate thehost’s immune and inflammatoryresp<strong>on</strong>ses that then cause b<strong>on</strong>e and s<str<strong>on</strong>g>of</str<strong>on</strong>g>ttissue destructi<strong>on</strong>. 6,8,9Socransky and colleagues 4,10 recognizedthat early plaque c<strong>on</strong>sists predominantly<str<strong>on</strong>g>of</str<strong>on</strong>g> gram-positive organismsand that if the plaque is leftundisturbed it undergoes a process <str<strong>on</strong>g>of</str<strong>on</strong>g>maturati<strong>on</strong> resulting in a more complexand predominantly gram-negativeflora. These investigatorsassigned the organisms <str<strong>on</strong>g>of</str<strong>on</strong>g> the subgingivalmicrobiota into groups, or complexes,based <strong>on</strong> their associati<strong>on</strong> withhealth and various disease severities(Figure 2). 4,10 Color designati<strong>on</strong>s wereused to denote the associati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> particularbacterial complexes with period<strong>on</strong>talinfecti<strong>on</strong>s. The blue,yellow, green, and purplecomplexes designate earlycol<strong>on</strong>izers <str<strong>on</strong>g>of</str<strong>on</strong>g> the subgingivalflora. Orange and red complexesreflect late col<strong>on</strong>izersassociated with mature subgingivalplaque. Certain bacterialcomplexes are associatedwith health or disease. 10,11For example, the bacteria inthe red complex are morelikely to be associated withclinical indicators <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>taldisease such as period<strong>on</strong>talpocketing and clinicalattachment loss.PlaqueRecognized as aBi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmFigure 2. Microbial complexes in subgingival bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. 4,10 (Modified fromSocransky SS, Haffajee AD, Cugini MA, et al. Microbial complexes insubgingival plaque. J Clin Period<strong>on</strong>tol 1998;25:134-144. Reprinted withpermissi<strong>on</strong> from Blackwell Publishing.)Research over the pastdecade has led to the recogniti<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> dental plaque as abi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm—a highly organizedSpecial <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 5
accumulati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong> communitiesattached to an envir<strong>on</strong>mental surface.Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms are organized to maximizeenergy, spatial arrangements,communicati<strong>on</strong>, and c<strong>on</strong>tinuity <str<strong>on</strong>g>of</str<strong>on</strong>g> thecommunity <str<strong>on</strong>g>of</str<strong>on</strong>g> microorganisms.Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms protect bacteria livingwithin their structures and therebyprovide an advantage over free-floating(plankt<strong>on</strong>ic) bacteria. The slimyextracellular matrix produced bybi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm bacteria encloses the <strong>microbial</strong>community and protects it fromthe surrounding envir<strong>on</strong>ment, includingattacks from chemotherapeuticagents. Chemotherapeutic agents havedifficulty penetrating the polysaccharidematrix to reach and affect themicroorganisms. 1,11-13 Thus, the matrixhelps to protect bacteria deep withinthe bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm from <strong>anti</strong>biotics and <strong>anti</strong>septics,increasing the likelihood <str<strong>on</strong>g>of</str<strong>on</strong>g>the col<strong>on</strong>ies’ survival. Furthermore,the extracellular matrix keeps the bacteriabanded together, so they are notflushed away by the acti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> salivaand gingival crevicular fluid. Mechanicalmethods, including toothbrushing,interdental cleaning, andpr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al scaling procedures, arerequired to regularly and effectivelydisrupt and remove the plaquebi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. Antiseptics, such as<strong>mouth</strong><strong>rinses</strong>, can help to c<strong>on</strong>trol thebi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm but must be formulated so asto be able to penetrate the plaquematrix and gain access to the pathogenicbacteria.Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms have a definite architecturalstructure. The bacteria are notuniformly distributed throughout thebi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm; rather, there are aggregates<str<strong>on</strong>g>of</str<strong>on</strong>g> microcol<strong>on</strong>ies that vary in shapeand size. Channels between thecol<strong>on</strong>ies allow for circulati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> nutrientsand by-products and provide asystem to eliminate wastes. 14,15Microorganisms <strong>on</strong> the outer surface<str<strong>on</strong>g>of</str<strong>on</strong>g> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms are not as str<strong>on</strong>glyattached within the matrix and tendto grow faster than those bacteriadeeper within the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. Surfacemicroorganisms are more susceptibleto detachment, a characteristic thatfacilitates travel to form new bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmcol<strong>on</strong>ies <strong>on</strong> nearby oral structures andtissues.Bacteria in bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm communicatewith each other by a process calledquorum sensing. This dynamic,sophisticated communicati<strong>on</strong> systemenables bacteria to m<strong>on</strong>itor eachother’s presence and to modulate theirgene expressi<strong>on</strong> in resp<strong>on</strong>se to thenumber <str<strong>on</strong>g>of</str<strong>on</strong>g> bacteria in a given area <str<strong>on</strong>g>of</str<strong>on</strong>g>the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. 8 In additi<strong>on</strong>, as a result<str<strong>on</strong>g>of</str<strong>on</strong>g> quorum sensing, porti<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> thebi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm can become detached in orderto maintain a cell density compatiblewith c<strong>on</strong>tinued survival.Stages <str<strong>on</strong>g>of</str<strong>on</strong>g> Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmFormati<strong>on</strong>The growth and development <str<strong>on</strong>g>of</str<strong>on</strong>g>bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm are characterized by 4 stages:initial adherence, lag phase, rapidgrowth, and steady state. Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm formati<strong>on</strong>begins with the adherence <str<strong>on</strong>g>of</str<strong>on</strong>g>bacteria to a tooth surface, followedby a lag phase in which changes ingenetic expressi<strong>on</strong> (phenotypic shifts)occur. A period <str<strong>on</strong>g>of</str<strong>on</strong>g> rapid growth thenoccurs, and an exopolysaccharidematrix is produced. During the steadystate, the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm reaches growth equilibrium.Surface detachment andsloughing occur, and new bacteria areacquired.Initial Adherence and Lag PhaseThe first phase <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingivalbi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm formati<strong>on</strong> is the depositi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>salivary comp<strong>on</strong>ents, known asacquired pellicle, <strong>on</strong> tooth surfaces.This pellicle makes the surface receptiveto col<strong>on</strong>izati<strong>on</strong> by specific bacteria.Salivary glands produce a variety<str<strong>on</strong>g>of</str<strong>on</strong>g> proteins and peptides that furtherc<strong>on</strong>tribute to bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm formati<strong>on</strong>. ForBacteria in bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm communicate with each other bya process called quorum sensing. This dynamic,sophisticated communicati<strong>on</strong> system enablesbacteria to m<strong>on</strong>itor each other’s presence and tomodulate their gene expressi<strong>on</strong> in resp<strong>on</strong>se to thenumber <str<strong>on</strong>g>of</str<strong>on</strong>g> bacteria in a given area <str<strong>on</strong>g>of</str<strong>on</strong>g> the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm.example, salivary mucins, such asMUC 5 B and MUC 7 , c<strong>on</strong>tribute to theformati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> acquired pellicle, 16,17 andstatherin, a salivary acidic phosphoprotein,and proline-rich proteins promotebacterial adhesi<strong>on</strong> to tooth surfaces.18 Acquired pellicle formati<strong>on</strong>begins within minutes <str<strong>on</strong>g>of</str<strong>on</strong>g> a pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>alprophylaxis; within 1 hour,microorganisms attach to the pellicle.Usually, gram-positive cocci are thefirst microorganisms to col<strong>on</strong>ize theteeth. As bacteria shift from plankt<strong>on</strong>icto sessile life, a phenotypicchange in the bacteria occurs requiringsignificant genetic up-regulati<strong>on</strong>(gene signaling that promotes thisshift). As genetic expressi<strong>on</strong> shifts,there is a lag in bacterial growth.Rapid GrowthDuring the rapid growth stage,adherent bacteria secrete large amounts<str<strong>on</strong>g>of</str<strong>on</strong>g> water-insoluble extracellular polysaccharidesto form the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm matrix.The growth <str<strong>on</strong>g>of</str<strong>on</strong>g> microcol<strong>on</strong>ies withinthe matrix occurs. With time, additi<strong>on</strong>alvarieties <str<strong>on</strong>g>of</str<strong>on</strong>g> bacteria adhere tothe early col<strong>on</strong>izers—a process knownas coaggregati<strong>on</strong>—and the bacterialcomplexity <str<strong>on</strong>g>of</str<strong>on</strong>g> the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm increases.These processes involve unique, selectivemolecular interacti<strong>on</strong>s leading tostructural stratificati<strong>on</strong> within thebi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. Coaggregati<strong>on</strong> and subsequentcell divisi<strong>on</strong> also increase the thickness<str<strong>on</strong>g>of</str<strong>on</strong>g> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. 19-21Steady State/DetachmentDuring the steady state phase, bacteriain the interior <str<strong>on</strong>g>of</str<strong>on</strong>g> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms slowtheir growth or become static. Bacte-6 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
ia deep within the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm show signs<str<strong>on</strong>g>of</str<strong>on</strong>g> death with disrupted bacterial cellsand other cells devoid <str<strong>on</strong>g>of</str<strong>on</strong>g> cytoplasm;bacteria near the surface remain intact.During this phase, crystals can beobserved in the interbacterial matrixthat may represent initial calculusmineralizati<strong>on</strong>. 22 As noted above, duringthe steady state stage, surfacedetachment and sloughing also occur,with some bacteria traveling to formnew bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm col<strong>on</strong>ies.Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm and OralDiseaseFigure 3. Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm lodges in the crevices around the teeth both aboveand below the gingival margin. Accumulati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmcan result in dental caries and period<strong>on</strong>tal disease. (Figure copyright2006 Keith Kasnot, MA, CMI, FAMI.)Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms can cover surfacesthroughout the oral cavity. Microcol<strong>on</strong>iesexist <strong>on</strong> oral mucosa, thet<strong>on</strong>gue, biomaterials used for restorati<strong>on</strong>sand dental appliances, and toothsurfaces above and below the gingivalmargin (Figure 3). It is importantfor oral health pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als to communicateto their patients that bothdental caries and period<strong>on</strong>tal diseaseare infectious diseases resulting fromdental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm accumulati<strong>on</strong>.Each <str<strong>on</strong>g>of</str<strong>on</strong>g> these diseases requires specificstrategies for preventi<strong>on</strong> andtreatment.With respect to period<strong>on</strong>tal disease,dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm dem<strong>on</strong>strates asuccessi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong> col<strong>on</strong>izati<strong>on</strong>with changes in bacterial floraobserved from health to disease.Researchers studied over 13,000plaque samples from 185 patients withc<strong>on</strong>diti<strong>on</strong>s ranging from oral health toperiod<strong>on</strong>tal disease. 4,23 As notedabove, based <strong>on</strong> their findings, a number<str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong> complexes were identifiedthat were associated with variousstages <str<strong>on</strong>g>of</str<strong>on</strong>g> disease initiati<strong>on</strong> andprogressi<strong>on</strong>. Bacterial species c<strong>on</strong>tainedin the yellow, green, and purplecomplexes appear to col<strong>on</strong>ize the subgingivalsulcus first and predominatein gingival health. In c<strong>on</strong>trast, orangecomplex bacteria are associated withgingivitis and gingival bleeding. Interestingly,bacteria <str<strong>on</strong>g>of</str<strong>on</strong>g> the orange complexmay also be associated with redcomplex microorganisms includingPorphyrom<strong>on</strong>as gingivalis, Tannerellaforsythensis, and Trep<strong>on</strong>ema denticola,organisms found in greater numbersin diseased sites and in moreadvanced period<strong>on</strong>tal disease. 10,24Bacterial communities living in abi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm possess resourceful survivalstrategies, including a broader habitatfor growth, nutriti<strong>on</strong>, waste eliminati<strong>on</strong>,and new col<strong>on</strong>izati<strong>on</strong>; envir<strong>on</strong>mentalniches for safety; barriers tothwart <strong>anti</strong><strong>microbial</strong> drug therapy; protecti<strong>on</strong>from the host’s defense systemincluding phagocytosis; and enhancedpathogenicity. 1,8 These strategiesaccount for the <strong>on</strong>going challenge <str<strong>on</strong>g>of</str<strong>on</strong>g>successfully c<strong>on</strong>trolling period<strong>on</strong>talinfecti<strong>on</strong> and disease progressi<strong>on</strong>. 25As the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm matures and proliferates,soluble compounds producedby pathogenic bacteria penetrate thesulcular epithelium. These compoundsstimulate host cells to producechemical mediators associated withthe inflammatory process 26 (see Figure4 <strong>on</strong> page 9).• Interleukin-1 beta (IL-1β),prostaglandins, tumor necrosis factoralpha (TNF-α), and matrixmetalloproteinases are mediatorsthat recruit neutrophils to the areavia chemotaxis and cause increasedpermeability <str<strong>on</strong>g>of</str<strong>on</strong>g> gingivalblood vessels, permitting plasmaproteins to migrate from within theblood vessels into the tissue.• As the gingival inflammatoryprocess c<strong>on</strong>tinues, additi<strong>on</strong>almediators are produced, and moreinflammatory cell types such asneutrophils, T cells, and m<strong>on</strong>ocytesare recruited to the area.• Proinflammatory cytokines are producedin the tissues as a resp<strong>on</strong>se tothe chr<strong>on</strong>ic inflammatory process,and these proteins may further escalatethe local inflammatoryresp<strong>on</strong>se and affect the initiati<strong>on</strong>and progressi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> systemic inflammati<strong>on</strong>and disease.The result <str<strong>on</strong>g>of</str<strong>on</strong>g> this chr<strong>on</strong>ic inflammati<strong>on</strong>is a breakdown <str<strong>on</strong>g>of</str<strong>on</strong>g> gingival collagenand accumulati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> an inflammatoryinfiltrate, leading to theclinical signs <str<strong>on</strong>g>of</str<strong>on</strong>g> gingivitis. In someindividuals, the inflammatory processwill also lead to the breakdown <str<strong>on</strong>g>of</str<strong>on</strong>g> collagenin the period<strong>on</strong>tal ligament andresorpti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the supporting alveolarb<strong>on</strong>e. It is at this point that the lesi<strong>on</strong>progresses from gingivitis to period<strong>on</strong>titis,c<strong>on</strong>tinuing the same challengefrom proinflammatory mediatorsas with chr<strong>on</strong>ic gingivitis. Thus,c<strong>on</strong>trolling dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm isessential to preventing and reversingSpecial <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 7
gingivitis as well as preventing andmanaging period<strong>on</strong>titis.Period<strong>on</strong>tal Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmInfecti<strong>on</strong> and SystemicHealthIn recent years, studies havedem<strong>on</strong>strated an associati<strong>on</strong> betweenperiod<strong>on</strong>titis and various systemic diseasesand c<strong>on</strong>diti<strong>on</strong>s, including cardiovasculardisease, diabetes mellitus,respiratory disease, adverse pregnancyoutcomes, obesity, pancreatic cancer,and Alzheimer’s disease. 27-57 Whileseveral <str<strong>on</strong>g>of</str<strong>on</strong>g> these associati<strong>on</strong>s have notbeen definitively established, biologicalmechanisms explaining some <str<strong>on</strong>g>of</str<strong>on</strong>g>the more extensively studied relati<strong>on</strong>shipsare emerging.The associati<strong>on</strong> between period<strong>on</strong>taldisease and some systemic diseasesmay relate to the ability <str<strong>on</strong>g>of</str<strong>on</strong>g> subgingivalplaque bacteria and/or their productsto gain access to the systemic circulati<strong>on</strong>through the ulceratedepithelium <str<strong>on</strong>g>of</str<strong>on</strong>g> the period<strong>on</strong>tal pocket.For example, envir<strong>on</strong>mental nicheslike a subgingival pocket that c<strong>on</strong>tainsanaerobic gram-negative microorganismscan potentially seed orange andred complex bacteria and/or theirproducts to distant sites through thecirculatory system. In this way, a dentalbi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm infecti<strong>on</strong> can potentiallyc<strong>on</strong>tribute to both oral and systemicinflammati<strong>on</strong>. 25Research <strong>on</strong> Period<strong>on</strong>tal MicroorganismsAtheromas. Direct evidence for therole <str<strong>on</strong>g>of</str<strong>on</strong>g> dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm infecti<strong>on</strong> in systemicinflammati<strong>on</strong> comes from findings<str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal microorganisms inhuman carotid atheromas. Studies <str<strong>on</strong>g>of</str<strong>on</strong>g>atheromatous lesi<strong>on</strong>s in carotid arteriesrevealed that over 40% <str<strong>on</strong>g>of</str<strong>on</strong>g> atheromasc<strong>on</strong>tain <strong>anti</strong>gens from period<strong>on</strong>talpathogens including P gingivalis, Tforsythensis, and Prevotella intermedia.28,58 In additi<strong>on</strong>, P gingivalis isknown to induce platelet aggregati<strong>on</strong>,a comp<strong>on</strong>ent <str<strong>on</strong>g>of</str<strong>on</strong>g> atheroma and thrombusformati<strong>on</strong>, 29 and invade endothelialcells in cell cultures. 59 While suchfindings suggest a possible invasi<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> atheromas by oral pathogens aswell as possible c<strong>on</strong>tributi<strong>on</strong> to theirdevelopment, it is important to notethat causality has yet to be established.Preterm Birth. Research suggeststhat period<strong>on</strong>tal pathogens may travelvia the bloodstream from the oral cavityto the placenta initiating pretermIn recent years, studies have dem<strong>on</strong>strated anassociati<strong>on</strong> between period<strong>on</strong>titis and varioussystemic diseases and c<strong>on</strong>diti<strong>on</strong>s, includingcardiovascular disease, diabetes mellitus,respiratory disease, adverse pregnancy outcomes,obesity, pancreatic cancer, and Alzheimer’s disease.birth. In an animal model, Han andcoworkers 60 found that period<strong>on</strong>talbacteria, including Fusobacteriumnucleatum, entered the bloodstreamfrom ulcerated gingival sulci or period<strong>on</strong>talpockets and negatively influencedthe normal birth process.Respiratory Disease. Likewise,bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm in the oral cavity may serve asa reservoir <str<strong>on</strong>g>of</str<strong>on</strong>g> infecti<strong>on</strong> leading to respiratorydisease. Pseudom<strong>on</strong>as aeruginosa,Staphylococcus aureus, andenteric bacteria have been shown tocol<strong>on</strong>ize the teeth <str<strong>on</strong>g>of</str<strong>on</strong>g> patients admittedto hospitals and l<strong>on</strong>g-term care facilities.These bacteria may be releasedinto saliva and aspirated into the lowerairway causing respiratory infecti<strong>on</strong>. 46-49,61Intubati<strong>on</strong> is another vehicle bywhich bacteria from the oral bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmcan be directly introduced into the respiratorysystem. Intubati<strong>on</strong> tubes supportbi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm growth c<strong>on</strong>tributing t<strong>on</strong>osocomial infecti<strong>on</strong> such as pneum<strong>on</strong>ia.This is <strong>on</strong>e reas<strong>on</strong> why oralintubati<strong>on</strong> raises the risk <str<strong>on</strong>g>of</str<strong>on</strong>g> nosocomialinfecti<strong>on</strong> in intensive and criticalcare hospital populati<strong>on</strong>s.Associati<strong>on</strong> With Chr<strong>on</strong>icDiseases and C<strong>on</strong>diti<strong>on</strong>sResearch has also suggested thatthe associati<strong>on</strong> between oral inflammati<strong>on</strong>and systemic inflammati<strong>on</strong>may be key to understanding andmanaging the significant, deleteriouseffects <strong>on</strong> the multiple organ systemsinvolved in some chr<strong>on</strong>ic diseases andc<strong>on</strong>diti<strong>on</strong>s (Figure 4). 26Cardiovascular Disease. Cardiovasculardisease is characterized byinflammatory plaque accumulati<strong>on</strong> inblood vessels that can cause thrombosesand lead to myocardial infarcti<strong>on</strong>.Atherosclerosis represents achr<strong>on</strong>ic inflammatory process thatcauses endothelial dysfuncti<strong>on</strong> andinjury to the elastic and muscular arterialtissue. Early atherosclerotic lesi<strong>on</strong>sc<strong>on</strong>tain neutrophils, m<strong>on</strong>ocytes, andlymphocytes. These leukocytes canaffect the vascular endothelial liningand cause oxidati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> low-densitylipoproteins. As a result, m<strong>on</strong>ocytes,induced to become macrophages, takeup these oxidized lipoproteins andbecome lipid-laden foam cells. As thelesi<strong>on</strong> progresses, the extracellularmatrix <str<strong>on</strong>g>of</str<strong>on</strong>g> the vessel wall is degraded byproteolytic enzymes and becomes susceptibleto rupture. Thromboses canocclude blood flow to the heart andbrain and eventually lead to infarcti<strong>on</strong>,heart attack, or stroke. 26Since atherosclerosis is inflammatoryby nature, identifying inflammatorymarkers that correlate with diseasestate is important. One recognized andc<strong>on</strong>sistent marker <str<strong>on</strong>g>of</str<strong>on</strong>g> systemic inflammati<strong>on</strong>and poor cardiovascular prognosisis the acute-phase protein C-reactiveprotein (CRP), the level <str<strong>on</strong>g>of</str<strong>on</strong>g> whichrises with systemic inflammati<strong>on</strong>. 62,63Animal model studies <str<strong>on</strong>g>of</str<strong>on</strong>g> the relati<strong>on</strong>shipbetween cardiovascular diseaseand period<strong>on</strong>tal disease dem<strong>on</strong>stratethat clinically induced oral infecti<strong>on</strong>with P gingivalis will increase atheromasize and elevate CRP levels in theblood. 30 C<strong>on</strong>versely, some studies have8 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Figure 4. Subgingival plaque bacteria and/or their products may gain access to distant sites in the bodythrough the circulatory system and may potentially c<strong>on</strong>tribute to systemic inflammati<strong>on</strong>; in this way, adental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm infecti<strong>on</strong> may potentially c<strong>on</strong>tribute to various systemic diseases and c<strong>on</strong>diti<strong>on</strong>s.(Illustrati<strong>on</strong> owned by McNEIL-PPC, Inc. and provided for educati<strong>on</strong>al purposes <strong>on</strong>ly. May not bereproduced without the prior written permissi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> McNEIL-PPC, Inc.)shown that treatment <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>titisdecreases CRP blood levels, 64 thoughthis has not been a c<strong>on</strong>sistent finding.Diabetes Mellitus. Diabetes mellitusis another chr<strong>on</strong>ic systemic diseaseassociated with period<strong>on</strong>titis. In fact,period<strong>on</strong>titis has been identified as <strong>on</strong>e<str<strong>on</strong>g>of</str<strong>on</strong>g> the major complicati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> diabetes.65 Although diabetes increases thesusceptibility to period<strong>on</strong>tal disease,38,39,65 period<strong>on</strong>titis may alsoincrease the difficulty <str<strong>on</strong>g>of</str<strong>on</strong>g> maintainingsatisfactory glycemic c<strong>on</strong>trol in peoplewith diabetes as compared withthose with diabetes without period<strong>on</strong>titis.40 One biological mechanism proposedto explain the increased incidenceand severity <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>taldisease in individuals with diabetes isthe finding <str<strong>on</strong>g>of</str<strong>on</strong>g> elevated levels <str<strong>on</strong>g>of</str<strong>on</strong>g> inflammatorymediators in the gingivalcrevicular fluid from period<strong>on</strong>tal pockets<str<strong>on</strong>g>of</str<strong>on</strong>g> patients with diabetes with poorglycemic c<strong>on</strong>trol as compared withthose with diabetes who are well c<strong>on</strong>trolledor those without diabetes. Thosewith poor glycemic c<strong>on</strong>trol had c<strong>on</strong>siderableperiod<strong>on</strong>tal destructi<strong>on</strong> withan equivalent bacterial challenge. 39,66Of note, the proinflammatory cytokineTNF-α plays a significant role in thisprocess. TNF-α has a major role ininsulin resistance, the primary cause <str<strong>on</strong>g>of</str<strong>on</strong>g>type 2 diabetes, and is produced inlarge qu<strong>anti</strong>ties by fat cells. Period<strong>on</strong>titisalso has been associated withincreased levels <str<strong>on</strong>g>of</str<strong>on</strong>g> TNF-α. Elevatedlevels <str<strong>on</strong>g>of</str<strong>on</strong>g> TNF-α may lead to greaterb<strong>on</strong>e loss by killing cells that repairdamaged c<strong>on</strong>nective tissue or b<strong>on</strong>e.Elevated TNF-α levels also may exacerbateinsulin resistance and worsenglycemic c<strong>on</strong>trol. 44,66,67Adverse Pregnancy Outcomes.Studies also dem<strong>on</strong>strate that period<strong>on</strong>taldiseases are associated withthe risk <str<strong>on</strong>g>of</str<strong>on</strong>g> adverse pregnancy outcomes,especially preterm low-birthweightinfants. 50-52 Chr<strong>on</strong>ic infecti<strong>on</strong>,such as that found with chr<strong>on</strong>ic period<strong>on</strong>titis,can stimulate the inflammatoryprocess throughout the body. Inthe placenta, this may lead to elevatedamniotic levels <str<strong>on</strong>g>of</str<strong>on</strong>g> prostaglandins,TNF-α, and IL-1 and IL-6, stimulatingpremature rupture <str<strong>on</strong>g>of</str<strong>on</strong>g> membranes,preterm labor, and the birth <str<strong>on</strong>g>of</str<strong>on</strong>g> lowbirth-weightinfants. Interventi<strong>on</strong> studiesare currently under way to investigatea cause and effect relati<strong>on</strong>shipSpecial <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 9
Table I. Examples <str<strong>on</strong>g>of</str<strong>on</strong>g> Antiseptic Mouth<strong>rinses</strong>*Active Ingredients Brands Indicati<strong>on</strong>s C<strong>on</strong>traindicati<strong>on</strong>s0.12% Chlorhexidine Peridex ®† (3M ESPE, Gingivitis, Those hypersensitive togluc<strong>on</strong>ate (available St Paul, MN) supragingival plaque chlorhexidinegluc<strong>on</strong>ate or otherby prescripti<strong>on</strong>) PerioGard ®† (Colgate formula ingredients.Oral Pharmaceuticals,L<strong>on</strong>g-term use: can causeInc., Cant<strong>on</strong>, MA)moderate staining, increasedPerioRx ®† (Discuscalculus formati<strong>on</strong>, and possible<str<strong>on</strong>g>Dental</str<strong>on</strong>g>, Culver City, CA)alterati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> taste percepti<strong>on</strong>Cant<strong>on</strong>, MA)Various generics †Four essential oils: Listerine ® Antiseptic † Supragingival plaque, Children under 12 yearseucalyptol, menthol, (Johns<strong>on</strong> & Johns<strong>on</strong> gingivitis, oral malodormethyl salicylate, Healthcare ProductsthymolDivisi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> McNEIL-PPC,Inc., Skillman, NJ)Various generics †Cetylpyridinium Breath Rx ® (Discus <str<strong>on</strong>g>Dental</str<strong>on</strong>g>, Supragingival plaque, Children under 6 yearschloride Culver City, CA) gingivitis, oral malodorColgate Viadent ® (Colgate-Palmolive, New York, NY)Crest ® Pro-Health Rinse(Procter & Gamble,Cincinnati, OH)* For the mechanisms <str<strong>on</strong>g>of</str<strong>on</strong>g> acti<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>septic <strong>mouth</strong><strong>rinses</strong>, see pages19 and 20.† Has received the ADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance; note that as the ADA Sealprogram has recently phased out prescripti<strong>on</strong> products, chlorhexidinegluc<strong>on</strong>ate products no l<strong>on</strong>ger carry the ADA Seal.between advanced period<strong>on</strong>titis andadverse pregnancy outcomes.Strategies for Managing<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm toPromote HealthAlthough dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm cannot becompletely eliminated, its pathogenicitycan be lessened through effectiveoral hygiene measures. Daily toothbrushing,interdental cleaning, and theuse <str<strong>on</strong>g>of</str<strong>on</strong>g> topical <strong>anti</strong><strong>microbial</strong> chemotherapeuticsare patient-based strategies toreduce the bacterial bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm and to helpprevent period<strong>on</strong>tal diseases. American<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> (ADA)–Accepted <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong>have been shown to help prevent andreduce plaque and gingivitis whenadded to a daily oral hygiene regimen<str<strong>on</strong>g>of</str<strong>on</strong>g> mechanical plaque removal. Further,bacteria from the bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm <strong>on</strong> mucosaland tooth surfaces are shed c<strong>on</strong>stantlyinto saliva and transferred to otherareas <str<strong>on</strong>g>of</str<strong>on</strong>g> the <strong>mouth</strong>. Since oral mucosa,which represents about 80% <str<strong>on</strong>g>of</str<strong>on</strong>g> the oralcavity surface, 68 can serve as a reservoirfor pathogenic bacteria that can betransferred to the tooth surface and sulcus,<str<strong>on</strong>g>supplement</str<strong>on</strong>g>ing mechanical plaquec<strong>on</strong>trol methods with topical <strong>anti</strong><strong>microbial</strong>smay also play an importantrole in reducing reservoirs <str<strong>on</strong>g>of</str<strong>on</strong>g>pathogens that are unaffected by brushingand flossing directed at the toothsurface.Using Evidence inPracticeProducts recommended to patientsshould be those that have documentedefficacy and safety (see pages 13 to25). Only 2 nati<strong>on</strong>ally branded <strong>anti</strong>septic<strong>mouth</strong><strong>rinses</strong> and their genericequivalents have received the ADACouncil <strong>on</strong> Scientific Affairs Seal <str<strong>on</strong>g>of</str<strong>on</strong>g>Acceptance for c<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingivalplaque and gingivitis: Listerine ®(fixed combinati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> essential oils)and Peridex ® (0.12% chlorhexidinegluc<strong>on</strong>ate). However, due to recentchanges in the ADA Seal Program,Peridex ® and its generic equivalentsno l<strong>on</strong>ger carry the ADA Seal becausechlorhexidine gluc<strong>on</strong>ate is a prescripti<strong>on</strong>product (see also page 32 formore informati<strong>on</strong> <strong>on</strong> the ADA SealProgram). The fixed combinati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>essential oils and cetylpyridiniumchloride have also been reviewed by aFood and Drug Administrati<strong>on</strong> (FDA)advisory committee and have receiveda Category I recommendati<strong>on</strong>, meaningthey have been found to be safeand effective for the c<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g>10 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
supragingival plaque and gingivitis.Peridex ® and its generic equivalents,which are prescripti<strong>on</strong> products, havebeen approved for marketing by theFDA via the New Drug Applicati<strong>on</strong>route (or for generics, the AbbreviatedNew Drug Applicati<strong>on</strong> process) (seealso pages 14 and 15). Examples <str<strong>on</strong>g>of</str<strong>on</strong>g>effective <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong>currently <strong>on</strong> the market appear inTable I.C<strong>on</strong>clusi<strong>on</strong><str<strong>on</strong>g>Dental</str<strong>on</strong>g> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm is a complex, organized<strong>microbial</strong> community that is theprimary etiologic factor for the mostfrequently occurring oral diseases,dental caries and period<strong>on</strong>tal diseases.Although the dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm cannot beeliminated, it can be c<strong>on</strong>trolled withcomprehensive mechanical andchemotherapeutic oral hygiene practices.Teaching patients to use dailybrushing, interdental cleaning, and<strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong> that carrythe ADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance increasesthe likelihood <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal diseasepreventi<strong>on</strong> and reducti<strong>on</strong>. Althoughadditi<strong>on</strong>al research is needed, there isthe possibility that these cost-effective,preventive strategies may minimizethe effect <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal diseases<strong>on</strong> specific systemic c<strong>on</strong>diti<strong>on</strong>s.References1. Costert<strong>on</strong> JW, Stewart PS, Greenberg EP. Bacterial bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms:a comm<strong>on</strong> cause <str<strong>on</strong>g>of</str<strong>on</strong>g> persistent infecti<strong>on</strong>s. Science.1999;284:1318-1322.2. van Houte J. Role <str<strong>on</strong>g>of</str<strong>on</strong>g> micro-organisms in caries etiology. JDent Res. 1994;73:672-681.3. Stenudd C, Nordlund A, Ryberg M, et al. The associati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>bacterial adhesi<strong>on</strong> with dental caries. J Dent Res.2001;80:2005-2010.4. Socransky SS, Haffajee AD, Cugini MA, et al. Microbial complexesin subgingival plaque. J Clin Period<strong>on</strong>tol. 1998;25:134-144.5. Haffajee AD, Socransky SS. Microbial etiological agents <str<strong>on</strong>g>of</str<strong>on</strong>g>destructive period<strong>on</strong>tal diseases. Period<strong>on</strong>tol 2000.1994;5:78-111.6. Loesche WJ. Chemotherapy <str<strong>on</strong>g>of</str<strong>on</strong>g> dental plaque infecti<strong>on</strong>s. OralSci Rev. 1976;9:65-107.7. Theilade E. The n<strong>on</strong>-specific theory in <strong>microbial</strong> etiology <str<strong>on</strong>g>of</str<strong>on</strong>g>inflammatory period<strong>on</strong>tal disease. J Clin Period<strong>on</strong>tol.1986;13:905-911.8. Thomas JG, Nakaishi LA. Managing the complexity <str<strong>on</strong>g>of</str<strong>on</strong>g> adynamic bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. J Am Dent Assoc. 2006;137(11 suppl):10S-15S.9. Loesche WJ. DNA probe and enzyme analysis in period<strong>on</strong>taldiagnostics. J Period<strong>on</strong>tol. 1992;63:1102-1109.10. Socransky SS, Haffajee AD. Period<strong>on</strong>tal <strong>microbial</strong> etiology.Period<strong>on</strong>tol 2000. 2005;38:135-187.11. Socransky SS, Haffajee AD. <str<strong>on</strong>g>Dental</str<strong>on</strong>g> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms: difficult therapeutictargets. Period<strong>on</strong>tol 2000. 2002;28:12-55.12. Brown MR, Gilbert P. Sensitivity <str<strong>on</strong>g>of</str<strong>on</strong>g> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms to <strong>anti</strong><strong>microbial</strong>agents. J Appl Bacteriol. 1993;74(suppl):87S-97S.13. Gilbert P, Das J, Foley I. Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm susceptibility to <strong>anti</strong><strong>microbial</strong>s.Adv Dent Res. 1997;11:160-167.14. Costert<strong>on</strong> JW, Lewandowski Z, DeBeer D, et al. Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms,the customized micr<strong>on</strong>iche. J Bacteriol. 1994;176:2137-2142.15. Wood SR, Kirkham J, Marsh PD, et al. Architecture <str<strong>on</strong>g>of</str<strong>on</strong>g> intactnatural human plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms studied by c<strong>on</strong>focal laser scanningmicroscopy. J Dent Res. 2000; 79:21-27.16. Levine MJ, Reddy MS, Tabak LA, et al. Structural aspects <str<strong>on</strong>g>of</str<strong>on</strong>g>salivary glycoproteins. J Dent Res. 1987;66:436-441.17. Tabak LA, Levine MJ, Mandel ID, Ellis<strong>on</strong> SA. Role <str<strong>on</strong>g>of</str<strong>on</strong>g> salivarymucins in the protecti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the oral cavity. J Oral Pathol.1982;11:1-17.18. Gibb<strong>on</strong>s RJ, Hay DI. Human salivary acidic proline-rich proteinsand statherin promote the attachment <str<strong>on</strong>g>of</str<strong>on</strong>g> Actinomycesviscosus LY7 to apatitic surfaces. Infect Immun. 1988;56:439-445.19. Costert<strong>on</strong> JW, Cheng KJ, Geesey GG, et al. Bacterial bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilmsin nature and disease. Annu Rev Microbiol. 1987;41:435-464.20. Gibb<strong>on</strong>s RJ. Microbial ecology: adherent interacti<strong>on</strong>s whichmay affect <strong>microbial</strong> ecology in the <strong>mouth</strong>. J Dent Res.1984;63:378-385.21. Whittaker CJ, Klier CM, Kolenbrander PE. Mechanisms <str<strong>on</strong>g>of</str<strong>on</strong>g>adhesi<strong>on</strong> by oral bacteria. Annu Rev Microbiol. 1996;50:513-552.22. Wirthlin MR Jr, Armitage GC. <str<strong>on</strong>g>Dental</str<strong>on</strong>g> plaque and calculus:<strong>microbial</strong> bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms and period<strong>on</strong>tal diseases. In: Rose LF,Mealey BL, Genco RJ, Cohen W, eds. Period<strong>on</strong>tics: Medicine,Surgery and Implants. St. Louis, MO: Elsevier Mosby;2004.23. Socransky SS, Haffajee AD, Ximenez-Fyvie LA, et al. Ecologicalc<strong>on</strong>siderati<strong>on</strong>s in the treatment <str<strong>on</strong>g>of</str<strong>on</strong>g> Actinobacillus actinomycetemcomitansand Porphyrom<strong>on</strong>as gingivalis period<strong>on</strong>talinfecti<strong>on</strong>s. Period<strong>on</strong>tol 2000. 1999;20:341-362.24. Kojima T, Yasui S, Ishikawa I. Distributi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> Porphyrom<strong>on</strong>asgingivalis in adult period<strong>on</strong>titis patients. J Period<strong>on</strong>tol.1993;64:1231-1237.25. Grossi S, Mealey BL, Rose LF. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal infecti<strong>on</strong><strong>on</strong> the systemic c<strong>on</strong>diti<strong>on</strong>. In: Rose LF, Mealey BL,Genco RJ, Cohen W, eds. Period<strong>on</strong>tics: Medicine, Surgeryand Implants. St. Louis, MO: Elsevier Mosby; 2004.26. Gurenlian JR. Inflammati<strong>on</strong>: the relati<strong>on</strong>ship between oralhealth and systemic disease. Access. 2006;20(4)(suppl):1-9.27. Epstein SE. The multiple mechanisms by which infecti<strong>on</strong>may c<strong>on</strong>tribute to atherosclerosis development and course.Circ Res. 2002;90:2-4.28. Haraszthy VI, Zamb<strong>on</strong> JJ, Trevisan M, et al. Identificati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>period<strong>on</strong>tal pathogens in atheromatous plaques. J Period<strong>on</strong>tol.2000;71:1554-1560.29. Herzberg MC, Meyer MW. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> oral flora <strong>on</strong> platelets:possible c<strong>on</strong>sequences in cardiovascular disease. J Period<strong>on</strong>tol.1996;67:1138-1142.30. Paquette DW. The period<strong>on</strong>tal-cardiovascular link. CompendC<strong>on</strong>tin Educ Dent. 2004;25:681-692.31. Desvarieux M, Demmer RT, Rundek T, et al. Period<strong>on</strong>talmicrobiota and carotid intima-media thickness: the oral infecti<strong>on</strong>sand vascular disease epidemiology study (INVEST).Circulati<strong>on</strong>. 2005;111:576-582.32. Ti<strong>on</strong>g AY, Brieger D. Inflammati<strong>on</strong> and cor<strong>on</strong>ary artery disease.Am Heart J. 2005;150:11-18.33. Meurman JH, Sanz M, Janket SJ. Oral health, atherosclerosis,and cardiovascular disease. Crit Rev Oral Biol Med.2004;15:403-413.34. Chun YH, Chun KR, Olguin D, Wang HL. Biological foundati<strong>on</strong>for period<strong>on</strong>titis as a potential risk factor for atherosclerosis.J Period<strong>on</strong>tal Res. 2005;40:87-95.35. Hung HC, Willett W, Merchant A, et al. Oral health and peripheralarterial disease. Circulati<strong>on</strong>. 2003;107:1152-1157.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 11
36. Wu T, Trevisan M, Genco RJ, et al. Period<strong>on</strong>tal disease andrisk <str<strong>on</strong>g>of</str<strong>on</strong>g> cerebrovascular disease: the first nati<strong>on</strong>al health andnutriti<strong>on</strong> examinati<strong>on</strong> survey and its follow-up study. ArchIntern Med. 2000;160:2749-2755.37. Joshipura KJ, Hung HC, Rimm EB, et al. Period<strong>on</strong>tal disease,tooth loss, and incidence <str<strong>on</strong>g>of</str<strong>on</strong>g> ischemic stroke. Stroke.2003;34:47-52.38. Nishimura F, Takahashi K, Kurihara M, et al. Period<strong>on</strong>tal diseaseas a complicati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> diabetes mellitus. Ann Period<strong>on</strong>tol.1998;3:20-29.39. Ryan ME, Carnu O, Kamer A. The influence <str<strong>on</strong>g>of</str<strong>on</strong>g> diabetes <strong>on</strong>the period<strong>on</strong>tal tissues. J Am Dent Assoc. 2003;134:34S-40S.40. Taylor GW, Burt BA, Becker MP, et al. Severe period<strong>on</strong>titisand risk for poor glycemic c<strong>on</strong>trol in patients with n<strong>on</strong>-insulindependentdiabetes mellitus. J Period<strong>on</strong>tol. 1996;67(suppl10):1085-1093.41. Grossi SG, Skrepcinski FB, DeCaro T, et al. Treatment <str<strong>on</strong>g>of</str<strong>on</strong>g>period<strong>on</strong>tal disease in diabetics reduces glycated hemoglobin.J Period<strong>on</strong>tol. 1997;68:713-719.42. Miller LS, Manwell MA, Newbold D, et al. The relati<strong>on</strong>shipbetween reducti<strong>on</strong> in period<strong>on</strong>tal inflammati<strong>on</strong> and diabetesc<strong>on</strong>trol: a report <str<strong>on</strong>g>of</str<strong>on</strong>g> 9 cases. J Period<strong>on</strong>tol. 1992;63:843-848.43. Mealey BL, Rethman MP. Period<strong>on</strong>tal disease and diabetesmellitus: bidirecti<strong>on</strong>al relati<strong>on</strong>ship. Dent Today. 2003;22:107-113.44. Grossi SG, Genco RJ. Period<strong>on</strong>tal disease and diabetesmellitus: a two-way relati<strong>on</strong>ship. Ann Period<strong>on</strong>tol. 1998;3:51-61.45. Taylor GW. Bidirecti<strong>on</strong>al interrelati<strong>on</strong>ships between diabetesand period<strong>on</strong>tal diseases: an epidemiologic perspective. AnnPeriod<strong>on</strong>tol. 2001;6:99-112.46. Scannapieco FA. Role <str<strong>on</strong>g>of</str<strong>on</strong>g> oral bacteria in respiratory infecti<strong>on</strong>.J Period<strong>on</strong>tol. 1999;70:793-802.47. Scannapieco FA, Bush RB, Paju S. Associati<strong>on</strong>s betweenperiod<strong>on</strong>tal disease and risk for nosocomial bacterial pneum<strong>on</strong>iaand chr<strong>on</strong>ic obstructive pulm<strong>on</strong>ary disease: a systematicreview. Ann Period<strong>on</strong>tol. 2003;8:54-69.48. Hayes C, Sparrow D, Cohen M, et al. The associati<strong>on</strong>between alveolar b<strong>on</strong>e loss and pulm<strong>on</strong>ary functi<strong>on</strong>: the VA<str<strong>on</strong>g>Dental</str<strong>on</strong>g> L<strong>on</strong>gitudinal Study. Ann Period<strong>on</strong>tol. 1998;3:257-261.49. Scannapieco FA, Ho AW. Potential associati<strong>on</strong>s betweenchr<strong>on</strong>ic respiratory disease and period<strong>on</strong>tal disease: analysis<str<strong>on</strong>g>of</str<strong>on</strong>g> Nati<strong>on</strong>al Health and Nutriti<strong>on</strong> Examinati<strong>on</strong> Survey III.J Period<strong>on</strong>tol. 2001;72:50-56.50. Offenbacher S, Katz V, Fertik G, et al. Period<strong>on</strong>tal infecti<strong>on</strong>as a possible risk factor for preterm low birth weight. J Period<strong>on</strong>tol.1996;67(suppl 10):1103-1113.51. Jeffcoat MK, Geurs NC, Reddy MS, et al. Period<strong>on</strong>tal infecti<strong>on</strong>and preterm birth: results <str<strong>on</strong>g>of</str<strong>on</strong>g> a prospective study. J AmDent Assoc. 2001;132:875-880.52. Scannapieco FA, Bush RB, Paju S. Period<strong>on</strong>tal disease asa risk factor for adverse pregnancy outcomes: a systematicreview. Ann Period<strong>on</strong>tol. 2003;8:70-78.53. Stein PS, Scheff S, Daws<strong>on</strong> DR III. Alzheimer’s disease andperiod<strong>on</strong>tal disease: mechanisms underlying a potential bidirecti<strong>on</strong>alrelati<strong>on</strong>ship. Grand Rounds Oral-Sys Med.2006;1:14-24D.54. Michaud DS, Joshipura K, Giovannucci E, Fuchs CS. Aprospective study <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal disease and pancreatic cancerin US male health pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als. J Natl Cancer Inst.2007;99:171-175.55. Stolzenberg-Solom<strong>on</strong> RZ, Dodd KW, Blaser MJ, et al. Toothloss, pancreatic cancer, and Helicobacter pylori. Am J ClinNutr. 2003;78:176-181.56. Al-Zahrani MS, Bissada NF, Borawskit EA. Obesity and period<strong>on</strong>taldisease in young, middle-aged, and older adults. JPeriod<strong>on</strong>tol. 2003;74:610-615.57. Reeves AF, Rees JM, Schiff M, Hujoel P. Total body weightand waist circumference associated with chr<strong>on</strong>ic period<strong>on</strong>titisam<strong>on</strong>g adolescents in the United States. Arch PediatrAdolesc Med. 2006;160:894-899.58. Chiu B. Multiple infecti<strong>on</strong>s in carotid atherosclerotic plaques.Am Heart J. 1999;138:S534-S536.59. Dorn BR, Burks JN, Seifert KN, Progulske-Fox A. Invasi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>endothelial and epithelial cells by strains <str<strong>on</strong>g>of</str<strong>on</strong>g> Porphyrom<strong>on</strong>asgingivalis. FEMS Microbiol Lett. 2000;187:139-144.60. Han YW, Redline RW, Li M, et al. Fusobacterium nucleatuminduces premature and term stillbirths in pregnant mice: implicati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> oral bacteria in preterm birth. Infect Immun.2004;72:2272-2279.61. Scannapieco FA. Period<strong>on</strong>tal inflammati<strong>on</strong>: from gingivitisto systemic disease? Compend C<strong>on</strong>tin Educ Dent.2004;25(suppl 1):16-25.62. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactiveprotein and other markers <str<strong>on</strong>g>of</str<strong>on</strong>g> inflammati<strong>on</strong> in the predicti<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> cardiovascular disease in women. N Engl J Med.2000;342:836-843.63. Liuzzo G, Biasucci LM, Gallimore JR, et al. The prognosticvalue <str<strong>on</strong>g>of</str<strong>on</strong>g> C-reactive protein and serum amyloid A protein insevere unstable angina. N Engl J Med. 1994;331:417-424.64. D’Aiuto F, Parkar M, Andreou G, et al. Period<strong>on</strong>titis and systemicinflammati<strong>on</strong>: c<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g> the local infecti<strong>on</strong> is associatedwith a reducti<strong>on</strong> in serum inflammatory markers. J Dent Res.2004;83:156-160.65. Löe H. Period<strong>on</strong>tal disease: the sixth complicati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> diabetesmellitus. Diabetes Care. 1993;16:329-334.66. Salvi GE, Yalda B, Collins JG, et al. Inflammatory mediatorresp<strong>on</strong>se as a potential risk marker for period<strong>on</strong>tal diseasesin insulin-dependent diabetes mellitus patients. J Period<strong>on</strong>tol.1997;68:127-135.67. Lalla E, Lamster IB, Feit M, et al. Blockade <str<strong>on</strong>g>of</str<strong>on</strong>g> RAGE suppressesperiod<strong>on</strong>titis-associated b<strong>on</strong>e loss in diabetic mice.J Clin Invest. 2000;105:1117-1124.68. Mager DL, Ximenez-Fyvie LA, Haffajee AD, Socransky SS.Distributi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> selected bacterial species <strong>on</strong> intraoral surfaces.J Clin Period<strong>on</strong>tol. 2003;30:644-654.12 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Safety and Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> Anti<strong>microbial</strong> Mouth<strong>rinses</strong>in Clinical PracticeLouis G. DePaola, DDS, MS, and Ann Eshenaur Spolarich, RDH, PhDIntroducti<strong>on</strong>Mechanical plaque removal throughtoothbrushing and flossing has beenthe universally accepted “gold standard”for maintaining oral health sincethe early 1960s. However, numerousstudies have shown that most patientsdo not effectively clean interdentallyto remove dental plaque daily. 1-3 By theearly 1980s, chemotherapeutic agentswere marketed as adjuncts to brushingand flossing; however, no definitiveguidelines for the evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> theirsafety and efficacy were available.Both the American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong>(ADA) and the Food and Drug Administrati<strong>on</strong>(FDA) have established standardsfor assessing the safety and efficacy<str<strong>on</strong>g>of</str<strong>on</strong>g> over-the-counter (OTC) andprescripti<strong>on</strong> <strong>mouth</strong><strong>rinses</strong>.ADA Safety andEfficacy Guidelines forMouth<strong>rinses</strong>AbstractEfficacy Overview. The use <str<strong>on</strong>g>of</str<strong>on</strong>g> an <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse is an importantadjunct to toothbrushing and interdental cleaning. To varying degrees,chlorhexidine gluc<strong>on</strong>ate (CHG), cetylpyridinium chloride (CPC), and essentialoils (EO) interrupt the integrity <str<strong>on</strong>g>of</str<strong>on</strong>g> the bacterial cell membrane, leadingto lysis and death. CHG binds to salivary mucins, tooth structure, dentalplaque, and oral s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissues and is released slowly into the <strong>mouth</strong>, whereit inhibits adsorpti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> bacteria <strong>on</strong>to teeth. CHG is active against a widerange <str<strong>on</strong>g>of</str<strong>on</strong>g> gram-positive and gram-negative microorganisms. CPC binds toteeth and plaque to a lesser degree than CHG and is generally less efficaciousthan CHG. CHG and EO penetrate plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm and producechanges in <strong>microbial</strong> cell surface morphology that alter coaggregati<strong>on</strong>,recol<strong>on</strong>izati<strong>on</strong>, and, thus, survival. CHG, CPC, and EO are active againsta wide variety <str<strong>on</strong>g>of</str<strong>on</strong>g> aerobic and anaerobic bacteria. An overview <str<strong>on</strong>g>of</str<strong>on</strong>g> the Foodand Drug Administrati<strong>on</strong> and American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> rigorousapproval processes for efficacy and safety is provided.Safety Overview. L<strong>on</strong>g-term use <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG or EO does not adversely affectthe ecology <str<strong>on</strong>g>of</str<strong>on</strong>g> oral <strong>microbial</strong> flora, including <strong>microbial</strong> overgrowth, opportunisticinfecti<strong>on</strong>, or development <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong> resistance. L<strong>on</strong>g-term use<str<strong>on</strong>g>of</str<strong>on</strong>g> CHG, CPC, or EO does not c<strong>on</strong>tribute to s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissue lesi<strong>on</strong>s or mucosalaberrati<strong>on</strong>s and has no serious adverse effect <strong>on</strong> salivary flow, taste, toothdeposits, or dental restorati<strong>on</strong>. There is no evidence <str<strong>on</strong>g>of</str<strong>on</strong>g> a causal linkbetween alcohol-c<strong>on</strong>taining <strong>mouth</strong><strong>rinses</strong> and the risk <str<strong>on</strong>g>of</str<strong>on</strong>g> oral and pharyngealcancer.Key words: Anti<strong>microbial</strong> <strong>mouth</strong>rinse, efficacy, gingivitis, mechanism <str<strong>on</strong>g>of</str<strong>on</strong>g>acti<strong>on</strong>, safetySince 1931, the ADA, through itsvoluntary Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance Program,has promoted the use <str<strong>on</strong>g>of</str<strong>on</strong>g> oraland dental products that are both safeand effective. Published guidelinesdeveloped by the ADA list the acceptancecriteria for each type <str<strong>on</strong>g>of</str<strong>on</strong>g> agent,product, or device. In order to obtainthe Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance, a companymust provide evidence establishingthat a submitted agent, product, ordevice meets or exceeds the guidelinesfor that particular usage and issafe and effective. Additi<strong>on</strong>ally, theproduct must have been approved formarketing in the United States by theFDA. In 1985, the ADA recognizedthe potential benefits <str<strong>on</strong>g>of</str<strong>on</strong>g> some chemotherapeuticformulati<strong>on</strong>s, givingimpetus to the development <str<strong>on</strong>g>of</str<strong>on</strong>g> guidelinesfor the evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>plaqueand <strong>anti</strong>gingivitis chemotherapeuticagents for inclusi<strong>on</strong> in the Seal Program,which are still in use today. 4 Inorder to be awarded the Seal, an<strong>anti</strong>plaque and <strong>anti</strong>gingivitis chemotherapeuticmust 5• Be tested in populati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> typicalproduct users in a randomized,parallel-group, or crossover clinicaltrial in which the test productis compared with a negative c<strong>on</strong>troland, if appropriate, an activec<strong>on</strong>trol• Be supported by data from atleast two 6-m<strong>on</strong>th studies c<strong>on</strong>ductedat independent sites, withassessment <str<strong>on</strong>g>of</str<strong>on</strong>g> gingivitis andqualitative and qu<strong>anti</strong>tativeassessment <str<strong>on</strong>g>of</str<strong>on</strong>g> plaque performedat baseline, an intermediate point(usually 3 m<strong>on</strong>ths), and 6m<strong>on</strong>ths• Document a statistically significantreducti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingivalplaque and gingivitis as comparedwith a negative c<strong>on</strong>trol ineach <str<strong>on</strong>g>of</str<strong>on</strong>g> the 2 studies and dem<strong>on</strong>stratea statistically significantreducti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> gingivitis for the<strong>mouth</strong>rinse group <str<strong>on</strong>g>of</str<strong>on</strong>g> at least 15%for any <strong>on</strong>e study and an averagereducti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> 20% in the 2studies compared with the c<strong>on</strong>trolgroupSpecial <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 13
Since 1931, the ADA, through itsvoluntary Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance Program,has promoted the use <str<strong>on</strong>g>of</str<strong>on</strong>g> oral anddental products that are both safeand effective.• Establish product safety withrespect to s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissues, teeth, toxicology,and effects <strong>on</strong> the oralflora (eg, adverse shifts in <strong>microbial</strong>populati<strong>on</strong>s, the development<str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong> resistance, and theemergence <str<strong>on</strong>g>of</str<strong>on</strong>g> opportunisticorganisms)Data from the studies are then presentedto and reviewed by the ADACouncil <strong>on</strong> Scientific Affairs. If theproduct meets the established standards,it is awarded the ADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g>Acceptance. 4,5For the pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al and c<strong>on</strong>sumer,the ADA Seal for <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong>indicates that• Product data have successfullyunderg<strong>on</strong>e an intensive, n<strong>on</strong>biasedsafety and efficacy review• Evidence supports the manufacturer’sclaim for effectivenessagainst supragingival dental plaqueand gingivitis• The product is safe when used asdirectedFDA Regulati<strong>on</strong>The FDA regulates prescripti<strong>on</strong>drugs as well as any OTC productsthat make therapeutic claims, such asthe reducti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> gingivitis. The FDAhas accepted key elements for gingivitisassessment used by the ADASeal Program as appropriate for itsreview. However, in c<strong>on</strong>trast to theADA, which evaluates products, theFDA evaluates active ingredientswhile recognizing that the way inwhich an ingredient is formulated mayaffect its clinical activity. In 2003, therecommendati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> the FDA’s <str<strong>on</strong>g>Dental</str<strong>on</strong>g>Plaque Subcommittee <str<strong>on</strong>g>of</str<strong>on</strong>g> the N<strong>on</strong>prescripti<strong>on</strong>Drugs Advisory Committeewere published, and theyincluded the c<strong>on</strong>diti<strong>on</strong>s under whichOTC products for the reducti<strong>on</strong> orpreventi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> dental plaque and gingivitiswould be recognized as safe,effective, and not misbranded. 6,7 Inadditi<strong>on</strong> to data supporting effectiveness,the following criteria are examinedby the FDA 6 :• Incidence and risk <str<strong>on</strong>g>of</str<strong>on</strong>g> adversereacti<strong>on</strong>s and significant sideeffects when used according toadequate directi<strong>on</strong>s• Margin <str<strong>on</strong>g>of</str<strong>on</strong>g> safety with normal use• Potential for harm from abuse ormisuse• Potential for inducing adverseside effects (such as irritati<strong>on</strong>,ulcerati<strong>on</strong>, inflammati<strong>on</strong>, erosi<strong>on</strong>,damage to teeth/restorati<strong>on</strong>s)• Benefit-risk ratioAfter assessing an OTC ingredient,the FDA assigns the ingredient to acategory <str<strong>on</strong>g>of</str<strong>on</strong>g> I, II, or III 6,7 :• Category I: The ingredient isboth safe and effective and is notmisbranded.• Category II: The ingredient isnot generally recognized as safeand effective or is misbranded.• Category III: There are insufficientdata to evaluate safetyand/or effectiveness.The FDA may also approve products,both prescripti<strong>on</strong> and OTC,through the New Drug Applicati<strong>on</strong>(NDA) process. The NDA process isa more lengthy <strong>on</strong>e that also requiresdocumentati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> both the safety andefficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> the product.Mouth<strong>rinses</strong> That MeetADA and/or FDAGuidelinesTwo <strong>anti</strong>septic <strong>mouth</strong><strong>rinses</strong> (andtheir generic equivalents) have beenawarded the ADA Seal for chemotherapeuticc<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingivalplaque and gingivitis: 0.12% chlorhexidinegluc<strong>on</strong>ate (CHG) <strong>mouth</strong>rinse(Peridex ® ) and essential oils (EO)<strong>mouth</strong>rinse (Listerine ® ). Because <str<strong>on</strong>g>of</str<strong>on</strong>g> arecent change in the ADA Seal Program,Peridex ® and its generic equivalentsas prescripti<strong>on</strong> products nol<strong>on</strong>ger carry the ADA Seal. However,no CPC formulati<strong>on</strong> has yet to obtainthe ADA Seal. (See also page 32 formore informati<strong>on</strong> <strong>on</strong> the ADA SealProgram.)The FDA’s <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Plaque Subcommittee<str<strong>on</strong>g>of</str<strong>on</strong>g> the N<strong>on</strong>prescripti<strong>on</strong>Drugs Advisory Committee has classified2 OTC <strong>mouth</strong>rinse ingredientsas both safe and effective and notKEY POINT:The ADA and FDA have rigorous approval processesThe ADA grants its Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance to <strong>mouth</strong><strong>rinses</strong> that havedocumented safety and efficacy through at least 2 l<strong>on</strong>gitudinal, c<strong>on</strong>trolledclinical trials. The FDA evaluates OTC ingredients making therapeuticclaims. It has adopted key elements for gingivitis assessment from theADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance criteria and assigns categories (I, II, or III)based <strong>on</strong> level <str<strong>on</strong>g>of</str<strong>on</strong>g> safety and efficacy. For certain prescripti<strong>on</strong><strong>mouth</strong><strong>rinses</strong>, the FDA evaluates safety and efficacy via the New DrugApplicati<strong>on</strong> (NDA) process.14 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Table I. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG and EO <strong>on</strong> Normal Oral FloraMouthrinse Study Descripti<strong>on</strong> Outcome References0.12% Several studies <str<strong>on</strong>g>of</str<strong>on</strong>g> 6 m<strong>on</strong>ths’ durati<strong>on</strong> Routine use <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG and EO did 8, 9,12Chlorhexidine or l<strong>on</strong>ger; dental plaque harvested at not cause adverse shifts in plaquegluc<strong>on</strong>ate (CGH) baseline, midpoint, and end. Minimum ecology, emergence <str<strong>on</strong>g>of</str<strong>on</strong>g> opportunisticand essential inhibitory c<strong>on</strong>centrati<strong>on</strong> <strong>microbial</strong> pathogens, or development <str<strong>on</strong>g>of</str<strong>on</strong>g>oils (EO) samples taken resistant <strong>microbial</strong> strains0.12% CHGand EO Candida species (C albicans, Both agents effective against test 13C dubliniensis, C krusei, C glabrata, fungal species at commerciallyC tropicalis) grown in vitro and treated available c<strong>on</strong>centrati<strong>on</strong>s withwith 0.12% CHG or EOcomparable inhibiti<strong>on</strong> betweenCHG and EOEO Randomized, crossover study with 29 Reducti<strong>on</strong> in S mutans: Recover- 14adults to determine whether regular able S mutans counts from the<strong>anti</strong><strong>microbial</strong> rinse use had theparticipants’ interproximal spacespotential for a selective increase <str<strong>on</strong>g>of</str<strong>on</strong>g> reduced by 75.4% with EO comparedStreptococcus mutans or an overgrowth with c<strong>on</strong>trol. Total streptococci in inter<str<strong>on</strong>g>of</str<strong>on</strong>g>fungal species. Participants rinsed proximal plaque declined by 69.9%.with EO or placebo for 14 daysEO activity 37.1% greater againstS mutans than against other streptococci.No increase in risk <str<strong>on</strong>g>of</str<strong>on</strong>g> cariesEO In vivo investigati<strong>on</strong>s in pers<strong>on</strong>s with Rinsing with EO twice daily was as 15,16denture stomatitis caused by an effective as nystatin oral suspensi<strong>on</strong>overgrowth <str<strong>on</strong>g>of</str<strong>on</strong>g> C albicans and other in reducing clinical palatal inflammati<strong>on</strong>fungal species in maxillary prostheses and candidiasismisbranded (Category I): cetylpyridiniumchloride (CPC; examples <str<strong>on</strong>g>of</str<strong>on</strong>g>products include Colgate Viadent ®and Crest ® Pro-Health Rinse) andEO. 6,7 CHG was reviewed and foundto be safe and effective by the FDAby means <str<strong>on</strong>g>of</str<strong>on</strong>g> an NDA and is availablein the United States <strong>on</strong>ly by prescripti<strong>on</strong>.Although many commercial <strong>mouth</strong>rinsemanufacturers claim <strong>anti</strong>plaqueand <strong>anti</strong>gingivitis properties, most lackthe efficacy data required to earn theADA Seal. Stannous fluoride hasreceived Category I recommendati<strong>on</strong>by the FDA’s advisory committee, andtriclosan has received NDA approvalby the FDA. However, these agents arenot found in <strong>mouth</strong>rinse formulati<strong>on</strong>sin the United States. This article discussesthe safety and efficacy data <str<strong>on</strong>g>of</str<strong>on</strong>g><strong>mouth</strong><strong>rinses</strong> that have been approvedby the FDA, recommended as CategoryI by the advisory committee, orawarded the ADA Seal.Anti<strong>microbial</strong>Mouthrinse SafetyTwo essential criteria for any productare safety and efficacy (see also pages 19to 22, Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> Mouth<strong>rinses</strong>). Themost effective product would be uselessif it were not safe; c<strong>on</strong>versely, thesafest product would be inc<strong>on</strong>sequentialif it did not work. Issues related tosafety in <strong>mouth</strong><strong>rinses</strong> include the following:• Are there any adverse effects <strong>on</strong>the oral <strong>microbial</strong> flora?• Are there any oral s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissueaberrati<strong>on</strong>s?• Does routine use adversely affectdental restorative materials?• Are there any c<strong>on</strong>traindicati<strong>on</strong>sfor the use <str<strong>on</strong>g>of</str<strong>on</strong>g> these products?Each <str<strong>on</strong>g>of</str<strong>on</strong>g> these c<strong>on</strong>cerns merits carefulc<strong>on</strong>siderati<strong>on</strong>.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 15
Evidence c<strong>on</strong>firms that daily, l<strong>on</strong>g-term use<str<strong>on</strong>g>of</str<strong>on</strong>g> CHG or EO does not adversely affectoral <strong>microbial</strong> flora, including no <strong>microbial</strong>overgrowth, opportunistic infecti<strong>on</strong>, ordevelopment <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong> resistance.Do Mouth<strong>rinses</strong> Have AdverseEffects <strong>on</strong> Oral Microbiota?Some dental pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als may fearthat <strong>anti</strong>septic <strong>mouth</strong><strong>rinses</strong> pose a riskin killing or inhibiting normal flora withsubsequent repopulati<strong>on</strong> with opportunisticand/or more pathogenic orresistant organisms. The <strong>microbial</strong> shiftwould manifest as an overgrowth <str<strong>on</strong>g>of</str<strong>on</strong>g>opportunistic organisms, such as Candida.Fortunately, studies document noadverse effects <strong>on</strong> supragingival dentalplaque micr<str<strong>on</strong>g>of</str<strong>on</strong>g>lora after 6 m<strong>on</strong>ths <str<strong>on</strong>g>of</str<strong>on</strong>g>c<strong>on</strong>tinued use with either CHG or EO. 8-12Table I describes the findings <str<strong>on</strong>g>of</str<strong>on</strong>g> severalstudies <str<strong>on</strong>g>of</str<strong>on</strong>g> the impact <str<strong>on</strong>g>of</str<strong>on</strong>g> EO andCHG <strong>on</strong> normal oral flora. Evidencec<strong>on</strong>firms that daily, l<strong>on</strong>g-term use (6m<strong>on</strong>ths or l<strong>on</strong>ger) <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG or EO doesnot adversely affect oral <strong>microbial</strong> flora,including no <strong>microbial</strong> overgrowth,opportunistic infecti<strong>on</strong>, or development<str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong> resistance.Do Mouth<strong>rinses</strong> Cause OralMucosal or Other S<str<strong>on</strong>g>of</str<strong>on</strong>g>t TissueAberrati<strong>on</strong>s?C<strong>on</strong>cerns about potential adverseeffects <strong>on</strong> oral mucosa and other s<str<strong>on</strong>g>of</str<strong>on</strong>g>ttissue include the following:KEY POINT:No link between ACMs and OPC• Does alcohol cause adverseeffects such as an increased risk<str<strong>on</strong>g>of</str<strong>on</strong>g> oral and pharyngeal cancer(OPC)?• Are the active ingredients foundin CHG, CPC, and EO safe forl<strong>on</strong>g-term use <strong>on</strong> the oral mucosa?• Do <strong>mouth</strong><strong>rinses</strong> affect salivaryflow?• Are there adverse effects <strong>on</strong> tasteor tooth deposits?Several studies have addressedthese issues and are discussed below.Does alcohol cause adverseeffects such as an increased risk <str<strong>on</strong>g>of</str<strong>on</strong>g>OPC? Many <strong>mouth</strong><strong>rinses</strong> c<strong>on</strong>tainpharmaceutical-grade alcohol to solubilizeactive ingredients, make thembiologically active, or dissolve flavoringagents. Typical alcohol levelsin <strong>mouth</strong><strong>rinses</strong> include the following:• CHG: generally 12.6% alcohol• CPC: 6% to 18% alcohol (traditi<strong>on</strong>al)and alcohol free, withhigh-bioavailability CPC, 0.07% 17• EO: 26.9% alcohol (original“gold” product) and 21.6% alcohol(flavored products)According to the FDA, Nati<strong>on</strong>al Cancer Institute, and ADA, there is noevidence <str<strong>on</strong>g>of</str<strong>on</strong>g> a causal relati<strong>on</strong>ship between ACMs and OPC. 6,28 Most<strong>mouth</strong><strong>rinses</strong> accepted by the ADA as safe and effective c<strong>on</strong>tain alcohol.The ADA Seal documents a product’s safety and efficacy, and the ADArecommends that patients c<strong>on</strong>tinue to use <strong>anti</strong>septic <strong>mouth</strong><strong>rinses</strong> asadvised by their dental hygienist and dentist. 28,34Oral care pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als may be reluctantto recommend an alcohol-c<strong>on</strong>taining<strong>mouth</strong>rinse (ACM) because<str<strong>on</strong>g>of</str<strong>on</strong>g> perceived risk for developingOPC. It is well known that tobaccousage and excessive alcoholic beveragec<strong>on</strong>sumpti<strong>on</strong> cause a subst<strong>anti</strong>alporti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the OPC. 18-20 Sincemost <strong>mouth</strong><strong>rinses</strong> c<strong>on</strong>tain alcohol, doACMs increase cancer risk as well?A number <str<strong>on</strong>g>of</str<strong>on</strong>g> studies have examineda cause-effect relati<strong>on</strong>ship betweenACMs and OPC with varyingresults. 19,21-27 A critical review <str<strong>on</strong>g>of</str<strong>on</strong>g>investigati<strong>on</strong>s that suggested a causeeffectrelati<strong>on</strong>ship revealed a number<str<strong>on</strong>g>of</str<strong>on</strong>g> deficiencies and study designflaws that necessitate rethinking theACM-cancer link 28,29 :• Lack <str<strong>on</strong>g>of</str<strong>on</strong>g> a dose-resp<strong>on</strong>se based <strong>on</strong>frequency and/or durati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>mouth</strong>washuse• Inc<strong>on</strong>sistent findings am<strong>on</strong>g studies• Lack <str<strong>on</strong>g>of</str<strong>on</strong>g> a scientific or biologicalbasis to explain inc<strong>on</strong>sistent findingsbetween males and females• Absence <str<strong>on</strong>g>of</str<strong>on</strong>g> correcti<strong>on</strong> for alcoholicbeverage ingesti<strong>on</strong> and tobacco use• Inclusi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> pharyngeal cancer,an improper classificati<strong>on</strong> as <strong>mouth</strong><strong>rinses</strong><strong>on</strong>ly c<strong>on</strong>tact the oral cavity• Inclusi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> other head and neckcarcinomas, lymphomas, and sarcomasas oral cancer, an improperclassificati<strong>on</strong> as <strong>mouth</strong><strong>rinses</strong> <strong>on</strong>lyc<strong>on</strong>tact the oral cavityA widely referenced study by theNati<strong>on</strong>al Cancer Institute err<strong>on</strong>eouslyc<strong>on</strong>cluded that OPC risks were elevated60% am<strong>on</strong>g female and 40%am<strong>on</strong>g male users <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>mouth</strong>wash(with >25% alcohol). 27 This epidemiologicretrospective investigati<strong>on</strong>c<strong>on</strong>sisted <str<strong>on</strong>g>of</str<strong>on</strong>g> interviews with 866patients with OPC, diagnosed January1984 through March 1985, and1249 c<strong>on</strong>trols from the general populati<strong>on</strong>without OPC sampled from4 areas <str<strong>on</strong>g>of</str<strong>on</strong>g> the United States. Reanalysis<str<strong>on</strong>g>of</str<strong>on</strong>g> this report by independentreviewers c<strong>on</strong>cluded that manypatients in the OPC group (6.6% <str<strong>on</strong>g>of</str<strong>on</strong>g>men and 12.6% <str<strong>on</strong>g>of</str<strong>on</strong>g> women) hadtumors <str<strong>on</strong>g>of</str<strong>on</strong>g> n<strong>on</strong>mucosal histology thatcould not have been c<strong>on</strong>tacted by an16 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Table II. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> EO <strong>on</strong> Salivary FlowStudy Descripti<strong>on</strong> Outcome ReferencesEffect <str<strong>on</strong>g>of</str<strong>on</strong>g> EO versus placebo Under exaggerated c<strong>on</strong>diti<strong>on</strong>s 54<strong>on</strong> the salivary flow rate and (3 <strong>rinses</strong>/day instead <str<strong>on</strong>g>of</str<strong>on</strong>g> theoral mucosa <str<strong>on</strong>g>of</str<strong>on</strong>g> 19 volunteers recommended 2), no lesi<strong>on</strong>swith documented xerostomia attributable to EO observedwho used 3 <strong>rinses</strong> daily for in the majority <str<strong>on</strong>g>of</str<strong>on</strong>g> patients.14 days followed by a cross- No statistically significantover after a 7-day washout differences detected betweenperiod. Pre- and postrinse pre- and postrinse salivarysalivary flow rates were flow rates for either the EOmeasured and oral s<str<strong>on</strong>g>of</str<strong>on</strong>g>t or c<strong>on</strong>trol grouptissues examined forevidence <str<strong>on</strong>g>of</str<strong>on</strong>g> irritati<strong>on</strong> andinflammati<strong>on</strong>Effect <strong>on</strong> salivary flow or No significant effect <strong>on</strong> 55symptoms <str<strong>on</strong>g>of</str<strong>on</strong>g> dry <strong>mouth</strong> salivary flow or dry <strong>mouth</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> an EO <strong>mouth</strong>rinse and between the 2 groupsa n<strong>on</strong>–alcohol-c<strong>on</strong>taining<strong>mouth</strong>rinseACM. Reanalysis <str<strong>on</strong>g>of</str<strong>on</strong>g> the data showedno relati<strong>on</strong>ship between ACMs andOPC. 6,30,31 Additi<strong>on</strong>al investigatorsc<strong>on</strong>tinue to report that there is no evidencethat ACM use increases OPCrisk. 28,32,33Data comparis<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> topical alcoholexposure <str<strong>on</strong>g>of</str<strong>on</strong>g> the oral mucosa fromACMs and alcoholic beverage c<strong>on</strong>sumpti<strong>on</strong>may be invalid. Two or even3 topical administrati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> a 25%ACM, each lasting 30 sec<strong>on</strong>ds, seemunlikely to produce the same effect asl<strong>on</strong>g-term, habitual alcoholic beveragec<strong>on</strong>sumpti<strong>on</strong>. Pharmaceuticalalcohol is not a carcinogen. 6,28 However,chemicals and additives foundin alcoholic beverages can cause cancer;for example, urethane, a knowncarcinogen, is comm<strong>on</strong>ly found inalcoholic beverages. 6,19,28 Commercial<strong>mouth</strong><strong>rinses</strong> c<strong>on</strong>tain pharmaceuticalgradedenatured alcohol (pureethanol), which is free from c<strong>on</strong>taminatingcarcinogens.Taking the following precauti<strong>on</strong>sshould limit any potential problemswith ACMs:• Advise patients to c<strong>on</strong>sult withtheir abuse sp<strong>on</strong>sor (counselor)before using an ACM.• EO is indicated for use in individualsover the age <str<strong>on</strong>g>of</str<strong>on</strong>g> 12 years.The effectiveness and safety <str<strong>on</strong>g>of</str<strong>on</strong>g>CHG have not been establishedin individuals under 18 years. 35,36• Use <str<strong>on</strong>g>of</str<strong>on</strong>g> an ACM in pers<strong>on</strong>s takingdisulfiram (Antabuse ® ) andmetr<strong>on</strong>idazole (Flagyl ® ) is c<strong>on</strong>traindicated,because in combinati<strong>on</strong>they may induce nausea,vomiting, and other unpleasantside effects. 37,38Do the active ingredients <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG,CPC, and EO adversely affect theoral mucosa? Evidence supports thatl<strong>on</strong>g-term use <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG, CPC, or EOdoes not c<strong>on</strong>tribute to s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissuelesi<strong>on</strong>s or mucosal aberrati<strong>on</strong>s. L<strong>on</strong>gtermclinical trials (at least 6 m<strong>on</strong>ths’durati<strong>on</strong>) produced subst<strong>anti</strong>al evidencedocumenting the safety <str<strong>on</strong>g>of</str<strong>on</strong>g> theactive ingredients <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG, CPC, andEO <strong>mouth</strong><strong>rinses</strong> <strong>on</strong> the oral mucosaand period<strong>on</strong>tium. 39-52 Complete orals<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissue examinati<strong>on</strong>s were performedat each data collecti<strong>on</strong> period(baseline, 3 m<strong>on</strong>ths, and 6 m<strong>on</strong>ths) inthese studies. Findings revealed nodifferences in the incidence or severity<str<strong>on</strong>g>of</str<strong>on</strong>g> adverse events between theCHG, CPC, or EO groups and c<strong>on</strong>trol/placebogroups. With EO, usersreport an initial tingling/burning sensati<strong>on</strong>that lessens rapidly with timeand is c<strong>on</strong>siderably reduced by theadditi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> flavoring such as citrus. 29,42A burning sensati<strong>on</strong> and occasi<strong>on</strong>almild desquamati<strong>on</strong> have also beenreported with CPC use. 53Do <strong>mouth</strong><strong>rinses</strong> affect salivaryflow? Xerostomia is a comm<strong>on</strong> sideeffect <str<strong>on</strong>g>of</str<strong>on</strong>g> many systemic diseases,radiati<strong>on</strong>/chemotherapy, and numerousOTC and prescripti<strong>on</strong> medicati<strong>on</strong>s.A misc<strong>on</strong>cepti<strong>on</strong> is that the use<str<strong>on</strong>g>of</str<strong>on</strong>g> an ACM desiccates the oralmucosa, leading to xerostomia. However,studies have shown that rinsingwith an EO <strong>mouth</strong>rinse does notinduce mucosal drying or aberrati<strong>on</strong>.54,55 Table II summarizes thesestudy findings.Are there adverse effects <strong>on</strong> tasteand tooth deposits? Some patientsmay experience a bitter taste with EOuse. 56 Taste alterati<strong>on</strong>, as well asA misc<strong>on</strong>cepti<strong>on</strong> is that the use <str<strong>on</strong>g>of</str<strong>on</strong>g> anACM desiccates the oral mucosa, leading toxerostomia. However, studies have shownthat rinsing with an EO <strong>mouth</strong>rinse does notinduce mucosal drying or aberrati<strong>on</strong>.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 17
Table III. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> Anti<strong>microbial</strong> Mouth<strong>rinses</strong> <strong>on</strong> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> MaterialsMouthrinse Study Descripti<strong>on</strong> Outcome ReferencesSeven <strong>mouth</strong><strong>rinses</strong> In vitro study <str<strong>on</strong>g>of</str<strong>on</strong>g> resin specimens placed No statistical difference 61(5 alcohol-c<strong>on</strong>taining in 1 <str<strong>on</strong>g>of</str<strong>on</strong>g> 7 <strong>mouth</strong><strong>rinses</strong> and vibrated for am<strong>on</strong>g the tested<strong>mouth</strong><strong>rinses</strong> [ACMs], 30 sec<strong>on</strong>ds or 1 minute twice daily (to soluti<strong>on</strong>s. ACMs caused1 alcohol free, simulate actual use exposure times) no increased reducti<strong>on</strong> inand 1 plain water) for 180 days composite resin hardnessEssential oils In vitro study measured effect <str<strong>on</strong>g>of</str<strong>on</strong>g> EO No differences in SBS 62(EO) <strong>on</strong> resin b<strong>on</strong>d strength <strong>on</strong> human found between the EOteeth embedded in dental st<strong>on</strong>e.and c<strong>on</strong>trol groups at allTooth surfaces etched and rinsed for diluti<strong>on</strong>s. EO had no30 sec<strong>on</strong>ds with distilled water or effect <strong>on</strong> resin b<strong>on</strong>dvarious EO diluti<strong>on</strong>s. Each tooth was strengththen dried, a film <str<strong>on</strong>g>of</str<strong>on</strong>g> adhesive resinapplied followed by composite resin,and shear b<strong>on</strong>d strength (SBS) recordedEO Direct effect <str<strong>on</strong>g>of</str<strong>on</strong>g> EO use <strong>on</strong> dental No significant differences 63materials. Specimens <str<strong>on</strong>g>of</str<strong>on</strong>g> amalgam, between the EO andglass i<strong>on</strong>omer, and composite subjected c<strong>on</strong>trol groups detectedto EO or distilled water for a c<strong>on</strong>tinuous in vitro or in vivo. EO use10-day period. For each material, com- had no adverse effect <strong>on</strong>pressive strength and water fluidrestorative materialsabsorpti<strong>on</strong> were compared; surface testedporosity was evaluated with scanningelectr<strong>on</strong> micrographs (SEM). Also, 10subjects wore appliances with implantedstudy materials and rinsed twice dailyfor 30 sec<strong>on</strong>ds with EO or placebo.After 10 days, dental materialsexamined by SEMincreased supragingival calculus formati<strong>on</strong>and brown staining <str<strong>on</strong>g>of</str<strong>on</strong>g> theteeth and t<strong>on</strong>gue, is associated withuse <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG and CPC. 42,46,56-60 CHGstains teeth, esthetic restorati<strong>on</strong>s, andimplant abutments, and this stainingcan be problematic in a society thatdesires cosmetic dentistry and whiterand brighter teeth. 36,56KEY POINT:CHG, CPC, and EO cause no serious adverse effects in agenerally healthy populati<strong>on</strong> when used according todirecti<strong>on</strong>sThis includes effects <strong>on</strong> salivary flow, taste, tooth deposits, and dentalrestorati<strong>on</strong>s. Some users may experience minor taste alterati<strong>on</strong>, staining,and supragingival calculus formati<strong>on</strong> with some CHG and CPCformulati<strong>on</strong>s.Does Routine Use <str<strong>on</strong>g>of</str<strong>on</strong>g> Mouth<strong>rinses</strong>Adversely Affect <str<strong>on</strong>g>Dental</str<strong>on</strong>g>Restorative Materials?A number <str<strong>on</strong>g>of</str<strong>on</strong>g> studies have addressedthe c<strong>on</strong>cern raised about theeffect <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong><strong>on</strong> dental materials. Other than thepotential for staining with CHG andCPC, there are no documentedadverse effects <strong>on</strong> dental materials.Table III summarizes the findings <str<strong>on</strong>g>of</str<strong>on</strong>g>these studies.18 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> Mouth<strong>rinses</strong>How Anti<strong>microbial</strong> Mouth<strong>rinses</strong>WorkAntiseptics are chemical agentsused to eliminate oral microorganismsin a variety <str<strong>on</strong>g>of</str<strong>on</strong>g> ways:Different <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong> havedem<strong>on</strong>strated efficacy against bacteria, fungi,viruses, and spores. Some products produce awide spectrum <str<strong>on</strong>g>of</str<strong>on</strong>g> activity, while others areeffective against selected microorganisms <strong>on</strong>ly.• By producing cell death• By inhibiting <strong>microbial</strong> reproducti<strong>on</strong>• By inhibiting cellular metabolismMost <strong>anti</strong>septic agents are bactericidal,although some are bacteriostatic.The effectiveness <str<strong>on</strong>g>of</str<strong>on</strong>g> these agentsvaries widely and is dependent up<strong>on</strong>product formulati<strong>on</strong>, c<strong>on</strong>centrati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>the active agent, dose, subst<strong>anti</strong>vity,compliance, and interacti<strong>on</strong>s with otherchemicals present in the oral cavity atthe time <str<strong>on</strong>g>of</str<strong>on</strong>g> use. Different <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> have dem<strong>on</strong>stratedefficacy against bacteria, fungi, viruses,and spores. Some products produce awide spectrum <str<strong>on</strong>g>of</str<strong>on</strong>g> activity, while othersare effective against selected microorganisms<strong>on</strong>ly. 56 Notably, most studies,including l<strong>on</strong>gitudinal trials, testing theefficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG used the commercialproduct Peridex ® , and Listerine ® wasthe EO commercial product used forall studies cited in this paper. CPCcommercial preparati<strong>on</strong>s used inresearch studies vary by product c<strong>on</strong>centrati<strong>on</strong>and brand.Mechanism <str<strong>on</strong>g>of</str<strong>on</strong>g> acti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG.CHG (0.12%) is a bactericidal bisbiguanide<strong>anti</strong>septic, with dem<strong>on</strong>stratedefficacy against the followingorganisms:• A wide range <str<strong>on</strong>g>of</str<strong>on</strong>g> gram-positiveand gram-negative organisms 64• Aerobes and anaerobes, many <str<strong>on</strong>g>of</str<strong>on</strong>g>which are associated with plaqueand gingivitis, including Fusobacteriumand Prevotella intermedia65• Herpes simplex virus 1 and 2,human immunodeficiency virus1, cytomegalovirus, influenza A,parainfluenza, and hepatitisB. 12,66,67 CHG is not approved forthe preventi<strong>on</strong> and treatment <str<strong>on</strong>g>of</str<strong>on</strong>g>viral infecti<strong>on</strong>s• Seven species <str<strong>on</strong>g>of</str<strong>on</strong>g> Candida andother yeasts 13,68,69 (<str<strong>on</strong>g>of</str<strong>on</strong>g>ten used al<strong>on</strong>eor in combinati<strong>on</strong> with other <strong>anti</strong>fungalmedicati<strong>on</strong>s to reduceopportunistic infecti<strong>on</strong>s in at-riskpopulati<strong>on</strong>s, such as those undergoingtreatment for leukemia orb<strong>on</strong>e marrow transplantati<strong>on</strong> 70,71 )Exposure to CHG causes rupturing<str<strong>on</strong>g>of</str<strong>on</strong>g> the bacterial cell membrane,which allows for leakage <str<strong>on</strong>g>of</str<strong>on</strong>g> the cytoplasmicc<strong>on</strong>tents, resulting in celldeath. 72,73 CHG binds to salivarymucins, reducing pellicle formati<strong>on</strong>and inhibiting col<strong>on</strong>izati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> plaquebacteria. 64,74 It also binds to bacteria,which inhibits their adsorpti<strong>on</strong> <strong>on</strong>tothe teeth. 64 CHG has been shown topenetrate the dental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm,which enables CHG to access andkill pathogens embedded within thebi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. 72CHG binds tightly to tooth structure,dental plaque, and oral s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissues.It is released slowly into the<strong>mouth</strong>, which allows <strong>anti</strong><strong>microbial</strong>effects to be sustained for up to 12hours, thus its high degree <str<strong>on</strong>g>of</str<strong>on</strong>g> subst<strong>anti</strong>vity.64,75 A 30-minute interval isoptimal between toothbrushing andrinsing with CHG to avoid an interacti<strong>on</strong>between the positively chargeddetergents found in dentifrices (eg,sodium lauryl sulfate) and thecati<strong>on</strong>ic CHG rinse. This interacti<strong>on</strong>,and possible inactivati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG,can also occur with the ani<strong>on</strong>ic fluoridei<strong>on</strong> found in stannous fluorideand in some toothpastes and<strong>mouth</strong><strong>rinses</strong>. 73,76Mechanism <str<strong>on</strong>g>of</str<strong>on</strong>g> acti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> CPC.CPC, a quaternary amm<strong>on</strong>ium compound,dem<strong>on</strong>strates bactericidalactivity. Its mechanism <str<strong>on</strong>g>of</str<strong>on</strong>g> acti<strong>on</strong> issimilar to CHG in that it ruptures thebacterial cell wall membrane, resultingin leakage <str<strong>on</strong>g>of</str<strong>on</strong>g> the intracellular c<strong>on</strong>tentsand eventual cell death. CPC isalso thought to alter bacterial metab-73, 77olism and inhibit cell growth.CPC binds to tooth structure anddental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm; however, thedegree <str<strong>on</strong>g>of</str<strong>on</strong>g> binding is not as str<strong>on</strong>g aswith CHG. Further, CPC is rapidlyreleased from binding sites, whichexplains why it is generally less efficaciousthan CHG. 73 Like CHG, thiscati<strong>on</strong>ic rinse may adversely interactwith other charged i<strong>on</strong>s found in dentifricesand <strong>mouth</strong><strong>rinses</strong>, possibly limitingits biological activity.Published data regarding the efficacy<str<strong>on</strong>g>of</str<strong>on</strong>g> CPC-c<strong>on</strong>taining <strong>mouth</strong><strong>rinses</strong>are limited. In the United States, CPCis available in 2 c<strong>on</strong>centrati<strong>on</strong>s:0.05% found in cosmetic <strong>mouth</strong><strong>rinses</strong>(Cepacol ® and Scope ® ) and0.07% found in therapeutic <strong>mouth</strong><strong>rinses</strong>(BreathRx ® and Crest ® Pro-Health Rinse). It has been suggestedthat the unique vehicle found in Crest ®Pro-Health Rinse is purported toincrease the product’s oral bioavailabilitywhen compared with otherCPC-c<strong>on</strong>taining <strong>mouth</strong><strong>rinses</strong>. 78In vitro studies have documentedthat CPC can be effective against thefollowing organisms:• Actinomyces viscosus, Porphyrom<strong>on</strong>asgingivalis, Campylobacterrectus, Streptococcus sanguis,Eikenella corrodens, Salm<strong>on</strong>ellatyphimurium, Fusobacteriumnucleatum, Haemophilus actinomycetemcomitans,Lactobacilluscasei, and P intermedia 78• Several species <str<strong>on</strong>g>of</str<strong>on</strong>g> Candida 68,69,79-81CPC, like CHG, has been suggestedas a possible agent for the preventi<strong>on</strong>Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 19
and treatment <str<strong>on</strong>g>of</str<strong>on</strong>g> fungal infecti<strong>on</strong>s.However, CPC <strong>mouth</strong><strong>rinses</strong> mayadversely affect systemic azole drugtreatment <str<strong>on</strong>g>of</str<strong>on</strong>g> oropharyngeal candidiasisin immunocompromised pers<strong>on</strong>s. Thisnegative outcome may be attributed toeither a cross-resistance to the azoledrugs against CPC-resistant organismsor drug antag<strong>on</strong>ism between CPC andazole <strong>anti</strong>fungal medicati<strong>on</strong>s whenthey are used in combinati<strong>on</strong>. 82 Two <str<strong>on</strong>g>of</str<strong>on</strong>g>5 fluc<strong>on</strong>azole-resistant C albicansstrains have also exhibited reducedsusceptibility to CPC. 82Mechanism <str<strong>on</strong>g>of</str<strong>on</strong>g> acti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> EO. EO<strong>anti</strong>septic <strong>mouth</strong>rinse is a bactericidalcombinati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> phenolic essentialoils, including eucalyptol, menthol,methyl salicylate, and thymol.Phenolic compounds exert their<strong>anti</strong><strong>microbial</strong> effects by the followingmechanisms 77, 83-87 :• Cause protein denaturati<strong>on</strong>• Alter the cell membrane, resultingin leakage <str<strong>on</strong>g>of</str<strong>on</strong>g> the intracellular c<strong>on</strong>tentsand eventual cell death• Alter bacterial enzyme activity• Exhibit <strong>anti</strong>-inflammatory propertiesby inhibiting prostaglandinsynthetase, an enzymeinvolved in the formati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>prostaglandins, which are primaryinflammatory mediators.Note that the <strong>anti</strong>-inflammatoryeffect <str<strong>on</strong>g>of</str<strong>on</strong>g> phenolic compoundsoccurs at c<strong>on</strong>centrati<strong>on</strong>s lowerthan those needed for <strong>anti</strong>bacterialactivity• Cause perforati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the cellmembrane and rapid efflux <str<strong>on</strong>g>of</str<strong>on</strong>g>intracellular c<strong>on</strong>tents (especiallythymol)• Alter neutrophil functi<strong>on</strong> by suppressingthe formati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> andscavenging existing free radicalsgenerated in neutrophils and byaltering neutrophil chemotaxis(especially thymol)A 30-sec<strong>on</strong>d exposure time to EOproduces morphologic cell surfacealterati<strong>on</strong>s in a variety <str<strong>on</strong>g>of</str<strong>on</strong>g> oralpathogens that suggest the loss <str<strong>on</strong>g>of</str<strong>on</strong>g> cellmembrane integrity. 88 Cell surfacechanges may also alter bacterial coaggregati<strong>on</strong>and recol<strong>on</strong>izati<strong>on</strong> thatcould potentially affect the growthand metabolism <str<strong>on</strong>g>of</str<strong>on</strong>g> these organisms.Microscopic evidence <str<strong>on</strong>g>of</str<strong>on</strong>g> cell surfaceroughening was obtained for the followingmicroorganisms:• C albicans• F nucleatum• A viscosus• Actinobacillus actinomycetemcomitans• S sanguisCell surface changes that resultfrom a short exposure time to EOmay adversely affect bacterial andfungal survival. 88 Exposure to levels<str<strong>on</strong>g>of</str<strong>on</strong>g> EO sublethal to microorganismsalso reduces bacterial coaggregati<strong>on</strong>with gram-positive pi<strong>on</strong>eer species,an essential step in plaque maturati<strong>on</strong>and the development <str<strong>on</strong>g>of</str<strong>on</strong>g> thecomplex pathogenic flora found ingingival disease. Decreased bacterialcoaggregati<strong>on</strong> reduces the rate <str<strong>on</strong>g>of</str<strong>on</strong>g>plaque maturati<strong>on</strong>, which in turnmay result in a decreased plaquemass, as is observed clinically withEO use. 89 EO also has been shownto extract endotoxins from gramnegativebacteria. 90 Endotoxins playan important role in pathogenesis;thus, reducti<strong>on</strong> in endotoxin levelshould manifest as a decrease in gingivalinflammati<strong>on</strong>.Unlike other OTC <strong>mouth</strong><strong>rinses</strong>,EO has been shown to penetrate thedental plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm and is activeagainst bacteria embedded within thebi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. 72,91-93 EO kills a wide variety<str<strong>on</strong>g>of</str<strong>on</strong>g> aerobic and anaerobic bacteriaassociated with plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm andgingivitis, including the following 94• A actinomycetemcomitans• A viscosus• S mutans• S sanguis• Bacteroides speciesEfficacy against gram-positive andgram-negative organisms occurs evenat c<strong>on</strong>centrati<strong>on</strong>s that are less than fullstrength. 94,95 A single 30-sec<strong>on</strong>d rinsereaches and exerts an <strong>anti</strong>bacterialeffect interproximally, an importantc<strong>on</strong>siderati<strong>on</strong> given that gingival diseasestarts between the teeth and thatindividuals <str<strong>on</strong>g>of</str<strong>on</strong>g>ten cannot access interproximalareas with mechanicalplaque removal techniques such astoothbrushing and flossing. Totalrecovered bacteria from proximaltooth surfaces was 43.8% lower followinga single 30-sec<strong>on</strong>d rinse <str<strong>on</strong>g>of</str<strong>on</strong>g> EOcompared with a c<strong>on</strong>trol (P=.001). 96Rinsing twice daily with EO as anadjunct to brushing for 11 daysreduced total recoverable streptococciin interproximal plaque by 69.9%(P
Table IV. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG <strong>on</strong> Supragingival Plaque and GingivitisTrial C<strong>on</strong>centrati<strong>on</strong> Plaque GingivitisLength No. <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG Decrease DecreaseInvestigator (m<strong>on</strong>ths) Subjects (%) (%) (%)Löe et al, 1976 49 24 120 0.20 45 27Lang et al, 1982 50 6 158 0.10 16.2 66.60.20 19.4 80.4Segreto et al, 1986 102 3 600 0.12 36 370.20 28 28Grossman et al, 1986 48 6 430 0.12 61 39Grossman et al, 1989 47 6 481 0.12 49 31Brightman et al, 1991 103 3 34 0.12 64.9 60.0Overholser et al, 1990 42 6 124 0.12 50.3 30.5Eat<strong>on</strong> et al, 1997 104 3 121 0.12 28 25Charles et al, 2004 46 6 108 0.12 21.6 18.2Table V. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> CPC <strong>on</strong> Supragingival Plaque and GingivitisTrial C<strong>on</strong>centrati<strong>on</strong> Plaque GingivitisLength No. <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG Decrease DecreaseInvestigator (m<strong>on</strong>ths) Subjects (%) (%) (%)Allen et al, 1998 105 6 111 0.05 28.2 24.0Mankodi et al, 2005 51 6 139 0.07 15.8 15.4Stookey et al, 2005 52 * 6 366 0.075 17 230.10 19 20* The <strong>mouth</strong>rinse formulati<strong>on</strong>s in this study were experimental.CHG. Results regarding the efficacy<str<strong>on</strong>g>of</str<strong>on</strong>g> CPC varied and were dependentup<strong>on</strong> product formulati<strong>on</strong>. 101 Efficacystudies <str<strong>on</strong>g>of</str<strong>on</strong>g> CHG, CPC, and EO aresummarized in Tables IV, V, and VI,respectively.The following observati<strong>on</strong>s can bemade from these study results:• CHG generally reduces moreplaque than either CPC or EO, apredictable outcome given itsgreater subst<strong>anti</strong>vity; the l<strong>on</strong>geran <strong>anti</strong><strong>microbial</strong> agent stays inc<strong>on</strong>tact with plaque bacteria, thegreater its effect.• CHG and EO are comparable inreducing gingivitis. 39-41,43-45,48-50,102-104• In head-to-head comparis<strong>on</strong>studies that evaluated both CHGand EO in the same participants,<strong>anti</strong>plaque effects were greaterfor CHG, but <strong>anti</strong>gingivitiseffects were similar for bothagents. 42,46,47• Both CHG and EO dem<strong>on</strong>strategreater reducti<strong>on</strong>s in supragingivalplaque and gingivitis as comparedwith CPC (see Tables IV-VI).Perhaps <strong>on</strong>e EO study best summarizesthe effectiveness <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>mouth</strong><strong>rinses</strong>as an aid to reducing supragingivalplaque and c<strong>on</strong>trolling gingivitis. In alarge, randomized, c<strong>on</strong>trolled clinicaltrial involving 237 participants, thosewho added twice-daily rinsing withEO to their homecare routine <str<strong>on</strong>g>of</str<strong>on</strong>g> regularbrushing and flossing dem<strong>on</strong>strateda 51.9% greater reducti<strong>on</strong> inplaque and a 21.0% greater reducti<strong>on</strong>Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 21
Table VI. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> EO (Listerine ® ) <strong>on</strong> Supragingival Plaque and GingivitisTrial Plaque GingivitisLength No. <str<strong>on</strong>g>of</str<strong>on</strong>g> Rinsing Decrease DecreaseInvestigator (m<strong>on</strong>ths) Subjects Supervisi<strong>on</strong> (%) (%)Lamster et al, 1983 40 6 145 Supervised 22 28Gord<strong>on</strong> et al, 1985 39 9 85 Supervised 19.5 23.9DePaola et al, 1989 41 6 107 Supervised 34 34Overholser et al, 1990 42 6 124 Supervised 36.1 35.9Charles et al, 2001 43 6 316 Unsupervised 56.1 22.9Bauroth et al, 2003 44 6 326 Unsupervised 21 12Sharma et al, 2004 45 6 237 Unsupervised 51.9 21.0Charles et al, 2004 46 6 108 Unsupervised 18.8 14.0in gingivitis, as compared with thosewho brushed and flossed <strong>on</strong>ly. 45 Thisstudy dem<strong>on</strong>strates the benefit <str<strong>on</strong>g>of</str<strong>on</strong>g>adding an EO <strong>mouth</strong>rinse to regularmechanical plaque removal andshows that <strong>mouth</strong><strong>rinses</strong> are able toreach bacteria in areas that are difficultto access and where mechanicalmethods <str<strong>on</strong>g>of</str<strong>on</strong>g>ten leave residual plaquebehind.Approved Mouth<strong>rinses</strong> Are EfficaciousThroughout the EntireMouthC<strong>on</strong>clusi<strong>on</strong>Anti<strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong> that areapproved by the FDA and carry theADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance are safe andeffective for the reducti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingivalplaque and gingivitis. Productsthat have not been evaluated in l<strong>on</strong>gtermclinical trials have no scientificevidence documenting safety or efficacyand should be used with cauti<strong>on</strong>.Anti<strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong> with establishedsafety and efficacy are animportant and effective additi<strong>on</strong> tomechanical plaque c<strong>on</strong>trol methods toestablish a healthy <strong>mouth</strong>. Mostpatients will benefit by adding anADA-Accepted <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinseto their self-care daily regimen<str<strong>on</strong>g>of</str<strong>on</strong>g> brushing and interdental cleaning.Using an <strong>anti</strong>septic <strong>mouth</strong>rinse producesan <strong>anti</strong><strong>microbial</strong> effect throughoutthe entire <strong>mouth</strong>, including areaseasily missed during toothbrushing andinterdental cleaning. Studies havedem<strong>on</strong>strated that <strong>anti</strong>septics kill bacteriain saliva and <strong>on</strong> the s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissues <str<strong>on</strong>g>of</str<strong>on</strong>g>the <strong>mouth</strong>, including the t<strong>on</strong>gue andoral mucosa, which are reservoirs <str<strong>on</strong>g>of</str<strong>on</strong>g>pathogenic bacteria that are able totransfer and col<strong>on</strong>ize <strong>on</strong>to the teeth. 98,105-108These collective research findings,with c<strong>on</strong>siderati<strong>on</strong> given to the respectiveadverse events pr<str<strong>on</strong>g>of</str<strong>on</strong>g>iles <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>septicagents, reinforce the value <str<strong>on</strong>g>of</str<strong>on</strong>g> usingCHG, CPC, and EO in additi<strong>on</strong> tomechanical plaque c<strong>on</strong>trol for l<strong>on</strong>gtermmaintenance <str<strong>on</strong>g>of</str<strong>on</strong>g> gingival health.Using an <strong>anti</strong>septic <strong>mouth</strong>rinseproduces an <strong>anti</strong><strong>microbial</strong> effectthroughout the entire <strong>mouth</strong>,including areas easily missed duringtoothbrushing and interdental cleaning.22 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
References1. Beals D, Ngo T, Feng Y, et al. Development and laboratoryevaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> a new toothbrush with a novel brushhead design. Am J Dent. 2000;13:5A-14A.2. Bader HI. Floss or die: implicati<strong>on</strong>s for dental pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als.Dent Today. 1998;17:76-82.3. Oliver RC, Brown LJ, Löe H. Period<strong>on</strong>tal diseases in theUnited States populati<strong>on</strong>. J Period<strong>on</strong>tol. 1998;69:269-278.4. Council <strong>on</strong> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Therapeutics. Guidelines for acceptance<str<strong>on</strong>g>of</str<strong>on</strong>g> chemotherapeutic products for the c<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g>supragingival dental plaque and gingivitis. J Am DentAssoc. 1986;112:529-532.5. American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> Council <strong>on</strong> Scientific Affairs.Acceptance Program Guidelines: Chemotherapeutic Productsfor C<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g> Gingivitis. Available at: http://www.ada.org/ada/seal/standards/guide_chemo_ging.pdf. PublishedJuly 1997. Accessed May 1, 2007.6. Food and Drug Administrati<strong>on</strong>. Oral health care drug productsfor over-the-counter human use; <strong>anti</strong>gingivitis/<strong>anti</strong>plaque drug products; establishment <str<strong>on</strong>g>of</str<strong>on</strong>g> a m<strong>on</strong>ograph;proposed rules. Fed Regist. May 29, 2003;68:32232-32287.7. Wu CD, Savitt ED. Evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the safety and efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g>over-the-counter oral hygiene products for the c<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g>plaque and gingivitis. Period<strong>on</strong>tol 2000. 2002;28:91-105.8. Minah GE, DePaola LG, Overholser CD, et al. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g>6 m<strong>on</strong>ths use <str<strong>on</strong>g>of</str<strong>on</strong>g> an <strong>anti</strong>septic <strong>mouth</strong>rinse <strong>on</strong> supragingivaldental plaque micr<str<strong>on</strong>g>of</str<strong>on</strong>g>lora. J Clin Period<strong>on</strong>tol.1989;16:347-352.9. Walker C, Clark W, Tyler K, et al. Evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>microbial</strong>shifts following l<strong>on</strong>g-term use <str<strong>on</strong>g>of</str<strong>on</strong>g> an oral <strong>anti</strong>septic<strong>mouth</strong>rinse [abstract]. J Dent Res. 1989;68:412. Abstract1845.10. Emils<strong>on</strong> CG, Fornell J. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g> toothbrushing withchlorhexidine gel <strong>on</strong> salivary micr<str<strong>on</strong>g>of</str<strong>on</strong>g>lora, oral hygiene, andcaries. Scand J Dent Res. 1976;84:308-319.11. Schiott CR, Briner WW, Loe H. Two year oral use <str<strong>on</strong>g>of</str<strong>on</strong>g>chlorhexidine in man. II. The effect <strong>on</strong> the salivary bacterialflora. J Period<strong>on</strong>tal Res. 1976;11:145-152.12. Briner WW, Grossman E, Buckner RY, et al. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g>chlorhexidine gluc<strong>on</strong>ate <strong>mouth</strong>rinse <strong>on</strong> plaque bacteria. JPeriod<strong>on</strong>tal Res. 1986;21(suppl):44-52.13. Meiller TF, Kelley JI, Jabra-Rizk MA, et al. In vitro studies<str<strong>on</strong>g>of</str<strong>on</strong>g> the efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong>s against fungi. Oral SurgOral Med Oral Pathol Oral Radiol Endod. 2001;91:663-670.14. Fine DH, Furgang D, Barnett ML, et al. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g> an essentialoil-c<strong>on</strong>taining <strong>anti</strong>septic <strong>mouth</strong>rinse <strong>on</strong> plaque andsalivary Streptococcus mutans levels. J Clin Period<strong>on</strong>tol.2000;27:157-161.15. DePaola LG, Minah GE, Elias SA, et al. Clinical and <strong>microbial</strong>evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> treatment regimens to reduce denturestomatitis. Int J Prosthod<strong>on</strong>t. 1990;3:369-374.16. DePaola LG, Minah GE, Leupold RL, et al. The effect <str<strong>on</strong>g>of</str<strong>on</strong>g><strong>anti</strong>septic <strong>mouth</strong><strong>rinses</strong> <strong>on</strong> oral <strong>microbial</strong> flora and denturestomatitis. Clin Prev Dent. 1986;8:3-8.17. White DJ. An alcohol-free therapeutic <strong>mouth</strong>rinse withcetylpyridinium chloride (CPC)—the latest advance in preventivecare: Crest Pro-Health Rinse. Am J Dent.2005;18:3A-8A.18. Parkin DM, Pisani P, Lopez AD, Masuyer E. At least <strong>on</strong>ein seven cases <str<strong>on</strong>g>of</str<strong>on</strong>g> cancer is caused by smoking: globalestimates for 1985. Int J Cancer. 1994;59:494-504.19. Blot WJ, McLaughlin JK, Winn DM, et al. Smoking anddrinking in relati<strong>on</strong> to oral and pharyngeal cancer. CancerRes. 1988;48:3282-3287.20. Negri E, La Vecchia C, Franceschi S, Tavani A. Attributablerisk for oral cancer in northern Italy. Cancer EpidemiolBiomarkers Prev. 1993;2:189-193.21. Garro AJ, Leiber CS. Alcohol and cancer. Annu Rev PharmacolToxicol. 1990;30:219-249.22. Weaver A, Fleming SM, Smith DB. Mouthwash use andoral cancer: carcinogen or coincidence? J Oral Surg.1979;37:250-253.23. Mashberg A, Barsa P, Grossman ML. A study <str<strong>on</strong>g>of</str<strong>on</strong>g> the relati<strong>on</strong>shipbetween <strong>mouth</strong>wash use and oral and pharyngealcancer. J Am Dent Assoc. 1985;110:731-734.24. Kabat GC, Herbert JR, Wynder EL. Risk factors for oralcancer in women. Cancer Res. 1989;49:2803-2806.25. Young TB, Ford CN, Brandenburg JH. An epidemiologicstudy <str<strong>on</strong>g>of</str<strong>on</strong>g> oral cancer in a statewide network. Am J Otolaryngol.1986;7:200-208.26. Wynder EL, Kabat G, Rosenberg S, Levenstein M. Oralcancer and <strong>mouth</strong>wash use. J Natl Cancer Inst.1983;70:255-260.27. Winn DM, Blot WJ, McLaughlin JK, et al. Mouthwash andoral c<strong>on</strong>diti<strong>on</strong>s in the risk <str<strong>on</strong>g>of</str<strong>on</strong>g> oral and pharyngeal cancer.Cancer Res. 1991;51:3044-3047.28. Ciancio SG. Alcohol in <strong>mouth</strong>rinse: lack <str<strong>on</strong>g>of</str<strong>on</strong>g> associati<strong>on</strong>with cancer. Biol Ther Dent. 1993;9:1-2.29. Silverman S, Wilder R. Anti<strong>microbial</strong> <strong>mouth</strong>rinse as part <str<strong>on</strong>g>of</str<strong>on</strong>g>a comprehensive oral care regimen: safety and compliancefactors. J Am Dent Assoc. 2006;137:22S-26S.30. Cole P et al. Alcohol-c<strong>on</strong>taining <strong>mouth</strong>wash and oropharyngealcancer: an epidemiologic prospective. Unpublishedstudy in OTC 2001;Vol 210476.31. FDC Reports. Alcohol-c<strong>on</strong>taining <strong>mouth</strong>wash c<strong>on</strong>cern“alleviated” by existing data. The Tan Sheet. June 10,1996;4(24):1-5.32. Cole P, Rodu B, Mathisen A. Alcohol-c<strong>on</strong>taining <strong>mouth</strong>washand oropharyngeal cancer: a review <str<strong>on</strong>g>of</str<strong>on</strong>g> the epidemiology.J Am Dent Assoc. 2003;134:1079-1087.33. Elmore JG, Horwitz RI. Oral cancer and <strong>mouth</strong>wash use:evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the epidemiologic evidence. OtolaryngolHead Neck Surg. 1995;113:253-261.34. American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> Council <strong>on</strong> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Therapeutics.Mouthrinse use and the risk <str<strong>on</strong>g>of</str<strong>on</strong>g> oral and pharyngealcancer (positi<strong>on</strong> statement) Sept. 29, 1991.35. Listerine ® Antiseptic [package insert]. Skillman, NJ: Johns<strong>on</strong>& Johns<strong>on</strong> Healthcare Products Divisi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> McNEIL-PPC, Inc.; 2007.36. Peridex ® (chlorhexidine gluc<strong>on</strong>ate 0.12% ) Oral Rinse[package insert]. West Palm Beach FL: 3M ESPE; 2007.37. Antabuse ® (disulfiram) [package insert]. East Hanover,NJ: Odyssey Pharmaceuticals, Inc.; 2001.38. Gage TW, Pickett FA. Mosby’s <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Drug Reference. 6thed. St Louis, MO. Mosby/Elsevier; 2003.39. Gord<strong>on</strong> JM, Lamster IB, Seiger MC. Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> Listerine<strong>anti</strong>septic in inhibiting the development <str<strong>on</strong>g>of</str<strong>on</strong>g> plaque and gingivitis.J Clin Period<strong>on</strong>tol. 1985;12:697-704.40. Lamster IB, Alfano MC, Seiger MC, et al. The effect <str<strong>on</strong>g>of</str<strong>on</strong>g> Listerine<strong>anti</strong>septic <strong>on</strong> the reducti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> existing plaque andgingivitis. Clin Prev Dent. 1983;5:12-16.41. DePaola LG, Overholser CD, Meiller TF, et al. Chemotherapeuticinhibiti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingival dental plaque and gingivitisdevelopment. J Clin Period<strong>on</strong>tol. 1989;16:311-315.42. Overholser CD, Meiller TF, DePaola LG, et al. Comparativeeffects <str<strong>on</strong>g>of</str<strong>on</strong>g> 2 chemotherapeutic <strong>mouth</strong><strong>rinses</strong> <strong>on</strong> thedevelopment <str<strong>on</strong>g>of</str<strong>on</strong>g> supragingival dental plaque and gingivitis.J Clin Period<strong>on</strong>tol. 1990;17:575-579.43. Charles CH, Sharma NC, Galustians HJ, et al. Comparativeefficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> an <strong>anti</strong>septic <strong>mouth</strong>rinse and an<strong>anti</strong>plaque/<strong>anti</strong>gingivitis dentifrice: a six-m<strong>on</strong>th clinical trial.J Am Dent Assoc. 2001;132:670-675.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 23
44. Bauroth K, Charles CH, Mankodi SM, et al. The efficacy<str<strong>on</strong>g>of</str<strong>on</strong>g> an essential oil <strong>anti</strong>septic <strong>mouth</strong>rinse vs. dental floss inc<strong>on</strong>trolling interproximal gingivitis: a comparative study. JAm Dent Assoc. 2003;134:359-365.45. Sharma N, Charles CH, Lynch MC, et al. Adjunctive benefit<str<strong>on</strong>g>of</str<strong>on</strong>g> an essential oil-c<strong>on</strong>taining <strong>mouth</strong>rinse in reducingplaque and gingivitis in patients who brush and floss regularly:a six-m<strong>on</strong>th study. J Am Dent Assoc. 2004;135:496-504.46. Charles CH, Mostler KM, Bartels LL, Mankodi SM. Comparative<strong>anti</strong>plaque and <strong>anti</strong>gingivitis effectiveness <str<strong>on</strong>g>of</str<strong>on</strong>g> achlorhexidine and an essential oil <strong>mouth</strong>rinse: 6-m<strong>on</strong>thclinical trial. J Clin Period<strong>on</strong>tol. 2004;31:878-884.47. Grossman E, Meckel AH, Issacs RL, et al. A clinical comparis<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>bacterial <strong>mouth</strong><strong>rinses</strong>: effects <str<strong>on</strong>g>of</str<strong>on</strong>g> chlorhexidine,phenolics and sanguinarine <strong>on</strong> dental plaque andgingivitis. J Period<strong>on</strong>tol. 1989;60:435-440.48. Grossman E, Reiter G, Sturzenberger OP, et al. Six-m<strong>on</strong>thstudy <str<strong>on</strong>g>of</str<strong>on</strong>g> the effects <str<strong>on</strong>g>of</str<strong>on</strong>g> a chlorhexidine <strong>mouth</strong>rinse <strong>on</strong> gingivitisin adults. J Period<strong>on</strong>tal Res. 1986;21(suppl 16):33-43.49. Löe H, Schiött CR, Glavind L, Karring G. Two years oraluse <str<strong>on</strong>g>of</str<strong>on</strong>g> chlorhexidine in man. I. General design and clinicaleffects. J Period<strong>on</strong>tal Res. 1976;11:135-144.50. Lang NP, Hotz P, Graf H, et al. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> supervisedchlorhexidine <strong>mouth</strong><strong>rinses</strong> in children. A l<strong>on</strong>gitudinal clinicaltrial. J Period<strong>on</strong>tal Res. 1982;17:101-111.51. Mankodi S, Bauroth K, Witt JJ, et al. A 6-m<strong>on</strong>th clinical trialto study the effects <str<strong>on</strong>g>of</str<strong>on</strong>g> a cetylpyridinium chloride <strong>mouth</strong>rinse<strong>on</strong> gingivitis and plaque. Am J Dent. 2005;18:9A-14A.52. Stookey GK, Beiswanger B, Mau M, et al. A 6-m<strong>on</strong>th clinicalstudy assessing the safety and efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> two cetylpyridiniumchloride <strong>mouth</strong><strong>rinses</strong>. Am J Dent. 2005;18:24A-28A.53. Ashley FP, Skinner A, Jacks<strong>on</strong> P, et al. The effect <str<strong>on</strong>g>of</str<strong>on</strong>g> a0.1% cetylpyridinium chloride <strong>mouth</strong>rinse <strong>on</strong> plaque andgingivitis in adult subjects. Br Dent J. 1984;157:191-196.54. Fischman SL, Aguirre A, Charles CH. Use <str<strong>on</strong>g>of</str<strong>on</strong>g> essential oilc<strong>on</strong>taining<strong>mouth</strong><strong>rinses</strong> by xerostomic individuals: determinati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> potential for oral mucosal irritati<strong>on</strong>. Am J Dent.2004;17:23-26.55. Kerr AR, Katz RW, Ship JA. A comparis<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the effects <str<strong>on</strong>g>of</str<strong>on</strong>g>two commercially available n<strong>on</strong>-prescripti<strong>on</strong> <strong>mouth</strong><strong>rinses</strong><strong>on</strong> salivary flow rates and xerostomia: a pilot study. QuintessenceInt. In press.56. Ciancio SG. Antiseptics and <strong>anti</strong>biotics as chemotherapeuticagents for period<strong>on</strong>titis management. CompendC<strong>on</strong>tin Educ Dent. 2000;21:59-78.57. Mandel ID. Chemotherapeutic agents for c<strong>on</strong>trolling plaqueand gingivitis. J Clin Period<strong>on</strong>tol. 1988;15:488-498.58. Kerr AR, Ship JA. Tooth discolorati<strong>on</strong>. Available at:http://www.emedicine.com/derm/topic646.htm. AccessedApril 8, 2007.59. Sheen S, Addy M. An in vitro evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the availability<str<strong>on</strong>g>of</str<strong>on</strong>g> cetylpyridinium chloride and chlorhexidine in some commerciallyavailable <strong>mouth</strong>rinse products. Br Dent J.2003;194:207-210.60. Basc<strong>on</strong>es A, Morante S, Mateos L, et al. Influence <str<strong>on</strong>g>of</str<strong>on</strong>g> additi<strong>on</strong>alactive ingredients <strong>on</strong> the effectiveness <str<strong>on</strong>g>of</str<strong>on</strong>g> n<strong>on</strong>-alcoholicchlorhexidine <strong>mouth</strong>washes: a randomized c<strong>on</strong>trolledtrial. J Period<strong>on</strong>tol. 2005;76:1469-1475.61. Norman R. Surface hardness effects <str<strong>on</strong>g>of</str<strong>on</strong>g> various<strong>mouth</strong><strong>rinses</strong> <strong>on</strong> a composite resin [abstract]. J Dent Res.1997;76:325. Abstract 2490.62. V<strong>on</strong> Fraunh<str<strong>on</strong>g>of</str<strong>on</strong>g>er JA, Kelley JJ, DePaola LG, Meiller TF. Theeffect <str<strong>on</strong>g>of</str<strong>on</strong>g> a dental unit waterline treatment soluti<strong>on</strong> <strong>on</strong> composite-dentinshear b<strong>on</strong>d strengths. J Clin Dent.2004;15:28-32.63. V<strong>on</strong> Fraunh<str<strong>on</strong>g>of</str<strong>on</strong>g>er J, Kelley JI, DePaola LG, Meiller TF. Theeffect <str<strong>on</strong>g>of</str<strong>on</strong>g> a <strong>mouth</strong>rinse c<strong>on</strong>taining essential oils <strong>on</strong> dentalrestorative materials. Gen Dent. 2006;54:403-407.64. Wolff LF. Chemotherapeutic agents in the preventi<strong>on</strong> andtreatment <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal disease. Northwest Dent.1985;64:15-24.65. De Boever EH, Loesche WJ. Assessing the c<strong>on</strong>tributi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>anaerobic micr<str<strong>on</strong>g>of</str<strong>on</strong>g>lora <str<strong>on</strong>g>of</str<strong>on</strong>g> the t<strong>on</strong>gue to oral malodor. J AmDent Assoc. 1995;126:1384-1393.66. Bernstein D, Schiff G, Echler G, et al. In vitro virucidaleffectiveness <str<strong>on</strong>g>of</str<strong>on</strong>g> a 0.12% chlorhexidine gluc<strong>on</strong>ate<strong>mouth</strong>rinse. J Dent Res. 1990;69:874-876.67. Baqui AA, Kelley JI, Jabra-Rizk MA, et al. In vitro effect <str<strong>on</strong>g>of</str<strong>on</strong>g>oral <strong>anti</strong>septics <strong>on</strong> human immunodeficiency virus-1 andherpes simplex virus type 1. J Clin Period<strong>on</strong>tol.2001;28:610-616.68. Giuliana G, Pizzo G, Milici ME, et al. In vitro <strong>anti</strong>fungalproperties <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>mouth</strong><strong>rinses</strong> c<strong>on</strong>taining <strong>anti</strong><strong>microbial</strong> agents.J Period<strong>on</strong>tol. 1997;68:729-733.69. Giuliana G, Pizzo G, Milici ME, Giangreco R. In vitro activities<str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong> agents against Candida species. OralSurg Oral Med Oral Pathol Oral Radiol Endod.1999;87:44-49.70. Shar<strong>on</strong> A, Berdicevsky I, Ben-Aryeh H, Gutman D. Theeffect <str<strong>on</strong>g>of</str<strong>on</strong>g> chlorhexidine <strong>mouth</strong> <strong>rinses</strong> <strong>on</strong> oral Candida in agroup <str<strong>on</strong>g>of</str<strong>on</strong>g> leukemic patients. Oral Surg Oral Med OralPathol. 1977;44:201-205.71. Epstein JB, Vickars L, Spinelli J, Reece D. Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g>chlorhexidine and nystatin <strong>rinses</strong> in preventi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> oralcomplicati<strong>on</strong>s in leukemia and b<strong>on</strong>e marrow transplantati<strong>on</strong>.Oral Surg Oral Med Oral Pathol. 1992;73:682-689.72. Foster JS, Pan PC, Kolenbrander PE. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong>agents <strong>on</strong> oral bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms in a saliva-c<strong>on</strong>diti<strong>on</strong>ed flowcell.Bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilms. 2004;1:5-12.73. Ciancio SG. Chemical agents: plaque c<strong>on</strong>trol, calculusreducti<strong>on</strong> and treatment <str<strong>on</strong>g>of</str<strong>on</strong>g> dentinal hypersensitivity. Period<strong>on</strong>tol2000. 1995;8:75-86.74. Fine DH. Mouth<strong>rinses</strong> as adjuncts for plaque and gingivitismanagement: a status report for the American <str<strong>on</strong>g>Journal</str<strong>on</strong>g><str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry. Am J Dent. 1988;1:259-263.75. Weeks C, Briner W, Rebitski G, et al. Immediate and prol<strong>on</strong>gedeffect <str<strong>on</strong>g>of</str<strong>on</strong>g> 0.12% chlorhexidine <strong>on</strong> salivary bacteria[abstract]. J Dent Res. 1988;67:326. Abstract 1711.76. Barkvoll P, Rølla G, Svendsen AK. Interacti<strong>on</strong> betweenchlorhexidine digluc<strong>on</strong>ate and sodium lauryl sulfate invivo. J Clin Period<strong>on</strong>tol. 1989;16:593-595.77. Scheie AA. Modes <str<strong>on</strong>g>of</str<strong>on</strong>g> acti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> currently known chemical<strong>anti</strong>plaque agents other than chlorhexidine. J Dent Res.1989;68:1609-1616.78. Witt J, Ramji N, Gibb R, et al. Antibacterial and <strong>anti</strong>plaqueeffects <str<strong>on</strong>g>of</str<strong>on</strong>g> a novel, alcohol-free oral rinse with cetylpyridiniumchloride. J C<strong>on</strong>temp Dent Pract. 2005;6:1-9.79. Meier S, Collier C, Scaletta MG, et al. An in vitro investigati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> the efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> CPC for use in toothbrush dec<strong>on</strong>taminati<strong>on</strong>.J Dent Hyg. 1996;70:161-165.80. Nakamoto K, Tamamoto M, Hamada T. In vitro effectiveness<str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>mouth</strong><strong>rinses</strong> against Candida albicans. Int JProsthod<strong>on</strong>t. 1995;8:486-489.81. Phillips BJ, Kaplan W. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g> cetylpyridinium chloride <strong>on</strong>pathogenic fungi and Nocardia asteroides in sputum. JClin Microbiol. 1976;3:272-276.82. Edlind MP, Smith WL, Edlind TD. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> cetylpyridiniumchloride resistance and treatment <strong>on</strong> fluc<strong>on</strong>azole activityversus Candida albicans. Antimicrob Agents Chemother.2005;49:843-845.83. Goods<strong>on</strong> JM. Resp<strong>on</strong>se. In: Loe H, Kleinman DV, eds.<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Plaque C<strong>on</strong>trol Measures and Oral <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Practices.Oxford, England: IRL Press; 1986:143-146.24 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
84. Walker CB. Microbiological effects <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>mouth</strong><strong>rinses</strong> c<strong>on</strong>taining<strong>anti</strong><strong>microbial</strong>s. J Clin Period<strong>on</strong>tol. 1988;15:499-505.85. Shapiro S, Meier A, Guggenheim B. The <strong>anti</strong><strong>microbial</strong>activity <str<strong>on</strong>g>of</str<strong>on</strong>g> essential oils and essential oil comp<strong>on</strong>entstowards oral bacteria. Oral Microbiol Immunol.1994;9:202-208.86. Kuehl FA Jr, Humes JL, Egar RW, et al. Role <str<strong>on</strong>g>of</str<strong>on</strong>g>prostaglandin endoperoxide PGG2 in inflammatoryprocesses. Nature. 1977;265:170-172.87. Azuma Y, Ozaza N, Ueda Y, Takagi N. Pharmacologicalstudies <strong>on</strong> the <strong>anti</strong>-inflammatory acti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> phenolic compounds.J Dent Res. 1986;65:53-56.88. Kubert D, Rubin M, Barnett ML, Vincent JW. Antiseptic<strong>mouth</strong>rinse-induced <strong>microbial</strong> cell surface alterati<strong>on</strong>s. AmJ Dent. 1993;6:277-279.89. Fine DH, Furgang D, Lieb R, et al. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> sublethalexposure to an <strong>anti</strong>septic <strong>mouth</strong>rinse <strong>on</strong> representativeplaque bacteria. J Clin Period<strong>on</strong>tol. 1996;23:444-451.90. Fine DH, Letizia J, Mandel ID. The effect <str<strong>on</strong>g>of</str<strong>on</strong>g> rinsing withListerine <strong>anti</strong>septic <strong>on</strong> the properties <str<strong>on</strong>g>of</str<strong>on</strong>g> developing dentalplaque. J Clin Period<strong>on</strong>tol. 1985;12:660-666.91. Pan P, Barnett ML, Coelho J, et al. Determinati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> thein situ bactericidal activity <str<strong>on</strong>g>of</str<strong>on</strong>g> an essential oil <strong>mouth</strong>rinseusing a vital stain method. J Clin Period<strong>on</strong>tol. 2000;27:256-261.92. Fine DH, Furgang D, Barnett ML. Comparative <strong>anti</strong><strong>microbial</strong>activities <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>septic <strong>mouth</strong><strong>rinses</strong> against isogenicplankt<strong>on</strong>ic and bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm forms <str<strong>on</strong>g>of</str<strong>on</strong>g> Actinobacillus actinomycetemcomitans.J Clin Period<strong>on</strong>tol. 2001;28:697-700.93. Ouhayoun JP. Penetrating the plaque bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm: impact <str<strong>on</strong>g>of</str<strong>on</strong>g>essential oil <strong>mouth</strong>rinse. J Clin Period<strong>on</strong>tol. 2003;30(suppl5):10-12.94. Ross NM, Charles CH, Dills SS. L<strong>on</strong>g-term effects <str<strong>on</strong>g>of</str<strong>on</strong>g> Listerine<strong>anti</strong>septic <strong>on</strong> dental plaque and gingivitis. J ClinDent. 1989;1:92-95.95. Whitaker EJ, Pham K, Feik D, et al. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g> an essentialoil-c<strong>on</strong>taining <strong>anti</strong>septic <strong>mouth</strong>rinse <strong>on</strong> inducti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> plateletaggregati<strong>on</strong> by oral bacteria in vitro. J Clin Period<strong>on</strong>tol.2000;27:370-373.96. Charles CH, Pan PC, Sturdivant L, Vincent JW. In vivo<strong>anti</strong><strong>microbial</strong> activity <str<strong>on</strong>g>of</str<strong>on</strong>g> an essential oil-c<strong>on</strong>taining<strong>mouth</strong>rinse <strong>on</strong> interproximal plaque bacteria. J Clin Dent.2000;11:94-97.97. Pitts G, Brogd<strong>on</strong> C, Hu L, et al. Mechanism <str<strong>on</strong>g>of</str<strong>on</strong>g> acti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> an <strong>anti</strong>septic,<strong>anti</strong>-odor <strong>mouth</strong>wash. J Dent Res. 1983;62:738-742.98. DePaola LG, Minah GE, Overholser CD, et al. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g> an<strong>anti</strong>septic <strong>mouth</strong>rinse <strong>on</strong> salivary microbiotia. Am J Dent.1996;9:93-95.99. Furgang K, Sinatra K, Schreiner H, et al. In vitro <strong>anti</strong><strong>microbial</strong>activity <str<strong>on</strong>g>of</str<strong>on</strong>g> an essential oil <strong>mouth</strong>rinse. J Dent Res.2002;81(special issue A). Abstract 2854.100. Dennis<strong>on</strong> DK, Meredith GM, Shillitoe EJ, Caffesse RG.The <strong>anti</strong>viral spectrum <str<strong>on</strong>g>of</str<strong>on</strong>g> Listerine <strong>anti</strong>septic. Oral SurgOral Med Oral Pathol Oral Radiol Endod. 1995;79:442-448.101. Gunsolley JC. A meta-analysis <str<strong>on</strong>g>of</str<strong>on</strong>g> six-m<strong>on</strong>th studies <str<strong>on</strong>g>of</str<strong>on</strong>g><strong>anti</strong>plaque and <strong>anti</strong>gingivitis agents. J Am Dent Assoc.2006;137:1649-1657.102. Segreto VA, Collins EM, Beiswanger BB, et al. A comparis<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>mouth</strong><strong>rinses</strong> c<strong>on</strong>taining two c<strong>on</strong>centrati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g>chlorhexidine. J Period<strong>on</strong>tal Res. 1986;21(suppl):23-32.103. Brightman LJ, Terezhalmy GT, Greenwell H, et al. Theeffects <str<strong>on</strong>g>of</str<strong>on</strong>g> a 0.12% chlorhexidine gluc<strong>on</strong>ate <strong>mouth</strong>rinse <strong>on</strong>orthod<strong>on</strong>tic patients aged 11 through 17 with establishedgingivitis. Am J Orthod Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthop. 1991;100:324-329.104. Eat<strong>on</strong> KA, Rimini FM, Zak E, et al. The effects <str<strong>on</strong>g>of</str<strong>on</strong>g> a 0.12%chlorhexidine–digluc<strong>on</strong>ate-c<strong>on</strong>taining <strong>mouth</strong>rinse versusa placebo <strong>on</strong> plaque and gingival inflammati<strong>on</strong> over a 3-m<strong>on</strong>th period. A multicentre study carried out in generaldental practices. J Clin Period<strong>on</strong>tol. 1997;24:189-197.105. Allen DR, Davies R, Bradshaw B, et al. Efficacy <str<strong>on</strong>g>of</str<strong>on</strong>g> a<strong>mouth</strong>rinse c<strong>on</strong>taining 0.05% cetylpyridinium chloride forthe c<strong>on</strong>trol <str<strong>on</strong>g>of</str<strong>on</strong>g> plaque and gingivitis: a 6-m<strong>on</strong>th clinicalstudy in adults. Compend C<strong>on</strong>tin Educ Dent. 1998;19(2suppl):20-26.106. Dahlen G. Effect <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong> <strong>on</strong> salivarymicr<str<strong>on</strong>g>of</str<strong>on</strong>g>lora in healthy subjects. Scand J Dent Res.1984;92:38-42.107. Jenkins S, Addy M, Wade W, Newcombe RG. The magnitudeand durati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the effects <str<strong>on</strong>g>of</str<strong>on</strong>g> some <strong>mouth</strong>rinseproducts <strong>on</strong> salivary bacterial counts. J Clin Period<strong>on</strong>tol.1994;21:397-401.108. Pitts G, Pianotti R, Feary TW, et al. The in vivo effects <str<strong>on</strong>g>of</str<strong>on</strong>g>an <strong>anti</strong>septic <strong>mouth</strong>wash <strong>on</strong> odor-producing microorganisms.J Dent Res. 1981;60:1891-1896.109. Fine DH, Furgang D, Sinatra K, et al. In vivo <strong>anti</strong><strong>microbial</strong>effectiveness <str<strong>on</strong>g>of</str<strong>on</strong>g> an essential oil-c<strong>on</strong>taining <strong>mouth</strong> rinse12 h after a single use and 14 days’ use. J Clin Period<strong>on</strong>tol.2005;32:335-340.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 25
Strategies for Incorporating Anti<strong>microbial</strong> Mouth<strong>rinses</strong>into Daily Oral CareJoanna Asadoorian, RDH, MScIntroducti<strong>on</strong>AbstractOverview. A cost-effective way <str<strong>on</strong>g>of</str<strong>on</strong>g> improving patient outcomes is adoptingpreventive practices known to be effective. As “fr<strong>on</strong>t-line” providers <str<strong>on</strong>g>of</str<strong>on</strong>g> dentalhealth services and informati<strong>on</strong>, dental hygienists are an important catalystfor the implementati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> evidence-based preventive practices—such as the twice-daily use <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong>—in the self-careroutines <str<strong>on</strong>g>of</str<strong>on</strong>g> patients. However, encouraging patients to adopt new behaviorscan present a challenge: providers may be uncomfortable with recommendingnew behaviors and patients may be resistant to learning newskills. As expert clinicians, educators, and counselors, dental hygienists arein an excellent positi<strong>on</strong> to help patients make changes and learn newbehaviors.Clinical Implicati<strong>on</strong>s. This article discusses practical methods for promotingchange. Targeting interventi<strong>on</strong>s to individual patient values, stage <str<strong>on</strong>g>of</str<strong>on</strong>g>readiness to change, and skill set encourages patient incorporati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> newbehaviors. Time should be allotted for supervised practice <str<strong>on</strong>g>of</str<strong>on</strong>g> new skills, andpatients should be supported in planning for effective and lasting behaviorchange. Through effective communicati<strong>on</strong>, skills teaching, and use <str<strong>on</strong>g>of</str<strong>on</strong>g> follow-up,dental hygienists can help patients adopt healthy behaviors.Key words: Anti<strong>microbial</strong> <strong>mouth</strong>rinse, compliance, dental hygiene, oralhealth, patient educati<strong>on</strong>The merits <str<strong>on</strong>g>of</str<strong>on</strong>g> oral hygiene to healthhave l<strong>on</strong>g been valued by oral healthcare providers. However, publicawareness <str<strong>on</strong>g>of</str<strong>on</strong>g> the importance <str<strong>on</strong>g>of</str<strong>on</strong>g> oralhealth and the links between oral andsystemic health and disease hasincreased in recent years, particularlysince the publicati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> Oral Health inAmerica: A Report <str<strong>on</strong>g>of</str<strong>on</strong>g> the Surge<strong>on</strong>General in 2000 and the subsequentrelease and implementati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> theNati<strong>on</strong>al Call to Acti<strong>on</strong> to PromoteOral Health, a public-private partnershipunder the leadership <str<strong>on</strong>g>of</str<strong>on</strong>g> the Office<str<strong>on</strong>g>of</str<strong>on</strong>g> the Surge<strong>on</strong> General. 1,2 <str<strong>on</strong>g>Dental</str<strong>on</strong>g>hygienists now have an importantwindow <str<strong>on</strong>g>of</str<strong>on</strong>g> opportunity to counselpatients <strong>on</strong> behaviors that promoteoral health. Health care providers,including dental hygienists, can act ascatalysts for change by teachingpatients about oral health, modelinghealth behaviors, and helping patientsadopt healthy behaviors. 3It has been noted that “the mostcost-effective opportunity to improvepatient outcomes over the next quartercentury will likely come not fromdiscovering new therapies but fromdiscovering how to deliver therapiesthat are known to be effective.” 4 Theaim <str<strong>on</strong>g>of</str<strong>on</strong>g> this article is to enable dentalhygienists to put evidence-basedinformati<strong>on</strong> about <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> into practice by effectivelycommunicating research findingswith patients and promotingincorporati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> healthy behaviorsinto their self-care regimens. Thisreview will focus <strong>on</strong> practical methodsfor promoting positive change andsuggest ways to involve patients inoptimizing their oral health. By promotingoptimal oral care, dentalhygienists can make a significant differencein the health and well-being <str<strong>on</strong>g>of</str<strong>on</strong>g>their patients.Initiating BehavioralChangeWhile encouraging patients toadopt new, healthful behaviors issomething dental hygienists frequentlydo, they may find it difficultto recommend new behaviors, such asuse <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong>. Barriersto change are varied and include:• Habit: <str<strong>on</strong>g>Dental</str<strong>on</strong>g> hygienists may recommendtraditi<strong>on</strong>al oral hygienemethods most <str<strong>on</strong>g>of</str<strong>on</strong>g>ten (such asbrushing and flossing), despiteresearch dem<strong>on</strong>strating the effectiveness<str<strong>on</strong>g>of</str<strong>on</strong>g> other oral hygiene aidsand techniques. 5• Lack <str<strong>on</strong>g>of</str<strong>on</strong>g> c<strong>on</strong>fidence 6 : <str<strong>on</strong>g>Dental</str<strong>on</strong>g>hygienists may lack the c<strong>on</strong>fidenceto use motivati<strong>on</strong>al interviewingtechniques (please seePractical Strategies for Change)• Lowered expectati<strong>on</strong>s: Hygienistsmay feel that patients are unlikelyto change their behaviors despitecounseling. Patients that dentalhygienists have the lowest expectati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g>—those with high plaquelevels—may receive less genuineverbal interacti<strong>on</strong> and not receivethe more intensive instructi<strong>on</strong>they need. 7 These more challengingpatients may be ideal candidatesfor dental hygienists tobegin targeting for incorporating<strong>anti</strong><strong>microbial</strong> oral rinsing intodaily home care.• Not enough time: Lack <str<strong>on</strong>g>of</str<strong>on</strong>g> interestand resistance from the patient26 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
Practical Strategies for ChangeThe patient is the center <str<strong>on</strong>g>of</str<strong>on</strong>g> any successful change effort.Promoting change starts with listening to the patient andproviding suggesti<strong>on</strong>s and skills teaching that are alignedwith the patient’s values. <str<strong>on</strong>g>Dental</str<strong>on</strong>g> hygienists need to be comfortablewith actively questi<strong>on</strong>ing and interviewing patientsto elicit the patient’s beliefs and values about oral hygiene,health, and disease and be prepared for resp<strong>on</strong>ses that d<strong>on</strong>ot c<strong>on</strong>form with ideals. 28 Effective questi<strong>on</strong>ing minimizespatient defensiveness, allowing patients to c<strong>on</strong>sider change.The following are strategies that can promote effective dialogueand support adopti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> healthy behaviors.• Ask patient about current oral health practicesBegin with determining the patient’s current level <str<strong>on</strong>g>of</str<strong>on</strong>g> selfcare.Example: “What do you do each day to take care<str<strong>on</strong>g>of</str<strong>on</strong>g> your teeth and gums?” You may want to ask thepatient questi<strong>on</strong>s that elicit felt needs, such as, “If youcould change anything about your oral health, whatwould you change?” Avoid a c<strong>on</strong>fr<strong>on</strong>tati<strong>on</strong>al approach,and be sure to support healthy activities the patient isalready performing.• Assess patient readiness to changeDetermine the patient’s readiness to incorporate newself-care behaviors. 23 The initial questi<strong>on</strong> may be “Wouldyou be willing to try using an <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinsetwice daily?” If the patient resp<strong>on</strong>ds positively, move topractical support. If the patient resp<strong>on</strong>ds with disinterest,determine any obstacles to change. “Have you triedthem in the past? Did you find <strong>on</strong>e you liked? Why not?Why d<strong>on</strong>’t you think it would be helpful?” Be sure tomaintain a n<strong>on</strong>c<strong>on</strong>fr<strong>on</strong>tati<strong>on</strong>al attitude. It may help towrite down patient objecti<strong>on</strong>s, and c<strong>on</strong>tinue to listen toobjecti<strong>on</strong>s until the patient is finished. Active listeningmay diffuse patient resistance. If the patient is unwillingto c<strong>on</strong>sider change, providing interventi<strong>on</strong>s over multiplevisits can encourage the patient to rethink his or herdecisi<strong>on</strong>. Always work within the patient’s stage <str<strong>on</strong>g>of</str<strong>on</strong>g> readinessto change.• Supervise new skills / behaviorsIf the patient is ready to attempt new behaviors, supervisedpractice will enhance patient self-efficacy. 3 Encouragethe patient to practice using <strong>mouth</strong>rinse, and showthe patient what to look for <strong>on</strong> the label. This will increasethe patient’s comfort level and success with the newbehavior. Remind the patient that if a product was shownvia research to be effective with twice daily use, using theproduct <strong>on</strong>ce daily may not yield the desired outcomes.• Structure a plan for successful adopti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the newbehaviorIf the patient is ready to change, it is also important to helpwith the plan for success. Unlike other negative behaviorssuch as overeating or smoking, patients do not derivepositive satisfacti<strong>on</strong> when neglecting oral self-care. Theprimary obstacle is apathy. Work with the patient todevelop a brief change plan that incorporates envir<strong>on</strong>mentalsupport. Encourage the patient to be specific.These planning steps maximize the likelihood <str<strong>on</strong>g>of</str<strong>on</strong>g> successfulchange. Example: “I’m glad you’re ready to makea positive change. I’ve seen many patients significantlyimprove the health <str<strong>on</strong>g>of</str<strong>on</strong>g> their gums by adding an <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse to their daily routine. Do you have an<strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse? Do you know where to look t<str<strong>on</strong>g>of</str<strong>on</strong>g>ind out if your rinse is ADA-Accepted? When do youplan to use your rinse? Will your use <str<strong>on</strong>g>of</str<strong>on</strong>g> the rinse matchthe manufacturer’s recommendati<strong>on</strong>s for daily care?”• Anticipate obstaclesStressful life experiences can disrupt the formati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g>positive habits. 18 Encourage the patient to incorporateexternal memory triggers (eg, notes to self) to allow himor her to maintain or resume positive oral health practicesduring disruptive or stressful periods. If the patientdoes not discuss obstacles, you may want to engage inself-disclosure or share examples from your experiencewith other patients. Example: “It can be hard sometimesto remember new healthy habits when we’re busy, sick,traveling, or stressed out. I’m a dental hygienist, andsome days I’m so busy I barely have time to brush myteeth. What are some ways that help you remember todo things when life is stressful? What are some obstaclesthat may keep you from using an <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse twice daily?”• Follow up with the patientAsk the patient about whether he or she has successfullyincorporated the behavior and any obstacles thatwere encountered: “Were you able to find a productyou really liked? Could you easily access the product?Was it hard to be c<strong>on</strong>sistent? What was your biggestchallenge?” Praise any progress toward the desiredbehavior, and revise the patient’s acti<strong>on</strong> plan accordingly:“Even though you weren’t able to use the rinseevery day twice daily, I’m glad that you were able touse it before bed most nights. You have made a greatstart! Do you think you can use it more <str<strong>on</strong>g>of</str<strong>on</strong>g>ten? When doyou think you can incorporate a sec<strong>on</strong>d rinse into yourday?” Specific follow-up dem<strong>on</strong>strates care for thepatient and is appreciated. Follow-up is also central tomaintaining change. 26,27While it takes time to change behaviors, the above interventi<strong>on</strong>sare brief and can be incorporated into a preventive,therapeutic, or period<strong>on</strong>tal maintenance visit. Throughuse <str<strong>on</strong>g>of</str<strong>on</strong>g> effective questi<strong>on</strong>ing and encouraging patients toshare their health values and behaviors, dental hygienistscan <str<strong>on</strong>g>of</str<strong>on</strong>g>fer targeted advice and be perceived as caring andsupportive while fulfilling their resp<strong>on</strong>sibility to educatepatients. N<strong>on</strong>c<strong>on</strong>fr<strong>on</strong>tati<strong>on</strong>al questi<strong>on</strong>ing minimizes patientdefensiveness and ensures they will be as receptive aspossible to receiving informati<strong>on</strong> <strong>on</strong> their oral health.Repeated interventi<strong>on</strong>s can assist patients as they adoptpositive behaviors that will improve oral health and quality<str<strong>on</strong>g>of</str<strong>on</strong>g> life.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 27
and poor financial incentives fororal hygiene instructi<strong>on</strong> may c<strong>on</strong>tributeto limiting the time spent<strong>on</strong> educati<strong>on</strong>. 8,9For all <str<strong>on</strong>g>of</str<strong>on</strong>g> these reas<strong>on</strong>s, dentalhygienists may tend to c<strong>on</strong>tinue torecommend the traditi<strong>on</strong>al therapies<str<strong>on</strong>g>of</str<strong>on</strong>g> brushing and flossing al<strong>on</strong>e. However,compliance with daily flossinghas been reported to be generally low,ranging from <strong>on</strong>ly 10% to 30%, 5 sopatients may benefit from informati<strong>on</strong>about new and adjunctive methods forthorough plaque removal.But changing dental hygienistbehavior is difficult due to the complexity<str<strong>on</strong>g>of</str<strong>on</strong>g> the process, and differentbarriers likely resp<strong>on</strong>d to differentapproaches to change. 10,11 Simpleexposure to new knowledge may beinsufficient to overcome most barriersto change practices, 11,12 but disseminati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> informati<strong>on</strong> can be more effectivein changing behavior when combinedwith other methods such asinteractive educati<strong>on</strong>al activities,enabling tools, and reminders. 13 Inadditi<strong>on</strong>, comparing <strong>on</strong>e’s currentpractice behaviors to sources <str<strong>on</strong>g>of</str<strong>on</strong>g> evidence,such as guidelines and externalfeedback, has been shown to motivatechange. 12,14 Reading journal articlesthat summarize the evidence base in asubject area, like the <strong>on</strong>es published inthis journal <str<strong>on</strong>g>supplement</str<strong>on</strong>g>, and comparingthe findings to <strong>on</strong>e’s current practicemay stimulate a need that encouragespractiti<strong>on</strong>ers to change theirpr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al behaviors.Recently, two pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al dentalorganizati<strong>on</strong>s have <str<strong>on</strong>g>of</str<strong>on</strong>g>ficially acknowledgedevidence about the adjunctiveuse <str<strong>on</strong>g>of</str<strong>on</strong>g> daily <strong>anti</strong><strong>microbial</strong> rinsing. TheAmerican <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> (ADA)released a statement in support <str<strong>on</strong>g>of</str<strong>on</strong>g> theuse <str<strong>on</strong>g>of</str<strong>on</strong>g> ADA–Accepted <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> in additi<strong>on</strong> to traditi<strong>on</strong>albrushing and interdental cleaning. 15The Canadian <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists’Associati<strong>on</strong> (CDHA) published a positi<strong>on</strong>statement supporting the incorporati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong> rinsing inpatient home care routines. 16 Both <str<strong>on</strong>g>of</str<strong>on</strong>g>these documents provide support forthe dental hygienist as he or she recommendsthat patients incorporate oralrinsing into their daily routine.EncouragingCompliance / AdherenceOnce a dental hygienist decides toassist patients in improving their oralhealth status through the implementati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> an evidence-based product, (eg,an <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse), the dentalhygienist must motivate the patientto change his or her daily oral care routine.Research c<strong>on</strong>firms what dentalhygienists know intuitively, thatAdherence versus Compliancepatients are reluctant to change theirhome care routines and, overall, maynot display interest in oral hygieneinstructi<strong>on</strong>. 9,17Despite the value people place <strong>on</strong>oral health, patients are increasinglyDespite the value people place <strong>on</strong> oral health,patients are increasingly strained withmeeting the demands <str<strong>on</strong>g>of</str<strong>on</strong>g> daily life.Stressful life events have also been shown tointerfere with self-care.strained with meeting the demands <str<strong>on</strong>g>of</str<strong>on</strong>g>daily life. 18 Stressful life events havealso been shown to interfere with selfcare.18 In a study examining the impact<str<strong>on</strong>g>of</str<strong>on</strong>g> oral hygiene educati<strong>on</strong>, patientswith poor oral hygiene subsequent toinstructi<strong>on</strong>s and educati<strong>on</strong> reportedhaving difficulty taking care <str<strong>on</strong>g>of</str<strong>on</strong>g> theirteeth and had more factors that interferedwith self-care than the more successfulstudy participants. 19 Moreover,because incorporating complex behaviors—suchas traditi<strong>on</strong>al oral self-carebehaviors—may be met with lesscompliance than simpler strategies, 19oral rinsing interventi<strong>on</strong>s may produceimproved adherence (see Adherenceversus Compliance below).Further complicating the issue <str<strong>on</strong>g>of</str<strong>on</strong>g>compliance, research evidence dem<strong>on</strong>stratesthat even pers<strong>on</strong>s with highplaque levels believe they are doing agood job with their oral home care. 19The fact that patients have an inabilityto evaluate their oral hygiene effectivenessand m<strong>on</strong>itor their oral healthstatus has been raised as a weaknessCompliance is a comm<strong>on</strong> term used in oral health care literature to describea patient’s willingness to follow a practiti<strong>on</strong>er’s instructi<strong>on</strong>s. 20,28 The term hasbeen criticized because it implies that the patient assumes a passive role andacquiesces to pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al recommendati<strong>on</strong>s he or she may not understandor agree with. 17,20,28 Some authors use the term adherence instead <str<strong>on</strong>g>of</str<strong>on</strong>g>compliance, as it implies that the patient takes a more active role in decisi<strong>on</strong>making and thereby improves behavior change. 20undermining dental hygiene instructi<strong>on</strong>.8 Finally, compliance in behaviorspreventing c<strong>on</strong>diti<strong>on</strong>s perceived to ben<strong>on</strong>–life threatening, such as period<strong>on</strong>taldisease and dental caries, mayhave a lower priority for patients. 18,20<str<strong>on</strong>g>Dental</str<strong>on</strong>g> hygienists can encouragepatients to adopt healthy behaviors,such as the twice-daily use <str<strong>on</strong>g>of</str<strong>on</strong>g> anADA-Accepted <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse,by a variety <str<strong>on</strong>g>of</str<strong>on</strong>g> methods. <str<strong>on</strong>g>Dental</str<strong>on</strong>g>hygienists can listen to patientfeelings and values and emphasizethe value and relevance <str<strong>on</strong>g>of</str<strong>on</strong>g> oralhygiene care before providing oralhygiene educati<strong>on</strong>. 21 This allowspatients to link improved healthbehaviors to these values, enhancing28 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
20, 22-23Table I. Transtheoretical Stages <str<strong>on</strong>g>of</str<strong>on</strong>g> Change and Suggested Interventi<strong>on</strong>sStage Characteristics Suggested Interventi<strong>on</strong>Prec<strong>on</strong>templati<strong>on</strong> Patient is unaware <str<strong>on</strong>g>of</str<strong>on</strong>g> the Verify patient’s state <str<strong>on</strong>g>of</str<strong>on</strong>g> readinessneed for behavior changeor resistant to changeRaise patient awareness“I w<strong>on</strong>’t change” “Are you aware <str<strong>on</strong>g>of</str<strong>on</strong>g> the health benefits <str<strong>on</strong>g>of</str<strong>on</strong>g> using an<strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse twice daily?”C<strong>on</strong>templati<strong>on</strong> Patient has c<strong>on</strong>sidered Verify patient’s state <str<strong>on</strong>g>of</str<strong>on</strong>g> readinesschanging behavior but isnot currently taking acti<strong>on</strong> Compliment patient <strong>on</strong> thinking about making a change“I might change” “Sounds like you’ve been thinking about making changesin your oral self-care. That’s great! What would you sayis holding you back from taking that step?”Preparati<strong>on</strong> Patient is ready to take Verify patient’s state <str<strong>on</strong>g>of</str<strong>on</strong>g> readinesspositive acti<strong>on</strong>Provide acti<strong>on</strong>able informati<strong>on</strong>“I will change”I’m glad you’re ready to make a healthy change. If youwanted to use <strong>mouth</strong>rinse t<strong>on</strong>ight, what steps would youneed to take? (eg, suggest purchasing a <strong>mouth</strong>rinse knownto reduce plaque and gingivitis)Acti<strong>on</strong> Patient is making initial Verify patient’s state <str<strong>on</strong>g>of</str<strong>on</strong>g> readinesssteps toward behaviorchangeSupport change“I am making a change” “I’m glad you decided to give <strong>mouth</strong>rinse a try. Have youthought about ways to make it easier to c<strong>on</strong>tinue yournew habit?” (eg, suggest placing it <strong>on</strong> the counters inall the bathrooms, placing a reminder note <strong>on</strong> thebathroom mirror, or including it in an oral care kit at work)Maintenance Patient has incorporated Verify patient’s state <str<strong>on</strong>g>of</str<strong>on</strong>g> readinessbehavior change successfully,although some relapseSupport behavior maintenance, explore potentialmay have occurredobstacles, make c<strong>on</strong>tingency plans“I have been making “That’s w<strong>on</strong>derful to hear you’re using <strong>mouth</strong>rinse! I canchanges”see the improvement in your plaque and gingival bleedingscores. It takes time to change lifetime habits. We will keepm<strong>on</strong>itoring your oral health status at each dental hygienevisit. Let me show you how to m<strong>on</strong>itor yourself at home.”their readiness to make positivechanges. 21In additi<strong>on</strong>, change efforts shouldbe tailored to the patient’s expressedreadiness to change. According to theTranstheoretical Model <str<strong>on</strong>g>of</str<strong>on</strong>g> Change,patients are in <strong>on</strong>e <str<strong>on</strong>g>of</str<strong>on</strong>g> several stages<str<strong>on</strong>g>of</str<strong>on</strong>g> readiness to incorporate new20, 22-23behaviors, and interventi<strong>on</strong>sshould be targeted accordingly. TableI shows stages <str<strong>on</strong>g>of</str<strong>on</strong>g> change and appropriateinterventi<strong>on</strong>s based <strong>on</strong> thepatient’s stages <str<strong>on</strong>g>of</str<strong>on</strong>g> readiness.In additi<strong>on</strong> to matching educati<strong>on</strong>alinterventi<strong>on</strong>s to patient readiness forchange, it is important to tailor informati<strong>on</strong>to each individual patient.Through the skillful use <str<strong>on</strong>g>of</str<strong>on</strong>g> listening,questi<strong>on</strong>ing, imparting knowledge,and teaching skills, the dental hygienistcan influence the key dimensi<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g>patient behavior including acquiringknowledge, changing attitudes, heighteningperceived needs, and improvingmotivati<strong>on</strong>. 19,24 While the actual interventi<strong>on</strong>srecommended may be thesame across a variety <str<strong>on</strong>g>of</str<strong>on</strong>g> patients—forSpecial <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 29
Table II. <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienist Acti<strong>on</strong>s for Supporting Patient Behavior ChangeGeneral for All PatientsIndividualized to Specific PatientTarget high-risk patientsClarify patient valuesDetermine the patient’s state <str<strong>on</strong>g>of</str<strong>on</strong>g> readiness for changeInquire about current behaviorsTailor approach—ensure relevanceC<strong>on</strong>vince patient <str<strong>on</strong>g>of</str<strong>on</strong>g> effectiveness <str<strong>on</strong>g>of</str<strong>on</strong>g> interventi<strong>on</strong>Highlight the pleasurable sensati<strong>on</strong>s and socialbenefits <str<strong>on</strong>g>of</str<strong>on</strong>g> oral hygiene and healthMaintain a positive envir<strong>on</strong>mentDisplay warmth and genuinenessProvide <strong>on</strong>going remindersBe prepared for relapseProvide sufficient c<strong>on</strong>tact timeEnsure mastery <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>on</strong>e skill at a timeProvide meaningful praiseInclude intraoral dem<strong>on</strong>strati<strong>on</strong>sInclude supervised practiceEncourage a partnership incorporating two-waycommunicati<strong>on</strong>Ensure patient can self-m<strong>on</strong>itor improvements (eg,decreased redness, swelling, and bleeding)Provide patient specific written educati<strong>on</strong>al materials to<str<strong>on</strong>g>supplement</str<strong>on</strong>g> interventi<strong>on</strong>sAssist patient in managing when home care will occur,incorporating c<strong>on</strong>tingency plansKey elements to maximize that patients maintaintheir new behaviors include the use <str<strong>on</strong>g>of</str<strong>on</strong>g>positive feedback, patient reminders(such as ph<strong>on</strong>e calls and postcards),and adapting dental hygiene instructi<strong>on</strong>sto the needs <str<strong>on</strong>g>of</str<strong>on</strong>g> the patientexample, twice daily use <str<strong>on</strong>g>of</str<strong>on</strong>g> an <strong>anti</strong><strong>microbial</strong>rinse—the individual tailoring<str<strong>on</strong>g>of</str<strong>on</strong>g> educati<strong>on</strong>al sessi<strong>on</strong>s to these behavioraldimensi<strong>on</strong>s are critical for motivatingchange. 19,25 As new products areintroduced to the market, the dentalhygienists’ role becomes crucial inhelping patients understand the pers<strong>on</strong>alhealth care implicati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> theresearch literature. 25The provisi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> informati<strong>on</strong> aboutsafe and effective <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong> is important, but informati<strong>on</strong>al<strong>on</strong>e will not change patientbehavior. 8,9 The teaching <str<strong>on</strong>g>of</str<strong>on</strong>g> new skillsis a necessary comp<strong>on</strong>ent <str<strong>on</strong>g>of</str<strong>on</strong>g> an effectiveinterventi<strong>on</strong>. Skills acquisiti<strong>on</strong> isfacilitated by introducing skills <strong>on</strong>e ata time, allowing time for supervisedpractice. This approach increases thechance for successful transfer <str<strong>on</strong>g>of</str<strong>on</strong>g>knowledge from the <str<strong>on</strong>g>of</str<strong>on</strong>g>fice to thehome setting. 7 Using qu<strong>anti</strong>tativehygiene assessment tools such asplaque and gingivitis scores can helppatients see the relevance <str<strong>on</strong>g>of</str<strong>on</strong>g> instructi<strong>on</strong>to their oral health. 7Table II summarizes important features<str<strong>on</strong>g>of</str<strong>on</strong>g> successful dental hygieneinterventi<strong>on</strong>s designed to motivatepatients into changing their home carebehaviors. These factors combinedwith the patient’s belief that he or shehas c<strong>on</strong>trol over his or her oralhygiene and health will increase thelikelihood for positive behaviorchange. 3The fact that research-supported,oral health–promoting behaviors(such as the twice-daily use <str<strong>on</strong>g>of</str<strong>on</strong>g> a safeand effective <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse)need to be carried out over<strong>on</strong>e’s lifetime c<strong>on</strong>tributes to the challenge.17 Studies c<strong>on</strong>sistently showthat modest gains achieved initiallyin changing patient behavior diminishwith time and minimize initialgains. 19 Key elements to maximizethat patients maintain their newbehaviors include the use <str<strong>on</strong>g>of</str<strong>on</strong>g> positivefeedback, patient reminders (such asph<strong>on</strong>e calls and postcards), andadapting dental hygiene instructi<strong>on</strong>sto the needs <str<strong>on</strong>g>of</str<strong>on</strong>g> the patient. 20 In aseries <str<strong>on</strong>g>of</str<strong>on</strong>g> 3 studies evaluating themaintenance <str<strong>on</strong>g>of</str<strong>on</strong>g> self-care behaviorprograms, adherence was improvedwhen reminders were used, seeminglyfor as l<strong>on</strong>g as the reminderswere provided. 26 Therefore, maintenance<str<strong>on</strong>g>of</str<strong>on</strong>g> behavioral change is an<strong>on</strong>going and deliberate process. 27C<strong>on</strong>clusi<strong>on</strong>sAs preventive oral health experts,dental hygienists must c<strong>on</strong>tinually evaluatemethods <str<strong>on</strong>g>of</str<strong>on</strong>g> enhancing oral healthand recommend those techniques andproducts with evidence-based effectivenessto their patients. This articlehas examined strategies for promotingbehavioral change in the c<strong>on</strong>text <str<strong>on</strong>g>of</str<strong>on</strong>g>adopti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> twice-daily use <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong><strong>microbial</strong><strong>mouth</strong><strong>rinses</strong>, which have beenshown to effectively reduce plaque andpromote oral health when used as part<str<strong>on</strong>g>of</str<strong>on</strong>g> a daily self-care regimen. These principlescan also be applied when teachingpatients about other health careproducts and behaviors.30 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
References1. US Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Health and Human Services. Oral Healthin America: A Report <str<strong>on</strong>g>of</str<strong>on</strong>g> the Surge<strong>on</strong> General. Rockville,MD: US Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Health and Human Services,Nati<strong>on</strong>al Institute <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> and Crani<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Research,Nati<strong>on</strong>al Institutes <str<strong>on</strong>g>of</str<strong>on</strong>g> Health; 2000. http://www2.nidcr.nih.gov/sgr/sgrohweb/welcome.htm.2. US Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Health and Human Services. Nati<strong>on</strong>alCall to Acti<strong>on</strong> to Promote Oral Health. Rockville, MD: USDepartment <str<strong>on</strong>g>of</str<strong>on</strong>g> Health and Human Services, Public HealthService, Nati<strong>on</strong>al Institutes <str<strong>on</strong>g>of</str<strong>on</strong>g> Health, Nati<strong>on</strong>al Institute <str<strong>on</strong>g>of</str<strong>on</strong>g><str<strong>on</strong>g>Dental</str<strong>on</strong>g> and Crani<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Research; 2003. NIH Publicati<strong>on</strong>No. 03-5303. http://www.surge<strong>on</strong>general.gov/topics/oralhealth/nati<strong>on</strong>alcalltoacti<strong>on</strong>.htm.3. Koelen MA, Lindstrom B. Making healthy choices easychoices: the role <str<strong>on</strong>g>of</str<strong>on</strong>g> empowerment. Eur J Clin Nutr. 2005;59(suppl 1):S10-S16.4. Berenholz S, Pr<strong>on</strong>ovost PJ. Barriers to translating evidenceinto practice. Curr Opin Crit Care. 2003;9:321-325.5. Asadoorian J. Flossing: Canadian <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists Associati<strong>on</strong>Positi<strong>on</strong> Statement: CDHA Positi<strong>on</strong> Paper. CJDH.2006;40:112-1446. Cabana MD, Rand CS, Powe NR, et al. Why d<strong>on</strong>’t physiciansfollow clinical practice guidelines? A framework forimprovement. JAMA. 1999;282:1458-1465.7. Milgrom P, Weinstein P, Melnick S, et al. Oral hygieneInstructi<strong>on</strong> and health risk assessment in dental practice. JPublic Health Dent. 1989:49:24-31.8. McC<strong>on</strong>aughy FL, Lukken KM. Toevs SE. Health promoti<strong>on</strong>behaviors <str<strong>on</strong>g>of</str<strong>on</strong>g> private practice dental hygienists. J DentHyg.1991:54: 222-230.9. Bass<strong>on</strong> WJ. Oral health educati<strong>on</strong> provided by oral hygienistsin private practice. SADJ. 1999;54: 53-57.10. Bosse G, Breuer JP, Spies C. The resistance to changingguidelines—what are the challenges and how to meet them.Best Pract Res Clin Anaesthesiol. 2006;20:379-395.11. Bain KT. Barriers and strategies to influencing physicianbehavior. Am J Med Qual. 2007;22, 5-7.12. Bloom BS. Effects <str<strong>on</strong>g>of</str<strong>on</strong>g> c<strong>on</strong>tinuing medical educati<strong>on</strong> <strong>on</strong> improvingphysician clinical care and patient health: A review <str<strong>on</strong>g>of</str<strong>on</strong>g>systematic reviews. Int J Technol Assess Health Care. 2005;21:380-385.13. Gray J. Changing physician prescribing behaviour. Can JClin Pharmacol. 2006;13:e81-e84.14. Mead P. Clinical guidelines: promoting clinical effectivenessor a pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al minefield? J Adv Nurs. 2000;31:110-116.15. ADA affirms benefits <str<strong>on</strong>g>of</str<strong>on</strong>g> ADA-Accepted <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong> and toothpastes, fluoride <strong>mouth</strong> <strong>rinses</strong> [newsrelease].Chicago, IL: American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong>; May 23,2007. http://ada.org/public/media/releases/0705_release03.asp. Accessed July 27, 2007.16. Asadoorian J. Oral rinsing: Canadian <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Hygienists Associati<strong>on</strong>Positi<strong>on</strong> Statement. CDHA positi<strong>on</strong> paper <strong>on</strong> commerciallyavailable over-the-counter oral rinsing products.CJDH. 2006;40:168-183.17. Blinkhorn AS. Factors affecting the compliance <str<strong>on</strong>g>of</str<strong>on</strong>g> patients withpreventive dental regimens. Int Dent J.1993;43,294-298.18. Ower P. The role <str<strong>on</strong>g>of</str<strong>on</strong>g> self-administered plaque c<strong>on</strong>trol in themanagement <str<strong>on</strong>g>of</str<strong>on</strong>g> period<strong>on</strong>tal diseases: 2. Motivati<strong>on</strong>, techniquesand assessment. Dent Update. 2003;30:110-116.19. Weinstein P, Milgrom P, Melnick S, et al. How effective isoral hygiene instructi<strong>on</strong>? Results after 6 and 24 weeks. JPublic Health Dent. 1989;49:32-38.20. Silverman S, Wilder R. Anti<strong>microbial</strong> <strong>mouth</strong>rinse as part <str<strong>on</strong>g>of</str<strong>on</strong>g> acomprehensive oral care regimen: safety and compliancefactors. J Am <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Assoc. 2006;137(11 suppl ):22S-26S.21. Horowitz LG, Dillenberg J, Rattray J. Self-care motivati<strong>on</strong>: amodel for primary preventive oral health behavior change. JSch Health. 1987;57:114-11822. Prochaska JO, Norcross JC, DiClemente CC. Changing forGood: The Revoluti<strong>on</strong>ary Program That Explains the SixStages <str<strong>on</strong>g>of</str<strong>on</strong>g> Change and Teaches You How to Free YourselfFrom Bad Habits. New York: William Morrow; 1994.23. Astroth, DB, Cross-Poline GN, Stach DJ, et al. The transtheoreticalmodel: an approach to behavioral change. J DentHyg. 2002;76:286-295.24. Uitenbroek DG, Schaub RMH, Tromp JA, Kant JH. <str<strong>on</strong>g>Dental</str<strong>on</strong>g>hygienists’ influence <strong>on</strong> the patients’ knowledge, motivati<strong>on</strong>,self-care, and percepti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> change. Community Dent OralEpidemiol. 1989;17:87-90.25. Gluch-Scrant<strong>on</strong> J. Motivati<strong>on</strong>al strategies in dental hygienecare. Semin Dent Hyg. 1991;3:1-4, 6-8.26. McCaul KD, Glasgow RE, O’Neill HK. The problem <str<strong>on</strong>g>of</str<strong>on</strong>g> creatinghabits: establishing health-protective dental behaviors.Health Psychol. 1992;11:101-110.27. Cifuentes M, Fernald DH, Green LA, et al. Prescripti<strong>on</strong> forhealth: changing primary care practice to foster healthybehaviors. Ann Fam Med. 2005;3:S4-S12.28. Chu R, Craig B. Understanding the determinants <str<strong>on</strong>g>of</str<strong>on</strong>g> preventiveoral health behaviours. Probe. 1996; 30:12-18.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 31
C<strong>on</strong>clusi<strong>on</strong>Anti<strong>microbial</strong> Mouth<strong>rinses</strong> in C<strong>on</strong>temporary <str<strong>on</strong>g>Dental</str<strong>on</strong>g><str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Practice: The Take Home MessageMichele Le<strong>on</strong>ardi Darby, RDH, MSIntroducti<strong>on</strong>The primary indicati<strong>on</strong> for <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse use is to achieve areducti<strong>on</strong> in supragingival plaque andgingivitis. Evidence shows that anAmerican <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> (ADA)–Accepted <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinsecan result in a greater reducti<strong>on</strong> inplaque and gingivitis than brushingand flossing al<strong>on</strong>e. 1 Therefore, eventhe most diligent brusher and flossercan benefit from the additi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> anADA-Accepted <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinseto the daily homecare regimen.Anti<strong>microbial</strong> <strong>mouth</strong><strong>rinses</strong> reducethe bacterial count and inhibit thepathogenic bacterial activity in dentalbi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm that can cause gingivitis, aprecursor to period<strong>on</strong>titis. Brushingand flossing al<strong>on</strong>e may not always beenough to c<strong>on</strong>trol the pathogenicity<str<strong>on</strong>g>of</str<strong>on</strong>g> dental bi<str<strong>on</strong>g>of</str<strong>on</strong>g>ilm. Untreated, gingivitiscan advance to period<strong>on</strong>titis andtooth loss and may be associated withother chr<strong>on</strong>ic diseases and c<strong>on</strong>diti<strong>on</strong>ssuch as diabetes mellitus, cardiovasculardisease, obesity, and pre-termbirth. Most patients will improve theiroral health by adding an ADA-Accepted <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinse totheir self-care daily regimen <str<strong>on</strong>g>of</str<strong>on</strong>g> brushingand interdental cleaning. Therefore,the incorporati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> an ADA-Accepted <strong>mouth</strong>rinse into the dailyregimen <str<strong>on</strong>g>of</str<strong>on</strong>g> brushing and cleaninginterdentally is important to achieveoptimal oral health outcomes.The ADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g>Acceptance ProgramMore than 100 companies voluntarilyparticipate in the ADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g>Acceptance Program and more than400 oral care products marketeddirectly to c<strong>on</strong>sumers carry the ADASeal (Figure 1). 2 Oral health care pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>alsand c<strong>on</strong>sumers can visithttp://www.ada.org/ada/seal/adaseal_c<strong>on</strong>sumer_shopping.pdf to identifyproducts that have earned the ADASeal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance to guide their recommendati<strong>on</strong>sand purchases <str<strong>on</strong>g>of</str<strong>on</strong>g> overthe-counter(OTC) products. GivenMore than 100 companies voluntarilyparticipate in the ADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g>Acceptance Program and more than400 oral care products marketed directly toc<strong>on</strong>sumers carry the ADA Seal.Figure 1. The American<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> Seal<str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance. (Courtesy<str<strong>on</strong>g>of</str<strong>on</strong>g> the American<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong>.)the importance <str<strong>on</strong>g>of</str<strong>on</strong>g> oral and systemichealth, and product safety and efficacy,this list is likely to expand andshould be reviewed regularly.The safety and efficacy data for thetwice-daily use <str<strong>on</strong>g>of</str<strong>on</strong>g> an <strong>anti</strong>plaque and<strong>anti</strong>gingivitis <strong>anti</strong><strong>microbial</strong> <strong>mouth</strong>rinseis unequivocal. Products thathave been found effective againstplaque and gingivitis and that haveearned the ADA Seal are those thatc<strong>on</strong>tain 0.12% chlorhexidine gluc<strong>on</strong>ate(CHG) or a fixed combinati<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g> essential oils (EO). Listerine ® — afixed combinati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> EO—and itsgeneric equivalents carry the ADASeal; however, because <str<strong>on</strong>g>of</str<strong>on</strong>g> recentchanges in the ADA Seal program,prescripti<strong>on</strong> products such as Peridex ®(0.12% CHG), even if they have pre-32 The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g>
viously earned the ADA Seal, are nol<strong>on</strong>ger included in the ADA Seal program,as the gr<strong>anti</strong>ng <str<strong>on</strong>g>of</str<strong>on</strong>g> the ADA Sealfor prescripti<strong>on</strong> product has beenphased out.Evidence-BasedLiteratureIn additi<strong>on</strong> to the ADA Seal, wellprepared,published systematicreviews and meta-analyses that synthesizea large number <str<strong>on</strong>g>of</str<strong>on</strong>g> rigorousstudies <strong>on</strong> a focused topic and thatarrive at clear c<strong>on</strong>clusi<strong>on</strong>s can beextremely valuable in guiding clinicaldecisi<strong>on</strong>s regarding products,devices, treatments, and interventi<strong>on</strong>s.Many such studies and reviews inadditi<strong>on</strong> to original research papersare cited throughout this <str<strong>on</strong>g>supplement</str<strong>on</strong>g>,and these references can provide furtherbackground and informati<strong>on</strong> <strong>on</strong>the benefits <str<strong>on</strong>g>of</str<strong>on</strong>g> using an <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse as part <str<strong>on</strong>g>of</str<strong>on</strong>g> a daily regimen.One good example cited withinthese pages is a recent meta-analysis<str<strong>on</strong>g>of</str<strong>on</strong>g> 6-m<strong>on</strong>th studies <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>plaque and<strong>anti</strong>gingivitis agents. 3 Moreover, systematicreviews <strong>on</strong> a variety <str<strong>on</strong>g>of</str<strong>on</strong>g> dentalsubject areas are also available fromthe Cochrane Library including theCochrane Database <str<strong>on</strong>g>of</str<strong>on</strong>g> SystematicReviews at www.cochrane.org. Thissite is an essential resource for busydental hygienists who strive to maintainan evidence-based practice.In general, possessing a basicknowledge <str<strong>on</strong>g>of</str<strong>on</strong>g> what c<strong>on</strong>stitutes appropriateresearch methods and the abilityto read the pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al literatureincreases the dental hygienist’s competenceas a critical c<strong>on</strong>sumer <str<strong>on</strong>g>of</str<strong>on</strong>g>research, enabling the dental hygienistto translate important research findingsinto practice in a timely manner.C<strong>on</strong>clusi<strong>on</strong>sIn c<strong>on</strong>clusi<strong>on</strong>, most patients willimprove their oral health by adding anADA-Accepted <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse to their self-care daily regimen<str<strong>on</strong>g>of</str<strong>on</strong>g> toothbrushing and interdentalcleaning. Within the c<strong>on</strong>text <str<strong>on</strong>g>of</str<strong>on</strong>g> clinicalpractice and current research evidence,dental hygienists should recommendthat patients practice a three-step dailyoral hygiene regimen <str<strong>on</strong>g>of</str<strong>on</strong>g> brushing,interdental cleaning, and rinsing withan ADA-Accepted <strong>anti</strong><strong>microbial</strong><strong>mouth</strong>rinse to help prevent and reduceplaque and gingivitis and speak withtheir dental hygienist or dentist foradditi<strong>on</strong>al guidance. Understandingthe process <str<strong>on</strong>g>of</str<strong>on</strong>g> change and matchingpr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>al oral care recommendati<strong>on</strong>sto patient’s specific needs, goals,values, and levels <str<strong>on</strong>g>of</str<strong>on</strong>g> readiness tochange may lead to patient adherenceand attainment <str<strong>on</strong>g>of</str<strong>on</strong>g> desired clinical outcomesover the l<strong>on</strong>g term. Regardless<str<strong>on</strong>g>of</str<strong>on</strong>g> the level <str<strong>on</strong>g>of</str<strong>on</strong>g> adherence to pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>alrecommendati<strong>on</strong>s, patients needregular instructi<strong>on</strong> and encouragementfrom a dental hygienist they trust.References1. Sharma N, Charles CH, Lynch MC, etal. Adjunctive benefit <str<strong>on</strong>g>of</str<strong>on</strong>g> an essentialoil-c<strong>on</strong>taining <strong>mouth</strong>rinse in reducingplaque and gingivitis in patients whobrush and floss regularly: a six-m<strong>on</strong>thstudy. J Am Dent Assoc. 2004;135:496-504.2. About the ADA Seal <str<strong>on</strong>g>of</str<strong>on</strong>g> Acceptance.American <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Associati<strong>on</strong> Website. http://www.ada.org/ada/seal/index.asp. Accessed July 30, 2007.3. Gunsolley JC. A meta-analysis <str<strong>on</strong>g>of</str<strong>on</strong>g> sixm<strong>on</strong>thstudies <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>anti</strong>plaque and<strong>anti</strong>gingivitis agents. J Am Dent Assoc.2006;137:1649-1657.Special <str<strong>on</strong>g>supplement</str<strong>on</strong>g> The <str<strong>on</strong>g>Journal</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Hygiene</str<strong>on</strong>g> 33
©McNEIL-PPC, Inc. 2007Rinse twice a day and call me in the morning.Taking care <str<strong>on</strong>g>of</str<strong>on</strong>g> your <strong>mouth</strong> may be important to your overall health. Rinsing with LISTERINE ® Antisepticmay help. It kills germs that cause gingivitis. That’s important because, if left untreated, gingivitis couldprogress to advanced gum disease, which emerging science associates with heart disease, diabetes andother health problems. To learn more, visit www.listerine.com, or ask your dentist, dental hygienistor physician about the <strong>mouth</strong>-body c<strong>on</strong>necti<strong>on</strong>.*DO IT FORDO IT FORThe Seal <strong>on</strong> the product means: *If brushing and flossing aren’t enough, use as directed as part <str<strong>on</strong>g>of</str<strong>on</strong>g> your regular oral care routine to help prevent and reduce plaque and gingivitis.“The ADA Council <strong>on</strong> Scientific Affairs’ Acceptance <str<strong>on</strong>g>of</str<strong>on</strong>g> Listerine is based <strong>on</strong> its finding that the product is effective in helping to prevent or reduce gingivitis and plaque above thegumline, when used as directed.”