The Role of an IG Infusion Nurse - Igliving.com
The Role of an IG Infusion Nurse - Igliving.com
The Role of an IG Infusion Nurse - Igliving.com

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
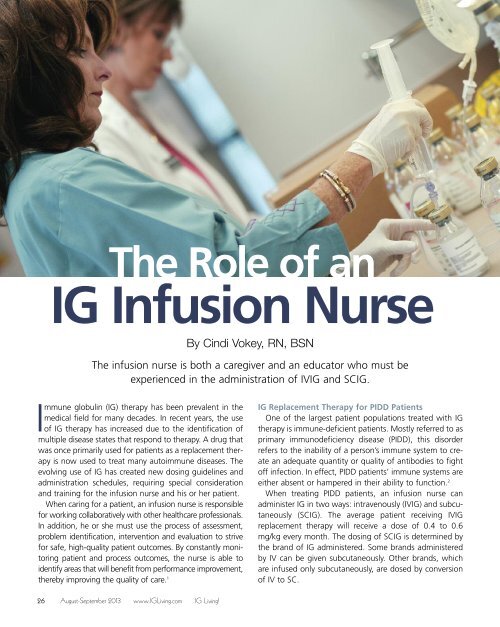
<strong>The</strong> <strong>Role</strong> <strong>of</strong> <strong>an</strong><strong>IG</strong> <strong>Infusion</strong> <strong>Nurse</strong>By Cindi Vokey, RN, BSN<strong>The</strong> infusion nurse is both a caregiver <strong>an</strong>d <strong>an</strong> educator who must beexperienced in the administration <strong>of</strong> IV<strong>IG</strong> <strong>an</strong>d SC<strong>IG</strong>.Immune globulin (<strong>IG</strong>) therapy has been prevalent in themedical field for m<strong>an</strong>y decades. In recent years, the use<strong>of</strong> <strong>IG</strong> therapy has increased due to the identification <strong>of</strong>multiple disease states that respond to therapy. A drug thatwas once primarily used for patients as a replacement therapyis now used to treat m<strong>an</strong>y autoimmune diseases. <strong>The</strong>evolving use <strong>of</strong> <strong>IG</strong> has created new dosing guidelines <strong>an</strong>dadministration schedules, requiring special consideration<strong>an</strong>d training for the infusion nurse <strong>an</strong>d his or her patient.When caring for a patient, <strong>an</strong> infusion nurse is responsiblefor working collaboratively with other healthcare pr<strong>of</strong>essionals.In addition, he or she must use the process <strong>of</strong> assessment,problem identification, intervention <strong>an</strong>d evaluation to strivefor safe, high-quality patient out<strong>com</strong>es. By const<strong>an</strong>tly monitoringpatient <strong>an</strong>d process out<strong>com</strong>es, the nurse is able toidentify areas that will benefit from perform<strong>an</strong>ce improvement,thereby improving the quality <strong>of</strong> care. 1<strong>IG</strong> Replacement <strong>The</strong>rapy for PIDD PatientsOne <strong>of</strong> the largest patient populations treated with <strong>IG</strong>therapy is immune-deficient patients. Mostly referred to asprimary immunodeficiency disease (PIDD), this disorderrefers to the inability <strong>of</strong> a person’s immune system to create<strong>an</strong> adequate qu<strong>an</strong>tity or quality <strong>of</strong> <strong>an</strong>tibodies to fight<strong>of</strong>f infection. In effect, PIDD patients’ immune systems areeither absent or hampered in their ability to function. 2When treating PIDD patients, <strong>an</strong> infusion nurse c<strong>an</strong>administer <strong>IG</strong> in two ways: intravenously (IV<strong>IG</strong>) <strong>an</strong>d subcut<strong>an</strong>eously(SC<strong>IG</strong>). <strong>The</strong> average patient receiving IV<strong>IG</strong>replacement therapy will receive a dose <strong>of</strong> 0.4 to 0.6mg/kg every month. <strong>The</strong> dosing <strong>of</strong> SC<strong>IG</strong> is determined bythe br<strong>an</strong>d <strong>of</strong> <strong>IG</strong> administered. Some br<strong>an</strong>ds administeredby IV c<strong>an</strong> be given subcut<strong>an</strong>eously. Other br<strong>an</strong>ds, whichare infused only subcut<strong>an</strong>eously, are dosed by conversion<strong>of</strong> IV to SC.26August-September 2013 www.<strong>IG</strong>Living.<strong>com</strong> <strong>IG</strong> Living!
Hizentra ® , Immune Globulin Subcut<strong>an</strong>eous (Hum<strong>an</strong>), 20% LiquidInitial U.S. Approval: 2010BRIEF SUMMARY OF PRESCRIBING INFORMATION<strong>The</strong>se highlights do not include all the information needed to use Hizentrasafely <strong>an</strong>d effectively. See full prescribing information for Hizentra.-----------------------------------INDICATIONS AND USAGE----------------------------------Hizentra is <strong>an</strong> Immune Globulin Subcut<strong>an</strong>eous (Hum<strong>an</strong>) (<strong>IG</strong>SC), 20% Liquid indicated forthe treatment <strong>of</strong> primary immunodeficiency (PI) in adults <strong>an</strong>d pediatric patients 2 years <strong>of</strong>age <strong>an</strong>d older.-----------------------------DOSAGE AND ADMINISTRATION--------------------------------For subcut<strong>an</strong>eous infusion only. Do not inject into a blood vessel.Start treatment with Hizentra 1week after the patient’s last Immune Globulin Intravenous(Hum<strong>an</strong>) (<strong>IG</strong>IV) infusion, when the patient has received <strong>IG</strong>IV infusions at regular intervalsfor at least 3 months.Dosage Calculate the initial weekly dose <strong>of</strong> Hizentra needed to achieve a systemic serum IgGexposure (area under the concentration-time curve [AUC]) not inferior to that <strong>of</strong> theprevious <strong>IG</strong>IV treatment.Initial dose = Previous <strong>IG</strong>IV dose (in grams) x 1.53No. <strong>of</strong> weeks between <strong>IG</strong>IV dosesTo convert the dose in grams to milliliters (mL), multiply the calculated dose (ingrams) by 5. Adjust the dose <strong>of</strong> Hizentra over time based on clinical response <strong>an</strong>d serum IgG troughlevels.Measure the serum IgG trough level during <strong>IG</strong>IV therapy prior to switching toHizentra <strong>an</strong>d again after 2 to 3 months <strong>of</strong> treatment with Hizentra. Adjust the doseto achieve a serum IgG trough level that is approximately 290 mg/dL higher th<strong>an</strong> thelast trough level during prior <strong>IG</strong>IV therapy.Administration <strong>Infusion</strong> sites – Abdomen, thigh, upper arm, <strong>an</strong>d/or lateral hip. Use up to 4 injectionsites simult<strong>an</strong>eously, with at least 2 inches between sites. <strong>Infusion</strong> volume – For the first infusion, up to 15 mL per injection site. This may beincreased to 20 mL per site after the fourth infusion <strong>an</strong>d to a maximum <strong>of</strong> 25 mL persite as tolerated. <strong>Infusion</strong> rate – For the first infusion, up to 15 mL/hr per site. This may be increased, toa maximum <strong>of</strong> 25 mL/hr per site as tolerated. However, the maximum flow rate isnot to exceed a total <strong>of</strong> 50 mL/hr for all sites <strong>com</strong>bined.-------------------------------DOSAGE FORMS AND STRENGTHS----------------------------0.2 g/mL (20%) protein solution for subcut<strong>an</strong>eous injection--------------------------------------CONTRAINDICATIONS ------------------------------------ Anaphylactic or severe systemic reactions to hum<strong>an</strong> immune globulin or <strong>com</strong>ponents <strong>of</strong>Hizentra, such as polysorbate 80 Hyperprolinemia (Hizentra contains the stabilizer L-proline) IgA-deficient patients with <strong>an</strong>tibodies against IgA <strong>an</strong>d a history <strong>of</strong> hypersensitivity----------------------------------WARNINGS AND PRECAUTIONS---------------------------- IgA-deficient patients with <strong>an</strong>ti-IgA <strong>an</strong>tibodies are at greater risk <strong>of</strong> severehypersensitivity <strong>an</strong>d <strong>an</strong>aphylactic reactions. Discontinue use if hypersensitivity reactionoccurs. Thrombotic events have been reported with the use <strong>of</strong> immune globulin products,including Hizentra. Aseptic meningitis syndrome has been reported to occur with <strong>IG</strong>IV or <strong>IG</strong>SC treatment (5.3). Monitor patients for reactions reported to occur with <strong>IG</strong>IV treatment that may occurwith <strong>IG</strong>SC treatment, including renal dysfunction/failure, thrombotic events, hemolysis,<strong>an</strong>d tr<strong>an</strong>sfusion-related acute lung injury (TRALI). Products made from hum<strong>an</strong> plasma c<strong>an</strong> contain infectious agents, e.g., viruses <strong>an</strong>d,theoretically, the Creutzfeldt-Jakob disease (CJD) agent.------------------------------------ADVERSE REACTIONS---------------------------------------<strong>The</strong> most <strong>com</strong>mon adverse reactions, observed in 5% <strong>of</strong> study subjects, were localreactions (i.e., swelling, redness, heat, pain, <strong>an</strong>d itching at the injection site), headache,diarrhea, fatigue, back pain, nausea, pain in extremity, cough, rash, pruritus, vomiting,abdominal pain (upper), migraine, <strong>an</strong>d pain.To report SUSPECTED ADVERSE REACTIONS, contact CSL BehringPharmacovigil<strong>an</strong>ce at 1-866-915-6958 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.-----------------------------------DRUG INTERACTIONS-----------------------------------------<strong>The</strong> passive tr<strong>an</strong>sfer <strong>of</strong> <strong>an</strong>tibodies may: Lead to misinterpretation <strong>of</strong> the results <strong>of</strong> serological testing. Interfere with the response to live virus vaccines.-----------------------------USE IN SPECIFIC POPULATIONS---------------------------------- Pregn<strong>an</strong>cy: No hum<strong>an</strong> or <strong>an</strong>imal data. Use only if clearly needed. Pediatric: No pediatric-specific dose requirements are necessary to achievethe desired serum IgG levels.Storage <strong>an</strong>d H<strong>an</strong>dlingWhen stored at room temperature (up to 25°C [77°F]), Hizentra is stable for up to 30months, as indicated by the expiration date printed on the outer carton <strong>an</strong>d vial label.DO NOT FREEZE. Do not use product that has been frozen. Do not shake. Keep Hizentra inits original carton to protect it from light.Revised: December 2012
IV<strong>IG</strong> <strong>The</strong>rapy for Autoimmune DiseasesIV<strong>IG</strong> therapy is used as <strong>an</strong> immune modulator to treatm<strong>an</strong>y autoimmune diseases such as chronic inflammatorydemyelinating peripheral neuropathy, myasthenia gravis,Guillain-Barré syndrome, multiple sclerosis, polymyositis<strong>an</strong>d dermatomyositis. <strong>The</strong> <strong>com</strong>plete mech<strong>an</strong>ism <strong>of</strong> <strong>IG</strong> isnot fully understood; however, it is believed that throughthe administration <strong>of</strong> higher doses <strong>of</strong> <strong>IG</strong>, the immune systemis able to reverse the autoimmune process. Althoughdosing c<strong>an</strong> be different for several diseases, treatment is<strong>com</strong>monly given every three to four weeks, <strong>an</strong>d it is usuallyadministered at a high dose (generally 1 to 2 grams <strong>of</strong>IV<strong>IG</strong> per kg <strong>of</strong> body weight) to attempt to decrease theseverity <strong>of</strong> the autoimmune disease. It is import<strong>an</strong>t for <strong>an</strong>infusion nurse to be familiar with the <strong>com</strong>mon scheduling<strong>of</strong> IV<strong>IG</strong> for each disease.When preparing the <strong>IG</strong>,maintaining aseptictechnique is import<strong>an</strong>t.<strong>The</strong> <strong>Nurse</strong>’s <strong>Role</strong> in Administering IV<strong>IG</strong> <strong>The</strong>rapyWhen administering IV<strong>IG</strong>, <strong>an</strong> infusion nurse must assessthe patient’s health history <strong>an</strong>d perform a risk assessmentprior to each infusion. Special consideration needs to betaken in regard to the patient’s history <strong>of</strong> exposure to IV<strong>IG</strong>.For inst<strong>an</strong>ce, patients are categorized in the followingm<strong>an</strong>ner:• IV<strong>IG</strong> naïve: patients who have never received IV<strong>IG</strong>• IV<strong>IG</strong> initial infusions: patients who have received IV<strong>IG</strong>but may have ch<strong>an</strong>ged br<strong>an</strong>ds or have not received therapywithin six weeks• IV<strong>IG</strong> subsequent infusions: patients who will receivetherapy after they have received their first dose from <strong>an</strong>ew br<strong>an</strong>d, after the first lifetime dose or after havingreceived the same drug within a six-week time frame (subsequentinfusions are also defined as infusions that arewell-tolerated without a reaction or signific<strong>an</strong>t ch<strong>an</strong>ge invital signs)<strong>The</strong> nurse must also be familiar with each br<strong>an</strong>d <strong>of</strong> IV<strong>IG</strong>,its label <strong>an</strong>d specifications <strong>an</strong>d its titration guidelines.Prior to preparing <strong>IG</strong> for administration, IV access (eitherperipherally or through a vascular access device) must beobtained. <strong>Infusion</strong> nurses receive specialized training forperipheral IV insertion. When accessing peripherally, athorough assessment <strong>of</strong> the patient’s ease for accessshould be made. Should there be <strong>an</strong>y previous difficultieswith IV access, the nurse should report that to the prescribingphysici<strong>an</strong>.Patients who have been receiving therapy for a prolongedperiod <strong>of</strong> time or who have been diagnosed withpoor peripheral IV access will have a vascular access devicefor IV administration. <strong>The</strong> infusion nurse must haveextensive experience with these devices, which include:• PICC lines (must be experienced with dressingch<strong>an</strong>ges, flushing requirements <strong>an</strong>d cap ch<strong>an</strong>ges)• Port-a-caths (must be experienced with accessing <strong>an</strong>dde-accessing)• Tunneled catheters such as Hickm<strong>an</strong> or Groshong(must be able to identify which tunneled catheter thepatient has <strong>an</strong>d what the flushing requirements are)Central lines should always be assessed for signs <strong>of</strong>infection, <strong>an</strong>dthenurseshouldeducate the patient in theproper identification <strong>of</strong> central line infections.When preparing the <strong>IG</strong>, maintaining aseptic technique isimport<strong>an</strong>t. To maintain a sterile infusion, <strong>an</strong>tiseptic c<strong>an</strong> beused on rubber stoppers.For proper <strong>IG</strong> administration, the nurse must be familiarwith the necessary equipment. Most infusions require theuse <strong>of</strong> several glass vials that will need a vented spikeadapter to be added to the tubing. In addition, the use <strong>of</strong>infusion pumps is re<strong>com</strong>mended. <strong>The</strong>refore, knowledge <strong>of</strong><strong>com</strong>mon infusion pumps is required.Both prior to <strong>an</strong>d throughout the infusion, the nurseshould assess the patient’s vital signs (pulse, blood pressure,respirations <strong>an</strong>d temperature). <strong>The</strong> nurse also shouldensure the patient has taken premedications as ordered bythe physici<strong>an</strong> <strong>an</strong>d that the patient is adequately hydrated.Once IV<strong>IG</strong> therapy has been initiated, careful assessment<strong>of</strong> the patient for infusion-related reactions is crucial. <strong>The</strong>nurse should underst<strong>an</strong>d the initial intervention for raterelatedreactions, including stopping the infusion <strong>an</strong>dassessing the patient’s status, as well as decreasing therate <strong>of</strong> infusion. All side effects should be documented<strong>an</strong>d reported, including mild to moderate rate-relatedreactions such as headache, nausea <strong>an</strong>d vomiting, chills,rigors <strong>an</strong>d flushing. 3While <strong>an</strong>aphylaxis is rare, it c<strong>an</strong> occur during IV<strong>IG</strong> <strong>an</strong>dSC<strong>IG</strong> administration. As such, the nurse’s knowledge <strong>of</strong>the m<strong>an</strong>agement <strong>of</strong> <strong>an</strong>aphylaxis is crucial. <strong>The</strong> nurse must28August-September 2013 www.<strong>IG</strong>Living.<strong>com</strong> <strong>IG</strong> Living!
know where the <strong>an</strong>aphylaxis kit is located <strong>an</strong>d should befamiliar with the administration <strong>of</strong> <strong>an</strong> EpiPen <strong>an</strong>d othermedications included in the kit. Should <strong>an</strong>aphylaxis occur,<strong>IG</strong> administration should be immediately stopped, <strong>an</strong>d theappropriate <strong>an</strong>aphylaxis medications should beadministered. <strong>The</strong> patient should then be evaluated byemergency medical services personnel, <strong>an</strong>d the prescribingphysici<strong>an</strong> should be notified.Following the infusion, the nurse should discuss import<strong>an</strong>tpatient interventions such as staying well-hydrated,continuing premedications <strong>an</strong>d monitoring urine output.<strong>The</strong> <strong>Nurse</strong>’s <strong>Role</strong> in Administering SC<strong>IG</strong> <strong>The</strong>rapy<strong>The</strong> use <strong>of</strong> SC<strong>IG</strong> administration has been increasing overthe past few years, <strong>an</strong>dthere are now several products onthe market. SC<strong>IG</strong> <strong>of</strong>fers several adv<strong>an</strong>tages for the patient.IV access is not needed because the drug is administeredin the subcut<strong>an</strong>eous tissue. A steady state <strong>of</strong> IgG ismaintained, providing better long-term coverage frompotential infections. And, the patient tends to have lesssystemic side effects. Ultimately, the goal is to allow thepatient to be<strong>com</strong>e independent in therapy <strong>an</strong>d to selfadministerhis or her infusion on a weekly basis, <strong>an</strong>d thenurse plays <strong>an</strong> essential role in this.<strong>The</strong> nurse administering or teaching the patient toadminister SC<strong>IG</strong> should be knowledgeable about thedrug’s clinical indication <strong>an</strong>d implementation <strong>an</strong>d shoulddemonstrate <strong>com</strong>petency in clinical judgment <strong>an</strong>d practice.Patient education is a crucial element to the success<strong>of</strong> SC<strong>IG</strong> therapy. <strong>The</strong> nurse should always maintain <strong>an</strong>deducate the patient regarding infection control practices<strong>an</strong>d aseptic technique. And, he or she must underst<strong>an</strong>dhow to m<strong>an</strong>age patient side effects <strong>an</strong>d to recognize themost <strong>com</strong>mon ones.Site selection <strong>an</strong>d needle selection play <strong>an</strong> import<strong>an</strong>trole in the proper administration <strong>of</strong> SC<strong>IG</strong>. Often, the nursewill educate the patient regarding needle <strong>com</strong>fort. If thepatient is new to SC<strong>IG</strong>, the nurse c<strong>an</strong> explain the use <strong>of</strong>different needle lengths <strong>an</strong>d the option <strong>of</strong> choosing multiplesites. In some situations, the nurse may encouragethe patient to use several sites at once, thereby administeringless volume <strong>of</strong> <strong>IG</strong> into each site.When teaching the patient to self-administer, thereare two essential points. First, the patient should betaught to prime the drug but to not allow the drug t<strong>of</strong>low toward the end <strong>of</strong> the needles. Allowing a “drystick” (when the drug does not reach the end <strong>of</strong> theneedles) helps decrease skin reactions. Second, once theneedles have been inserted, checking for proper placementis crucial. <strong>The</strong> nurse <strong>an</strong>d/or the patient must drawback on the plunger to check for a blood return. If ablood return occurs, the needles may be entering a vasculararea. When this happens, the needles should be discarded<strong>an</strong>d a new set should be primed <strong>an</strong>d inserted asinstructed. 3Site reactions, which include swelling, itching <strong>an</strong>d redness,occur frequently in patients. <strong>The</strong>se reactions shoulddecrease over 24 to 48 hours as the drug is slowlyabsorbed after the infusion, <strong>an</strong>d they should decrease inoccurrence over time. For inst<strong>an</strong>ce, reactions occur more<strong>of</strong>ten in patients who are initiating therapy, <strong>an</strong>d they usuallydecrease over the first eight to 10 weeks <strong>of</strong> therapy. 4It’s import<strong>an</strong>t for the nurse to educate the patient regardinglocal reactions <strong>an</strong>d symptomatic treatment <strong>of</strong> them,including warm or cool <strong>com</strong>presses (whichever is preferredby the patient). But the patient should be instructed not touse hot <strong>com</strong>presses, as they c<strong>an</strong> cause the drug to absorbtoo quickly.Even after the patient be<strong>com</strong>es independent with SC<strong>IG</strong>,ongoing patient education is import<strong>an</strong>t. And, while thenurse’s responsibilities may decrease <strong>com</strong>pared with those<strong>of</strong> IV<strong>IG</strong>, his or her responsibilities are still vastly import<strong>an</strong>t.Ensuring Expert Care<strong>The</strong> infusion nurse plays <strong>an</strong> import<strong>an</strong>t role in the properadministration <strong>of</strong> <strong>IG</strong> therapy. To ensure expert care, thenurse must maintain the necessary qualifications <strong>an</strong>d education.And, he or she must underst<strong>an</strong>d that a key <strong>com</strong>ponent<strong>of</strong> both IV<strong>IG</strong> <strong>an</strong>d SC<strong>IG</strong> administration is patienteducation. Throughout the infusion process, the goal is toinstill trust <strong>an</strong>d confidence in the patient <strong>an</strong>d to maintainpr<strong>of</strong>essionalism in the patient-nurse relationship.CINDI VOKEY, RN, BSN, is the clinical educator at NuFACTORSpecialty Pharmacy.References1. Alex<strong>an</strong>der, M, Corrig<strong>an</strong>, A, Gorski, L, <strong>an</strong>d H<strong>an</strong>kins, J. <strong>Infusion</strong>Nursing: An Evidence-Based Approach. Elsevier Health Sciences,2009.2. Immune Deficiency Foundation. About Primary ImmunodeficiencyDiseases. Accessed at www.primaryimmune.org/about-primaryimmunodeficiency-disease.3. Younger, ME, Aro, L, <strong>an</strong>d Blouin, W, et al. Nursing Guidelines forAdministration <strong>of</strong> Immunoglobulin Replacement <strong>The</strong>rapy. Journal <strong>of</strong><strong>Infusion</strong> Nursing, J<strong>an</strong>-Feb 2013.4. Immune Globulin Nursing Society. Subcut<strong>an</strong>eous Immunoglobulin(SC<strong>IG</strong>) Treatment. Accessed at www.ig-ns.org/scig_treatment.August-September 2013 www.<strong>IG</strong>Living.<strong>com</strong> <strong>IG</strong> Living!29