Fractures and dislocations of the carpal bones - Punjab Orthopaedic ...
Fractures and dislocations of the carpal bones - Punjab Orthopaedic ...
Fractures and dislocations of the carpal bones - Punjab Orthopaedic ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
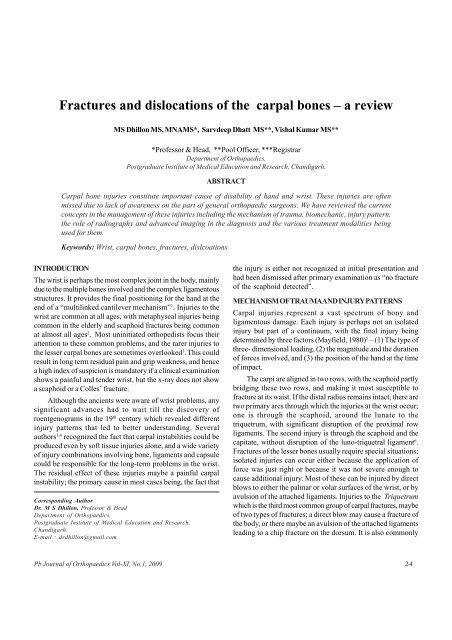
<strong>Fractures</strong> <strong>and</strong> <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> <strong>carpal</strong> <strong>bones</strong> – a reviewMS Dhillon MS, MNAMS*, Sarvdeep Dhatt MS**, Vishal Kumar MS***Pr<strong>of</strong>essor & Head, **Pool Officer, ***RegistrarDepartment <strong>of</strong> <strong>Orthopaedic</strong>s,Postgraduate Institute <strong>of</strong> Medical Education <strong>and</strong> Research, Ch<strong>and</strong>igarh.ABSTRACTCarpal bone injuries constitute important cause <strong>of</strong> disability <strong>of</strong> h<strong>and</strong> <strong>and</strong> wrist. These injuries are <strong>of</strong>tenmissed due to lack <strong>of</strong> awareness on <strong>the</strong> part <strong>of</strong> general orthopaedic surgeons. We have reviewed <strong>the</strong> currentconcepts in <strong>the</strong> management <strong>of</strong> <strong>the</strong>se injuries including <strong>the</strong> mechanism <strong>of</strong> trauma, biomechanic, injury pattern,<strong>the</strong> role <strong>of</strong> radiography <strong>and</strong> advanced imaging in <strong>the</strong> diagnosis <strong>and</strong> <strong>the</strong> various treatment modalities beingused for <strong>the</strong>m.Keywords: Wrist, <strong>carpal</strong> <strong>bones</strong>, fractures, dislcoationsINTRODUCTIONThe wrist is perhaps <strong>the</strong> most complex joint in <strong>the</strong> body, mainlydue to <strong>the</strong> multiple <strong>bones</strong> involved <strong>and</strong> <strong>the</strong> complex ligamentousstructures. It provides <strong>the</strong> final positioning for <strong>the</strong> h<strong>and</strong> at <strong>the</strong>end <strong>of</strong> a “multilinked cantilever mechanism” 1 . Injuries to <strong>the</strong>wrist are common at all ages, with metaphyseal injuries beingcommon in <strong>the</strong> elderly <strong>and</strong> scaphoid fractures being commonat almost all ages 2 . Most uninitiated orthopedists focus <strong>the</strong>irattention to <strong>the</strong>se common problems, <strong>and</strong> <strong>the</strong> rarer injuries to<strong>the</strong> lesser <strong>carpal</strong> <strong>bones</strong> are sometimes overlooked 3 . This couldresult in long term residual pain <strong>and</strong> grip weakness, <strong>and</strong> hencea high index <strong>of</strong> suspicion is m<strong>and</strong>atory if a clinical examinationshows a painful <strong>and</strong> tender wrist, but <strong>the</strong> x-ray does not showa scaphoid or a Colles’ fracture.Although <strong>the</strong> ancients were aware <strong>of</strong> wrist problems, anysignificant advances had to wait till <strong>the</strong> discovery <strong>of</strong>roentgenograms in <strong>the</strong> 19 th century which revealed differentinjury patterns that led to better underst<strong>and</strong>ing. Severalauthors 1,4 recognized <strong>the</strong> fact that <strong>carpal</strong> instabilities could beproduced even by s<strong>of</strong>t tissue injuries alone, <strong>and</strong> a wide variety<strong>of</strong> injury combinations involving bone, ligaments <strong>and</strong> capsulecould be responsible for <strong>the</strong> long-term problems in <strong>the</strong> wrist.The residual effect <strong>of</strong> <strong>the</strong>se injuries maybe a painful <strong>carpal</strong>instability; <strong>the</strong> primary cause in most cases being, <strong>the</strong> fact thatCorresponding AuthorDr. M S Dhillon, Pr<strong>of</strong>essor & HeadDepartment <strong>of</strong> <strong>Orthopaedic</strong>s,Postgraduate Institute <strong>of</strong> Medical Education <strong>and</strong> Research,Ch<strong>and</strong>igarh.E-mail : drdhillon@gmail.com<strong>the</strong> injury is ei<strong>the</strong>r not recognized at initial presentation <strong>and</strong>had been dismissed after primary examination as “no fracture<strong>of</strong> <strong>the</strong> scaphoid detected”.MECHANISM OF TRAUMA AND INJURY PATTERNSCarpal injuries represent a vast spectrum <strong>of</strong> bony <strong>and</strong>ligamentous damage. Each injury is perhaps not an isolatedinjury but part <strong>of</strong> a continuum, with <strong>the</strong> final injury beingdetermined by three factors (Mayfield, 1980) 5 – (1) The type <strong>of</strong>three- dimensional loading, (2) <strong>the</strong> magnitude <strong>and</strong> <strong>the</strong> duration<strong>of</strong> forces involved, <strong>and</strong> (3) <strong>the</strong> position <strong>of</strong> <strong>the</strong> h<strong>and</strong> at <strong>the</strong> time<strong>of</strong> impact.The carpi are aligned in two rows, with <strong>the</strong> scaphoid partlybridging <strong>the</strong>se two rows, <strong>and</strong> making it most susceptible t<strong>of</strong>racture at its waist. If <strong>the</strong> distal radius remains intact, <strong>the</strong>re aretwo primary arcs through which <strong>the</strong> injuries at <strong>the</strong> wrist occur;one is through <strong>the</strong> scaphoid, around <strong>the</strong> lunate to <strong>the</strong>triquetrum, with significant disruption <strong>of</strong> <strong>the</strong> proximal rowligaments. The second injury is through <strong>the</strong> scaphoid <strong>and</strong> <strong>the</strong>capitate, without disruption <strong>of</strong> <strong>the</strong> luno-triquetral ligament 6 .<strong>Fractures</strong> <strong>of</strong> <strong>the</strong> lesser <strong>bones</strong> usually require special situations;isolated injuries can occur ei<strong>the</strong>r because <strong>the</strong> application <strong>of</strong>force was just right or because it was not severe enough tocause additional injury. Most <strong>of</strong> <strong>the</strong>se can be injured by directblows to ei<strong>the</strong>r <strong>the</strong> palmar or volar surfaces <strong>of</strong> <strong>the</strong> wrist, or byavulsion <strong>of</strong> <strong>the</strong> attached ligaments. Injuries to <strong>the</strong> Triquetrumwhich is <strong>the</strong> third most common group <strong>of</strong> <strong>carpal</strong> fractures, maybe<strong>of</strong> two types <strong>of</strong> fractures; a direct blow may cause a fracture <strong>of</strong><strong>the</strong> body, or <strong>the</strong>re maybe an avulsion <strong>of</strong> <strong>the</strong> attached ligamentsleading to a chip fracture on <strong>the</strong> dorsum. It is also commonlyPb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200924
<strong>Fractures</strong> <strong>and</strong> <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> <strong>carpal</strong> <strong>bones</strong> – a reviewfractured as a part <strong>of</strong> perilunate dislocation.The Capitate is <strong>the</strong> largest bone in <strong>the</strong> wrist <strong>and</strong> has morearticulations than any o<strong>the</strong>r <strong>carpal</strong> bone; it also forms <strong>the</strong> centralportion <strong>of</strong> <strong>the</strong> perilunate disruptions. It could also be similarlyinjured in its neck, with a hyper dorsiflexion strain impinging<strong>the</strong> capitate against <strong>the</strong> radius. A special situation is <strong>the</strong> socalled naviculo-capitate syndrome, with fractures <strong>of</strong> <strong>the</strong>scaphoid <strong>and</strong> capitate, without any dislocation being observed.The neck fracture occurs if <strong>the</strong> injuring force follows a moredistally based arc than <strong>the</strong> commoner perilunate dislocation,with a tension fracture <strong>of</strong> <strong>the</strong> scaphoid permitting acute hyperextension <strong>and</strong> impingement <strong>of</strong> <strong>the</strong> capitate against radius. Theproximal fragment <strong>of</strong>ten rotates 180 degrees in <strong>the</strong> plane <strong>of</strong> <strong>the</strong>palm, as <strong>the</strong> wrist reduces spontaneously 7 .<strong>Fractures</strong> through <strong>the</strong> Trapezium are produced bycompression caused by <strong>the</strong> base <strong>of</strong> 1 st meta<strong>carpal</strong>, or as avulsionfractures due to <strong>the</strong> pull <strong>of</strong> <strong>the</strong> capsular attachments. Cordery<strong>and</strong> Ferrer-Torell 8 , after reviewing <strong>the</strong> world literature, found 37out <strong>of</strong> 75 reported fractures to be isolated injuries, <strong>and</strong> identifiedtwo major types: avulsion <strong>of</strong> <strong>the</strong> ridge <strong>and</strong> a vertical fractureassociated with dislocation <strong>of</strong> <strong>the</strong> 1 st Meta<strong>carpal</strong> <strong>and</strong> <strong>the</strong> radialfragment. The mechanism is usually a blow on <strong>the</strong> adductedthumb or a fall with <strong>the</strong> hyper extended h<strong>and</strong> in radial deviation 5.The Pisiform, being relatively more superficial, is generallyinjured by a direct injury such as a fall on <strong>the</strong> dorsiflexed h<strong>and</strong>,or <strong>the</strong> use <strong>of</strong> <strong>the</strong> h<strong>and</strong> as a hammer to strike an object. Since <strong>the</strong>flexor carpi ulnaris can potentially hold it in tension against <strong>the</strong>triquetrum, it can also sustain an osteochondral compressionfracture at <strong>the</strong> pisotriquetral joint, or its distal pole can beavulsed. Vasilas et al 9 reported that <strong>the</strong> fractures can be linear,comminuted or chip-in type.The Hamate can be fractured through its body, with orwithout articular surface involvement, or a fracture <strong>of</strong> <strong>the</strong> hookcould occur with a fall on <strong>the</strong> dorsiflexed h<strong>and</strong>, <strong>and</strong> tensionbeing exerted through <strong>the</strong> transverse <strong>carpal</strong> <strong>and</strong> pisohamateligaments. This is perhaps a relatively common sports relatedinjury, occurring with <strong>the</strong> use <strong>of</strong> bats or racquets or clubs. Thehook is usually avulsed from its base, but avulsion fractures <strong>of</strong><strong>the</strong> tip have also been reported. <strong>Fractures</strong> <strong>of</strong> <strong>the</strong> hamate bodyare perhaps only observed in direct crushing or blast injuries,<strong>and</strong> are reportedly clubbed into two main groups, those inwhich <strong>the</strong> fracture line is radial to <strong>the</strong> hook <strong>and</strong> those in whichit is ulnar to <strong>the</strong> hook. The Trapezoid is generally injured by alongitudinal force applied through <strong>the</strong> second meta<strong>carpal</strong>, <strong>and</strong>due to its shape <strong>and</strong> protected position, is perhaps <strong>the</strong> leastcommonly fractured carpus; it could, however be dorsallydislocated by a volar directed blow on <strong>the</strong> second meta<strong>carpal</strong>,with <strong>the</strong> occasionally reported fracture.Dislocations <strong>of</strong> <strong>the</strong> o<strong>the</strong>r carpus in isolation are rare, withtrapezium <strong>dislocations</strong> being commoner. The triquetrum hasstrong ulnar, palmar <strong>and</strong> dorsal ligaments, minimizing <strong>the</strong>chances <strong>of</strong> dislocation in isolation being <strong>the</strong> primary injury,<strong>and</strong> <strong>the</strong> hamate <strong>and</strong> capitate are relatively protected between<strong>the</strong> bases <strong>of</strong> <strong>the</strong> meta<strong>carpal</strong>s <strong>and</strong> <strong>the</strong> convex shape <strong>of</strong> <strong>the</strong>proximal <strong>carpal</strong> row.The lunate is discussed separately as both fractures <strong>and</strong><strong>dislocations</strong> <strong>of</strong> this “keystone bone” <strong>of</strong> <strong>the</strong> proximal <strong>carpal</strong>row are frequently encountered. Isolated fractures may beavulsion injuries, or repetitive stress could lead to avascularnecrosis. Most fractures result from hyper-extension injuries,with avulsions from <strong>the</strong> dorsal pole being more frequent due to<strong>the</strong> tension in <strong>the</strong> scapholunate ligament <strong>of</strong> a dorsally rotatinglunate.Diagnosis <strong>and</strong> radiologyThe diagnosis <strong>of</strong> <strong>the</strong>se injuries is based on a thorough clinicalexamination <strong>of</strong> an acutely injured wrist, with a high index <strong>of</strong>suspicion once fractures <strong>of</strong> <strong>the</strong> scaphoid are ruled out. Pain<strong>and</strong> tenderness are usually appropriately situated, with swelling,prominence <strong>and</strong> limited motion helping to localize <strong>the</strong> specificinjury. A good knowledge <strong>of</strong> <strong>the</strong> pertinent wrist anatomy isessential to locate <strong>the</strong> injury specifically.Radiographic examination is perhaps <strong>the</strong> most importantmodality for accurate diagnosis. The fractures or <strong>dislocations</strong>,however, may be very subtle at times, <strong>and</strong> awareness <strong>of</strong> <strong>the</strong>normal alignments as well as <strong>the</strong> requisition <strong>of</strong> special viewsfor specific injuries is usually required. Gilula 10 , reviewedradiographic wrist relationships <strong>and</strong> particularly, emphasized<strong>the</strong> postero-anterior view. He analyzed <strong>the</strong> three normal arcs<strong>and</strong> <strong>the</strong>ir abnormalities. Arc 1 follows <strong>the</strong> convex proximalcurvatures <strong>of</strong> <strong>the</strong> scaphoid, lunate <strong>and</strong> triquetrum, Arc II outlines<strong>the</strong> distal curvatures <strong>of</strong> <strong>the</strong>se three <strong>bones</strong>, <strong>and</strong> Arc III traces<strong>the</strong> main proximal curvatures <strong>of</strong> <strong>the</strong> capitate <strong>and</strong> <strong>the</strong> hamate. Inaddition to looking for breaks in <strong>the</strong>se arcs, specific fracturesare picked up in specific views. Transverse triquetrum fracturesare easily identified on PA views, but dorsal chip fractures mayneed a slightly oblique, pronated lateral view. A true AP (Roberts)view may be needed to outline <strong>the</strong> body <strong>of</strong> <strong>the</strong> trapezium withoutsuperimposition, while <strong>carpal</strong> tunnel views may sometimes beneeded to identify trapezium ridge fractures as well as pisiforminjuries <strong>and</strong> fractures <strong>of</strong> <strong>the</strong> hamate hook. The pisiform is alsowell evaluated by a lateral view with <strong>the</strong> forearm in 30 degreessupination. Injuries to <strong>the</strong> hamate <strong>and</strong> <strong>the</strong> capitate are usuallyeasily identified by <strong>the</strong> PA or AP views. If a lucent line isvisualized in <strong>the</strong> neck <strong>of</strong> <strong>the</strong> capitate, <strong>the</strong> lateral view should beexamined carefully to identify <strong>the</strong> head <strong>of</strong> <strong>the</strong> bone, to assessPb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200925
Dhillon et alfor displacement or rotation. A trapezoid dislocation/ fracturecan be best visualized on <strong>the</strong> AP view as loss <strong>of</strong> normalrelationship between <strong>the</strong> 2 nd meta<strong>carpal</strong> <strong>and</strong> <strong>the</strong> trapezoid.Special situations may need tomography or even MRI fordetection <strong>of</strong> occult fractures <strong>and</strong> chondral injuries. Hamate hookfractures can be best defined by CT scans, but care must betaken not to confuse <strong>the</strong> Os hamulus proprium, a separatelyossified hook, as a fracture.Management <strong>of</strong> injuries <strong>of</strong> <strong>the</strong> lesser carpusIsolated <strong>carpal</strong> injuries, if undisplaced, are all similarly treatedby a regimen <strong>of</strong> POP cast support for a period <strong>of</strong> 6 weeks.Closed treatment also suffices for a variety <strong>of</strong> <strong>dislocations</strong> aswell as displaced fractures, when satisfactory reduction can beachieved by a finger trap apparatus <strong>and</strong> good muscle relaxation,followed by direct manipulation. Operative intervention isrequired only in a few special situations:Triquetrum : Chip fractures <strong>of</strong>ten do not heal, needing excision<strong>of</strong> <strong>the</strong> fragment as well as ligament repair. Triquetral orientationmust be carefully scrutinized if <strong>the</strong>re is doubt about volarligament injury. Osteonecrosis does not usually occur as <strong>the</strong>fracture are mostly undisplaced, <strong>and</strong> <strong>the</strong>re is a good bloodsupply from <strong>the</strong> extensive ligamentous attachments.Pisiform : This is a sesamoid in <strong>the</strong> tendon <strong>of</strong> <strong>the</strong> flexorcarpi ulnaris, <strong>and</strong> is <strong>the</strong> contact point for stabilizing <strong>the</strong>h<strong>and</strong> in precise movements. Occasional excision <strong>of</strong> afragment is necessary if splinting does not help; althoughosteonecrosis has not been reported, <strong>the</strong> potential for latearthrosis as well as instability is present if <strong>the</strong>re is associatedligament disruption.Hamate : Body fractures heal well with splinting, but fractures<strong>of</strong> <strong>the</strong> hook usually need operative intervention. Open reductionhas its proponents 6 but <strong>the</strong> success rates are not reproducible.Excision <strong>of</strong> <strong>the</strong> hook has given good results in many series;tendon fraying or even rupture could occur secondary tononunion <strong>of</strong> <strong>the</strong> hamate hook, as well as <strong>the</strong> frequentlyassociated problem <strong>of</strong> ulnar neuropathy involving <strong>the</strong> deepbranch <strong>of</strong> <strong>the</strong> nerve. In late cases, mild discomfort couldnever<strong>the</strong>less persist.Trapezium : Surgical options include primary internal fixationwith K wires or <strong>the</strong> late excision <strong>of</strong> a chip fracture if it causespain. In primary reductions, <strong>the</strong> size <strong>of</strong> <strong>the</strong> fragment as well as<strong>the</strong> joint stability are important determinants in decisionmaking.Trapezoid : Being <strong>the</strong> keystone <strong>of</strong> its arc, long term problemslike wrist pain may occur due to arthrosis <strong>of</strong> <strong>the</strong> 2nd CM joint;this may sometimes need arthrodesis. Osteonecrosis has neverFig 1. Fracture proximal pole <strong>of</strong> Capitate in a complex wrist instabilityinjurybeen recorded with fractures, but since dislocation is morecommon, has been occasionally been reported.Capitate : Although cast support is <strong>the</strong> recommended treatmentfor undisplaced fractures, non union is common. Largerfragments may even reabsorb with non-union, leading to latecollapse <strong>and</strong> overriding. As <strong>the</strong> proximal fragment is almosttotally articular, osteonecrosis is also a frequent problem. Thisinjury should preferably be treated by open reduction <strong>of</strong> <strong>the</strong>larger fragments. Late arthrosis may need limited inter<strong>carpal</strong>fusion.Lunate fractures : These are injuries which are frequentlyunrecognized <strong>and</strong> may only present when <strong>the</strong>y becomesymptomatic as Kienbock’s disease. This produces significantdisability in relatively young people, with no totally reliabletreatment option. Lunate injuries are usually missed initiallydue to various reasons: <strong>the</strong> patient may ignore it as a simplesprain, or <strong>the</strong> doctor may not be able to pick up an occultfracture line in x-rays (like sometimes seen in <strong>the</strong> scaphoid).Most times, <strong>the</strong> vascularity <strong>of</strong> <strong>the</strong> bone is disrupted, leading tolate sclerosis <strong>and</strong> osteochondral collapse.Most cases with lunate fractures have a history <strong>of</strong>a hyper extension injury; occasionally repetitive use <strong>of</strong> <strong>the</strong>wrist may cause a sudden “snap”. A proximally directed forcepushes <strong>the</strong> capitate against <strong>the</strong> palmar pole <strong>of</strong> <strong>the</strong> lunate, <strong>and</strong>also shifts <strong>the</strong> lunate ulnarwards; this stresses <strong>the</strong> radio-lunateligament. Avulsion fractures on <strong>the</strong> dorsum occur by pull <strong>of</strong><strong>the</strong> scapho-lunate ligament, while avulsion fractures <strong>of</strong> <strong>the</strong>palmar pole are usually associated with a perilunar dislocationvariant.Pb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200926
<strong>Fractures</strong> <strong>and</strong> <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> <strong>carpal</strong> <strong>bones</strong> – a reviewFig 2. Incomplete Fracture <strong>of</strong> Lunate. Note osteolytic areaFig 3. MRI confirms <strong>the</strong> articular breakMost fresh fractures are ei<strong>the</strong>r palmar or dorsal hornavulsions, more commonly from <strong>the</strong> radial corner; bodyfractures, occurring most <strong>of</strong>ten between <strong>the</strong> mid <strong>and</strong> palmarthirds, are usually in <strong>the</strong> coronal plane. A fracture in <strong>the</strong> sagittalplane maybe seen in ulnar minus wrists, where <strong>the</strong> radio-ulnardifferential step may have an important role to play. Thesefractures may also be fragmented injuries, <strong>and</strong> <strong>the</strong> differentiationfrom <strong>the</strong> late fragmentation <strong>of</strong> Kienbock’s disease is usually aproblem.Radiographic assessment is usually difficult due to <strong>the</strong>overlap <strong>of</strong> <strong>the</strong> surrounding <strong>bones</strong> in both AP <strong>and</strong> lateral views,which may hide a non displaced crack fracture. Clinicalsuspicion must take precedence over x-ray films, <strong>and</strong> insuspected cases, technetium bone scans or even MRI couldbe helpful in <strong>the</strong> early stages. Oblique views will pick up somefractures, but CT scans <strong>and</strong> polyaxial tomograms are perhaps<strong>the</strong> best. MRI is <strong>the</strong> best modality for evaluating vascularchanges. Special note should be made on radiographs <strong>of</strong> <strong>the</strong><strong>carpal</strong> collapse, if any.Treatment : It is important to underst<strong>and</strong> that a lunate fracturemay progress to <strong>carpal</strong> instability, non union <strong>and</strong> late AVN. Allfractures treated with POP casts should have serial follow-upwith tomography <strong>and</strong> even MRI. If <strong>the</strong> fragments are separatedby intrusion <strong>of</strong> <strong>the</strong> capitate, union is impossible. Open reduction<strong>and</strong> fixation is a possibility, but no large studies are available toprove <strong>the</strong> efficacy; distraction with an external fixator could<strong>the</strong>oretically allow cooptation <strong>of</strong> <strong>the</strong> lunate fragments. All POPcasts should be long arm types, with compression over <strong>the</strong>lunate.The treatment <strong>of</strong> established AVN is to be done on <strong>the</strong>lines <strong>of</strong> Kienbock’s disease.The prognosis, <strong>of</strong> body fractures, with minimaldisplacement, is relatively good, especially in younger ages.Non union is rare, as most cases will progress to Kienbock’sdisease.SCAPHOID FRACTURESThe most common, <strong>and</strong> also <strong>the</strong> most problematic, fracture in<strong>the</strong> wrist is that <strong>of</strong> <strong>the</strong> <strong>carpal</strong> scaphoid. It accounts for 70% <strong>of</strong>all <strong>carpal</strong> fractures <strong>and</strong> is most prevalent in <strong>the</strong> 15- to 30-yearoldpopulation 2 . The scaphoid bone has an irregular shape,<strong>and</strong> 80% <strong>of</strong> <strong>the</strong> surface is covered by articular cartilage. Bloodsupply to <strong>the</strong> scaphoid has been well documented by Panagiset al 11 , who have shown that dorsal vessels supply 70% to 80%<strong>of</strong> vascularity, <strong>the</strong> majority <strong>of</strong> which enters at <strong>the</strong> dorsal ridge<strong>of</strong> <strong>the</strong> scaphoid. Because <strong>of</strong> <strong>the</strong> vascular anatomy, proximalpole fractures have a worse prognosis for healing than moredistal injuries.When examining a patient with a suspected scaphoidinjury, it is important to compare <strong>the</strong> injured wrist with <strong>the</strong>uninjured wrist. The classic hallmark <strong>of</strong> an anatomicsnuffbox tenderness on examination if a highlysensitive (90%) indication <strong>of</strong> scaphoid fracture, but it isnonspecific (specifically, 40%) 12 . There are variousimaging options for assessing a patient with suspectedscaphoid injury. They include plain radiographs,Magnetic resonance imaging (MRI) <strong>and</strong> <strong>bones</strong>cintigraphy. Anteroposterior, lateral <strong>and</strong> obliqueradiographic views are required for evaluation <strong>of</strong> a scaphoidfracture.Pb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200927
Dhillon et alFig 4. Fracture across scaphoid waist showing sclerotic lineOccasionally, a special radiograph called a scaphoid viewmay be helpful; <strong>the</strong> wrist is ulnarly deviated <strong>and</strong> extended while<strong>the</strong> film is shot from a dorsal-volar angle.Historically, <strong>the</strong> bone scan has been used to look for occultfractures <strong>of</strong> <strong>the</strong> scaphoid <strong>and</strong> o<strong>the</strong>r <strong>bones</strong>. In a studycomparing bone scan with MRI, 13 <strong>the</strong> authors found <strong>the</strong> twomethods to be equivalent. In this study, 59 patients with clinicalsuspicion <strong>of</strong> scaphoid fracture <strong>and</strong> negative radiographs atpresentation had a bone scan <strong>and</strong> MRI. Both methods foundall fractures, but <strong>the</strong> MRI found some significant ligamentous<strong>and</strong> <strong>carpal</strong> instabilities. A Cochrane review 14 <strong>of</strong> <strong>the</strong> data foundthat bone scintigraphy was a cost effective <strong>and</strong> accuratemethod for assessing occult scaphoid fractures compared withrepeat plain radiography.Fig 5. Fracture <strong>of</strong> scaphoid tuberosity, with step in distal articularsurface, best seen in oblique viewFig 6. Same case, MRI findingsInternal fixation should be regarded as <strong>the</strong> treatment <strong>of</strong>choice for all proximal pole fracture 15,16 . In contrast to fracturesthrough <strong>the</strong> waist, which can be classified as stable or unstableaccording to <strong>the</strong> amount <strong>of</strong> displacement <strong>and</strong> <strong>the</strong> direction <strong>of</strong><strong>the</strong> fracture line, all proximal pole fractures should be regardedas unstable, whe<strong>the</strong>r or not <strong>the</strong>y are displaced, for <strong>the</strong> reasonsmentioned above. It is essential that <strong>the</strong> fracture is completelyimmobilized in order to optimize <strong>the</strong> conditions forrevascularization <strong>and</strong> healing. This is difficult, if not impossible,to achieve with external splintage alone, because <strong>the</strong>re is noextrinsic ligamentous support around <strong>the</strong> proximal part <strong>of</strong> <strong>the</strong>scaphoid, which without doubt explains why proximal polefractures have such high rates <strong>of</strong> nonunion. Internal fixation isbest carried out through a dorsal approach, using anintraosseous fixation device appropriate to <strong>the</strong> small size <strong>of</strong> <strong>the</strong>proximal fragment. The dorsal approach provides limited accesswith partial opening <strong>of</strong> <strong>the</strong> second <strong>and</strong> third extensorcompartments <strong>and</strong> <strong>the</strong> wrist capsule over <strong>the</strong> scapholunatejoint. It does not cause any fur<strong>the</strong>r compromise to <strong>the</strong> bloodsupply <strong>of</strong> <strong>the</strong> proximal fragment <strong>and</strong> allows clear visualization<strong>of</strong> <strong>the</strong> fracture <strong>and</strong> exact placement <strong>of</strong> <strong>the</strong> screw 16 . Thereis no real advantage to percutaneous insertion as noligaments are incised with <strong>the</strong> open technique <strong>and</strong> <strong>the</strong> risk <strong>of</strong>incorrect positioning <strong>of</strong> <strong>the</strong> screw increases with <strong>the</strong> closedtechnique.The mini-Herbert screw, which has a shank diameter <strong>of</strong>1.5mm <strong>and</strong> small threads, can be easily inserted under directvision into <strong>the</strong> small proximal fragment using a freeh<strong>and</strong>technique. The small size <strong>of</strong> this screw minimizes <strong>the</strong> risk <strong>of</strong>displacement <strong>and</strong> disruption <strong>of</strong> <strong>the</strong> small proximal fragmentduring fixation <strong>and</strong> allows <strong>the</strong> screw to be buried beneath <strong>the</strong>cartilage. The wrist is immobilized postoperatively for 2 weeksPb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200928
<strong>Fractures</strong> <strong>and</strong> <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> <strong>carpal</strong> <strong>bones</strong> – a reviewin a below elbow cast <strong>and</strong> heavy manual activity is restrictedduring <strong>the</strong> first 6 weeks. Full activities are resumed once X-rays demonstrate fracture union. This treatment regime has ahigh success rate in our h<strong>and</strong>s, even for proximal pole fractureswhich present up to 4 months following <strong>the</strong> injury.COMPLICATIONS OF CARPAL BONE INJURIES1. Refracture: rare, commoner with scaphoid than o<strong>the</strong>r <strong>bones</strong>2. Nerve Injury: more common with <strong>dislocations</strong>; usuallydirect injury or stretching. Median nerve commonly injuredin lunate dislocation, but fractures <strong>of</strong> pisiform <strong>and</strong> hamatehook could injure ulnar nerve also.3. Nonunion: May occur as maintaining immobility is aproblem, <strong>and</strong> early diagnosis is frequently lacking. Willalways need open reduction <strong>and</strong> bone graft to regain <strong>carpal</strong>height.4. Pain dysfunction syndrome: Could be associated with any<strong>carpal</strong>/wrist trauma.DISLOCATIONS OF THE CARPAL BONESAcute fracture-<strong>dislocations</strong> <strong>of</strong> <strong>the</strong> carpus are uncommoninjuries. Although <strong>carpal</strong> bone <strong>dislocations</strong> have beenrecorded for many years, <strong>the</strong> mechanisms <strong>and</strong> classificationhave only been recently clarified. These are complex injuries,with specified patterns <strong>of</strong> trauma. Most <strong>carpal</strong> <strong>dislocations</strong> arecaused by hyper extension trauma, with fall being <strong>the</strong>commonest mechanism. As per <strong>the</strong> simplest explanation, <strong>the</strong>primary dislocation occurs at <strong>the</strong> mid<strong>carpal</strong> joint, with <strong>the</strong>capitate usually displaced dorsal to <strong>the</strong> lunate. As <strong>the</strong>scaphoid bridges both <strong>the</strong> rows, it may ei<strong>the</strong>r fracture or rotatewhen <strong>the</strong> capitate dislocates dorsally. This leads toligamentous instability, <strong>and</strong> if <strong>the</strong> injury stops at thisstage, it is classified as a Perilunate dislocation(transscaphoid, or if <strong>the</strong>re is no fracture, simple perilunatedislocation). The same mechanism may occur with a volarlydirected force, leading to Volar Perilunate <strong>dislocations</strong>.Previously a lunate dislocation was thought to be an isolatedinjury, but now this is understood to be <strong>the</strong> end result <strong>of</strong> aperilunate injury, where <strong>the</strong> dislocated carpus, on relocation,pushes <strong>the</strong> lunate from its position. As in all ligamentousinjuries, <strong>the</strong>re is a spectrum <strong>of</strong> damage in <strong>the</strong>se injuries, rangingfrom partial tears to total disruption <strong>of</strong> <strong>the</strong> complex ligamentousstructures. These are <strong>the</strong> so called wrist instabilities, whichpresent as inter<strong>carpal</strong> segmental dissociations, <strong>and</strong> are aseparate entity in <strong>the</strong>mselves. Broadly speaking, <strong>the</strong> keydistinctions from management point <strong>of</strong> view are whe<strong>the</strong>r <strong>the</strong>scaphoid is fractured or subluxated, <strong>and</strong> whe<strong>the</strong>r <strong>the</strong>displacement <strong>of</strong> <strong>the</strong> distal row is dorsal or volar.TABLE 11. Dorsal perilunate/volar lunate dislocation2. Dorsal trans scaphoid perilunate dislocation3. Volar perilunate/dorsal lunate dislocation4. VARIANTSTransradial styloid, perilunateNaviculocapitate syndromeTranstriquetralMiscellaneous5. Isolated rotary scaphoid subluxationAcute subluxationRecurrent subluxation6. Total dislocation <strong>of</strong> <strong>the</strong> scaphoid7. Isolated <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> lesser <strong>carpal</strong> <strong>bones</strong>The list <strong>of</strong> potential <strong>dislocations</strong> is given in Table 1.Dorsal Perilunate/ Volar Lunate dislocationPatients with perilunate fracture-<strong>dislocations</strong> usually presentwith wrist pain, swelling, <strong>and</strong> crepitus. The digits <strong>of</strong>ten areheld in a semiflexed position, <strong>and</strong> passive extension is painful.There also is abnormal wrist alignment with <strong>the</strong> capitatedisplaced dorsally, which can be apparent on clinicalexamination. These patients usually also complain <strong>of</strong>pares<strong>the</strong>sias in <strong>the</strong> median nerve distribution. Radiographicevaluation is important to evaluate <strong>the</strong> extent <strong>of</strong> injury. Ofperilunate injuries, 20% are misdiagnosed with <strong>the</strong> initialradiographic evaluation. This is best diagnosed on lateral x-rays; <strong>the</strong> capitate is seen dorsal to <strong>the</strong> lunate, with <strong>the</strong> proximalscaphoid pole being rotated dorsally. AP views demonstrateoverlap between <strong>the</strong> proximal <strong>and</strong> distal <strong>carpal</strong> rows. In caseswhere <strong>the</strong> deforming forces have relocated <strong>the</strong> distal row, <strong>the</strong>lunate will be seen volarly, <strong>and</strong> will be rotated 90 degrees on<strong>the</strong> lateral x-ray (“Spilled tea-cup” sign). The capitate may partlyarticulate with <strong>the</strong> distal radius. In AP views <strong>the</strong> shape <strong>of</strong> <strong>the</strong>lunate becomes triangular or wedge shaped, as compared to<strong>the</strong> normal trapezoidal shape. An additional posteroanteriorradiograph <strong>of</strong> <strong>the</strong> wrist with a loaded fist is made to rule outscapholunate instability. The presence <strong>of</strong> associated fracturesmay divert <strong>the</strong> attention <strong>of</strong> physicians away from <strong>the</strong> <strong>carpal</strong>subluxations or <strong>dislocations</strong>. Distraction radiographs are helpfulto identify scaphocapitate syndrome or to delineate any o<strong>the</strong>rassociated fracture or dislocation that was not apparent at <strong>the</strong>first evaluation. Tomography <strong>of</strong> <strong>the</strong> wrist is useful for evaluating<strong>the</strong> alignment <strong>of</strong> <strong>the</strong> <strong>carpal</strong> <strong>bones</strong> <strong>and</strong> for assessing fracturesPb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200929
Dhillon et al<strong>and</strong> fracture- <strong>dislocations</strong>. It also provides useful crosssectionalimages <strong>and</strong> is particularly helpful if three-dimensionalreconstruction is performed.Traditional treatment <strong>of</strong> <strong>carpal</strong> <strong>dislocations</strong> or fracture<strong>dislocations</strong> in <strong>the</strong> acute stages include reduction with fingertrap traction, open reduction <strong>and</strong> internal fixation <strong>of</strong> fractures<strong>and</strong> primary capsular <strong>and</strong> ligament repair followed by castimmobilization for a period <strong>of</strong> 10±12 weeks. 6,17,18 . This is <strong>the</strong>st<strong>and</strong>ard protocol preferred by <strong>the</strong> authors 5 for <strong>the</strong> so-calledsimple <strong>dislocations</strong> <strong>the</strong>se being: <strong>the</strong> transscapho-perilunar<strong>dislocations</strong> seen early <strong>and</strong> <strong>the</strong> perilunar <strong>dislocations</strong> with orwithout complete dislocation <strong>of</strong> one <strong>carpal</strong> bone. These twolast injury patterns correspond to stages I±IV <strong>of</strong> Mayfield’sprogressive perilunar instabilities <strong>of</strong> <strong>the</strong> “lesser arc” 19 .Open reduction can be done through <strong>the</strong> dorsal approach,or a combined dorsal <strong>and</strong> volar one 20 . The authors prefer atransverse dorsal skin incision, with a longitudinal incision in<strong>the</strong> capsule. This gives adequate exposure to reduce <strong>the</strong> lunateas well as fix <strong>the</strong> scaphoid; volar ligamentous repair however isnot possible through this incision, but we have had nosubsequent instability in our experience. It is important tounderst<strong>and</strong> that restoration <strong>of</strong> <strong>the</strong> relationship between <strong>the</strong>scaphoid, lunate <strong>and</strong> capitate is essential; this should bemaintained with k-wires. In trans-scaphoid injuries, <strong>the</strong> proximalpole <strong>of</strong> <strong>the</strong> scaphoid is displaced with <strong>the</strong> lunate, <strong>and</strong> this hasto be reduced <strong>and</strong> fixed with a screw. The inter<strong>carpal</strong> k-wiresshould be left for a minimum <strong>of</strong> 8 weeks to prevent late lunatesubluxation <strong>and</strong> allow inter<strong>carpal</strong> ligamentous healing. A longarm POP cast should also be continued till this time.ROLE OF EXTERNAL FIXATORS IN THE MANAGEMENTOF CARPAL FRACTURE-DISLOCATIONSFor <strong>the</strong> so-called complex fracture <strong>dislocations</strong> represented by:(a) injuries to <strong>the</strong> “greater arc” with fracture <strong>of</strong> two or more<strong>carpal</strong> <strong>bones</strong>, (b) complete irreducible palmar <strong>dislocations</strong>associated with intraarticular fractures <strong>of</strong> <strong>the</strong> distal radius, <strong>and</strong>(c) open <strong>carpal</strong> injuries, a wrist fixator is routinely used. This isnot only as a means to obtain indirect reduction byligamentotaxis, but also for protective immobilization using <strong>the</strong>frame in a neutralizing mode to block <strong>the</strong> axial load <strong>of</strong> <strong>the</strong> cartilageon <strong>the</strong> injured proximal <strong>carpal</strong> row, <strong>and</strong> to maintain normal <strong>carpal</strong>alignment during <strong>the</strong> initial stages <strong>of</strong> ligament healing 21,22 .Subsequently, external fixation was found particularly usefulin <strong>the</strong> treatment <strong>of</strong> <strong>carpal</strong> <strong>dislocations</strong> with ipsilateral fractures<strong>of</strong> <strong>the</strong> upper extremity, especially forearm <strong>and</strong> elbow fractures.This permits cast free after treatment, providing earlyrehabilitation <strong>of</strong> forearm rotation <strong>and</strong> elbow motion. Fur<strong>the</strong>rindications for external fixation include <strong>the</strong> old neglectedunreduced transscaphoperilunate <strong>dislocations</strong>, as well as <strong>the</strong>compression fracture <strong>of</strong> <strong>the</strong> lunate as a result <strong>of</strong> an axiallydirected force on <strong>the</strong> proximal row.External fixation <strong>of</strong> <strong>the</strong> wrist as a method <strong>of</strong> immobilization<strong>of</strong> <strong>carpal</strong> fracture <strong>dislocations</strong> was proposed in 1980 by Ballmer<strong>and</strong> Buchler (personal communication). It could be shown that<strong>the</strong> principle <strong>of</strong> ligamentotaxis using an external fixator across<strong>the</strong> wrist was not only useful to restore <strong>the</strong> joint surface <strong>of</strong> <strong>the</strong>distal radius 21, 22, 23 but also to reduce <strong>and</strong> maintain <strong>carpal</strong>alignment in difficult <strong>carpal</strong> fracture <strong>dislocations</strong> 24 .External fixation greatly facilitates both exposure <strong>and</strong>reduction <strong>of</strong> dislocated <strong>carpal</strong> <strong>bones</strong>. The constant distractingforce <strong>of</strong> <strong>the</strong> external fixator frees <strong>the</strong> surgeon intraoperativelyfrom <strong>the</strong> continuous struggle to move <strong>the</strong> distal <strong>carpal</strong> “out <strong>of</strong><strong>the</strong> way”, allowing him to concentrate his efforts on <strong>the</strong> properrealignment, internal fixation, <strong>and</strong> bone grafting <strong>of</strong> <strong>the</strong>dislocated or fractured <strong>bones</strong>. The frame should be used during<strong>the</strong> operation as a distraction device, to allow indirect reduction,but after completion <strong>of</strong> bone <strong>and</strong> ligament reconstructiondistraction should be reduced allowing <strong>the</strong> fixator to functiononly as a neutralization frame. Thus normal <strong>carpal</strong> alignment ismaintained protecting <strong>the</strong> ligament repair especially at <strong>the</strong>scapholunate junction during <strong>the</strong> first 8±10 weeks. Fur<strong>the</strong>rmore,<strong>the</strong> use <strong>of</strong> a fixator has <strong>the</strong> advantage over conventionaltechniques, because it permits unrestricted, cast-free early activeforearm rotation <strong>and</strong> elbow motion in cases in which <strong>the</strong> <strong>carpal</strong><strong>dislocations</strong> are associated with ipsilateral forearm or elbowfractures.CONCLUSIONSIn conclusion, this review is presented to increase <strong>the</strong>awareness <strong>of</strong> this complex problem; even today we are seeingwrist injuries which had been missed at initial presentation.This is most probably due to a lack <strong>of</strong> awareness <strong>of</strong> this problemamong <strong>the</strong> general orthopaedic surgeons.REFERENCES1. Cooney WP, Linscheid RL, Dobyns JH. <strong>Fractures</strong> <strong>and</strong> <strong>dislocations</strong><strong>of</strong> <strong>the</strong> wrist.In: Rockwood <strong>and</strong> Green’s <strong>Fractures</strong> in Adults, LippincottRaven Publishers, Philadelphia, 1996: pp 745-80.2. Gutierrez G. Office management <strong>of</strong> Scaphoid fractures. Phys SportsMed 1996; 24:60-70.3. Greene WB. Essentials <strong>of</strong> musculoskeletal care. 2nd ed. Rosemont,Illinois, American Academy <strong>of</strong> <strong>Orthopaedic</strong> Surgeons, 2001: pp252-54.4. Fisk GR: Carpal instability <strong>and</strong> <strong>the</strong> fractured scaphoid. Ann R. CollSurg Engl.46; 63-73, 19705. Mayfield JK, Johnson RP, Kilcoyne RK. Carpal <strong>dislocations</strong>:Pathomechnaics <strong>and</strong> progressive perilunar instability. J H<strong>and</strong> SurgPb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200930
<strong>Fractures</strong> <strong>and</strong> <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> <strong>carpal</strong> <strong>bones</strong> – a review[Am] 1980; 5: 226-41.6. O’Brien ET. Acute fracture <strong>and</strong> <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> carpus. OrthopClin N Am 1984; 15:237-58.7. Stein F, Siegel MW. Naviculocapitate fracture syndrome: a casereport <strong>and</strong> new thoughts on <strong>the</strong> mechanism <strong>of</strong> injury. J Bone JointSurg 1969; 51-A:391.8. Cordrey LJ, Ferrer-Torrels M: Management <strong>of</strong> fractures <strong>of</strong> <strong>the</strong>greater multangular. J Bone Joint Surg 1960; 42-A, 1111-18.9. Vasilas A, Gireco RV, Bartone NF. Roentgen aspects <strong>of</strong> injuries to<strong>the</strong> pisiform bone. J Bone Joint Surg. 42-A; 1317, 196010. Gilula LA. Carpal injuries: Analytic approach <strong>and</strong> case exercises.Am J Roentgenol 1979; 133:503-17.11. Panagis JS, Gelberman RH, Taleisnik J, Baumgaertner M. The arterialanatomy <strong>of</strong> <strong>the</strong> human carpus. Part II: The intraosseous vascularity.J H<strong>and</strong> Surg [Am] 1983; 8:375-82.12. Freel<strong>and</strong> P. Scaphoid tubercle tenderness: a better indicator <strong>of</strong>scaphoid fractures? Arch Emerg Med 1989; 6:46-50.13. Gutierrez G. Office management <strong>of</strong> Scaphoid fractures. Phys SportsMed 1996; 24:60-70.14. Tiel-van Buul MM, Broekhuizen TH, Van Beek EJ, Bossuyt PM.Choosing a strategy for <strong>the</strong> diagnostic management <strong>of</strong> suspectedscaphoid fracture: a cost-effectiveness analysis. J Nucl Med 1995;36:45-48.15. Herbert TJ. The fractured scaphoid. Quality Medical Publishing, St.Louis, 1990: pp 57.16. Rettig ME, Raskin KB. Retrograde compression screw fixation <strong>of</strong>acute proximal pole scaphoid fractures. J H<strong>and</strong> Surg [Am] 1999;24:1206-1210.17. Panting AL, Lamb OW, Noble J et al. Dislocations <strong>of</strong> <strong>the</strong> lunatewith or without fractures <strong>of</strong> <strong>the</strong> scaphoid. J Bone Joint Surg 1984;66-B:391-95.18. Worl<strong>and</strong> RL, Dick HM. Transnavicular perilunate <strong>dislocations</strong>. JTrauma 1975; 15;407-12.19. Monheim MS, H<strong>of</strong>mann KE, Omer GE. Transscaphoid perilunatefracture dislocation. Results <strong>of</strong> open reduction <strong>and</strong> internal fixation.Clin Orthop 1984; 190: 227.20. Green DP, O’Brien ET. Classification <strong>and</strong> Management <strong>of</strong> <strong>carpal</strong><strong>dislocations</strong>. Clin Orthop 1980; 149:55-72.21. Fern<strong>and</strong>ez DL, Jakob RP, Buchler U. External fixation <strong>of</strong> <strong>the</strong> wrist.Current indications <strong>and</strong> technique. Ann Chir Gyn 1983; 72:298-302.22. Fern<strong>and</strong>ez DL, Ghillani R. External fixation <strong>of</strong> complex <strong>carpal</strong><strong>dislocations</strong>: a preliminary report. J H<strong>and</strong> Surg [Am] 1984; 12:335-47.23. Jakob RP, Fern<strong>and</strong>ez DL. The treatment <strong>of</strong> wrist fractures with <strong>the</strong>small AO external fixation device. In: Uhth<strong>of</strong>f HK, ed. Currentconcepts <strong>of</strong> external fixation <strong>of</strong> fractures, Spriner Verlag, Berlin,1982; pp 307-14.24. Cooney WP, Bussey U, Dobyns JH, Linscheid RL. Difficult wristfractures: Perilunate fracture <strong>dislocations</strong> <strong>of</strong> <strong>the</strong> wrist. Clin Orthop1987; 214:136-47.Pb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-XI, No.1, 200931