PARATHYROID AND THYROID IMAGING - Neuroradiology
PARATHYROID AND THYROID IMAGING - Neuroradiology
PARATHYROID AND THYROID IMAGING - Neuroradiology
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
HEAD <strong>AND</strong> NECK <strong>IMAGING</strong> 1052-5149/96 $0.00 + .20<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong><strong>THYROID</strong> <strong>IMAGING</strong>David M. Yousem. MD<strong>PARA<strong>THYROID</strong></strong> <strong>IMAGING</strong>Imaging of the parathyroid glands revolvesaround the detection of parathvroid adenomas andhyperplastic parathyroid glands in the setting oIprimary hyperparathyroidism. Arguments for andagainst imaging and which imaging modality touse have been hotly debated in the radiologic andsurgical literature.Anatomy and lmagingThe parathyroid glands are derived from the third(lower parathyroid glands) and fourth (upper parathyroidglands) pharyngeal pouches. Whereas themajority of people have four glands (a pair at theupper and lower poles of the thyroid gland),25%of individuals have more than this number.3e,a0 Althoughthe parathyroid glands may be aberrantlylocated anywhere from the carotid bifurcation to theanterior mediastinum, inferior migration of thoseglands derived from the third pharyngeal pouchoccurs most frequently.3t Of the two dominant celltypes in the parathyroid glands, the chief cells andthe oxyphil cells, the former are the predominantsource of parathormone.Vascular supply to the parathyroid glands is usuallythrough the superior and inferior thyroidal arteries,with drainage to thyroidal veins. The glandsare innervated through the cervical sympatheticplexus.There are several options for imaging the parathyroidglands; these include ultrasonography, computedtomography (CT), magnetic resonance (MR)imaging, angiography, and nuclear medicine scintigraphy.The advantages and disadvantages o{each of the imaging modalities described are summarizedin Table 1.High frequency (5-10 MHz) ultrasonography isthe least invasive of the imaging modalities usedto search for parathyroid adenomas because it doesnot require intravenous injections of any compounds.Unfortunatelp its accuracy is less than thatof the other modalities mainly because of the difficultyin identifying ectopic parathyroid adenomasthat may occur throughout the neck, behind airfilledstrucfures, or in the anterior mediastinumwhere acoustic impedance by bone or air preventsadequate imaging. Nonetheless, for parathyroid adenomasthat are located in a perithvroidal location.ultrasonography is an excellent imaging choice.CT offers the benefit of cross-sectional imagingfor parathyroid adenoma localization. Because theentire neck from skull base to anterior mediastinumcan be scanned with CT, the possibility of detectingectopic parathyroid adenomas is increased. Distinguishinglymphadenopathy from parathyroid adenomasis a problem encountered with CT (as well aswith ultrasonography and MR imaging). The otherdisadvantage of CT is that it requires the administrationof iodinated intravenous contrast agents.These contrast agents are essential for distinguishingblood vessels from adenomas or lymphadenopathy.Moreover, the use of iodinated contrast agentsprevents subsequent imaging with iodine-based nuclearmedicine agents because of the uptake of contrastby the thyroid gland. It is necessary to wait atleast 6 weeks after contrast-enhanced CT scans toimage the thyroid gland with iodinated nuclearFrom the Departments of Radiology and Otorhinolaryngology-HeadMedical Center, Philadelphia, Pennsylvaniaand Neck Surgery, The University of PennsylvaniaNEURO<strong>IMAGING</strong> CLINICS OF NORTH AMERICAVOLUME 6 . NUMBER 2. i|'{AY'].996435
436 YOUSEMTable 1. ADVANTAGES <strong>AND</strong> DISADVANTAGES OF VARIOUS <strong>IMAGING</strong> MODALITIES FOR DETECTION OF<strong>PARA<strong>THYROID</strong></strong> ADENOMASCTExamination Advantages DisadvantagesMR imagingNuclear medicinescintigraphyUltrasonographyExamines head. neck. and chestEasy detection of calcificationBiopsy capableExamines head. neck. and chestNo iodinated conlrast reouiredExcellent soft tissue discriminationExamines head and neck wellFunctional, not anatomic imagingDistinguishes nodes from adenomasReasonable costExamines neck welllnexoensiveNoninvasiveReal-time, biopsy capableRequires iodinated contrastlodinated contrast affects thyroid imaging by scintigraphyShoulder artifactsDifficulto differentiate node versus adenomaExoensiveDifficulto differentiate node versus adenomaIntravenous gadolinium agent employedRequires patient cooperation, no claustrophobiaVery expensiveLower yield for ectopic glands especially in chestIntrathyroidal masses indistinguishable from adenomasSmaller lesions easily missedExamines head and chest poorlyCannot differentiate nodes and adenomasmedicine agents. Contrast enhancement is not thesolution to parathyroid imaging; only 25% of parathyroidadenomas demonstrate noticeable enhancement.zFalse-negative studies with CT also may occurin the setting of poor-quality images fromshoulder artifacts.MR imaging with gadolinium enhancement is anotheruseful study for evaluating patients with hyperparathyroidism.On T2-weighted scans andpost-gadolinium T1-weighted scans, parathyroidadenomas are bright against a dark, fat-suppressedbackground.3l'36'56'67'76 MR imaging is limited by thedistribution and coverage of the surface coil usedto detect parathyroid adenomas and also by anymotion artifact that may occur during imaging.Nonetheless, with the appropriate surface coil andinstructions to the patient, MR imaging is able toadeouatelv evaluate the entire neck and anteriormediastinum. As with the other modalities listed,the potential for misdiagnosing lymphadenopathyas parathyroid adenomas also exists with MR imaging.The choices for scintigraphic localization of parathgoidadenomas include thallium (Tl)-201-technetium(Tc)-99m pertechnetate subtraction scanning,ee-Tc-sestamibi (hexakis-2-methoxy-isobutylisonitrile)subtraction imaging with iodine-123(I-123) or ehTc pertechnetate, and ee^Tc-sestamibiimaging without subtraction. The subtractiontechnioues allow tracers that are concentrated inthe thyroid gland (pertechnetate and iodine) to besubtracted from those (thallium and sestamibi) thataccumulate in both thyroid glands and parathyroidadenomas. Thallium is a potassium analogue thatmay concentrate in parathyroid adenomas becauseof changes in potassium turnover in active cells.The mechanism for sestamibi uptake is poorly understoodbut may relate to mitochondrial densityin oxyphil cells, blood flow within adenomas, orpotassium turnover.ae'sa Because sestamibi uptake inparathyroid adenomas persists after thyroid glandwashout, it can be used without subtraction techniquesif one performs delayed images. The difficulttask of patient immobilization and accurate superimpositionof subtracted images, required bythallium-pertechnetate studies, is obviated with delayedsestamibi imaging.Of the parathyroid agents, thallium emits lowenergy,low-penetrating 80 keV photons andwashes out of parathyroid adenomas relatively rapidly.ee'Tc-sestamibi has 140 keV photons that penetratethe anterior neck and mediastinal soft tissuesbetter and is concentrated at a higher rate and fora longer time within an adenoma than thallium.ee*Tc-sestamibi, therefore, produces higher signalto-noiseimages than thallium subtraction scans.saSingle-photon emission computed tomography(SPECT) scanning also can be combined with highdoseee'Tc sestamibi scintigraphy for more accurateparathyroid adenoma localization.aeHyperparathyroidismHyperparathyroidism has an incidence of 0.0377oin the United States.28 Patients mav present withthe classic findings of stones (renal laiculi), groans(abdominal pain), bones (demineralization or arthritis),or moans (psychiatric disturbances). Primaryhyperparathyroidism is caused by a solitaryparathvroid adenoma in 80% to 85% of cases.20'21'6a.s+,ss iltp"rplastic parathyroid glands (12-15%),multiple adenomas (2-3E"), and parathyroid carcinoma(
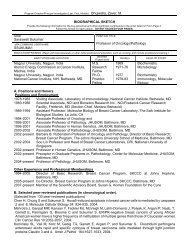
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 437Parathyroid imaging is controversial not onlyfrom the standpoint of the indications for imagingbut also from the issue of which modality (if any)to choose. In most institutions, preoperative localizationof the parathyroid glands by imaging is notperformed before the first surgery (for previouslyoperated patients, see subsequent discussion). Thisstems from the early surgical literature that suggeststhat operative time, morbidity, and mortality is notsignificantly influenced by preoperative localizationof parathyroid adenomas for hyperparathyroidism.7'a6,62 The surgical exploration entails bilateraldissection of the perithyroidal region, emphasizingthe inferior poles, where most parathyroid adenomasoccur. In experienced hands, this surgical procedurecan be performed quickly and accuratelywith success rates of over 90Vo.12'5e,62,65,84 This hasled Doppman84 to state that the best localizationprocedure a patient can obtain for parathyroid adenomasis to locate "an experienced parathyroidsurgeon."Proponents of preoperative localization of parathyroidadenomas even in unoperated cases cite(1) the need for only unilateral dissections when anadenoma is evident on imaging; (2) the identificationof ectopic adenomas preoperatively, allowingbetter planning and patient education; (3) detectionof other head and neck masses that mav reouiretreatment at the same time (e.g., thyroid masies);and (4) the reduction in operating room time, recurrentlaryngeal nerve paralysis, and postoperativehypoparathyroidism when preoperative imaging isperformed.38'43'63'6'86 In two studies bv Russell andtasas and their colleagues, the differ6nce betweenmean operating times with (71 minutes and 135minutes) and without (97 minutes and 180 minutes)preoperative imaging justified the cost of the imagingtest.8'63 The operative success rate also improvedfrom 90% to 1,00Vo with preoperative imaging.8Uden also noted that the time for surgeryand anesthesia decreased with preoperative imaging;however, when a cost-benefit analysis wasperformed, he found that the cost of the imagingprocedure outweighed its benefit.8T A reduction of28 minutes of operating room time in the study byRoe and colleagues did not justify the $901 meancost of localization.62 Other surgeons take a centristposition regarding bilateral or unilateral neck explorations.They perform unilateral neck dissectionsif imaging studies are definitive but convert to bilateralsurgery if (1) imaging is equivocal or showsmultifocal abnormality, (2) more than one enlargedgland is identified at surgery, (3) the patient hasa multiple endocrine neoplasia (MEN) syndrome(often associated with parathyroid hyperplasia), or(4) a unilateral exploration is unrevealing.63When a parathyroid adenoma is not identified ina stereotypical perithyroidal location, the surgeonmay empirically explore the anterior mediastinum,deep cervical space, periesophageal grooves, or carotidsheath region. The yield of surgery in thisscenario is much lower (907osuccess rate), and the surgiial complicationrate increases with such blind exoorations.l2The intrathvroidal parathvroid adenomi. which accountsfor a small'percentage of cases, cannot bereadily distinguished from thyroid adenomas andposes a particularly difficult problem.a5'84 To confusematters further, thyroidal abnormalities occur in asmany as 40% to 48Vo of patients with hyperparathyroidism.la5e. e5 These factors have led lessexperiencedsurgeons and those who have had aIess successful track record to choose preoperativelocalization of parathyroid adenomas.Parathyroid AdenomasExactly how accurate are the imaging studiesfor detecting parathyroid adenomas? On ultrasonography,parathyroid adenomas appear as oval,oblong, or bulbous lesions with echogenicity lessthan that of the thyroid gland (Fig. t;.s0, u Usinghigh-resolution ultrasound in a study of more than150 patients, a sensitivity of 64Vo and specificityof 94Vo for adenomas and hyperplastic glands wasachieved.5e Of those glands greater than 1 g in size,ultrasonography had a detection rate of 95%.se Otherinvestigators also quote sonographic sensitivities ofFigure 1. Ultrasonogram of parathyroid adenoma. Deepto the thyroid tissue, one can see a hypoechoic mass(arrows) representing a parathyroid adenoma.
438 YOUSEM60Va to 707o and specificities in the range of 907a to967a.20,21,36, nWhen Stark and colleagues compared the accuracyof high-resolution CT with ultrasonographyfor detecting parathyroid adenomas, they found thesensitivity of CT to be 70% with a specificity o{90Vo,77 an improvernent over their experience withultrasonography. Sommer and colleagues alsofound CT to be more accurate than ultrasonographyby over 10%; combining the studies yields a detectionrate of 89% in patients without previoussurgery.'"Spritzer and co-workers were among the first toreport on the accuracy of MR imaging (Fig. 2) indetecting parathyroid adenomas.T6 Seventeen patientshad adenomas, and MR imaging correctlyidentified 14 of them (82.3Va). Two false-positiveand three false-negative studies for adenomis werereported; given the possibility of 72 glands, thisyields an MR accuracy of 92% for adenomas.The numerous options for nuclear medicine scanningfor parathyroid adenomas stem from the factthat there are no agents that are exclusively taken upby the parathyroid glands or adenomas. Therefore,agents that are taken up by parathyroid adenomasand the thyroid glands (thallium and ee^Tc sestamibi)must be subtracted from those that are onlytaken up by the thyroid glands (ry*Tc pertechnetateand 123I) (Fig. 3). This then allows visualization ofabnormal uptake by parathyroid adenomas. Computerprocessing is required to enhance accuracywith subtraction techniques.2 At most centers, however,ee^Tc sestamibi imiging is performed withoutsubtraction. Ten to thirtv mCi of ee-Tc sestamibi areinjected with scanning a1 1S-minute intervals for uplo 2 to 4 hours after iniection.aT Because the agentwashes out of the thyroid gland rapidly but iJ retainedby parathyroid (and thyroid) adenomas, de-Iayed images are all that are usually necessary forgood localization (Fig. 4).It is not necessary to sacrifice accuracy with thesimpler sestamibi study. The overall sensitivity ofthallium-ee'Tc pertechnetate subtraction scintigraphyfor parathyroid adenoma detection (75-85Vo1z'szis substantially less than that of ee'Tc sestamibi,which runs in the range of 90% to 100%.2e,33,53.54.80No thallium-positive adenomas have been sestamibi-negativeto date. Furthermore, in a comparativestudy of nonoperated patients, Kneeland andcolleagues found scintigraphy (82Vo) to have highersensitivity rate than MR imaging (74%), CT (74%),and ultrasonography (59%).36 The differences wereonly statistically significant between scintigraphyand ultrasonography.When Price reviewed the presestamibi literatureup until 1993 Q43 to 1785-cases). he found thatMR imaging had the highest sensitivity rate for thedetection of adenoma (74%) followed by nuclearmedicine studies (72%), CT (65%), and ultrasonography(63%).58 The false-positive rate of nuclearmedicine (.1.Vo) was lowest compared with MR imaging(14%), CT (16Vo), and ultrasono graphy (187").Sestamibi data over the past 2 years suggest thatit surpasses all other techniques in sensitivity andaccuracy. Unfortunately, the high rate of thyroidabnormalities (40-487") that coexist with parathyroidadenomas may lead to false-positive scintigrams because thyroid lesions may concentrate radiotracersto the same degree as parathyroidadenomas.as,53,sa Reports of ee*Tc sestamibi uptakein thyroid cancers and their nodal and distant metastasesignal the possibility for false-positive studles.'' '"Parathyroid Hype rplasiaApproximately 30% of patients with parathyroidhyperplasia have familial hyperparathyroidism, includingvariants of the multiple endocrine neoplasia(MEN) syndromes (Table 2). As noted earlier, hy-Figure 2. A and B, MR images of parathyroid adenoma. A, A small soft tissue nodule (arror,rr) is seenadjacent to the trachea located below the thyroid gland on the right side. This was a parathyroidadenoma in a low perithyroidal location. A After gadolinium injection, the lesion (arrow'1 enhances avidly.
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 439..'4.:;:-',1. i" .,*Figure 3. Thallium subtraction study. The thallium scan (top left) can be sequentially subtracted fromthe technetium pertechnetate scan of the thyroid gland (fop right). On the lower set of images, notehow the thyroid gland uptake is eliminated allowing visualization of the inferior pole parathyroid adenomaon the left (arrows\.Figure 4. A and B, se'Tc sestamibi scan of a parathyroid adenoma. A, Initial technetium-ggm sestamibiscan of the parathyroid region demonstrates uptake in the thyroid gland and parathyroid adenoma(arrows)" B, On delayed imaging, the thyroid uptake has washed out, whereas the parathyroid adenoma(arrow\ has persistentracer accumulation.
440 YOUSEMTable 2. MULTIPLE ENDOCRINE NEOPLASTA (MEN) SyNDROMESFeature MEN I MEN IIA MEN IIBEponymParathyroid abnormalityThyroid lesionPituitary lesionsPheochromocytomaOther manifestationsChromosomalinkageWermerHyperparathyroidism (90%)due to hyperplasia morecommonly than adenomaGoiter, adenomas,thyroiditis are rareAdenomas (20-30"/.)NoPancreatic islet celladenomas (insulinoma orgastrinoma) 30-35%Adrenal codex adenomasor carctnomasRarely glucagonomas,VlPomas, carcinoidZollinger-Ellison syndromeA-D chromosome 11SippleParathyroid hyperplasia in20-300/0Medullary thyroid carcinomaNoYesA-D chromosome 10Mucosal neuroma syndromeVery rareMedullary thyroid carcinomaNoYesMucocutaneous neuromasMarfanoid faciesCafe au lait spotsA-D. chromosome 10perplasia accounts lor 727o to 75% of patients withhyperparathyroidism.CT is- Leported to have a sensitivity rate of 457oto 88%s'! ultrasonography, 307o to 697o20,21,35,58,n.and MR imaging, 40Vo to 63Va58'76 for detecting hyperplasticglands. Parathyroid hyperplasia is detectedin43%to 657o of cases with thallium subtractionand 55% to 75% with ee-Tc sestamibi.20,21,53, s8' e3The added accuracy in identifying hyperplasticglands has led to a growing consensus in supportof the use of ee^Tc sestamibi as the optimal agentfor p-alathyroid adenoma and hyperplasia localization.53,5480Parathyroid CarcinomaOf all patients with hyperparathyroidism, the incidenceof parathyroid carcinoma (Fig. 5) is onlyFigure 5. MR image of parathyroid carcinoma. A large softtissue mass (arrows) is seen anterolateral to the tracheaon the left side. The mass seems to be invading the inferiorplatysma-sternocleidomastoid musculature and invades ajugular vein (J). Histopathologically, this was a parathyroidcarcinoma.7% to 2%, although parathyroid carcinoma causeshyperparathyroidism in 85Va to 90Vo of cases.3e,aoMetastases to lymph nodes occur in one third ofcases, and distant metastases in27Vo to287a ofpatients.Men and women are affected eouallv.Edmonson and colleagues noted thai a paratnyroidcarcinoma may have the same sonographic appearanceas a benign large adenoma (hypoechoicwith or without heterogeneity); only the presenceof local invasion into the thyroid gland, muscles orvessels, or nodal metastases would suggest this diagnosis.l3Parathyroid carcinomas have been reported toaccumula te oo'Tc sestamibi.L alReoperation for HyperparathyroidismDuring reoperation of previously operated cases,307o to 75% of abnormal parathyroid glands arefound in a perithyroidal location, presumablyoverlooked or missed during the initial operation.12'4s'46'61Parathyroid adenomas in patients whohave failed initial operation are located in the anteriormediastinum in 20Vo to 38V0, in a paraesophagealor deep cervical location in approxim ately 20Va,intrathyroidal in 8Vo, and parathymic in 2Vo.45' 46' 61Supernumerary adenomatous glands are present in15% of cases. Of those located in the chest, posteriormediastinal ectopic adenomas are one-fifth as commonas anterior ones.sThe risks associated with reoperation outweighthe cost of preoperative imaging. In those patientswho are reoperated, the risk of vocal-cord injurybecause of damage to the recurrent laryngeal nerv-eor vagus nerve is approximately 77o compared withthe initial operating room risk of 1..3%.a6 When imagingis not performed prior to reoperation for hyperparathyroidism,surgery is approximately 60Voto707o successful; when imaging is performed prior
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 441to reoperation, the success rate increases to 80%to 90%.58 In reoperated cases, the sensitivities ofultrasonography (36-7 6V"),'n'45' 58' 77scintigr aphy (26-g0 vo), z+, +s,so, sa cT (45_ 63%),24,4s,s8, 77 and MR imaging(50-91Vo)'n'"'n5'56's8 have ranged widely. In a reviewof the literature, Price concluded that MR imagingwas the best cross-sectional imaging study to performin this scenario, and nuclear scintigraphy thebest functional examination.s8 The latest figures onsestamibi scintigraphy have shown sensitivities inthe range of 80% to90Vo.a1'e2Parathyroid hyperplasiais the most difficult diagnosis to make and accountsfor most false-negative studies.al e2 Nonetheless,Majors and colleagues found that sestamibi scanningidentified parathyroid tissue in all nine previouslyoperated patients, including one with parathyroidcancer.*tBy combining ultrasonography, CT, and scintigraphy,one can increase the sensitivity rate to 78%,but at a high cost.as Although more invasive studieshave a greater yield, they are more demanding.Miller and colleagues' study found parathyroid venoussampling (80Vo), intraoperative ultrasonography(787"), and arteriography (49-60Vo) Io havehigher sensitivity rates than the noninvasive imagingstudies.aa The expense and technical difficultyin performing these invasive examinations precludestheir routine use, but they may be held inabeyance for cases with equivocal or nonrevealing,noninvasive sfudies.In the patient who has failed prior surgery for aparathyroid adenoma, both imaging and surgerymust contend with scar tissue in and around thethyroid glands, a loss of tissue planes, postoperativeinflammation, lymphadenopathy simulating parathyroidadenomas, and distortion of landmarks.False-negative scans (caused by obscured anatomy)tend to occur in the perithymic or perithyroidaloperative beds. The incidence of false-positive examinations(usually caused by lymphadenopathy)is lowest with nuclear medicine studies, followedby MR imaging, ultrasonography, and CT accordingto Miller and colleagues.asTherefore, which study should one perform in thepreviously operated patient? Two camps of opinionhave formed. Sestamibi scintigraphy is probably themost accurate and affordable studv currentlv availableto identify parathyroid adenomas; its disadvantageis that the surrounding anatomy is not visualizedfor surgical orientation. It alone or combinedwith ultrasonography or CT is an effective option.Alternatively, the most accurate (and most expensive)cross-sectional imaging technique is MR imaging,which provides good anatomic detail, althoughit has the small risk of mistaking a lymphnode for an adenoma. Because re-reoperation is ananathema to the surgeon, multiple studies are notuncommonly performed if one is not definitive. Theidea of using a morphologic test (CT, ultrasonography,or MR imaging) and a functional test (ee-Tcsestamibi) is appealing. Use of this algorithm in-creases the reoperation success rate by more than30%.16Secondary and TertiaryHyperparathyroidismThe evaluation of patients with secondary ortertiary hyperparathyroidism is rarely centeredaround the parathyroid glands because the kidneysare the source ofabnormality in these diseases. Parathyroidglandular hyperplasia usually occurs in associationwith chronic renal failure and renal osteodystrophy.e-Tc sestamibi has been able to identifybilateral uptake in hyperplastic glands and residualparathyroid tissue in those individuals treated surgicallyin the neck for secondary hyperparathyroidism.e3Therapeutic TechniquesEthanol ablation of parathyroid adenomas hasbeen performed under ultrasound guidance by percutaneousinjection of absolute ethanol.sl' 71' 8e Thistechnique may be used in patients with primary orsecondary hyperparathyroidism who are not surgicalcandidates because of medical illnesses. Approximately0.5 mL to 1 mL of ethanol (95Vo) may beinjected at multiple sites within an adenoma witha22-gauge needle. The success of this technique ismonitored by following serial serum calcium levels;the technique may be repeated until normocalcemiais achieved.Parathyroid CystsCysts of the parathyroid glands are more commonin women than in men and mav be presentin the neck (Fig. 6) or anterior mediastinum. Atpresentation, they may be very large in size, andthe differential diagnosis may include thyroid cysts,thymic cysts, and necrotic lymph nodes. They usuallyarise in the region of the inferior pole of thethyroid gland. They are virtually never found inchildren; most cases present in the fourth and fifthdecade of life.a0 They are usually unilocular, large,and may have hyperproteinaceous contents yieldinghigh intensity on Tl-weighted MR scans. Theetiology may be congenital because of remnants ofpharyngeal pouches, or cysts may develop fromdegenerated parathyroid adenomas.HypoparathyroidismThe most common cause of hypoparathyroidismis iatrogenic removal of all functioning parathyroidtissue during surgery for hyperparathyroidism orthyroid disease. Primary idiopathic hypoparathy-
442 YOUSEMFigure 6. A and B, MR images of parathyroid cyst. A, Coronal T1-weighted scan demonstrates arounded cystic mass (arrows) with low intensity fluid. @ The cyst (c) is bright on axial T2-weightedscan. This patient is status posfthryoidectomy.roidism is a disease of childhood unassociated withcervical abnormalities. Pseudohypoparathyroidismmay be caused by renal disease; the serum parathormone(PTH) levels are paradoxically high becauseof a lack of renal responsiveness to the hormone.The glands may be normal or hyperplastic. In pseudopseudohypoparathyroidism,the calcium andphosphate levels are normal, although the physicalfeatures of pseudohypoparathyroidism (coarse facies,dwarfism, mental retardation, round face,stubby fingers) may be present.Imaging of parathyroid glands in patients withhypoparathyroidism is limited to the surveillancefor congenital absence, which is best accomplishedwith scintigraphic methods<strong>THYROID</strong> <strong>IMAGING</strong>The thyroid gland offers a multitude of interestingpathologic entities and lends itself to many differentimaging modalities. Depending on the clinicalpresentation and suspected abnormality, theclinician may order nuclear medicine scintigraphy,ultrasonography, CT, or MR imaging. The evaluationof an infant with a midline cystic mass in thelower neck is entirely different from that of a40-year-old man with a solid palpable nodule inthe thyroid gland. Once the anatomy and imagingoptions available to study the thyroid gland areunderstood, it is useful to divide thyroid lesionsinto neoplastic, congenital, and inflammatory categories.AnatomyThe thyroid gland is positioned anterolateral andsuperficial to the larynx and trachea and is fixed tothe airway by fibrous septa. Although no true lobesof the gland exist, it is enveloped by portions ofthe deep cervical fascia. The thyroid isthmus is themidline portion of the gland and from it may arisea pyramidal "lobe" (50-807, of patients) lying superiicialto the thyroid cartilage.;"The vascular supply to the thyroid gland is derivedfrom paired superior thyroidal arteries(branches of the external carotid arteries) and inferiorthyroidal arteries (branches of the thyrocervicaltrunks of the subclavian arteries). The inconstantthyroidea ima arises directly from the aortic archand supplies a small inferior portion of the gland.The thyroid gland drains into superior, middle, andinferior thyroidal veins, which pass to internal jugularand brachiocephalic veins. Vagal and sympatheticplexus branches provide innervation.Histologically, the gland contains follicular cellsthat secrete the thyroid hormones and parafollicular("C") cells that elicit thyrocalcitonin. Interspersedwithin the gland one finds fibrous septa arid colloiddeposits.lmaging Features of MassesUltrasonographyThe main role of cross-sectional thyroid imaging(ultrasonography, CT, MR) is to evaluate thyioidmasses for_potential malignancy. Ultrasonogriphy,because of its simplicity, low cost, and adility todistinguish cystic from solid lesions is often theiirstmodality used to evaluate a thyroid mass in theeuthyroid patient. Good quality ultrasonographyrequires transducers that have 7.5 to 10 MHz frequencies.2o,7EThese allow excellent detail of the superficialportions of the gland but enough penetrationto evaluate posteriorly to the level of the spine.When a solid leiion is hyperechoic, the incidenceof malignancy is only 4%.72 If a solid lesion is isoechoic,the incidence of malignancy incre ases to 26Voand, if hypoechoic, malignancy occurs in 63%.72Pap-
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 443illary carcinoma most commonly presents as a solidhypoechoic (77Vo) or isoechoic (14%) mass with orwithout calcification (calcifications are hvperechoicbut cause acoustic shadowing that is hypoechoic)(Fig. 7) .?'zIf a cancer is hyperechoic on ultrasonogra-phy, it is usually because of the sclerosing form ofpapillary carcinoma or medullary carcinoma.r6If the margins of tumors on ultrasonography arestudied, 16% of malignant lesions will be found tohave sharply marginated, well-defined borders,Figure 7. ,4-C, Ultrasonograms of papillary carcinoma. A, A reasonably well-defined soft tissue mass(M) is present surrounded by normal thyroid tissue. The mass is hypoechoic. Fine-needle aspirationrevealed papillary carcinoma. B, On transverse sonographic images of a different patient, a soft tissuemass (M) is identified that has internal heterogeneity to its echotexture. This mass was also a papillarycarcinoma of the thyroid gland. C, The longitudinal sonographic view of this mass (M) shows theabsence of an echopenic halo around the lesion and ill-defined inferior borders (arrows\.
444 YOUSEMwhereas irregular or ill-defined borders occur inapproximately 60% of cancers.T2 Unfortunately, irregularor ill-defined borders also occur in approximately45Vo of benign lesions.T2 When a mass has acomplete halo of echopenia around it, the lesion istwelve times more likely to be benign than malignant.If the halo is incomplete, a benign etiology isstill approximately four times more likely than amalignant one.72 Lesions meeting the absolute criteriafor cysts (well-demarcated, smooth-walled, anechoic,and demonstrating enhanced throughtransmission)are usually benign.t6 A cystic lesionwith punctate, calcified mural nodules is indicativeof papillary carcinoma (Fig. 8).Nuclear MedicineA nuclear medicine studv may be another firstlineimaging modality in a patieirt with a palpablethyroid mass. The agents used for thyroid imaginginclude 123I, 131l, ee'Tc pertechnetate, and 201T1. Thehalf-lives, whole-bodv radiation doses, and thvroidradiation doses are listed in Table 3.5& e0 Scanningis performed 15 minutes after administration of5 ti, 10 mCi of ee'Tc pertechnetate, 4 to 24 hoursafter administration of 100 to 400 p.Ci of 123I iodine,and 24 to 72 hours after administration of 30 pCiof r31I agents. With 'zolTl, scanning is performed 5 to10 minutes after thallium administration. Becausethe radiation energy of 131I is so high (364 keV), it isthe preferred agent for imaging substernal thyroidglands or to perform whole-body imaging after thyroidablation to detect metastatic foci of thyroidcancer. The other agents have energies of 140 keV(ee-Tc) and 159 keV (123l).eoThe major role of scintigraphy in the evaluationof a thyroid mass is the determination of whetherthe lesion is hot (more uptake than the normal thyroidgland), warm (some activity but not as much2ts the normal gland), or cold (little to no uptake).The risk of cancer in a hot nodule is between 1%and 4Vo, a warm nodule 8% and'l,jVo, and a coldnodule 15% and ZSVI (FiB. 9).se'0+,0t In a patient whohas a prior historv of head and neck irradiation. therisk oi malignanci itr a cold nodule doubles to 30%to 50%.58 Cold nodules in men have a higher rateof malignancy because women have a greater incidenceof benign cold nodules from degenerated adenomas.If one performs dynamic injection ee-Tcpertechnetate scintigraphy, one may find that hypoperfusedlesions (less vascularity than that of nativethyroid gland) are virtually never cancers, whereasmost malignancies are "euperfused" or hyperperfused.35Increased thallium uptake on both earlvand delayed scintigrams also iras been anecdotallyreported in thyroid malignancies.raRarely, a lesion is cold on 123I scintigraphy buthot or warm on a e-Tc pertechnetate scan (a "discordantnodule"). It is beiieved that this phenomenonis caused by a lesion that traps iodine (assessed withpertechnetate) but does not organify it (the iodinescan). The differential diagnosis includes malignancy/goiter, or follicular adenomas. Often, a biopsyis required in this situation.Computed TomographyFigure 8. Cyst and nodule. The ultrasonogram shows acyst with a nodule (arrow) protruding into the cyst. Notethe throughtransmission (arrowheads) from the cyst. Thiswas a colloid cyst with benign nodule. Calcification of themural nodule would make papillary carcinoma more likely.The presence of calcification, cysts, hemorrhage,hypodensity or hyperdensity, or well-defined bordersin a solitary mass on CT does not exclude acarcinoma (Fig. 10). Peripheral eggshell-like calcificationand large multiple chunks of calcium suggestbenignity, whereas fine punctate calcification ismore indicative of malignancy.60 Calcification occursin 13Vo of all thyroid lesions, including 17% ofall malignancies and 1,1,% of all benign processes.T2Similarly, cystic areas occur in many thyroidmasses; 38% of malignancies have cystic components,and 62Vo of benign masses may be entirelyor partly cystic.72 Hemorrhage may be found in papillarycarcinomas or goiters. Multiplicity of nodulesin an enlarged thyroid gland usually suggests abenign process (or metastases).The presence of lymphadenopathy or infiltrationof adjacent tissues suggests malignancy. More than50Vo of patients with papillary carcinoma havenodal spread at presentation, and 22Vo have occultthyroid tumors.a Curiously, the lymph nodes of thyroidpapillary carcinoma may show calcification,cyst formation, colloid accumulation, hemorrhage,or necrosis.T3'7a Sometimes the wall of a cystic nodemay be unidentifiable, thereby simulating a
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 445Table 3. SCINTIGRAPHIC AGENTS USED FOR <strong>THYROID</strong> <strong>IMAGING</strong>Agent Half-life Total Body Dose (rads) Dose to Thyroid Gland (rads) Dose Administeredt-123t-125l-131Tc-99mTr-20113.6 h60.1 d8.05 d6.02 h3d0.030.29o.020.21h : hours; d: days; PO: oral; lV = intravenous; Ci : curies.2-880-45030-1 000.04-2.0o.92100-400 pCi PO30-1 00 pCi30-100 pCi PO5-10 mCi lV2-3 mOi lVbranchial cleft cyst. Papillary carcinoma of the thyroidmay metastasize to posterior triangle, submandibular,retropharyngeal, or jugular chain lymphnodes.73'74 The nodes mav enhance uniformlv anddramatically or, as with cystic or calcified nodes,not at all.73,7a Any lymph node seen in a patient withpapillary carcinoma is suspected of being malignant,no matter the size because of the relativelyhigh rate of lymphatic spread.Enhanced CT has a maior drawback in the evaluationof thyroid lesions. Because of the iodine uptakefrom the contrast agent, thyroid localization withnuclear scintigraphy and radioactive iodine treatmentmust be delayed 4 to 8 weeks after administrationof iodinated contrast agents.MR lmagingHistologic specificity of thyroid lesions is not improvedwith MR imaging. The key to the diagnosisof thyroid cancer at MR imaging is the presence ofmalignant lymphadenopathy. Irregular marginationand clustered nodularity is characteristic, butnot specific for carcinomas (Fig. 11).18 Lesions thathave an intact and symmetric pseudocapsule areusually benign, whereas those with pseudocapsulesthat are penetrated or destroved are usually cancers.18'52Lesions that have capsules with irrbguhrthicknesses may be malignant or benign. On MRimaging, the nodes of papillary carcinoma may bebright or dark on Tl-weighted and T2-weightedscans, possibly related to the presence of intranodalhemorrhage or colloid accumulation.Postoperatively, thyroid carcinoma recurrencesare usually medium to high intensity on T2-weighted scans, whereas scar in the operative bedis usually low intensity.l Postoperative edema, infection,or hemorrhage may simulate recurrent tumor.131I scintigrams are the best modality to evaluatethe operative bed and to screen for distant metastasesaiter thyroidectomy. MR imaging, in conjunctionwith 131I radioisotope scanning, has been recommendedfor confusing postoperative cases.6Fine-Needle AspirationIntimately associated with any imaging techniqueis fine-needle aspiration cytology. Many palpablelesions of the thyroid gland may be aspirated withoutimaging, but ultrasound is the most commonmodality used to guide aspirations because it imagesin real time. Aspiration cytology in skilledhands yields outstanding results. In a series of11,000 guided and unguided samples performed atthe Mavo Clinic. the sensitivitv of the technioue wasfound io be 98% with a 99% positive pr"di.tin"value for cancer.le Nondiagnostic specimens werepresent in21% of cases, however. Using fine needleaspiration with ultrasound guidance yields resultsof nearly 1,00% sensitivity and specificities near9}Vo,while reducing nondiagnostic samples.l6Malignancies of the Thyroid GlandFigure 9. Cold nodule on scintigraphy. This ee'Tc pertechnetatescan demonstrates a cold nodule (arrows) in thelateral aspect of the left thyroid gland. A solitary cold nodulesuch as this one has a 15% to 25% chance of beino malignant.Thyroid cancers are a mixed group of lesions.The most common histologic subtype is papillarycarcinoma that accounts for 55% to 80% of thyroidmalignancies.3e' 58' 78 Although follicular elements ina papillary carcinoma are common, and this hasled to a "mixed papillary-follicular" or "follicular
446 YOUSEMFigure 10. A and B, CT scans of papillary carcinoma. A, This enhanced CT scan demonstrates amass (M), which has irregular calcification within it, in the left side of the thyroid gland. The presenceof lymph nodes (arrouvs) is highly suggestive of papillary carcinoma. & This cystic lesion with peripheralcalcification in the wall (arrowy proved to be a degenerated adenoma.Figure 11. A-D, Papillary carcinoma on MR scans and scintigraphy.4, Axial T1-weighted scandemonstrates a hyperintense mass (M) with peripheral hypointensity representing calcification. Thewafl, however, is not intact at its anterior-most border (arrows\. The remainder of the gland showsdiffuse enlargement with heterogeneousignal intensity compatible with goiter. The patient presentedwith an enlarging right-sided thyroid mass. 4 Post-gadolinium-enhanced scan demonstrates minimalenhancement because it was bright on pregadolinium T1-weighted scans. No invasion of adjacentstructures was identified. C On T2-weighted scan, the border, though irregular, seems to be intact.Note that on the left side, the signal intensity of the goiterous thyroid gland is inhomogeneous.D, Scintigraphy of this mass revealed bilateral cold areas (C) within the thyroid gland with only a centralarea (arrows) of relatively normal uptake. Biopsy revealed papillary carcinoma of the thyroid gland.This shows how a benign appearance can be present with malignancies of the thyroid gland.
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 447variant" histologic classification, the "mixed cancer"ultimately behaves like a papillary carcinoma(vide infra). Purely follicular carcinoma occursin 5% to 15%. Anaplastic carcinoma represents 3%lo 10% of all malignancies, with m-edullary orHurthle's cell carcinoma accounting for 4Vo lo5Vo.1e'3e Medullary carcinoma may present in associationwith the multiple endocrine neoplasia syndromes(see Table 2) and serologically may expresscalcitonin. The other histologic diagnoses to considerin thyroid malignancies are non-Hodgkin'slymphoma and metastases.Imaging has a well-defined role in the workupof the patient with a solitary nodule in the thyroidgland. Unless a classic appearance of a benign conditionis present, however, pathologic sampling isrequired. This is because the appearance of thyroidmalignancies may simulate many benign processes,and vice versa. The specificity of imaging findingsis low.The detection and characterization of a thyroidneoplasm is not the only role of imaging. Imagingshould also evaluate for infiltration of the adiacentsoft tissue, aerodigestive tract, paraspinal musculature,and carotid arteries. The presence or absenceof adenopathy is also important for prognostic implicationswith thyroid cancer.Papillary CarcinomaThe presence of psammoma bodies (laminatedcalcific spherules in25-40Vo of cases), ground glassnuclei, and a branching pattern with a fibrovascularpapillary stroma are the histologic signatures ofpapillary carcinoma of the thyroid gland.3e As notedearlier, follicular growth patterns may coexist. Cystformation (cystadenocarcinoma), encapsulation,multifocality, and anaplasia may be present withina thyroid gland with papillary carcinoma.Papillary carcinoma is the thyroid malignancythat has the greatest likelihood of spread to lymphnodes; the nodes may be tiny, cystic, hemorrhagic,or calcified (Fig. 12). The incidence of nodal metastasesduring diagnosis is50%, whereas distant metastasesare reported to occur in 4Va to 7Vo, usu.ally tothe lungs, bone, or central nervous system.3e Despitethese features, the 2O-year survival rate is reportedto be as high as 90%. Approximately 10% of papillarycarcinomas are bilateral.eaFollicular CarcinomaPure follicular carcinoma is relatively uncommonwhen the follicular variant of papillary carcinomais excluded. The tumor mav be diffuselv invasiveor well encapsulated. Follicular carcinorna less freqentlyspreads to lymph nodes (2-10%) than doespapillary carcinoma, but disseminates hematogenouslymore readily.3e The prognosis depends onthe presence of hematogenous metastases or localinvasiveness but is not as optimistic as that for papil-lary carcinoma. No distinguishing features on imagingstudies suggest this diagnosis as opposed toother cancers, although, on ultrasonography, follicularcarcinoma is isoechoic in 52% and hypoechoicin44Vo.20'72 Compared with papillary carcinoma, follicularcarcinoma rarely becomes cystic and morefrequently invades vessels.3eAnaplastic CarcinomaThis type of cancer is one of the most aggressivemalignancies of the head and neck with prognosesmarked in months rather than years. Older patientsare usually affected. Anaplastic thyroid carcinomasoccur within a substrate of goiters in 47Vo of cases3eand often coexist with other forms of better differentiatedthyroid cancer. The outcome in mixed tumorcases is dominated by the poor prognosis of anar:lastic^ carcinoma.On ultrasonography, these carcinomas are mostcommonly hypoechoiq20,D,72 whereas on CT, anaplasticcarcinomas show evidence of dense amorphouscalcification in SBVo of cases and necrosis in74Vo.u Metastatic lymph nodes are present in 74Voto 80% of cases and show necrotic areas 50% of thetime.e'82 Invasion into carotid arteries or adjacentaerodigestive structures occurs in 34% to 55% ofpatients, and in 25Vo the primary tumor extendsinto the mediastinum (Fig. 13).q8'?Rapid growth andobliteration of adjacent tissue planes are hallmarksof this deadly tumor with a median survival ofapproximately 7 months.Medullary CarcinomaMedullary carcinoma originates in the parafollicularor "C" cells of the thyroid gland, cells derivedfrom neural crest tissue in the ultimobranchial bodiesof the branchial pouch system. These cells normallvsecrete thvrocalcitonin, which decreases serum'calcium.Eiahty percent to 90% of medullarycarcinomas express calcitonin. Functioning tumorshave a better prognosis.qMedullary carcinomas are usually hypoechoic onultrasonographyzo' zz' 72; however, echogenic focicaused by deposits of calcium may be seen withinthese tumors and metastatic lymph nodes whenpresent.22 These tumors usually do not take up iodinebut may be thallium or gallium avid. Somatostatinreceptor scintigraphy also may detect medullarycarcinoma.ll The tumor is solid on CT and MRimaging and spreads to lymph nodes in more than50Va of cases (Fig. 14).Medullary carcinoma has a familial incidence of"lOVo to 20Vo. Sipple syndrome is the association ofmedullary carcinoma with pheochromocytoma andparathyroid adenoma or hyperplasia. This is alsoknown as the MEN 24. When mucosal neuromasand marfanoid facies coexist, MEN 28 is said to bepresent (see Table 2). Both syndromes have beenlocalized to an abnormal gene on the tenth chromosome.
448 YOUSEMFigure 12. 4-E, Metastases of papillary carcinoma. A, This postcontrast axial CT scan shows twohypodense lymph nodes (n) on the right side of the neck from papillary carcinoma" 8, Note that thepatient had diffuse metastases to the lungs represented by multiple miliary-like nodules. C, In a differentpatient, a densely enhancing lymph node (n) on the left side is seen deep to the sternocleidomastoidmuscle. D, This patient had a cystic and sotid fymph node metastasis (arrows) from the primary thyroidcarcinoma (c). E, T1-weighted MR scan shows a hyperintense node (arrow) from colloid, hemorrhage,thyroglobulin, or high protein.LymphomaThyroid lymphoma may present as a solitarymass (80%) or as multiple nodules (20%).81 An antecedenthistory of Hashimoto's thyroiditis in an elderlyfemale with a rapidly enlarging, compressive,and infiltrative mass suggests lymphoma. Mostare B-cell neoplasms.3e Response to chemotherapyand radiation is variable; some patients do verywell.Lymphomas are usually hypoechoic at sonography-z0z-z t2 Lymphoma is iold bn technetium or"iodinenuclear medicine studies; however, galliumscans may show increased activity. Other lymphoproliferative(leukemia) and granulomatous'diseases(e.9., sarcoidosis) also may be gallium avidand are in the differential diagnosis. The tumor ishypodense on unenhanced and enhanced CT studiesand shows necrosis or calcification in only 7%of cases (Fig. 15).81 Invasion of the carotid sheath
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 449Figure 13, Anaplastic carcinoma on CT scan. Diffuse enlargementwith inegular contrast enhancement is noted inthe thyroid gland of this patient with anaplasti carcinoma.The predominant density is hypodense to the native thyroidtissue. One would expect to see marked enhancement inthe normal thyroid gland due to iodine accumulation.(19-51,7") or metastases to lymph nodes (1,4-44Vo)are not uncommon.8l The absence of calcificationand necrosis, the rarity of invasion into surroundingsoft tissues, and the lower incidence of nodal disseminationhelp to distinguish lymphom a fuom anar:lastic^ carcinoma.Lymphoma is usually homogeneously hyperintenseon T2-weighted MR scans. Although someworkers have found Hashimoto's thyroiditis to below in intensity on T2-weighted images and, therefore,distinguishable from lymphoma (which isbright),6e most investigators have found their signalintensities to overlap.18, 55' 57MetastasesMetastases to the thyroid gland are often clinicallyoccult. Pathologicallp metastases to the glandmay be present in2% to 4Vo of patients dying frommalignant disease.66 The two most commonprimarytumors to metastasize to the thyroid gland are bron-Figure 15. CT scan of thyroid lymphoma. Diffuse infiltrationof the left thyroid gland is noted on this contrast-enhancedexaminalion.chogenic carcinoma and renal cell carcinoma. Multifocalityis the norm (Fig. 16), and hemorrhage isnot uncommon with renal metastases.Benign MassesF u nction i ng Thyroi d Ade nom asMore than ninety percent of solitary hot noduleson scintigraphy are benign in etiology, usually adenomasor hyperplasias that are expressing thyroidhormone. Plummer's disease is hyperthyroidism resultingfrom a solitary autonomous hot nodule (Fig.17).58 The difference between an autonomous anda hypertrophic functioning hot nodule depends onthe response to a thyroid suppression test. After adiagnostic course of thyroid hormone administration(with confirmation of depressed thyroid stimu-Iating hormone [TSH]), a lesion that is persistentlyhot on a eemTc pertechnetate scan is considered anautonomous lesion, whereas one that becomes coldis considered hypertrophic.un Other sources of hotFigure 14. A and B, Medullary carcinoma of the thyroid gland. l, This patient has a thyroid mass (.)on the right that has invaded the tracheal wall accounting for the thickening (arrows) seen lateral tothe endotracheal tube. lt was medullary carcinoma. B, Note absence of right lateral tracheal wallfurther down.
450 YOUSEMFigure 16. Metastatic renal cell carcinoma to the thyroidgland. The multiple masses in this enlarged thyroid glandwere caused by metastases from a primary renal cell carcinoma.Because the thyroid gland absorbs so much iodinateddye, they appear as filling defects amidst the gland.nodules include thyroiditis, normal variation in thyroidfunction, and ectopic tissue.58"Toxic" adenomas rarely cause clinically apparenthyperthyroidism until they exceed 2.5 cm insize.16 The patient usually presents with a slowlygrowing neck mass. The imaging features of toxicadenomas are nonspecific on nonscintigraphic modalities.The lesions are usually solid and enhancing.N onfu nction i ng Thy roi d Ade n omasA cold (nonfunctioning) nodule is approachedmore aggressively than a hot nodule because ofthe higher rate of malignancy, especially in youngwomen and in men of all ages. A biopsy or aspirationis often required early in the diagnostic algo-rithm. The majority of cold nodules are caused bydegenerated (follicular) adenomas (Fig. 18) nodularhemorrhage, cysts, goiters, inflammatory conditions(see subsequent discussion), or amyloid deposition.6aFollicular adenomas occur in all age groups,in women more than in men, and are usually lessthan 3 cm in size. As adenomas outgrow their bloodsupply, they may involute or encyst. Alternatively,they may develop intralesional hemorrhage (andacutely expand), necrosis, calcification, or scarring.Malignant degeneration is not believed to occurin adenomas.Hurthle's cell adenomas (which some investiqatorsbelieve are malignant in character) are morevariable in size and shape with less well-definedborders.Occasionallp one will find a hyperplastic adenomathat is responsive to TSH in a patient withGrave's disease. this appea.s as a cold nodule becausethe hyperthyroidism of Grave's disease suppressesTSH, which in turn suppresses the adenomaon a nuclear medicine studv. This entitv is calledMa r i n e- Le nha r t sy nd ro me.oaIn one of the earliest articles on the subiect of MRimaging, Gefter and colleagues identified adenomatousnodules as small as 4 mm to 5 mm in size.l8They noted that follicular adenomas appeared aswell-circumscribed nodules with heterogeneous intensity,bright on T2-weighted images (Fig. 19).CystsMost thyroid cysts actually represent degenerationof adenomas. Cysts of any kind are anechoicor echopenic on ultrasonography, show a distinctback wall, and demonstrate enhanced throughtransmission.They are low density on CT unlesshemorrhagic or infected. The density and intensityof the cyst mav not simulate that of cerebrospinalfluid on CT anci trrtR imaging because of the p.esen"eof hyperproteinaceous colloid within the cyst. Col-Ioid cysts are characterizedby homogeneous highsignalon Tl-weighted scans6a; however, this findingis not specific to colloid cysts because areas of hemorrhage,also bright on Tl-weighted scans, can beseen in goiters, adenomas, and traumatized cysts.Even thyroglossal duct cysts (vide infra) may behyperintense because of high protein content.Figure 17. Hot nodule on nuclear scintigraphy. Note intenseupdate of radiotracer in this functioning adenoma(arrow). The remainder of the gland shows relatively littleuptake owing to the suppression incurred by reduced TSHfrom the outpouring of thyroid hormone by the "toxicnodule."Multinodular GoiterAnother common palpable thyroid abnormalityis the multinodular goiter. A goiter is simply anenlarged thyroid gland that may be seen with hyperthyroidismor hypothyroidism. In the UnitedStates, the common vernacular is to imply a nontoxicgoiter when the term is used. A euthyroidor hypothyroid goiter is the most common thyroidlesion in the United States. Patients, usually olderwomen, present because of hypothyroidism, neckmasses, or tracheal-esophageal compression. In rare
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong>45'],Figure 18. A and B, Cold nodule. A, A cold nodule was seen along the lateral aspect of the left sideof the thyroid gland (arrow) on this anteroposterior view. B, The MR scan demonstrates two lesionson this slice that were adenomas in a multinodular goiter. In retrospect, the other lesion could be seenposteriorly on the oblique scintigrams.instances, a previously nonfunctioning multinodulargoiter evolves into one with hyperfunctioningnodules and causes hyperthyroidism. The incidenceof carcinoma in a multiodular goiter is very low(below 3%) and the characteristic appearance ofmultiple cold areas interspersed with hot areas in alarge gland usually obviates the need for aggressivebiopsy of a palpable nodule (Fig. 20).6a A large,dominant, hard, or growing mass amidst a goitershould probably still be biopsied (see Fig. 1).70Nontoxic multinodular thyroid glands show minimalto moderate heterogeneity with nodularity andmildly increased signal intensity on T1-weightedMR image.l& s2 Hemorrhagic foci are noted in 60%of cases and the lesions are often heterogenous onT2-weighted scans.s2 Goiters usually dJnot havepseudocapsules.s2 On CT and ultrasonography,mixed solid and cystic zones within an enlarged,nodular thyroid gland with or without calcificationis the characteristic appearance of a multinodulargoiter (Fig. 21).TeratomasThese are rare neoplasms of the thyroid gland.As in other locations in the body, thyroid teratomasmay demonstrate fluid, fat, c;lcificatiory and osseodentaldensities in various combinations. Theyusually occur in the midline.HyperthyroidismThe three most common causes of hyperthyroidismare Graves' disease (diffuse toxic goiter), toxicFigure 19. A and B, MR images of a thyroid adenoma. A, Note the inhomogeneousignal intensityin this hemorrhagic mass (M) on this T2-weighted fat-suppressed MR scan. B, On T1-weighted scan,one sees high signal intensity within the central portion of the mass. lt may be unclear as to whetherthis represents colloid material, hemorrhage, or hyperproteinaceous secretions. The capsule aroundthe lesion (arrows) seems to be well defined, except at its anteromedial aspect.
452 YOUSEM.. ,,..,.i ri:rir::i"ll':'::'Figure 20. Goiter. Nuclear scintigraphy demonstrates anenlarged inhomogeneous thyroid gland. Multiple cold areasare present as well as warm areas and hot areas withinthis gland.multinodular goiter, and toxic adenomas. The toxicadenomas (discussed earlier) are separated intothose that are TSH-responsive (hypertrophic) orTSH-independent (autonomous). Occasionally, inflammationof the thyroid gland (thyroiditis) producesa transient state of hyperthyroidism. On rareoccasions, ectopic thyroid tissue (lingual or ovarian)causes hyperthyroidism.Intenzo and colleagues have proposed a uniquealgorithm for evaluating a hyperthyroid patient.3OIf thyroid function tests (TFTs) are elevated and the24-hour radioactive iodine uptake (RAIU) is alsoelevated (normal, below 357"), the differential diagnosisis Graves' disease or Marine-Lenhardt disease(Graves' with coexistent TSH-dependent nodules).The latter appears on scintigraphy as a gland withdiffuse increased trapping of the radiotracer withsuperimposed cold nodules. If the TFTs are elevatedbut the RAIU is normal, one should consider Plummer'sdisease (hyperthyroidism due to a solitaryautonomous hot nodule that suPPresses the remainderof the gland), Graves' disease with rapid iodineturnover, or a laboratory error.m If TFTs are elevatedbut RAIU is depressed, the possibilities include subacutegranulomatous thyroiditis, subacute lymphocyticthyroiditis, postpartum thyroiditis, andstruma ovarii. With thyroiditides, thyroid hormonemay escape ruptured follicles leading to transienthyperthyroidism, although the damaged gland cannotconcentrate iodine so the RAIU and thyroidscans show depressed uptake.3oGraves' DiseaseGraves' disease is the most common cause of hyoerthvroidism.This disease affects women moreiommonly than men and a familial tendency is present.Patients may have heat intolerance, weight loss,fatigue, insomnia, tremors, palpitations, increasedthirst and hunger, and agitation. Exophthalmosmay be present, although thyroid eye disease neednot occur only in the setting of hyperthyroidism; itmay be present post-therapy when the patient iseuthyroid or even hypothyroid. Blood tests are usuallyable to make the diagnosis of Graves' diseasebecause of the autoimmune phenomenon associatedwith the disease. Thyroid-stimulating immunoglobulins,such as long-acting thyroid stimulator,simulate the function of TSH and cause hyperthyroidism.On iodine scans, there is markedly elevatediodine uptake within a nonfocal, hot, enlarged thyroidgland.Figure 21. Ultrasonography and CT scan of goiter. A, This ultrasound examination reveals multiplenodules (arrows\ seen as hypoechoic areas within an enlarged thyroid gland. 4 In a different patient,one can see bilateral enlargement of the thyroid gland with a hypodense central area on the left side andirregularity and inhomogeneity on the right side. The gland is enlarged and, curiously, is predominantlyposterior to the airway.
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 453In a patient who is hyperthyroid, scintigraphymay be useful in distinguishing Graves' disease,which shows homogeneous diffuse intense uptake(70-85%) from thyroidltides (FiB. 22). Thyroiditisis less homogeneous and the uptake may be normal,high, or low depending on the state of the inflammatoryprocess. Because some thyroiditides (seesubsequent discussion) may revert to euthyroid activitywith time, the implications for theiapy areimportant; Graves' disease requires antithyroidmedication, radioactive iodine obliteration of thegland, or surgery. Thyroiditides are treated conservatively.Diffuse glandular enlargement with avid enhancementmay be noted on CT and MR imagingin patients with Graves' disease. A large pyramidallobe often coexists. Carcinoma of the thyroid glandin a patient with Graves' disease is rare, reportedin only 0.157o to 0.5Vo of patients.l0tries. Other etiologies include the other chronicthyroiditides. Postoperative and postradiotherapy(131I or external beam irradiation) patients also accountfor more hypothyroid patients. It is commonfor patients treated with radioactive iodine for hyperthyroidismto become hypothyroid after severaryears.Congenital hypothyroidism occurs more commonlyin the Japanese population (1 in 5500 newborns).83Possible causes include thyroid aplasia,hemiaplasia (the left gland is absent more commonlythan the right), or ectopia (80%), dyshormonogenesis(10-1,5%), pituitary or hypothalamic deficiency(< 5%) and autoimmune disease (< SVo).Prompt replacement of thyroid hormone is criticalbecause mental retardation is a possible complicationof undiagnosed neonatal hypothyroidism.83Both ultrasonography and scintigraphy are used toidentify thyroid tissue in this population.HypothyroidismHypothyroid patients have cold intolerance; fatigue;apathy; weight gain; bradycardia; constipation;edema; macroglossia; and poor condition ofthe hair, nails, and skin. Women are affected morefrequently than men. The response to thyroid hormonereplacement is excellent.Hashimoto's thyroiditis is the most commoncause of hypothyroidism in the United States (seesubsequent discussion). Worldwide, iodine deficiency(endemic goiter) is another cause of hypothyroidismbut is infrequently seen in developed coun-Figure 22. Graves' disease on nuclear scintigraphy. Thisgland was enlarged and showed increased radiotracer uptake.Note the pyramidalobe (arrows), which is also enlarged.Congenital LesionsThyroglossal Duct CystsTwo of the most common congenital abnormalitiesassociated with the thyroid gland are thyroglossalduct cysts and lingual thyroid glands. The thyroglossalduct cyst is a congenital lesion in which thetract of migration of the thyroid gland from theforamen cecum of the tongue (located in the midlineat the circumvallate papillae level) to the normalposition of the thyroid gland is persistent. Althougha congenital lesion, 50% of cases present after age10 years. Any epithelial-lined tract has the potentialfor obstruction and a cyst may occur due to retainedsecretions. In thyroglossal duct cyst, a midline cysticmass is observed, which is located in an infrahyoidlevel in 65V", hyoid level in 1,5%, and suprahyoidlevel in 20Vo of cases.3 It mav occur in a paramedianposition in 25Vo of cases, usually in the infrahyoidcompartment. The stereotypical locations of the thyroglossalduct cyst are embedded in the strap musclesbelow the hyoid bone, or at the midline junctionof the hyoid bone above the strap muscle insertions(Fig. 23).Because the fluid in the thyroglossal duct cystmay have a high protein content, it may appearcystic with some internal echoes on ultrasonography.It moves with swallowing or sticking thetongue out. On CT, the noninfected thyroglossalduct cyst varies in intensity from markedly hypodense(with no protein content) to slightly hyperdense(with high protein or hemorrhage within).On MR scans, the thyroglossal duct cyst may beeither dark or bright on Tl-weighted scans but istypically hyperintense on T2-weighted scans. Enhancementis uncommon in thyroglossal duct cystsunless the lesion has been traumatized or infected.In those instances, peripheral rim enhancementmay occur.
454 YOUSEMFigure 23. A and B, Thyroglossal duct cyst. A, A cyst embedded in the strap muscle can be seen onthis T2-weighted MR scan" Note the tract (arrows) extending from the midline to the right lateral positionin this paramedian thyroglossal ductal cyst. B, A different patient had a hyperintense midline thyroglossalductal cyst (arrows) on this T1-weighted scan.Ectopic thyroid tissue is found in approximately25Vo to 33% of thyroglossal duct cysts.3'27 The incidenceof carcinoma within the thyroid tissue of athyroglossal duct cyst is less than 'l.Vo.3'27 Y,lhen 1toccurs, it is usually papillary carcinoma.Recurrence rates of approximately 4% are observedafter attempted removal of thyroglossal ductcysts.26 The surgery removes the entire tract of theduct including the middle one fourth of the hyoidbone and a portion of the base of the tongue thatincludes the foramen cecum (Sistrunk procedure).23Rarely, the tract of the thyroglossil duct mayserve as conduit for infection to the thyroid glandleading to acute suppurative thyroiditis.3'?LingualThyroidGlandsLingual thyroid tissue occurs in 1 in 3000 patientswho have thyroid disease and represents the mostcommon form of functioning ectopic thyroid tissue.66Itis also the most common benign mass foundat the circumvallate papillae. The lingual thyroidgland represents arrest of migration of the thyroidtissue within the tongue, usually in the midline betweenthe circumvallate papillae and the epiglottis.This may be a complete arrest or incomplete arrestof migration. Lingual thyroid glands are associatedwith absence of thyroid tissue in the neck in 70%lo 80Vo of cases and are seen much more commonlyin women.6'23'66 Patients often present in puberty,when the tissue may expand rapidly. Variation insize with menstruation also has been reported.The primary role of imaging is to identify whethernormal thyroidal tissue is present in the lower neckso that complete excision or transplantation of thelingual thyroid tissue may be contemplated. If noother thyroid tissue is present, the patient is consignedto lifelong thyroid replacement therapy if thelingual thyroid gland is totally removed. A nuclearmedicine study to determine whether a lingual massrepresents thyroid tissue, and also to search forother (ectopic or normally located) thyroid tissue, isfavored over cross-sectional imaging. The thyroidaltissue within the tongue can be identified by its highattenuation on CT (due to iodine accumulation) orits avid contrast enhancement. In a similar fashion,the MR scan demonstrates bright tissue that avidlyenhances in the middle of the tongue.A malignancy arising within a lingual thyroidgland is more common than one in a thyroglossalduct cyst. At least one report noted an incidenceof 2.8%.aBAberrant Thyroid TissueThyroid tissue lateral to the jugular vein unassociatedwith lymphadenopathy may occur due toanomalous development and is termed lateral aberrantthyroid tissue. This phrase is rarely used noqbecause most cases of lateral aberrant thyroid tissueactually represented thyroid carcinoma metastasesto lymph nodes. Nonetheless, in rare instances, thyroidtissue may be "seeded" to this location bytrauma, surgery, thyroiditis, or goiters, and must bedistinguished from metastatic thyroid carcinoma.Undescended thyroid tissue sometimes may beseen in the anterior neck superficial to the hyoidbone. Aberrant thyroid tissue also may be found inthe trachea. In this site, women are affected morecommonly than men, and the thyroid tissue mayresPond to hormonal influences.Substernal thyroid tissue is not uncommon butusually occurs in association with a goitrous glandextending downward rather than as isolated tissue.Tracheal or esophageal compression on a chest radiographmay be the presenting finding. Imaging todistinguish a goiter from mediastinal adenopathy,thymoma, Iymphoma, teratoma, carcinoma, or an
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 455unusual bronchogenic cyst is usually pursuedwith CT.Struma ovarii, the presence of functioning thyroidtissue in the ovaries or in an ovarian teratomaor dermoid, is rare.Inflammatory LesionsNo specific scintigraphic, sonographic, CT, or MRappearances differentiate among the various inflammatoryprocesses involving the thyroid gland.The most useful imaging study is the nuclear medicinescan, performed with ee'Tc pertechnetate orradioactive iodins (tzal or 131I), which determinesthe activity of the thyroid gland. The value of theimaging studies, however, pales in comparisionwith that of serology for distinguishing various inflammatorylesions of the thyroid gland. On theother hand, if imaging is to be used as a map forsurgical correction or resection of the thyroid gland,MR imaging and ultrasonography seem to be ofparticular benefit. In some instances, the administrationof iodine on an enhanced CT scan mightprecipitate thyroid storm (acute outpouring of thyroidhormone), so CT usually is avoided.Suppu rative ThyroiditisAcute suppurative thyroiditis presents with acuteonset of pain and swelling in the thyroid glandassociated with fever, odynophagia, and dysphagia.25The role of imaging is to exclude a pyriformsinus or thyroglossal duct fistula as an etiology forthe acute suppurative thyroiditis. This entity occurssometimes in association with a fourth branchialcleft anomaly and has a left-sided predominance.2sImaging may identify leakage from the pyriformsinus to the lateral neck at the thyroid gland level.Acute suppurative thyroiditis is the rarest form ofthyroiditis but has the most fulminant clinical presentation.Hashimoto'sThyroiditisMost other forms of thyroiditis are subacute orchronic diseases. Hashimoto's (chronic lymphocyticthyroiditis) is the most common of the chronic thyroiditides,being five to ten times more frequentthan subacute thyroiditis.s8 It is the most commonthyroiditis in children. The diagnosis is based onserology because the disease is an autoimmune processwith antigenic stimulation to thyroglobulin,colloid, and other thyroid cell antigens. Serum levelsof antimicrosomal antibodies are elevated andFNAs may reveal a preponderance of lymphocytes,centroblasts, and Hurthle's cells.el Women are affectednearly 20 times more frequently than men,and the chief complaint is usually enlargement andtenderness of the thyroid gland. Hypothyroidismis present at presentation or develops later in 50%of cases.The gland with Hashimoto's thyroiditis is enlargedand shows multinodularity and heterogeneousincreased or decreased uptake of radiotracers.Although early in the disease there may beincreased uptake of iodine on nuclear medicinestudies, the usual response is diminished or normalthyroid uptake on imaging.el Patients who trapmore tracer have a greater chance of returning to aeuthyroid state than those who do not. AlthoughHashimoto's thyroiditis shows no greater risk forcarcinoma, it seems to predispose to non-Hodgkin'slymphoma.sl Hashimoto's thyroiditis in the presenceof thyroid lymphoma is seen In 25% to 67Voof cases.e'81On ultrasonography, the thyroid gland is symmetricallyenlarged and hypoechoic but may havenodules within it (Fig. 24). Calcification is seen inthe chronic stages. On T2-weighted scans, MR im-Figure 24. A and B, Hashimoto's thyroiditis on ultrasonography. 4, Sagittal scan through the right lobeshows an enlarged gland with some nodularity (arrows) to it. B, The transverse view also depicts aprominent irregular gland.
456 YOUSEMFigure 25. A and B, Riedel's thyroiditis. ,4, This thyroid "mass" has infiltrated the subglottis, causingthickening of the mucosa. Obliteration of the fat planes between thyroid gland and right side of esophagusalso is present. B, AI a more inferior level, one can see the diffuse infiltrative nature of the lesion intothe tracheal rinos.aging has shown increased signal intensity, sometimeswith linear low intensity bands thought torepresent fibrosis.18, 57Hashimoto's disease has been associated withother autoimmune entities, such as pernicious anemia,Sjogren's syndrome, lupus, rheumatoid arthritis,Addison's disease, and Graves' disease.Riedel's ThyroiditisReidel's thyroiditis (struma thyroiditis) is an uncommonchronic inflammatorv lesion of the thvroidgland and neck. The disease may be bilateial orunilateral and is more common in women than inmen. Patients present with evidence of mass effectwith compression of the trachea, hoarseness, anddifficulty ln swallowing. The patients are usuallyhypothyroid. On imaging, Riedel thyroiditis is homogeneouslyhypoechoic on ultrasound and is usuallyhypodense to normal thyroid tissue on CT.20.s7The lesion may be isodense to muscle on unenhancedCT. Riedel thyroiditis may spread to outsideof the thyroid gland, infiltrating and obliteratingadjacent tissue planes (Fig. 25). The characteristicfinding on MR images is hypointensity on T1- andT2-weighted sequences with infiltration of adjacentstructures of the neck.sT The low intensity on MRimages is believed to be caused by the fibrotic natureof the disorder. This lesion may be associated withretroperitoneal fibrosis, mediastinal fibrosis, sclerosingcholangitis, and orbital pseudotumor. It isdistinguished from Hashimoto's thyroiditis, whichis typically increased in intensity on T2-weightedMR images.de Queruain's Thyroiditisde Quervain's thyroiditis (subacute thyroiditis)is a disease of middle age occurring most commonlyin women after an upper respiratory infection. Coxsackie,ECHO, and mumps viruses have been impli-cated.3e Pain, fever, and fatigue are common presentingsymptoms. Subacute thyroiditis may present(50% of cases) with acute toxic hyperthyroidismwith subsequent return to a euthyroid state after1 to 2 months.66 Hypothyroidism occurs approximately2 to 4 months after onset and, typically by6 months after the acute onset, the patient revertsto euthyroidism.s8 Patients are treated medically becausethe prognosis is good for return of normalthyroid function. Subacute thyroiditis is hypoechoicon ultrasonography, although there may be atrophyof thyroidal tissue with time.20 Nuclear medicinestudies show heterogeneous uptake that varies accordingto the stage of the disease.MiscellaneousExternal beam radiation may cause a chronic thyroiditisassociated with fibrosis. In low doses (usedin years past for radiating the thymus, adenoids,acne/ or ringworm), radiation predisposes to papillarycarcinoma. Radioactive iodine treatment alsocauses severe fibrosis and atrophy of the gland.Amyloidosis and hemochromatosis may affectthe thyroid gland and lead to decreased signal intensityon T2-weighted MR scans.Tuberculosis, sarcoidosis, and fungal infectionsmay cause a granulomatous inflammation of thethyroid gland but are uncommon conditions.2References1. Auffermann W, Clark OH, Thurnher S, et al: Recurrentthyroid carcinoma: Characteristics on MR images. Radiology'1.68:7 53 -7 57, 1.9882. Basso LV, Keeling C, Goris ML: Parathyroid imaging.Use of dual isotope scintigraphy for the localizationof adenomas before surgery. Clin Nucl Med 17:380-383,1.992
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 4573. Batsakis JG: Tumors of the Head and Neck. Clinicaland Pathological Considerations. Baltimore, Williams& Wilktns, "1979.4. Beahrs OH, Kiernan PD, Hubert JP Jr: Cancer of thethyroid gland. In Suen JY, Myers E (eds): Cancer ofthe Head and Neck. New York, Churchill Livingstone,1981, pp 599-6325. Brown LR" Aughenbaugh LG: Masses of the anteriormediastinum: CT and MR imaging. AJR Am J RoentgenolL57 :1.77-7780, 79976. Burman KD, Anderson JH, Wartofsky L, et al: Managementof patients with thyroid carcinoma: Applicationof thallium-20l scintigraphy and magnetic resonanceimaging. I Nucl Med 31:1958-1964,79907. Carlson GL, Farndon JR, Clayton B, et al: Thalliumisotope scintigraphy and ultrasonography: Comparativestudies of localization techniques in primary hyperparathyroidism.Br J Stulrg 77:327-329,79908. Casas AT, Burke Gj, Mansberger AR jr, et al: Impactof technetium-99m-sestamibi localization on operativetime and success of operations for primary hyperparathyroidism.Am Surg 60:72-76,79949. Compagno J, Oertel fE: Malignant lymphoma andother lymphoproliferative disorders of the thyroidgland: Clinicopathologic study of 245 cases. Am J ClinPathol 74:1-11,198010. Compagno J: Diseases of the thyroid. In Barnes L (ed):Surgical Pathology of the Head and Neck. New York,Marcel Dekker, 1,985, pp 7435-148611. Dorr U, Wurstlin S, Frank-Raue K, et al: Somatostatinreceptor scintigraphy and magnetic resonance imagingin recurrent medullary thyroid carcinoma: Acomparative study. Horm Metab Res Suppl 27:48-55, 1,99312. Edis AJ, Sheedy PF, Beahrs OH, et al: Results of reoperationfor hyperparathyroidism, with evaluation of preoperativelocalization studies. Surgery 84:384-397,797813. Edmonson G& Charboneau JW, James EM, et aI: Parathyroidcarcinoma: High-frequency sonographic features.Radiology 767:65-67, 798614. el-Desouki M: T1-201 thyroid imaging in differentiatingbenign from malignant thyroid nodules. Clin NuclMed'16:425-430, 199115. Foldes I, Levay A,Stotz G: Comparative scanning ofthyroid nodules with technetium-99m pertechnetateand technetium-99m methoxyisobutylisonitrile. EurJ Nucl Med 20:330-333,799316. Freitas JE, Freitas AE: Thyroid and parathyroid imaging[review]. Semin Nucl Med 24:234-245,799417. Funari M, Campos Z, Gooding GA, et al: MRI andultrasound detection of asymptomatic thyroid nodulesin hyperparathyroidism. Journal of ComputedAxial Tomography 76:675-679, 199218. Gefter WB, Spritzer CE, LiVolsi VA, et al: Thyroidimaging with high-field strength surface-coil MR. Radiology764:483- 490, 198719. Gharib H, Goellner JR" Johnson DA: FNA cytology ofthe thyroid: A 12 year experience with 11,000 biopsies.Clin Lab Med 13:699-71,0, 199520. Gooding GA: Sonography of the thyroid and par athy -roid. Radiol Clin North Am 37:967-989, 799321. Gooding GAW, Okerlund MD, Stark DD, et al: Parath1'roidimaging: Comparison of double-tracer(Tl-201, Tc-99m) scintigraphy and high-resolution ultrasound.Radiology 161,:57-64, 1,98622. Gorman B, Charboneau JW, James EM, et al: Medullarythyroid carcinoma: Role of high-resolution US.Radiology 762:'147 -1,50, 798723. Guneri A, Ceryan K, Igci E. et al: Lingual thyroid:The diagnostic value of magnetic resonance imaging.J Laryngol Otol 105:493-495,799724. Hamilton R" Greenburg BM, Gefter W, et al: Successfullocalization of parathyroid adenomas by magnetic resonanceimaging. Am I Surg 155:370-373,798825. Hatabu H, Kasagi K, Yamamoto K, et al: Acute suppurativethyroiditis associated with pyriform sinus fistula:Sonographic findings. AJR Am J Roentgenol755:845-847, 199026. Hawkins DB, Jacobsen BE, Klatt EC: Cysts of the thp'oglossalduct. Laryngoscope 92:7254-7258, L98227. Hays LL, Marlow SF Jr: Papillary carcinoma arisingin a thyroglossal duct cyst. Laryngoscope 78:2L89-2793,196828. Health H, Hodgson SF, Kennedy MA: Primary hyperparathyroidism,incidence, morbidity, and potentialimpact in a community. N Engl J Med 302:189-193,198029. Hindie E, Melliere D, Simon D, et aI: Primary hyperparathyroidism:Is technetium 99m-sestamibi/iodine-123 subtraction scanning the best procedure to locateenlarged glands before surgery? J Clin EndocrinolMetab 80:302-307, 1,99530. Intenzo CM, Park CH, Kim SM: Thyroid scintigraphyof hyperthyroxinemia [review]. Clin Nucl Med1.8:987-985, 799331. Kang YS, Rosen K, Clark OH, et al: Localization ofabnormal parathyroid glands of the mediastinum withMR imaging. Radiology 789:737 -747, 799332. Kawanaka M, Sugimoto Y, Suehiro M, et al: Thyroidimaging in a typical case of acute suppurative thyroiditiswith abscess formation due to infection from apersistent thyroglossal duct. Ann Nucl Med 8:159-762,799433. Khan A, Samtani S, Varma VM, et al: Preoperativeparathyroid localization: Prospective evaluition oftechnetium 99m sestamibi. Otolaryngol Head NeckSur g 1.71 :467- 472, 1,99 434. Kitapci MT, Tastekin G, Turgut M, et ai: Preoperatrvelocalization of parathyroid carcinoma using Tc-99mMIBI. Clin Nucl Med 78:277-279,799335. Klieger PS, Wilson GA, Greenspan BS: The usefulnessof the dynamic phase in pertechnetate thyroid imagingfor solitary hypofunctioning nodules. Clin Nucl Med17:617-622,199236. Kneeland JB, Kruback AJ, Lawson TL, et al: Enlargedparathyroid glands: High-resolution local coil MR imaging.Radiolo gy 162:143-746, 198737. Lebouthillier G, Morais f, Picard M, et al: Tc-99m sestamibiand other agents in the detection of metastaticmedullary carcinoma of the thyroid. Clin Nucl Med18:657-661,199338. Levin KE, Clark AH, Duh QY, et al: Reoperative thyroidsurgery. Surgery 171:604-609, 199239. Livolsi V: The thyroid and parathyroid.Iz Sternberg SS(ed): Diagnostic Surgical Pathology, ed 2. New York,Raven Press, 7994, pp 523-56040. Livolsi VA: Pathology of the parathyroid glands. 1zBarnes L (ed): Surgical Pathology of the Head andNeck. Marcel Dekker, New York, 1985, pp 1487-756341. Majors JD, Burke GJ, Mansberger AR Jr, et al: TechnetiumTc-99m sestamibi scan for localizing abnormalparathyroid glands after previous neck operations:
458 YoUSEMPreliminary experience in reoperative cases. SouthMed J 88:327-330, l9c542. Mancuso AA, Dillon WP: The neck. Radiol Ciin NorthAm 27:407-434, 798943. Mattar AG, Wright ES, Chittal SM, et al: Impact onsurgery of preoperative localization of parathyroid lesionswith dual radionuclide subtraction scanning.Can J Surg 29:57-59,798644. Miller DL, Doppman JL, Krudy AG, et al: Localizationof parathyroid adenomas in patients who have undergonesurgery. Part IL lnvasive procedures. Radiology762:138-747, 198745. Miller DL, Doppman JL, Shawker TH, et al: Localizationof parathyroid adenomas in patients who haveundergone surgery. Part L Noninvasive imagingmethods. Radiology 162:133-737, 798746. Miller DL: Pre-operative localization and internationaltreatment of parathyroid tumors: When and how?World J 9:rg 75:706-775, 799747. Mitchell BK, Kinder BI(, Cornelius E, et aI: Primaryhyperparathyroidism: Preoperative localization usingtechnetium-sestamibi scanning. J Clin Endocrinol Metabol80:7-70,199548. Montgomery ML: Lingual thyroid: Comprehensive review.West J St:ng 43:66L-677, 1.93549. Morita ET, Kwan WP, Clark OH: Technetium Tc-99msestamibi for parathyroid imaging. West Med761,:41,3, 199450. Neumann DR, Esselstyn CB, Eastwood J, et al: Localizationof mediastinal parathyroid adenoma in recurrentpostoperative hyperparathyroidism with Tc-99msestamibi SPECT. Clin Nucl Med 20:775, 1.99551. Nishimura K: Imaging of the thyroid and parathyroid.Curr Opin Radiol 4:136-1 40, 199252. Noma S, Kanaoka M, Minami S, et al: Thvroid masses:MR imaging and patholgic correlation. Radiology768:759*764, 198853. O'Doherty MJ, Kettle AG, Wells P, et al: Parathyroidimaging with technetium-99m-sestamibi: Preoperativelocalization and tissue uptake studies. J Nucl Med33:373-378, 1,99254. Oates E: Improved parathyroid scintigraphy with Tc-99rn MIBI, a superior radiotracer. Appl Radiol 37-42,799455. Ohnishi T, Noguchi S, Murakami N, et aI: MR imagingin patients with primary thyroid lymphoma. AJNRAm J Neuroradiol 13:1196-1198, 799256. Peck WW, Higgins CB, Fisher MR, et al: Hyperparathyroidism:Comparison of MR imaging with radionuclidescanning. Radiology 163:41.5-420, 1.98757. Perez Fontan FJ, Cordido Carballido F, PomboFelipe F, et al: Riedel thyroiditis: US, CT, and MRevaluation. J Comput Assist Tomogr 77:324-325,199358. Price DC: Radioisotopic evaluation of the thyroid andthe parathyroids. Radiol Clin North Am 31:991-7075, 1,99359. Reading CC, Charboneau JW, James EM, et al: Highresolutionparathyroid sonography. AIR Am J Roentgenol139:539-546, 798260. Reading CC, Gorman CA: Thyroid imaging techniques.Clin Lab Med '13:777-724, 199361. Rodriquez JM, Tezelman S, Siperstein AE, et al: Localizationprocedures in patients with persistent or recurrenthyperparathyroidism. Arch Surg. 1.29:870-875,1.99462. Roe SM, Burns RP, Graham LD et al: Cost-effectivenessof preoperative localization studies in primary hyperparathyroiddisease. Ann Surg 219:582-586, 199463. Russell CF, Laird JD, Ferguson WR: Scan-directed unilateralcervical exploration for parathyroid adenoma:A legitimate approach? World J Surg 74:406-409, 1,99064. Sandler MP, Patton JA, Ossoff RH: Recent advancesin thyroid imaging. Otolaryngol Clin North Am23:257-270,199065. Satava RM, Beahrs OH, Scholz DA: Success rate ofcervical exploration for hyperparathyroidism. ArchSurg 110:625-627,197566. Schwartz SI, Shires GT, Spencer FC, et al: Principlesof Surgery, ed 3. New Yorl McGraw Hill, 7979, p 754767. Seelos KC, DeMarco R, Clark OH, et al: Persistentand recurrent hyperparathyroidism: Assessment withgadopentetate dimeglumine-enhanced MR imaging.Radiology 177 :373-378, 199068. Shamma FN, Abrahams Jj: Imaging in endocrine disorders.J Reprod Med 37:39-45, 199269. Shibata T, Noma S, Nakano Y, et al: Primary thyroidlymphoma: MR appearance. J Comput Assist Tomogr15:629-633,799770. Shulkin BL, Shapiro B: The role of imaging tests inthe diagnosis of thyroid carcinoma. Endocrinol MetabClin North Am 79:523-543, 199071. Solbiati L, Giangrande A, De Pra L, et aI: Percutaneousethanol inlection of parathyroid tumors and ultrasoundguidance: Treatment for secondary hyperparathyroidism.Radiology 755:607-670, 798572. Solbiati L, Volterrani L,Rizzatto G, et aI: The thyroidgland with low uptake lesions: Evaluation by ultrasound.Radiology 755:187 -197, 198573. Som PM, Brandwein M, Lidov M, et al: The variedappearance of papillary carcinoma cervical nodal disease:CT and MR findings. AINR Am J Neuroradiol75:71.29-11.38, 799474. Som PM: Lymph nodes of the neck. Radiology165:593-600, 798775. Sommer B, Welter HF, Spelsberg R et al: Computedtomography for localizing enlarged parathyroidglands in primary hyperparathyroidism. ]ournal ofComputer Assisted Tomography 6:521-526, 198276. Spritzer CE, Gefter WB, Hamilton R" et al: Abnormalparatyroid glands: High resolution MR imaging. Radiology162-487 -491, 198777. Stark DD, Cooding GAW, Moss AA: Parathyroid imaging:Comparison of high-resolution CT and highresolutionsonography. AJR Am J Roentgenol 141:633-638,198378. Sutton RT, Reading CC, Charboneau JW, et aI: USguidedbiopsy of neck masses in postoperative managementof patients with thyroid cancer. Radiology168:769-772, 198879. Szybinski Z, Huszno B, Golkowski F, et al: Technetium99m-methoxyisobutylisonitrile in early diagnosis ofthyroid cancer. Endokrynologia Polska 44:427-433,799380. Taillefer R, Boucher Y, Potvin C, et al: Detection andlocalization of parathyroid adenomas in patients withhyperparathyroidism using a single radionuclide imagingprocedure with technetium-99m-sestamibi(double phase study). J Nucl Med 33:7801-7807, 799281. Takashima S, Ikezoe J, Morimoto S, et al: Primarythyroid lymphoma: Evaluation with CT. Radiology768:765-768, 198882. Takashima S, Morimoto S, Ikezoe J, et al: CT evaluationof anaplastic thyroid carcinoma. AJR Am J Roentgenol754:7079 -1.985, 7990
<strong>PARA<strong>THYROID</strong></strong> <strong>AND</strong> <strong>THYROID</strong> <strong>IMAGING</strong> 45983. Takashima S, Nomura N, Tanaka H, et al: Congenitalhypothyroidism: Assessment with ultrasound. AJNRAm J Neuroradiol 16:"11,1,7 -1,'123, 799584. Thompson CT: Localization studies in patients withhyperparathyroidism. Br J Surg 75:97-98,798885. Thompson NW, Eckhauser FE, Harness JK: The anatomyof primary hyperparathyroidism. Surgery 92:81.4-821.,1.982Tibblin S, Bondeson AG, Ljungberg O: Unilateral parathyroidectomyin hyperparathyroidism due to singleadenoma. Ann Surg 795:245-252, 1,98287. Uden P, Aspelin P, Berglund f, et al: Preoperativelocalization in unilateral parathyroid surgery. A costbenefitstudy on ultrasound, computed tomographyand scintigraphy. Acta Chir Scand 1,50:29-35, 1,99088. van Heerden |A, Weiland LH, ReMine WH, et al: Cancerof the parathyroid gland. Arch *rg 774:475-479,1.97989 Verges B, Cercueil JP, Pfitzenmyer P, et al: Percutaneousethanol injection of parathyroid adenomas in primaryhyperparathyroidism. Lancet 337:7421,-7422,1,99790. Walker JM, Margouleff D: A Clinical Manual of NuclearMedicine. Norwalk, CT, Appleton-Century-Crofts, 198491. Wang PW, Chen HY, Li CH, et al: Tc-99m pertechnetatetrapping and thyroid function in Hashimoto's thyroiditis.Clin Nucl Med 79:777-780, 199492. Weber CJ, Vansant J, Alazraki N, et al: Value oftechnetium 99m sestamibi iodine 123 imaging inreoperative parathyroid surgery. Surgery 174:1,077-7078, 199393. Wei fP, Burke GJ, Mansberger AR Jr: Preoperativeimaging of abnormal parathyroid glands in patientswith hyperparathyroid disease using combinationTc-99m-pertechnetate and Tc-99m-sestamibi radionuclidescans. Ann Surg 279:568-572,799494. Woolner LB, Beahs OH, Black BM, et al: Classificationand prognosis of thy'roid cancer. Am J Surg 102:354-387,1961.95. Yao M, Jamieson C, Blend R: Magnetic resonance imagingin preoperative localization of diseased parathyroidglands: A comparison with isotope scanning andultrasonography. Can J Swg 36:241-244, 199396. Yen TC, Lin HD, Lee CH, et al: The role of technetium-99m sestamibi whole-body scans in diagnosing metastaticHurthle cell carcinoma of the thyroid gland aftertotal thvroidectomv: A comparison with iodine-131and thailium-2Of #note-Uoay scans. Eur J Nucl Med27:980-983,7994Address reprint requests toDavid M. Yousem, MDDepartment of RadiologyUniversity of Pennsylvania Medical Center3400 Spruce StreetPhiladelphia, PA 19104