

View PDF Edition - U.S. Pharmacist
View PDF Edition - U.S. Pharmacist
View PDF Edition - U.S. Pharmacist

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
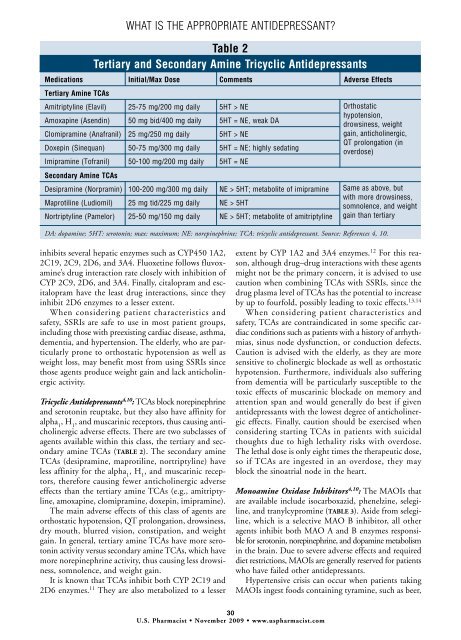
WHAT IS THE APPROPRIATE ANTIDEPRESSANT?Table 2Tertiary and Secondary Amine Tricyclic AntidepressantsMedications Initial/Max Dose Comments Adverse EffectsTertiary Amine TCAsAmitriptyline (Elavil) 25-75 mg/200 mg daily 5HT > NEAmoxapine (Asendin) 50 mg bid/400 mg daily 5HT = NE, weak DAClomipramine (Anafranil) 25 mg/250 mg daily 5HT > NEDoxepin (Sinequan) 50-75 mg/300 mg daily 5HT = NE; highly sedatingImipramine (Tofranil) 50-100 mg/200 mg daily 5HT = NESecondary Amine TCAsDesipramine (Norpramin) 100-200 mg/300 mg daily NE > 5HT; metabolite of imipramineMaprotiline (Ludiomil) 25 mg tid/225 mg daily NE > 5HTNortriptyline (Pamelor) 25-50 mg/150 mg daily NE > 5HT; metabolite of amitriptylineOrthostatichypotension,drowsiness, weightgain, anticholinergic,QT prolongation (inoverdose)Same as above, butwith more drowsiness,somnolence, and weightgain than tertiaryDA: dopamine; 5HT: serotonin; max: maximum; NE: norepinephrine; TCA: tricyclic antidepressant. Source: References 4, 10.inhibits several hepatic enzymes such as CYP450 1A2,2C19, 2C9, 2D6, and 3A4. Fluoxetine follows fluvoxamine’sdrug interaction rate closely with inhibition ofCYP 2C9, 2D6, and 3A4. Finally, citalopram and escitalopramhave the least drug interactions, since theyinhibit 2D6 enzymes to a lesser extent.When considering patient characteristics andsafety, SSRIs are safe to use in most patient groups,including those with preexisting cardiac disease, asthma,dementia, and hypertension. The elderly, who are particularlyprone to orthostatic hypotension as well asweight loss, may benefit most from using SSRIs sincethose agents produce weight gain and lack anticholinergicactivity.Tricyclic Antidepressants 4,10 : TCAs block norepinephrineand serotonin reuptake, but they also have affinity foralpha 1, H 1, and muscarinic receptors, thus causing anticholinergicadverse effects. There are two subclasses ofagents available within this class, the tertiary and secondaryamine TCAs (TABLE 2). The secondary amineTCAs (desipramine, maprotiline, nortriptyline) haveless affinity for the alpha 1, H 1, and muscarinic receptors,therefore causing fewer anticholinergic adverseeffects than the tertiary amine TCAs (e.g., amitriptyline,amoxapine, clomipramine, doxepin, imipramine).The main adverse effects of this class of agents areorthostatic hypotension, QT prolongation, drowsiness,dry mouth, blurred vision, constipation, and weightgain. In general, tertiary amine TCAs have more serotoninactivity versus secondary amine TCAs, which havemore norepinephrine activity, thus causing less drowsiness,somnolence, and weight gain.It is known that TCAs inhibit both CYP 2C19 and2D6 enzymes. 11 They are also metabolized to a lesserextent by CYP 1A2 and 3A4 enzymes. 12 For this reason,although drug–drug interactions with these agentsmight not be the primary concern, it is advised to usecaution when combining TCAs with SSRIs, since thedrug plasma level of TCAs has the potential to increaseby up to fourfold, possibly leading to toxic effects. 13,14When considering patient characteristics andsafety, TCAs are contraindicated in some specific cardiacconditions such as patients with a history of arrhythmias,sinus node dysfunction, or conduction defects.Caution is advised with the elderly, as they are moresensitive to cholinergic blockade as well as orthostatichypotension. Furthermore, individuals also sufferingfrom dementia will be particularly susceptible to thetoxic effects of muscarinic blockade on memory andattention span and would generally do best if givenantidepressants with the lowest degree of anticholinergiceffects. Finally, caution should be exercised whenconsidering starting TCAs in patients with suicidalthoughts due to high lethality risks with overdose.The lethal dose is only eight times the therapeutic dose,so if TCAs are ingested in an overdose, they mayblock the sinoatrial node in the heart.Monoamine Oxidase Inhibitors 4,10 : The MAOIs thatare available include isocarboxazid, phenelzine, selegiline,and tranylcypromine (TABLE 3). Aside from selegiline,which is a selective MAO B inhibitor, all otheragents inhibit both MAO A and B enzymes responsiblefor serotonin, norepinephrine, and dopamine metabolismin the brain. Due to severe adverse effects and requireddiet restrictions, MAOIs are generally reserved for patientswho have failed other antidepressants.Hypertensive crisis can occur when patients takingMAOIs ingest foods containing tyramine, such as beer,30U.S. <strong>Pharmacist</strong> • November 2009 • www.uspharmacist.com








