

View PDF Edition - U.S. Pharmacist
View PDF Edition - U.S. Pharmacist
View PDF Edition - U.S. Pharmacist

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
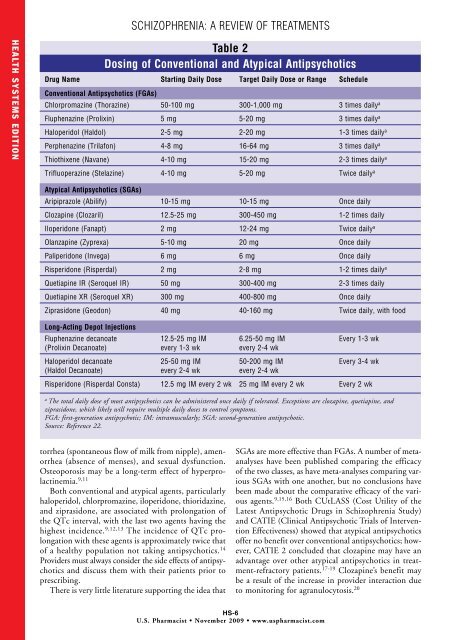
SCHIZOPHRENIA: A REVIEW OF TREATMENTSHEALTH SYSTEMS EDITIONTable 2Dosing of Conventional and Atypical AntipsychoticsDrug Name Starting Daily Dose Target Daily Dose or Range ScheduleConventional Antipsychotics (FGAs)Chlorpromazine (Thorazine) 50-100 mg 300-1,000 mg 3 times daily aFluphenazine (Prolixin) 5 mg 5-20 mg 3 times daily aHaloperidol (Haldol) 2-5 mg 2-20 mg 1-3 times daily aPerphenazine (Trilafon) 4-8 mg 16-64 mg 3 times daily aThiothixene (Navane) 4-10 mg 15-20 mg 2-3 times daily aTrifluoperazine (Stelazine) 4-10 mg 5-20 mg Twice daily aAtypical Antipsychotics (SGAs)Aripiprazole (Abilify) 10-15 mg 10-15 mg Once dailyClozapine (Clozaril) 12.5-25 mg 300-450 mg 1-2 times dailyIloperidone (Fanapt) 2 mg 12-24 mg Twice daily aOlanzapine (Zyprexa) 5-10 mg 20 mg Once dailyPaliperidone (Invega) 6 mg 6 mg Once dailyRisperidone (Risperdal) 2 mg 2-8 mg 1-2 times daily aQuetiapine IR (Seroquel IR) 50 mg 300-400 mg 2-3 times dailyQuetiapine XR (Seroquel XR) 300 mg 400-800 mg Once dailyZiprasidone (Geodon) 40 mg 40-160 mg Twice daily, with foodLong-Acting Depot InjectionsFluphenazine decanoate 12.5-25 mg IM 6.25-50 mg IM Every 1-3 wk(Prolixin Decanoate) every 1-3 wk every 2-4 wkHaloperidol decanoate 25-50 mg IM 50-200 mg IM Every 3-4 wk(Haldol Decanoate) every 2-4 wk every 2-4 wkRisperidone (Risperdal Consta) 12.5 mg IM every 2 wk 25 mg IM every 2 wk Every 2 wkaThe total daily dose of most antipsychotics can be administered once daily if tolerated. Exceptions are clozapine, quetiapine, andziprasidone, which likely will require multiple daily doses to control symptoms.FGA: first-generation antipsychotic; IM: intramuscularly; SGA: second-generation antipsychotic.Source: Reference 22.torrhea (spontaneous flow of milk from nipple), amenorrhea(absence of menses), and sexual dysfunction.Osteoporosis may be a long-term effect of hyperprolactinemia.9,11Both conventional and atypical agents, particularlyhaloperidol, chlorpromazine, iloperidone, thioridazine,and ziprasidone, are associated with prolongation ofthe QTc interval, with the last two agents having thehighest incidence. 9,12,13 The incidence of QTc prolongationwith these agents is approximately twice thatof a healthy population not taking antipsychotics. 14Providers must always consider the side effects of antipsychoticsand discuss them with their patients prior toprescribing.There is very little literature supporting the idea thatSGAs are more effective than FGAs. A number of metaanalyseshave been published comparing the efficacyof the two classes, as have meta-analyses comparing variousSGAs with one another, but no conclusions havebeen made about the comparative efficacy of the variousagents. 9,15,16 Both CUtLASS (Cost Utility of theLatest Antipsychotic Drugs in Schizophrenia Study)and CATIE (Clinical Antipsychotic Trials of InterventionEffectiveness) showed that atypical antipsychoticsoffer no benefit over conventional antipsychotics; however,CATIE 2 concluded that clozapine may have anadvantage over other atypical antipsychotics in treatment-refractorypatients. 17-19 Clozapine’s benefit maybe a result of the increase in provider interaction dueto monitoring for agranulocytosis. 20HS-6U.S. <strong>Pharmacist</strong> • November 2009 • www.uspharmacist.com








