Role of The Professional Nurse Role of The Professional Nurse
Role of The Professional Nurse Role of The Professional Nurse
Role of The Professional Nurse Role of The Professional Nurse
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
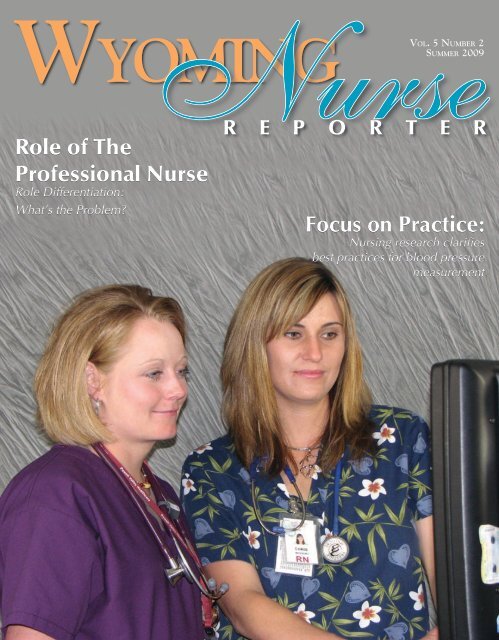
<strong>Nurse</strong>R E P O R T E RWy o m i n g<strong>Role</strong> <strong>of</strong> <strong>The</strong>Pr<strong>of</strong>essional <strong>Nurse</strong><strong>Role</strong> Differentiation:What’s the Problem?Vo l. 5 Nu m b e r 2Su m m e r 2009Focus on Practice:Nursing research clarifiesbest practices for blood pressuremeasurement
A Rare Opportunity to Becomea Part <strong>of</strong> Nursing ExcellenceWHY CHOOSE EXCELLENCE?Our nurses enjoy alow nurse-to-patient ratio,a warm, family-oriented environment,state-<strong>of</strong>-the-art facilities, and anemphasis on balancing work and life.Maybe that’s why our hospital receivesnear-perfect patient satisfactionsurvey scores every month!We are currently accepting applications forRNs trained in the following specialties:Surgical • ICU/Critical Care • ERCNAs — Full-Time and PRNPositions Available(307) 995 - 81006550 E. 2ND STREET • CASPER, WYOMING • WWW.MOUNTAINvIEWREGIONAlhOSPITAl.COMMVRH_Job_Recruit_Full.indd 15/28/09 1:26:00 PM
<strong>Nurse</strong>Summer 2009 Vo l. 5 Nu m b e r 2Ma n a g i n g Ed i t o rMarcia L. Dale, RN, EdD, FAANR E P O R T E R“protecting the public through excellence in nursing...”T a b l e o f Co n t e n t sWy o m i n gPublished by theWyoming State Board <strong>of</strong> Nursing1810 Pioneer Ave.Cheyenne, Wyoming 82002Phone: 307-777-7601Fax: 307-777-3519Web Address: http://nursing.state.wy.usAgency Mission: <strong>The</strong> Wyoming State Board <strong>of</strong>Nursing is responsible for the protection <strong>of</strong> the public’shealth, welfare, and safety through the regulation <strong>of</strong>nursing, nursing education, nursing practice, anddisciplinary standards. <strong>The</strong> responsibility <strong>of</strong> the Board<strong>of</strong> Nursing is to implement a cost-effective and efficientsystem <strong>of</strong> regulation, which meets the consumerdemand for safe, competent, ethical practitioners <strong>of</strong>nursing which includes advanced practice nurses, registeredpr<strong>of</strong>essional nurses, licensed practical nurses,and certified nursing assistants.Ex e c u t i v e Di re c t o rMary Kay Goetter, PhD, RNC, NEA-BCAssistant Ex e c u t i v e Di re c t o r ,Pr a c t i c e a n d Ed u c a t i o n Co n s u l t a n tMary Beth Stepans, PhD, RNCo m p l ia n c e Co n s u l t a n tPatti Hefflin, BSN, RNBrenda Burnett, MSN, RNFi n a n c i a l a n d Hu m a n Resources OfficerCindy StillahnEx e c u t i v e AssistantJoAnn ReidLi c e n s i n g Co o r d i na t o rLaVelle OjedaLi c e n s i n g Co o r d i na t o rMaxine HernandezDisciplinary AssistantDebra BallNella MartinezWyoming <strong>Nurse</strong> Reporter does not necessarilyendorse advertisements contained herein. <strong>The</strong>publisher reserves the right to accept or rejectadvertisements for Wyoming <strong>Nurse</strong> Reporter.For Advertising Information:Victor Hornevhorne@pcipublishing.com501.221.9986 or 800.561.4686Created By:Publishing Concepts, Inc.Virginia Robertson, Publishervrobertson@pcipublishing.comBo a r d o f Nu r s i n g MembersJennifer Zettl, RNPresidentTracy Waserburger, RN, GAPRN Vice-presidentMarguerite HermanConsumer SecretaryKim Williamson, LPNMemberMarcie Burr, RNMemberCarrie Deselms, APRN, FNP-BC MemberKellie Clausen, FNP, WHCNP, RN Memberwww.thinkaboutitnursing.comPublishing Concepts, Inc.14109 Taylor Loop RoadLittle Rock, AR 72223EDITION 173 Nursing Practice4 Letters to the Editor5 Congratulations Graduates!6 <strong>Role</strong> Differentiation7 Focus on Practice8 Scope <strong>of</strong> Practice- Decision Tree10 Title Protection11 Certified Nursing Assistant II (CNA II) withCertified Medication Administrative Certification14 NCSBN - Transition to Practice Model15 Invest in <strong>The</strong> Future16 NCSBN - Transition to Practice Model- Frequently asked Questions18 Parish <strong>Nurse</strong> Ministry18 Healthcare without Harm20 Advanced Practice Registered <strong>Nurse</strong> in a Specialty Clinic22 Why all the Confusion about Midwives and Home Birth28 Disciplinary Actions30 NCSBN Unveils New Nursys.com Web Site30 Nursys UpdateGreetingsFrom Mary Kay GoetterExecutive DirectorNursing Practice<strong>The</strong> Summer 2009 issue <strong>of</strong> theWyoming <strong>Nurse</strong> Reporter (WNR) isdedicated to the practice <strong>of</strong> nursingin the state <strong>of</strong> Wyoming. <strong>The</strong> staff <strong>of</strong>the Wyoming State Board <strong>of</strong> Nursing(WSBN) have been culling our telephoneand e-mail logs for the mostcommon questions and pressingissues related to nursing practice.Several <strong>of</strong> these practice issuesbrought forth to the board have beenhighlighted in the articles <strong>of</strong> this issue.Usually, questions posed to theWSBN are in regards to whethersome specific task or skill is withinthe scope and standards <strong>of</strong> nursingpractice, as determined by the Wyoming<strong>Nurse</strong> Practice Act (“<strong>Nurse</strong>Practice Act,” 2005) and AdministrativeRules and Regulations (WyomingState Board <strong>of</strong> Nursing, 2003).However, before plunging into specificquestions related to scope andstandards <strong>of</strong> nursing practice in thisstate, let’s first look at the definition<strong>of</strong> nursing practice.A quick review <strong>of</strong> one <strong>of</strong> my favoritereferences, Encarta onlinedictionary and thesaurus, definespractice as “to do something repeatedlyin order to improve performancein a sport, art or hobby…todo something as an established customor habit…to work in a pr<strong>of</strong>ession,especially law or medicine…[and] the process <strong>of</strong> carrying out anidea, plan or theory” (Micros<strong>of</strong>t Corporation,2009). Synonyms listed forrepetition (as it relates to practice)are rehearsal, exercise, preparation,training, run-through and drill.Synonyms for habit (as it relatesto practice) are custom, tradition,way, system, routine, ritual, manner,praxis and method. I would like totake this opportunity to pose a questionto each <strong>of</strong> Wyoming’s practicingnurses. Which definition bestdescribes your nursing practice: 1)doing something repeatedly to improveyour performance in the art<strong>of</strong> nursing, or 2) doing something byestablished custom or habit?Nursing has a long-standingreputation for practicing our pr<strong>of</strong>essionby tradition, intuition, andritual. <strong>The</strong>re is evidence to supportthat there are different ways <strong>of</strong>knowing and that each holds its ownvalue. Barbara Carper (1978, 2004)Continued on next page
Continued from previous pagerevolutionized nursing knowledge development whenshe presented her theory <strong>of</strong> nursing’s unique patterns <strong>of</strong>knowing which include empirical, aesthetic, personal andethical knowledge. <strong>The</strong> “personal way <strong>of</strong> knowing” (2004,p. 225) she described includes intuition and personalinstinct. However, the pr<strong>of</strong>ession is at a disadvantagewhen it relies solely on this type <strong>of</strong> knowledge to informpractice.Pr<strong>of</strong>essional nursing care was one <strong>of</strong> the first bigbudget line items to get slashed when health care administratorsand third party payers sought to cut costs in thelast decade. Unlicensed assistive personnel (UAPs) replacedmany pr<strong>of</strong>essional nurses with disastrous results(Harrison, 2007). As the nursing pr<strong>of</strong>ession continues t<strong>of</strong>ace the challenge <strong>of</strong> quantifying its contribution to positivepatient outcomes, the answer cannot be, “We justknow that patients get better faster with good nursingcare than without it”. Nursing researchers answered thecall to support this intuitive deduction with empirical evidence:nurse staffing levels and educational preparationpositively affect patient care outcomes (Aiken, Clarke,Cheung, Sloan, & Silber, 2003; Aiken, Clarke, & Sloan,2002); healthy working environments for nurses promotepatient safety outcomes (Clarke, 2006; Laschinger & Leiter,2006); and, the strength in numbers and education <strong>of</strong>the nursing workforce is critical to healthcare outcomes(Buerhaus, 2008).<strong>The</strong>se studies are critical in guiding healthcare policymakers at the state and national levels, but may notseem to have much bearing on the day to day practice orhabits <strong>of</strong> those reading the WNR. Wyoming nurses arepracticing the art and science <strong>of</strong> nursing in multiple anddiverse employment and volunteer settings: acute care,home health, schools, <strong>of</strong>fices, occupational settings, andcommunity-based outreach programs. <strong>The</strong> Wyoming Department<strong>of</strong> Employment regularly publishes statisticson nursing employment in Wyoming; see their websitefor further information and a detailed breakdown <strong>of</strong> ourstate’s nursing workforce http://doe.state.wy.us.When I first began my practice as an Intensive CareUnit nurse just 8 months after graduation from nursingschool, one <strong>of</strong> my preceptors was fond <strong>of</strong> reminding everyoneshe worked with (and me in particular) <strong>of</strong> how longshe had been an ICU nurse. In my first days on that unit,she would <strong>of</strong>ten preface a declarative statement with,“Well, I’ve been an ICU nurse for seven years, and in thattime I’ve learned…” and she would go on to make somedefinitive policy, standard, or procedural claim. At thattime in my life, 7 years <strong>of</strong> experience seemed astronomical!I could hardly wait to make the same claim. However,now that I could begin a sentence with, “Well, I’ve beena nurse for almost 30 years and I’ve learned…” I wouldhave to think long and hard on how to end that statement.I think now I would have to say now that I am nearing my30th anniversary as a nurse, what I have learned is thatthere is so much more knowledge to explore and so manyways my practice could be enhanced. Just as the Olympicmedalist or advanced yogi or accomplished musician stillembraces regular, deliberate, and mindful practice toseek excellence, so must a nurse.Several years ago, a colleague and I were having adiscussion about trying to implement an evidence-basedpractice change on a nursing unit where many <strong>of</strong> the staffhad longevity in that specialty area and <strong>of</strong>ten resistedopportunities for growth and improvement. I stated thatit was difficult to argue with someone who had over 20years <strong>of</strong> experience in that specialty. My colleague made asnappy and immediate comeback, “OK, so is that 20 years<strong>of</strong> growth moving to expert practice, or is it the same firstyear <strong>of</strong> practice repeated over and over for 20 more?” Welaughed at the time, but since then I have <strong>of</strong>ten thoughtabout that idea and believe it is true for many nurses. Justas the nurse who precepted me as a novice and soughtto impress me with her years <strong>of</strong> experience—and succeeded—thereare those who rest on their tenure in thepr<strong>of</strong>ession as the only criteria for being expert in theirpractice.Each specialty practice area has its own pr<strong>of</strong>essionalorganization that provides publications, guidance andpertinent research. I urge each <strong>of</strong> you to seek out theevidence and knowledge you need to support your ownpractice to improve the performance <strong>of</strong> your art. Thankyou for the invaluable service you provide to Wyoming.ReferencesAiken, L. H., Clarke, S. P., Cheung, R. B., Sloan, D. M., &Silber, J. H. (2003). Educational levels <strong>of</strong> hospital nursesand surgical patient mortality. Journal <strong>of</strong> the AmericanMedical Association, 290(12), 1617-1623.Aiken, L. H., Clarke, S. P., & Sloan, D. M. (2002). Hospitalstaffing, organization, and quality <strong>of</strong> care: Cross-nationalfindings. International Journal for Quality in HealthCare, 14(1), 5-13.Buerhaus, P. I. (2008). Current and future state <strong>of</strong> theUS nursing workforce. <strong>The</strong> Journal <strong>of</strong> the American MedicalAssociation, 300(20), 2422-2426.Carper, B. A. (1978). Fundamental patterns <strong>of</strong> knowingin nursing. Advances in Nursing Science, 1(1), 13-23.Carper, B. A. (2004). Fundamental patterns <strong>of</strong> knowingin nursing. In P. Reed, N. Schearer & L. Nicoll (Eds.), Perspectiveson nursing theory (4th ed., pp. 221-228). Philadelphia:Lippincott Williams & Wilkins.Clarke, S. P. (2006, September 28, 2006). Effects <strong>of</strong>nurses’ work environments on outcomes. Paper presentedat the Wyoming <strong>Nurse</strong>s Association Annual Conference,Casper, WY.Harrison, J. K. (2007). Influence <strong>of</strong> managed care onpr<strong>of</strong>essional nursing practice Journal <strong>of</strong> Nursing Scholarship,31(2), 161-166.Laschinger, H. K. S., & Leiter, M. P. (2006). <strong>The</strong> impact<strong>of</strong> nursing work environments on patient safety outcomes:<strong>The</strong> mediating role <strong>of</strong> burnout engagement. Journal <strong>of</strong>Nursing Administration, 36(5), 259-267.Micros<strong>of</strong>t Corporation. (2009). Encarta World EnglishDictionary: Bloomsbury Publishing Plc. Retrieved May 20,2009, from http://encarta.msn.com<strong>Nurse</strong> Practice Act (2005).Administrative rules & regulations, (2003).CorrectionsTomah Nesbitt’s tenure as Executive Director for WSBN was from 1988 to 1998. <strong>The</strong> editor apologizes for the error.Letters to the EditorFrom Susan Wiley, RN, BSN:I did not like the selection <strong>of</strong> two <strong>of</strong> the pictures in the article “100 Years <strong>of</strong> the Wyoming State Board <strong>of</strong> Nursing.”1. Why the can-can girl? Not the best image for a pr<strong>of</strong>essional nurse.2. Why the two girls in bed with quite a bit <strong>of</strong> skin showing? Is that the image <strong>of</strong> a student nurse? and it looks like they are in a double bed whichthe 1927 entry says they were not to sleep in. I understood the typewriter and the 10 dollar bill from the content <strong>of</strong> the story.4 Wy o m i n g Nu r s e Re p o r t e r
Congratulations Graduates!!<strong>The</strong> Wyoming State Board <strong>of</strong> Nursingwishes to congratulate all new graduates!We welcome you into the practice aswell as the pr<strong>of</strong>ession <strong>of</strong> nursing! If youhave questions about your application,please contact the Licensing and ExamCoordinators:Licensing and Exam Coordinators LaVelle OjedaPhone: 307-777-8620lojeda1@state.wy.us Maxine HernandezPhone: 307-777-6120mherna@state.wy.usQuestions about the “History” section <strong>of</strong> the applicationshould be directed to members <strong>of</strong> the ComplianceDepartment:Compliance Assistants Debra BallPhone: 307-777-7974dgotsc@state.wy.us Nella MartinezPhone: 307-777-5281nmarti2@state.wy.usCompliance Consultants Brenda Burnett, RN, MSNPhone: 307-777-7616bburne@state.wy.us Patti Hefflin, RN, BSNPhone: 307-777-8504pheffl@state.wy.usQuestions about the temporary graduate permit will beanswered by the Practice and Education Consultant:Assistant Executive DirectorPractice and Education Consultant Mary Beth Stepans, PhD, RNPhone: 307-777-6127mstepa@state.wy.usDo not forget that our Web site has many answers to yourquestions: http://nursing.state.wy.usWy o m i n g Nu r s e Re p o r t e r 5
Mary Beth Stepans PhD, RN<strong>Role</strong> Differentiation: What’s the Problem?Do nursing schools educate students aboutthe differences in the role and scope <strong>of</strong> practicebetween a licensed practical nurse (LPN) andregistered pr<strong>of</strong>essional nurse (RN)? Or are newgraduates “educated” by the existing nursing staffwho may never have read the <strong>Nurse</strong> PracticeAct (NPA)? Or do agencies and administratorsplace nurses in situations that create confusion?<strong>The</strong>re are no easy answers to these questions,but the problem seems to stem from a combination<strong>of</strong> underlying factors. As the Education andPractice Consultant, I receive questions on a dailybasis such as whether an LPN can serve as a unitmanager, be the sole nursing pr<strong>of</strong>essional in theemergency room, complete an Outcome and AssessmentInformation Set (OASIS) on a homehealth client, or complete the Resident AssessmentProtocols (RAPs), which is used to assessconditions identified by the Minimum Data Set(MDS) triggering mechanism. This set <strong>of</strong> circumstancesmade me realize that RNs and LPNs (aswell as their administrators) <strong>of</strong>ten do not understandthe differentiation in the levels <strong>of</strong> nursingthat are directly related to scope <strong>of</strong> practice.Nursing education programs and competencytesting (NCLEX-RN and NCLEX-PN) are designedto differentiate the levels <strong>of</strong> nursing practice.<strong>The</strong> mission <strong>of</strong> the Wyoming State Board<strong>of</strong> Nursing (WSBN) is to serve and safeguard thepeople <strong>of</strong> Wyoming through the regulation <strong>of</strong>nursing education and practice and our vision isto provide the foundation and framework essentialto support the growth <strong>of</strong> the nursing pr<strong>of</strong>ession.<strong>The</strong>refore, reviewing the Wyoming <strong>Nurse</strong> PracticeAct (NPA)(2005) and the Administrative Rulesand Regulations (2003) as they relate to scope <strong>of</strong>practice and applying the law to day-to-day situationsencountered in healthcare will further themission and vision <strong>of</strong> the WSBN.<strong>The</strong> definitions <strong>of</strong> the different levels <strong>of</strong> nursingare found in the <strong>Nurse</strong> Practice Act (33-21-120).(x) “Practice <strong>of</strong> practical nursing” meansthe performance <strong>of</strong> technical services and nursingprocedures which require basic knowledge<strong>of</strong> the biological, physical, behavioral, psychologicaland sociological sciences. <strong>The</strong>se skills andservices are performed under the direction <strong>of</strong> alicensed physician or dentist, advanced practiceregistered nurse or registered pr<strong>of</strong>essional nurse.Standardized procedures that lead to predictableoutcomes are utilized in the observation and care<strong>of</strong> the ill, injured and infirm, in provision <strong>of</strong> carefor the maintenance <strong>of</strong> health, in action directedtoward safeguarding life and health, in administration<strong>of</strong> medications and treatments prescribedby any person authorized by state law to prescribeand in delegation to appropriate assistive personnelas provided by state law and board rules andregulations;”(xi) “ ‘Practice <strong>of</strong> pr<strong>of</strong>essional nursing’ meansthe performance <strong>of</strong> pr<strong>of</strong>essional services requiringsubstantial knowledge <strong>of</strong> the biological, physical,behavioral, psychological and sociological sciences,and <strong>of</strong> nursing theory as the basis for applyingthe nursing process which consists <strong>of</strong> assessment,6 Wy o m i n g Nu r s e Re p o r t e rdiagnosis, planning, intervention and evaluation.<strong>The</strong> nursing process is utilized in the promotionand maintenance <strong>of</strong> health, case finding andmanagement <strong>of</strong> illness, injury or infirmity, restoration<strong>of</strong> optimum function and achievement <strong>of</strong> adignified death. Nursing practice includes but isnot limited to administration, teaching, counseling,supervision, delegation, evaluation <strong>of</strong> nursingpractice and execution <strong>of</strong> the medical regimen.<strong>The</strong> therapeutic plan includes the administration<strong>of</strong> medications and treatments prescribed by anyperson authorized by state law to prescribe. Eachregistered pr<strong>of</strong>essional nurse is accountable and responsiblefor the quality <strong>of</strong> nursing care rendered;”(pg. 3 <strong>of</strong> 18)Because the LPN’s “skills and services are performedunder the direction <strong>of</strong> a licensed physicianor dentist, advanced practice registered nurseor registered pr<strong>of</strong>essional nurse,” it is not withinthe LPN’s scope to serve as a unit manager orcharge nurse or as a sole nursing provider in anemergency room. <strong>The</strong>se roles require triage andclinical decision-making (Emergency <strong>Nurse</strong>s Association,1999)that are not included in the scope<strong>of</strong> practical nursing but are covered in the RN’sscope <strong>of</strong> practice as defined through the use <strong>of</strong> thewords, “administration,” “supervision,” “evaluation<strong>of</strong> nursing practice.” <strong>The</strong> AdministrativeRules and Regulations (R&R) go further to explainthe law held by the <strong>Nurse</strong> Practice Act. <strong>The</strong>internal boundaries include those forces which fallwithin the practice <strong>of</strong> pr<strong>of</strong>essional nursing.Chapter III, Section 3 (a)(C)(III) in the R&Rsfurther outlines LPN practice with the mandatethat in “complex patient care situations” (acutecare setting, for example) the care provided by theLPN must be under the “supervision <strong>of</strong> a licensedphysician, dentist or licensed pr<strong>of</strong>essional nurse”(pg 3-5). ‘Supervision’ means the immediateavailability <strong>of</strong> a licensed physician, dentist or registeredpr<strong>of</strong>essional nurse in the same patient careunit to continually observe, assist, coordinate andevaluate in person the practice <strong>of</strong> another” (ChapterI,(a)(Ix) pg 1-8). For example, if an LPN is towork in a labor and delivery area or intensive careunit, continuous supervision must be available.In other situations, like long term care, LPNs“provide care for clients in basic patient caresituations under the direction <strong>of</strong> a licensed physician,dentist or licensed pr<strong>of</strong>essional nurse. Basicpatient care situations as determined by a licensedphysician, dentist or licensed pr<strong>of</strong>essional nursemean the following three (3) conditions prevail atthe same time in a given situation:(1.) <strong>The</strong> client’s clinical condition is predictableand the responses <strong>of</strong> the client to the nursingcare are predictable;(2.) Medical or nursing orders do not changefrequently and do not contain complex modifications;and(3.) <strong>The</strong> client’s clinical condition requiresonly basic nursing care” [Chapter III, Section 3(a)(C)(II) pg 3-5].Thus, in basic care situations, the word “direction”is applicable.“ ‘Direction’ means the intermittent observation,guidance and evaluation <strong>of</strong> the nursingpractice <strong>of</strong> another by a licensed physician, dentistor registered pr<strong>of</strong>essional nurse who may onlyoccasionally be physically present; or joint development<strong>of</strong> a plan <strong>of</strong> care in advance by those individualsinvolved which will be implemented byothers without the physical presence <strong>of</strong> a licensedphysician, dentist, or registered pr<strong>of</strong>essional nurse.In the latter situation, a licensed physician, dentistor registered pr<strong>of</strong>essional nurse shall be availablefor consultation in the event circumstancesarise that cause consultation to be necessary. <strong>The</strong>degree <strong>of</strong> direction needed shall be determined byevaluation <strong>of</strong> the patient care situation, and theeducational preparation and demonstrated pr<strong>of</strong>iciency<strong>of</strong> others” (Chapter I,(a)(xx)iii pg 1-5).Another issue that frequently comes to my attentionis the LPN’s scope <strong>of</strong> practice as it relatesto assessment. Chapter 3 (Standards <strong>of</strong> NursingPractice), Section 3 (a) indicates that it is withinthe LPN’s scope <strong>of</strong> practice to:“A) Contribute to the nursing assessment by:(I) Collecting, reporting and recording objectiveand subjective data in an accurate and timelymanner. Data collection includes:(1.) Observation about the condition or changein condition <strong>of</strong> the client(2.) Signs and symptoms <strong>of</strong> deviation fromnormal health status” (pg. 3-4).“Contributing to the nursing assessment”means that there must be an initial assessmentcompleted by the RN, APRN or physician. Inaddition, federal rules associated with RAPs andOASIS specifically indicate that a registered pr<strong>of</strong>essionalnurse must complete these assessments.Collecting vital signs, allergies, medications andchief complaint is within the LPN’s scope <strong>of</strong> practice.However, the rest <strong>of</strong> the assessment must bedone by the RN. It is never appropriate to “cosign”unless both parties have witnessed and donethe same thing---for example, wasted a portion <strong>of</strong>a narcotic dose. Does this mean that the LPN’scontribution to care is less valued? Absolutelynot! Once the initial assessment is completed, theLPN’s technical skills are invaluable in monitoringthe client’s condition.Laws that govern nursing practice are based oneducational level and the national competencyexam (NCLEX). It is each licensee’s responsibilityto know and work within their scope <strong>of</strong> practice.Administrators are held to the additionalstandard <strong>of</strong> knowing the scope <strong>of</strong> practice, as wellas the unique skill set, experience and potentialcontributions that each member <strong>of</strong> the nursingcare team provides.Dr. Mary Beth Stepans is the assistant executivedirector and the practice and education consultantfor the Wyoming State Board <strong>of</strong> Nursing.ReferencesNPARules & REgsEmergency Nursing Association http://www.ena.org/publications/scopes/
Debra Ansombe Wood, RNCopyright 2008. Nursing Spectrum <strong>Nurse</strong> Wire(www.nurse.com). All rights reserved. Used withpermission.Focus on Practice: Nursing research clarifiesbest practices for blood pressure measurementAfter noticing that colleagues were measuringblood pressure on two different parts<strong>of</strong> patients’ arms, a team <strong>of</strong> Christiana CareHealth System nurses questioned whether thepractice yielded accurate results. Staff memberssometimes took readings on the forearminstead <strong>of</strong> the upper arm, the location consideredoptimal by the American Heart Association,because a large cuff was unavailable orthey perceived patient discomfort.<strong>The</strong> initiative <strong>of</strong> these nurses resulted ina research project that led to improved patientcare and expanded the pr<strong>of</strong>essions’ understandingabout how to accurately measureblood pressure.“It has made nurses see we can do studies,too, and we have something to add to thebody <strong>of</strong> knowledge on blood pressure,” saysKathleen Schell, RN, DNSc, assistant pr<strong>of</strong>essorat the University <strong>of</strong> Delaware in Newarkand lead author <strong>of</strong> two articles about the studypublished in the American Journal <strong>of</strong> CriticalCare. “Blood pressure is viewed as a mundanetask,” Schell says. “Yet it’s so important. Icannot tell you how many beta blockers orheart medications are given based on bloodpressure.” <strong>Nurse</strong>s use blood pressure readingsto make decisions about holding medicationsor adjusting dosages, and the readings help determinewhether nurses need to call the physicianfor further consultation, says Linda Bucher,RN, DNSc, nursing research facilitatorat Christiana Care Health System in Wilmington,Delaware, and associate pr<strong>of</strong>essor <strong>of</strong>nursing at the University <strong>of</strong> Delaware.Tackling a research question<strong>The</strong> first step for the research team---composed <strong>of</strong> staff nurses, advanced practicenurses, staff development nurses, and universityfaculty members---was to do a review <strong>of</strong>the literature. <strong>The</strong>y found limited data aboutthe practice <strong>of</strong> taking blood pressure in theforearm. <strong>The</strong> nurses formulated a researchquestion, obtained institutional review boardapproval, and began collecting data at theWilmington Hospital and Christiana Hospitalemergency departments.Blood pressure readings were obtainedfrom 204 clinically stable patients, followingthe 1993 American Heart Association standards—thepatient sitting up with the arm atheart level. Trained data collectors measuredthe upper arm and forearm circumferencesand used appropriately sized cuffs to take measurementsin the upper arm and lower arm.When the nurses analyzed their findings, theydiscovered the readings were not interchangeable.“We found significant differences betweenthe two numbers,” Bucher says. “We didn’texpect to see as large a difference as we did.Some <strong>of</strong> the [systolic] readings were as muchas 30 mmHg different. You might have 130mmHg in the upper [arm] and 100 mmHg inthe forearm, or vice versa. <strong>The</strong>re was no wayto predict.” <strong>The</strong> Christiana Care-University<strong>of</strong> Delaware team then conducted a secondstudy, comparing forearm and upper armblood pressure measurements in 221 medical/surgical inpatients positioned supine—flat inbed, with the head <strong>of</strong> bed elevated 45 degrees.<strong>The</strong> nurses again found wide variations andconcluded the measurements were not interchangeable.Research changes practiceBased on this evidence, Christiana Caredeveloped a clinical practice guideline fornurses and techs outlining how to take bloodpressure readings. <strong>The</strong> hospital developedan Internet-based educational module andrequired all nurses and techs to complete it.<strong>Nurse</strong> managers purchased cuffs in differentsizes to make upper arm measurements morecomfortable, as well as more accurate, forpatients. If a valid reason still exists for takinga forearm reading, the nurse or tech mustdocument the reason and site <strong>of</strong> the measurementin the patient’s chart. Subsequent bloodpressure measurements should be done usingthe same location so clinicians can evaluatetrends.To follow up on the new guideline, ChristianCare completed a performance improvementproject about a year after implementationto determine employee compliance.Departments with low rates <strong>of</strong> compliancewere targeted for a re-education campaign.Research has broader application<strong>The</strong> nurses’ research served as a basis for apractice alert about noninvasive blood pressuremonitoring issued by the American Association<strong>of</strong> Critical-Care <strong>Nurse</strong>s (AACCN) in2006. <strong>The</strong> Christiana Delaware team helpeddraft the alert, based on its project, which wasfunded in part by a grant from the AACCN’sSoutheastern Pennsylvania chapter, and otherstudies. Honor Society <strong>of</strong> Nursing, Sigma<strong>The</strong>ta Tau International awarded the team theprestigious Research Dissemination Award,which recognizes a major contribution to thedissemination <strong>of</strong> research for use in clinicalnursing practice, education, administration,research or public knowledge.Christiana Care values nursing research,Bucher says. “When nurses are taking care<strong>of</strong> you 24/7, you hope what they are doing isresearch-based and reflects best practice. Andwhen there are questions, those nurses knowhow to turn those questions into researchstudies and find the answers, so the quality <strong>of</strong>care at the bedside is the best we can <strong>of</strong>fer.”Debra Anscombe Wood, RN, is a freelance writer.NCLEX REGIONAL WORKSHOP FOR EDUCATORS DECLARED A SUCCESS!<strong>The</strong> Wyoming State Board <strong>of</strong> Nursing and Laramie County Community College (LCCC) hosted a NCLEX Regional Workshop for Educators May 17 and 18,in Cheyenne at Laramie County Community College. Marlene Ethier, from Western Wyoming College in Rock Springs, started the workshop with a meetand greet on Sunday evening to discuss nursing issues in Wyoming. Nicole Kent, MSN, RN-BC and Katherine Brown, MSN, MHA, RN from the NationalCouncil <strong>of</strong> State Boards <strong>of</strong> Nursing (NCSBN) shared information about the NCLEX exam with 75 nurse educators from Wyoming, Colorado and Nebraska.Highlights <strong>of</strong> the program included a hands-on item writing demonstration to show the audience how to apply principles <strong>of</strong> item writing in the NCLEX style.NCLEX Program Reports were also explored so that faculty take full advantage <strong>of</strong> the information <strong>of</strong>fered in these reports by identifying the strengths andweaknesses <strong>of</strong> their graduates. Dr. Joseph Stepans, Pr<strong>of</strong>essor Emeritus from the University <strong>of</strong> Wyoming, College <strong>of</strong> Education, also shared educational strategiesthat emphasize “learning and inquiry” rather than “teaching”. Since this will become an annual event, several <strong>of</strong> the educators requested that Dr. JosephStepans be invited to further explore innovative teaching strategies.Wy o m i n g Nu r s e Re p o r t e r 7
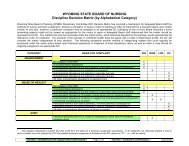
Scope <strong>of</strong> Practice Issues and the Decision TreeMary Beth Stepans, PhD, RNArlis Wozniak, RN<strong>The</strong> spring 2009 issue <strong>of</strong> the Wyoming <strong>Nurse</strong>Reporter presented the WSBN’s decision to usethe Decision Model to guide and direct nursingpractice. In addition, licensees were notifiedthat the board rescinded a number <strong>of</strong> practicedecisions. This article will further explainthe application <strong>of</strong> the decision model anddemonstrate that while the use <strong>of</strong> the DecisionModel replaces the need for the majority <strong>of</strong>advisory opinions, it does not really change many<strong>of</strong> the practice decisions. When each <strong>of</strong> thepractice advisory opinions was reviewed withinthe context <strong>of</strong> the Decision Model, only a fewwere retained because the Decision Model ledthe Practice Committee members to the sameconclusion. For example, one might ask, “Whywould the board rescind the final version <strong>of</strong> theadvisory opinion Peripheral Insertion <strong>of</strong> CentralVenous Catheters with or without the ModifiedSeldinger Technique (MST) with UltrasoundGuidance, RN (07-177) after putting in somuch effort to ‘get it right’?How would usingthe Decision Model lead to the same or betterconclusion?” To answer these questions, thedecision-making process will be illustrated usingthe PICC line insertion topic.Define the Activity/Taska. What is the problem or need?i. Using the “old” method <strong>of</strong> placing PICC(peripheral inserted central catheter) lines(Advisory Opinion 94-58) utilizing a 14gintroducer needle in the antecubital space isno longer considered the best practice in thePICC line insertions. Studies have showna decrease in complications and a muchimproved success rate utilizing the ModifiedSeldinger Technique (MST) with ultrasoundguidance (LaRue, 2000; Runde, 2007). <strong>The</strong>question is “are Wyoming RN’s allowed to useultrasound and MST for PICC placement?ii. Insertion by a physician is expensive forclients and requires much “wait time” (Kokotis,2005).b. Who are the people involved in thedecision?i. Registered pr<strong>of</strong>essional nurses (RNs) andphysicians as well as administrators in the acutecare setting should be involved.c. What is the decision to be made andwhere will it take place?i. <strong>The</strong> decision is whether (RNs) may use theMST with ultrasound guidance to insert PICClines.d. Why is the question being raised now?i. <strong>The</strong>re is new technology available makingthe PICC line insertion procedure safer, moresuccessful and less expensive for clients.2. Is the activity permitted by Wyoming <strong>Nurse</strong>Practice Act?i. Since PICC line insertion is permittedusing Advisory Opinion 94-58, the activity ispermitted.3. Is the activity/task precluded under anyother law, rule or policy?i. No law or rule precludes performance <strong>of</strong> thistask by RNs.ii. Note: check agency policy to determinewhether there is an agency policy thatprecludes the performance<strong>of</strong> this task by a RN.4. Is the act supported by the Standards <strong>of</strong>Nursing Practice (ANA), basic educationpreparation, or position statements from thepr<strong>of</strong>essional organization most relevant to thepractice question being asked, and research datain nursing and health related literature?i. Radiology Nursing: Scope and Standards<strong>of</strong> Practice (2007) do not specifically addressthe RN’s role in insertion <strong>of</strong> PICC lines usingMST. However, the document does addressthe RN’s role in knowing about technologicaladvances that affect patient care.ii. <strong>The</strong> Association for Vascular Access andInfusion <strong>Nurse</strong>s Society position statementsendorse placement <strong>of</strong> PICC s using MST byRNs who have demonstrated appropriatetraining (Association for Vascular Access,2005; Infusion <strong>Nurse</strong>s Society, 2003).iii. Research supports this technology toimprove patient outcomes (McMahon, 2002).*If the decision is to proceed, the next step is to writea policy that uses the content <strong>of</strong> the Association forVascular Access’s position statements and/or Infusion<strong>Nurse</strong>s Society’s practice standards outlining optimaltraining, validation <strong>of</strong> competency, and requirementsfor ongoing competency & skills assessment.5. Has the nurse completed special education ifneeded?i. Training programs for this technique are<strong>of</strong>ten <strong>of</strong>fered at the annual conferences <strong>of</strong>the American Radiology <strong>Nurse</strong>s Associationand Association <strong>of</strong> Vascular Access. Manyprivate teaching companies, such as “PICCExcellence” are available. Also, many PICCmanufacturers (Bard, Boston Scientific etc.)provide training classes.*<strong>The</strong> policy should include a statement aboutrequired education.6. Does the nurse possess appropriateknowledge?i. <strong>The</strong> Infusion <strong>Nurse</strong>s Society generated acompetency checklist for the RN to performthis procedure (Infusion <strong>Nurse</strong>s Society, 2003).*<strong>The</strong> agency policy should include a competencychecklist.7. Is there documented evidence <strong>of</strong> experienceand initial and continued competence?i. As above.*<strong>The</strong> agency policy should establish criteriafor initial and continued competency. Thisbecomes crucial when a highly technical skillthat may be used infrequently is considered. Forexample, the WSBN felt that 25 documentedsuccessful insertions per year on a specific patientpopulation (adult or pediatric) were necessary tomaintain competency. This should be based uponnational guidelines or research.Once appropriate knowledge, experience andcontinued competency are established to beadequate, the following questions apply to theparticular situation with a particular client:8. Would a reasonable & prudent nurseperform the act?9. Is patient safety assured?10. Is the nurse prepared to accept theconsequences <strong>of</strong> action?SummaryUsing this Decision Tree Model process led us tothe same conclusion that was agreed upon in thepractice advisory opinion issued by the WSBNin October 2008. When nurses in each agencyuse this process, they become familiar withhow to access and utilize information and makedecisions about their scope <strong>of</strong> practice basedon best nursing practices. By using this modelfor practice decisions, the WSBN contributedto their vision: To provide the foundation andframework essential to support the growth <strong>of</strong> thenursing pr<strong>of</strong>ession. Become empowered and growin your pr<strong>of</strong>ession! Develop an agency policyusing the Decision Tree! And don’t forget to adda reference list at the end <strong>of</strong> the policy so thatyou’ll know when to perform another literaturereview!!Acknowledgements: Nina Elledge, RN, CRNI,MBA and Arlis Wozniak, RN provided much<strong>of</strong> the information for this article when theywrote to the Wyoming State Board <strong>of</strong> Nursingrequesting revisions <strong>of</strong> Practice Advisory Opinion07-177. <strong>The</strong>ir work on this topic is reflective <strong>of</strong>the process that must be used in guiding practice.<strong>The</strong>y used the same process that is outlined bythe Decision Tree Model when they preparedmaterials for the board to consider!Dr. Mary Beth Stepans is the assistant executivedirector as well as the practice and educationConsultant for the Wyoming State Board <strong>of</strong>Nursing. Arlis Wozniak is a registered nurseworking in the Radiology Department atMemorial Hospital <strong>of</strong> Sheridan County.ReferencesAmerican Radiological <strong>Nurse</strong>s Association and American<strong>Nurse</strong>s Association. (2007). Radiology nursing: Scopeand standards <strong>of</strong> practice. Silver Spring, Maryland:American <strong>Nurse</strong>s Association.Association for Vascular Access. (2005). Use <strong>of</strong> modifiedSeldinger technique for peripherally inserted centralcatheter placement by registered nurses. Retrieved May9, 2009, from http://www.avainfo.org/website/download.asp?id=193200.Infusion <strong>Nurse</strong>s Society. (2003). Central vascular accessdevice competencies.KoKotis, K. (2005). Cost containment and infusionservices. Journal <strong>of</strong> Infusion Nursing, 28(35), S22-S32.LaRue, G.D. (2000). Efficacy <strong>of</strong> ultrasonography inperipheral venous cannulation. Journal <strong>of</strong> IntravenousNursing, 23(1), 29-34.McMahon, D.D (2002). Evaluating new technologyto improve patient outcomes: A quality improvementapproach. Journal <strong>of</strong> Infusion Nursing, 25(4), 250-255.Runde, D. (May, 2007). Ultrasound andmicrointroduction PICC Insertion success rates. Infusion<strong>Nurse</strong>s Society Annual meeting 2007.Wyoming State Board <strong>of</strong> Nursing (2009). Scope <strong>of</strong> practicedecision tree model.8 Wy o m i n g Nu r s e Re p o r t e r
Scope <strong>of</strong> Practice Decision Making ModelDefine the Activity/Task, Identify, Describe, Clarify Problem/Need.Can task bedelegated?Is the activity consistent withWyoming <strong>Nurse</strong> PracticeAct/Advisory Opinion?NoNoChapter 9StopYesUnsureIs the activity precluded underother law, rule or agency policy?YesStopNoIs the act supported by Standards<strong>of</strong> the Nursing Practice, basiceducational preparation, or scope <strong>of</strong>practice statements from pr<strong>of</strong>essionalNursing organizations, and researchdata in nursing and health relatedliterature?NoStopConsiderreferral toWSBNYesHas the nurse completed specialeducation if needed?NoStopYesDoes the nurse process theappropriate knowledge?NoStopYesIs there documented evidence <strong>of</strong> experience and initial and continued competence?YesNoStopWould a reasonable and prudent nurse perform the act?YesNoStopIs patient safety assured?YesNoStopYesIs the nurse prepared to assume accountability for the act ordelegation and for the outcome <strong>of</strong> the care?NoStop<strong>Nurse</strong> may perform theactivity/task according toacceptable and prevailing standards<strong>of</strong> safe nursing careIf you answered NO to any <strong>of</strong> the above questions, defer to apr<strong>of</strong>essional qualified to do the activity or task.ORDefer to the Wyoming State Board <strong>of</strong> Nursing for an AdvisoryOpinionWy o m i n g Nu r s e Re p o r t e r 9
Marcia L. Dale, RN, EdD, FAANTitle Protection: What does it mean interms <strong>of</strong> the Christian Science <strong>Nurse</strong>?<strong>The</strong> Directory <strong>of</strong> Christian Science CareFacilities provides contact information on 19Visiting <strong>Nurse</strong> Services (http://www.christianscienceinfo.com/directory.htm).Onlyone <strong>of</strong> these agencies indicates that it is aChristian Science Nursing service giving theclue that the “visiting nurse” is not a licensednurse. <strong>The</strong> confusion that this creates is obvious.I would have expected that it wouldbe illegal to use the title “nurse” to describeoneself unless licensed as a nurse. However,“there are just nine states that do not accommodatethe practice <strong>of</strong> Christian Science<strong>Nurse</strong>s” (Christian Science North Carolina,http://christiansciencenc.org/). This problemwill increase unless states legislate titleprotection. For example, House Bill 1286was introduced in April in North Carolinato allow Christian Science <strong>Nurse</strong>s to practiceand be recognized with the title “nurse” withoutthe education and training that licensednurses must attain.Within the section on “violations”, theWyoming <strong>Nurse</strong> Practice Act indicates thefollowing:(a) No person shall:(i) Engage in the practice <strong>of</strong>nursing as defined in this act [§§ 33 21 119through 33 21 156] without a valid, currentlicense or temporary permit, except as otherwisepermitted under this act;(ii) Practice nursing under cover <strong>of</strong> anydiploma, license or record illegally or fraudulentlyobtained or signed or issued unlawfullyor under fraudulent representation;(iii) Use any words, abbreviations,figures, letters, titles, signs, cards or devicestending to imply that the person is a registerednurse, licensed practical nurse or advancedpractice registered nurse unless theperson is duly licensed as a registered nurse,licensed practical nurse, or recognized as anadvanced practice registered nurse under thisact; (33 21 14, pg 12 <strong>of</strong> 18).<strong>The</strong>re is also a section in the Wyoming<strong>Nurse</strong> Practice Act that protects the titles <strong>of</strong>registered nurse (RN), and advanced practiceregistered nurse (33-21-134), licensed practicalnurse (LPN) (33-21-135), graduate pr<strong>of</strong>essionalnurse (GN) and graduate advancedpractice registered nurse (GAPRN)(33-21-136) as well as graduate practical nurse(GPN)(33-21-137). However, this may notbe enough to prevent one from using the term“Christian Science <strong>Nurse</strong>” in Wyoming.<strong>The</strong> qualifications <strong>of</strong> a licensed nurse anda Christian Science <strong>Nurse</strong> are not to be confused.<strong>The</strong> difference is formal education andestablished competency. This article willdescribe the history and educational background<strong>of</strong> Christian Science Nursing.HistoryMary Baker Eddy, because <strong>of</strong> her ownpersonal experiences <strong>of</strong> achieving healingthrough the Divine Mind, God, wrotea book in 1875, now known as Science andHealth with Key to the Scripture. In 1879,she founded the Church <strong>of</strong> Christ, Scientist.It is a Christian denomination based on JesusChrist’s teachings and works. Believerschoose to heal themselves and their childrenthrough prayer, rather than through the use<strong>of</strong> conventional health care. <strong>The</strong> believerprays for himself but may utilize a practitionerto give prayer assistance. A “practitioner” is afull-time believer who provides assistance tothe ill. <strong>The</strong> “practitioner” does not heal, butseeks the guidance <strong>of</strong> God (Robinson, 2007,p. 3).A Christian Science nurse is a person whohas knowledge <strong>of</strong> Christian Science practices,thoroughly understands the practicalwisdom required in a sick room, and can carefor a sick person (Church Manual, p. 49).<strong>The</strong> Christian Science nurse carries out theChristian Science beliefs in daily living andin the care <strong>of</strong> the sick (<strong>The</strong> Christian Science<strong>Nurse</strong>, 2007, p. 1).Eddy states that “the nurse should becheerful, orderly, punctual, patient, full <strong>of</strong>faith,--receptive to Truth and Love” (Eddy,1895, p. 395). <strong>The</strong> role <strong>of</strong> the Christian Sciencenurse is to provide physical care, comfort,and a normalcy for the patient. <strong>The</strong> sickperson’s role is to grow spiritually in order toheal himself. In order for this to take place, anatmosphere free <strong>of</strong> fear and conducive to faithin God must be maintained. <strong>The</strong> ChristianScience nurse supports the patient’s relianceon spiritual healing. <strong>The</strong> Christian Sciencenurse does not make a record <strong>of</strong> symptoms orconditions, administer medications or drugs,use medically-oriented techniques, massage,or physical therapy; does not give advice, norbecome involved in the relationship betweenthe patient, the Christian Science practitioner,nor his family.On the other hand, Christian Sciencenursing care does include the idea that immediatehealing will occur and encompasses givingspiritual reassurance; encouraging normalactivity; reading from the Bible and writingsby Mary Baker Eddy; communicating withthe Christian Science practitioner and familymembers; giving personal care; giving mobilityassistance, nourishment, instruction, anddressing wounds (2007, <strong>The</strong> Christian Science<strong>Nurse</strong>, pp. 1-2).Fourteen programs, thirteen in the UnitedStates, were found that taught classes inChristian Science nursing. <strong>The</strong> educationusually consists <strong>of</strong> classroom instruction andhands-on experience under the supervision<strong>of</strong> a mentor. <strong>The</strong> curriculum averages eighteenweeks in length. Topics <strong>of</strong> instructioninclude ethics, principles, and Christian Sciencenursing arts. One school <strong>of</strong>fered oneweek <strong>of</strong> maternity care. Upon completion <strong>of</strong>a course <strong>of</strong> study, the Christian Science nursemay advertise as a Christian Science nurse.<strong>The</strong> term “nurse” is not necessarily protectedin the state <strong>of</strong> Wyoming even though“RN”, “LPN”, “APRN”, “GN”, “GPN”, and“GAPRN” are protected titles. Using thenurse title is problematic because <strong>of</strong> the implicationsit has to members <strong>of</strong> the public.Summary<strong>The</strong> mission <strong>of</strong> the WSBN is to serve andsafeguard the people <strong>of</strong> Wyoming through theregulation <strong>of</strong> nursing education and practice.This mission is jeopardized when the title“nurse” is used by those who lack both theeducation and competency to be licensed assuch.ReferencesAmerican <strong>Nurse</strong>s Association. (2006).Faith community nursing: Scope & standards <strong>of</strong>practice. Silver Springs, MD: American <strong>Nurse</strong>sAssociation & Health Ministries Association.Baker, M.E. (1895). <strong>The</strong> manual <strong>of</strong> themother church. Retrieved April 28, 2009,from http://marybakereddy, rolf-witzsche.com/Mary=Baker-Eddy-Church-Manual/chapter.html.Christian Science Nursing (2008, August 1).Christian science nurse education. RetrievedApril 28, 2009, from http://www.aocsn.org/<strong>Nurse</strong>Education.htm.Christian Science Nursing (2007, December2). <strong>The</strong> Christian science nurse. RetrievedApril 28, 2009 from http://www.aocsn.org/<strong>The</strong> CS<strong>Nurse</strong>.htm .Robinson, B.A. (2007). <strong>The</strong> church <strong>of</strong>Christ, scientist. Retrieved April 28, 2009 fromhttp://www.religiousrolerance.org/cr_sci.htm.Christian Science Churches in North Carolina.(n.d.). House bill 1286: Christian sciencenursing/nursing practice act. Retrieved May 13,2009 from http://christiansciencenc.org/North Carolina <strong>Nurse</strong>s Association. (n.d.).Strong action from NCNA sidelines threat tonurse title. Retrieved May 13, 2009 from http://www.ncnurses.org/ncna_programs.asp10 Wy o m i n g Nu r s e Re p o r t e r
Mary Beth Stepans, PhD, RNCertified Nursing Assistant II (CNA II) withMedication Administration CertificationDuring the regularly scheduled meeting theWyoming State Board <strong>of</strong> Nursing (WSBN),the Board <strong>of</strong> Nursing approved the release <strong>of</strong>draft proposed rules “CNA II with medicationcertification” to provide education and getfeedback from nurses, facilities and the generalpublic, in preparation for adoption by the board.Presentation Objectives:• To present the proposed new role <strong>of</strong> CNA IIwith medication administration certification;• Explain how expansion <strong>of</strong> CNA scope<strong>of</strong> practice can enhance patient safety andimprove the working environment for nurses;• Present research related to patient safety andevidence that supports expanding CNA scope<strong>of</strong> practice; and• To solicit input and feedback from nurses andhealthcare stakeholders throughout the statefor the purpose <strong>of</strong> clarifying the proposed rules.Stakeholders who may have questions or concernswith these draft rules and what it means to nursingpractice here in Wyoming are invited to attend.Schedule:Wednesday June 101:30-3pm: LaramieIvinson Memorial Hospital,Grand RoomTuesday June 16th8am-9am: CasperWyoming Health Care AssociationParkway Plaza, Champagne RoomWednesday, June 17th3- 4:30pm: State Video ConferencingSystem (see next page for locations)Safe administration <strong>of</strong> medications by competentand trained personnel is the goal that broughtthese members <strong>of</strong> the committee together.• Cheri Benander (Vice President, ResidentCare Services, Powell Valley Health Care),• LouAnn Carmichael (Director <strong>of</strong> Operations,South Lincoln Medical Center),• JoAnn Farnsworth (Weston County HealthServices),• Mary Kay Goetter (Executive Director,Wyoming State Board <strong>of</strong> Nursing)• Marguerite Herman (Consumer, WyomingState Board <strong>of</strong> Nursing),• Faith Jones (Vice President, Patient CareServices, Powell Valley Health Care),• Tom Jones (Executive Director, WyomingHealth Care Association),• Dan Lex (Executive Director, Quality Healthcare Foundation),• Chris Newman (Deputy Administrator,Division <strong>of</strong> Disabilities),• Cyndy Rankin (Executive Director, WestviewHealth Care Center, Sheridan)• Mary Beth Stepans (Practice & EducationConsultant, Wyoming State Board <strong>of</strong>Nursing).Current Administrative Rules and Regulations,lack <strong>of</strong> funding, and scarce resources force someagencies to “go around” the rules and use untrainedpersonnel to administer medications under the“friend <strong>of</strong> the family” exemption to the <strong>Nurse</strong>Practice Act (33-21-154). Other agencies cannotuse their pr<strong>of</strong>essional staff to the fullest extentbecause <strong>of</strong> the time-intensive task <strong>of</strong> medicationadministration. Hospital and Nursing HomeAdministrators are strained by the need to adhereto overwhelming guidelines related to quality <strong>of</strong>care, control cost and maintain patient and staffsatisfaction. Governor Freudenthal directed theWSBN to collaborate with multiple stakeholdersto explore options for meeting Wyoming’s multiplehealthcare challenges and economic realities whilestill fulfilling our mission <strong>of</strong> public protection. Inanswer to these issues, the CNA II with medicationadministration certification role was drafted, basedupon the National Council <strong>of</strong> State Boards <strong>of</strong>Nursing (NCSBN) Model Rules for the CNA IIand Medication Assistant-Certified (MA-C). <strong>The</strong>following information was provided by members<strong>of</strong> the committee to provide answers to questionsthat might be posed about this new role.Long Term Care and Acute Care prospective(Faith Jones - Powell Valley Health Care--acute care; LouAnn Carmichael-South LincolnMedical Center- long-term care)1. How does adding the CNA II benefit thenursing pr<strong>of</strong>ession in Wyoming?<strong>The</strong> CNA II is one forward-thinking solution tothe long term problem <strong>of</strong> the nursing shortage.<strong>The</strong> CNA II provides a development path forthe CNA as well as enhancing the leadershipskills <strong>of</strong> the licensed nurse. <strong>The</strong> addition <strong>of</strong>these advanced skills will enable the CNAII to build confidence that can improve thelikelihood <strong>of</strong> successful completion <strong>of</strong> an RNprogram in their future.2. Can a CNA II be used in the acute caresetting?Yes, the CNA II with advanced skills can bedelegated to provide care to stable patients inany setting. <strong>The</strong> delegation <strong>of</strong> these tasks ispatient-centered and at the discretion <strong>of</strong> thelicensed nurse.3. Who will have control over the tasks thatare delegated to the CNA II?<strong>The</strong> licensed nurse will determine which tasksto delegate. By working in partnership withthe CNA II, the licensed nurse will retain his/her autonomy <strong>of</strong> practice as manager <strong>of</strong> thepatient’s plan <strong>of</strong> care.4. How is this going to help the nurse in LongTerm Care?A CNA II will be able to help with thoseresidents who require supervision and assistanceduring medication administration process.5. How does this help the workload <strong>of</strong> theCNAs who already have too much to do?Work flow for a CNA II should be enhanced.For example, a CNA II will be able to applysome topical medications, speeding up theprocess <strong>of</strong> resident care after a bath or during therush <strong>of</strong> getting up for breakfast in the morning.CNA IIs will also be able to adjust oxygen flowrates that may have been inadvertently altered,thereby eliminating or reducing the need forinterrupting the licensed nurse.Assisted Living Perspective (Cheri Benander- Powell Valley Health Care)1. In an Assisted Living facility, licensednurses are not always onsite. Will this preventCNA II’s ability to administer medications?No. Detailed instructions developed bythe licensed nurse will guide the CNA IIin medication administration. In addition,directions for PRN medications must bein writing and include the parameters forprovision <strong>of</strong> the PRN medication. Directionsfor observing, reporting, and monitoringmedication must be in writing.2. Can the CNA II administer all medicationsin all situations?No. <strong>The</strong> delegating nurse determines whichmedications can be administered by the CNAII. In delegating, the nurse uses pr<strong>of</strong>essionalnursing judgment as well as the AdministrativeRules and Regulations to guide decisions.3. Will there be any type <strong>of</strong> grandfatheringsystem developed for CNAs with severalWy o m i n g Nu r s e Re p o r t e r 11
years <strong>of</strong> experience?No. <strong>The</strong> CNA II requires additional educationabove and beyond a CNA. All CNAs desiringto advance to the higher level <strong>of</strong> practice will berequired to complete the additional course andtesting. Additionally, a person cannot becomea CNA II unless currently certified as a nursingassistant.Home Health Perspective (JoAnn Farnsworth-WCHS)1. What is the nurse’s liability if a CNA II doesnot follow instructions and harms a patient intheir home when the nurse is NOT on site?<strong>The</strong> liability is the same as with any other dutiesdelegated by a nurse to a CNA.2. Would this phase out nurses?No. <strong>The</strong> CNA II is there to assist in the workloadUNDER THE DIRECTION/SUPERIVISION <strong>of</strong>a licensed nurse ONLY. CNA II scope <strong>of</strong> practicedoes not include assessments, interpretations ordecision making at the level <strong>of</strong> the pr<strong>of</strong>essionalnurse.Division <strong>of</strong> Disabilities Perspective (ChrisNewman – Division <strong>of</strong> Disabilities)Background:<strong>The</strong> majority <strong>of</strong> community based servicesfor people with developmental disabilities andacquired brain injuries are funded by home andcommunity based waivers administered by theWyoming Department <strong>of</strong> Health, DevelopmentalDisabilities Division (the Division). Waiversprovide federal funding for services to participantsat risk <strong>of</strong> being placed in an institution so they canbe supported in their homes and communities,living as independently as possible among familyand friends at an average cost that is lower thanthat <strong>of</strong> institutional care. Services funded by thewaivers include residential habilitation services,day habilitation services, respite care, personal care,AftonLaw Enforcement/Sheriff’sOfficePublic Health <strong>Nurse</strong>sOffice421 JeffersonAfton, WY 83110Seating Capacity 10BasinRetirement Center890 Why 20 SouthBasin, WYSeating Capacity 14BuffaloVeterans Home700 Veterans LaneBuffalo, WY 82834Seating Capacity 20CasperWorkforce Center851 Werner Court,Suite 121Casper, WY 82601Seating Capacity 25case management and some therapy services notcovered under the Medicaid State Plan. Peoplereceiving waiver services live in their own homesand communities across Wyoming; they may live ina family home group home, or their own residence.<strong>The</strong> three waivers administered by the Divisionalso fund skilled nursing services, defined as serviceslisted in the individual plans <strong>of</strong> care that are withinthe scope <strong>of</strong> the Wyoming <strong>Nurse</strong> Practice Act. <strong>The</strong>seservices, including medication administration,must be authorized by a physician. <strong>The</strong> majority<strong>of</strong> participants receiving services on the waiversdo not require medication administration, butmost need some support and prompting to assuremedications are taken.Providers:<strong>The</strong> Division certifies approximately 930providers. Thirty <strong>of</strong> these providers are organizationswho are required to meet national accreditationstandards, including standards requiringcomprehensive training and documentation <strong>of</strong>medication administration. <strong>The</strong>se organizationsemploy direct support pr<strong>of</strong>essionals (DSPs) toprovide services around the clock, includinghabilitation services, personal care and respite.Approximately 900 providers are self-employedor independent providers, and over 400 <strong>of</strong> theseproviders provide respite and/or personal careservices to participants on the Children’s DDWaiver. Eleven organizations and 35 independentregistered nurses are certified to provide skillednursing.Current issues:For participants who require medicationadministration, it has been very difficult forHome and Community Based Waiver providerorganizations to hire and retain nurses to meetthe need 24 hours a day, seven days a week.According to providers, this difficulty is due to thenursing shortage, nurses wanting positions thatState Video Conferencing SitesCheyenneCity Center Building1920 Thomes Avenue,Suite 410Cheyenne, WY 82001Seating Capacity 14CodyWorkforce Center1026 BlackburnCody, WY 82414Seating Capacity 18EvanstonEmployment Services98 IndependenceEvanston, WY 82930Seating Capacity 16GilletteWorkforce Center1901 Energy Court,Suite 230Gillette, WY 82718Seating Capacity 25JacksonWorkforce Center155 West GillJackson, WY 83001Seating Capacity 12KemmererBurgoon Building136 Burgoon Drive(Also known as 20Advil Drive)Diamondville, WY83116Seating Capacity 15LanderState Training SchoolRothwell Building,Atlantic Room100 Meadow ViewDriveLander, WY 82520Seating Capacity 20LaramieWorkforce Center112 South 5th StreetLaramie, WY 82073Seating Capacity 12NewcastleWorkforce Center2013 West Main St.Newcastle, WY 82701Seating Capacity 12PinedalePinedale High SchoolBasement101 East HennickPinedale, WY 82941Seating Capacity 10RawlinsEmployment ServicesOffice1703 EdinburghRawlins, WY 82301Seating Capacity 12involve more than administering medications,and the unavailability <strong>of</strong> nurses in the evening,overnight and on weekends. In order to meet theneeds <strong>of</strong> participants in home and day settings,organizations(including those with nurses on staff)have developed training programs for direct supportstaff on medication monitoring and administrationso that staff can administer medications around theclock.Until recently it was understood that themajority <strong>of</strong> independent providers administeringmedications, especially those serving children, aredoing so under the “Friends and Family” exemptionon the <strong>Nurse</strong> Practice Act, under 33-21-154, thatpermitted “the incidental health care by members<strong>of</strong> the family and friends.” This incidental healthcare includes medication administration and ina handful <strong>of</strong> cases, more complex nursing tasks,including tube feeding and respiratory care.<strong>The</strong> result is that Wyoming’s current systemalready has unlicensed “medication aides” (directsupport staff and independent providers) andpotentially some nurses working outside the rules,both within organizations and as independentproviders. <strong>The</strong> Division has not been able topromulgate rules on medication administrationthat would cover minimum training requirementsand documentation requirements, includingmedication errors, due to the restrictions in the<strong>Nurse</strong> Practice Act which do not allow nurses todelegate medication administration to CNAs orunlicensed personnel. Instead <strong>of</strong> working outside<strong>of</strong> the current system, the Division has instead beenworking with the Board <strong>of</strong> Nursing and other keystakeholders to develop a feasible solution to thisissue. <strong>The</strong> CNA II would address these concernsfor many organizations and would assure that thehealth and safety needs <strong>of</strong> waiver participants arebeing met.Frequently Asked Questions related to theDivision <strong>of</strong> DisabilitiesRivertonWorkforce Center422 E. FremontRiverton, WY 82501Seating Capacity 20Rock SpringsWorkforce Center2441 Foothill Blvd.Rock Springs, WY82901Seating Capacity 12SheridanWorkforce Center61 South GouldSheridan, WY 82801Seating Capacity 15TorringtonWorkforce Center1610‐18 East M. StreetTorrington, WY 82240Seating Capacity 10WheatlandWorkforce Center956 MapleWheatland, WY 82201Seating Capacity 8WorlandCommunity Complex/Ag Extension1200 Culbertson,Suite GWorland, WY 82401Seating Capacity 112 Wy o m i n g Nu r s e Re p o r t e r
1. Have there been negative outcomes with thecurrent system? If not, why do we need to addrequirements to it that maynot be necessary?<strong>The</strong> Division is not aware <strong>of</strong> situations where therehave been adverse outcomes for a participant.However, through our current monitoring andprovider recertification processes, the Divisionhas identified concerns with the level <strong>of</strong> trainingand understanding providers and provider staffhave concerning medication administration,side effects, etc. After reviewing these concernsthe Division agreed to work with the WyomingState Board <strong>of</strong> Nursing on an approach thatwould provide comprehensive, consistent andnationally recognized training and certification.<strong>The</strong> Division can then promulgate rules that caninclude grandfathering trained staff as CNAs(not CNA IIs), clarification on if and when aprovider can work under the Friends and Familyclause <strong>of</strong> the <strong>Nurse</strong> Practice Act and establishclear standards for medication administration.2. It will be very difficult for organizations andindependent providers to meet the number <strong>of</strong>hours and training requirements for CNA IIs.How are providers expected to provide theappropriate levels <strong>of</strong> service and to fund thisadditional training?<strong>The</strong> Division acknowledges the constraints thatproviders are working under, including staffturnover, costs <strong>of</strong> training and requirementsto meet specific supervision levels. <strong>The</strong>Division continues to work with the WSBN toprovide flexibility in this program, by allowingorganizations to become an approved CNAtraining location, and by building flexibility inthe level <strong>of</strong> nursing direction needed by CNAIIs. <strong>The</strong> Division will continue to evaluatethe impact on costs to providers and work withproviders on a solution. <strong>The</strong> goal is to establisha system that assures the health and safety <strong>of</strong>participants but that does not adversely impactproviders’ ability to provide required services toparticipants.3. Would all providers and provider staff haveto become CNA IIs?No. This requirement would only be for staffadministering medications. Many participantsdo not require medication administration, but dorequire some support and oversight when takingtheir medications. <strong>The</strong> Division plans to developa Medication Administration Assessment Toolthat would be used to determine the level <strong>of</strong>medication assistance needed by a participant.Those participants who do not require medicationadministration, but do need reminders or promptsto take their medications (what we considermedication monitoring) would not be requiredto receive care from staff trained as CNA.SummaryPlease plan to attend one <strong>of</strong> the informationsessions as WSBN solicits input and feedbackfrom nurses and healthcare stakeholdersthroughout the state for the purpose <strong>of</strong> clarifyingthe proposed rules.THE STRENGTH TO HEALand focus on what matters most.If what matters most to you is the care <strong>of</strong> your patients, we’ve got an extra bonus for you. Asign-on bonus <strong>of</strong> $20,000 to $30,000. Or you can opt for a $10,000 bonus and up to $120,000to repay your education loans. Qualified nurses can continue their education and earn amaster’s or doctoral degree. You’ll serve our Soldiers, their Families and yourself.To learn more about the U.S. Army Health Care Team, call SFC Gregory Kraft at 303-873-0491,email gregory.kraft@usarec.army.mil, or visit healthcare.goarmy.com/info/ncra1.©2008. Paid for by the United States Army. All rights reserved.Wy o m i n g Nu r s e Re p o r t e r 13
April 24, 2009Description <strong>of</strong> NCSBN’s Transition to Practice ModelNCSBN’s Transition to Practice model is intended to be collaboratively implemented with education and practice,but through regulation. Collaboration will be essential for this model to be successful. Educators are the expertsin curriculum design and evaluation and will be able to assist with the design <strong>of</strong> the transition modules. Practiceprovides a crucial link that will provide new graduates with planned practice experiences with qualified nurses tomentor them. Nursing regulators provide new graduates with information on their scope <strong>of</strong> practice, the <strong>Nurse</strong>Practice Act, and maintaining their license throughout their careers. If adopted, regulation will be able to enforcethe transition program through licensure.This is an inclusive model, which would take place in all health care settings that hire newly graduated nurses andfor all educational levels <strong>of</strong> nurses, including practical nurse, associate degree, diploma, baccalaureate and otherentry-level graduates. <strong>The</strong> new graduate must first take and pass the NCLEX ® , obtain employment and then enterthe transition program.<strong>The</strong> preceptors in this model will be trained and most will work one-on-one with newly graduated nurses, though insome settings team preceptorships may be used. This model is strongly dependent on a well-developed preceptor-nurserelationship. Novice nurses will learn the importance <strong>of</strong> being a seasoned, dedicated preceptor and theresponsibility to transition new nurses into practice. In the future, becoming preceptors and mentors for new nurseswill be an expected part <strong>of</strong> pr<strong>of</strong>essional nursing.In this model orientation is defined as teaching the policies and procedures <strong>of</strong> the workplace, as well as role expectations.<strong>The</strong>refore, orientation is separate from the concept <strong>of</strong> transition to practice. Transition to practice isdefined as a formal program designed to support new graduates during their progression into practice.<strong>The</strong> eight transition modules for this model include delegating/supervising, role socialization, evidence-basedpractice, prioritizing/organizing, clinical reasoning, safety, communication, and specialty content. <strong>The</strong>se were identifiedfrom the literature and from successful transition programs. <strong>The</strong>se modules could be presented at the institutionwhere the new nurse works, in a collaborative program with other institutions, or via the Internet. <strong>The</strong> Transitionto Practice Committee is working with NCSBN’s E-Learning Department on the feasibility <strong>of</strong> developing a Web sitewith the online learning modules and with linking new nurses to preceptors.Feedback and reflection are essential parts <strong>of</strong> this model and must be integrated throughout the entire transitionprogram. This should be built into the preceptor-nurse relationship, but also should be maintained after the sixmonthtransition period is complete.<strong>The</strong> time period for this Transition Regulatory Model will be six months, though it is expected that the new graduatewill have ongoing support for another six months. At the end <strong>of</strong> the year, the new RN is expected to havemet the Quality and Safety Education for <strong>Nurse</strong>s (QSEN) competencies. <strong>The</strong> QSEN competencies, developedby experts from across the health care disciplines, are based on the Institute <strong>of</strong> Medicine’s (IOM) recommendedcompetencies for health care pr<strong>of</strong>essionals and include patient-centered care, teamwork and collaboration, evidence-basedpractice, quality improvement, safety, and informatics. <strong>The</strong> Transition to Practice Committee membersalready have developed some definitions <strong>of</strong> competencies for practical nursing, based on the QSEN definitions forRNs. <strong>The</strong> Transition to Practice Committee also has been working with NCSBN’s Research Department to developoutcome competency measures. If NCSBN develops a continued competency model, it is anticipated that therewill be some changes in this model so that these two models will be congruent.14 Wy o m i n g Nu r s e Re p o r t e r
In order for the new graduates to maintain licensure after one year in practice, it will be incumbent upon them toprovide the Board <strong>of</strong> Nursing with a Transition to Practice Verification (TPV) form, which will be signed by the newgraduates, their preceptors and their supervisors, verifying the new nurse has met all the requirements <strong>of</strong> the jurisdiction’stransition program. In many states new drivers have similar requirements for maintaining their license aftertheir first year <strong>of</strong> driving. In 2008 the Commission <strong>of</strong> Collegiate Nursing Education (CCNE) has developed standardsfor accrediting transition programs that use the UHC/AACN model, and it is hoped that accreditation <strong>of</strong> transitionto practice programs will continue, thus assisting with standardization.©2009 <strong>The</strong> National Council <strong>of</strong> State Boards <strong>of</strong> Nursing (NCSBN ® ) is a not-for-pr<strong>of</strong>it organization whose membersinclude the boards <strong>of</strong> nursing in the 50 states, the District <strong>of</strong> Columbia and four U.S. territories — American Samoa,Guam, Northern Mariana Islands and the Virgin Islands. <strong>The</strong> College <strong>of</strong> Registered <strong>Nurse</strong>s <strong>of</strong> British Columbia is anassociate memberMission: <strong>The</strong> National Council <strong>of</strong> State Boards <strong>of</strong> Nursing (NCSBN), composed <strong>of</strong> Member Boards, provides leadershipto advance regulatory excellence for public protection.For more information, please contact Nancy Spector, PhD, RN at 312.525.3657 or nspector@ncsbn.org.Invest in the FutureFaith M. Jones, MSN, RN, NEA-BCWith the current state <strong>of</strong> the economy, varioushealthcare publications have had comments regardingthe expense involved in hiring and orientingnew graduate nurses. So why wait until theyare new grads? Through the use <strong>of</strong> a nurse externprogram, future grads can begin their orientationinto the organization as part <strong>of</strong> their educationalexperience.Three years ago, Northwest College (NWC),School <strong>of</strong> Nursing changed the curriculum for lastsemester students from traditional clinical rotationsto a precepted model which includes two 12-hour shifts a week with a staff nurse preceptor. Althoughthe change to the precepted model allowsthe student to further develop their pr<strong>of</strong>essionalpractice by prioritizing and organizing their skillsthroughout an entire shift, the time commitmentmakes it difficult for students to work during thissemester. In an effort to ease the stress <strong>of</strong> jugglingschedules, along with a potential financial impacton the students, Powell Valley Health Care set outto develop a program that would incorporate theeducational process into a real-world mentoredpractice that <strong>of</strong>fered the stability <strong>of</strong> employment.Take a moment to reflect how you felt as a newgraduate nurse during that first year. In a recentarticle which appeared in the March 2008 issue<strong>of</strong> Nursing Management, “From Novice to Expert:Transitioning Graduate <strong>Nurse</strong>s”, Grochow summarizesa study that was conducted at University<strong>of</strong> California, Irvine using Benner’s theory. Herfindings revealed that the graduate nurse reachedthe level <strong>of</strong> “competence” after gaining two rothree years <strong>of</strong> experience.Navigating the complexities <strong>of</strong> healthcare andputting new skills into practice is far less scary in afamiliar environment where pr<strong>of</strong>essional networkshave already been established. Having an understanding<strong>of</strong> the culture, the tools to communicateeffectively, and the ability to establish relationshipsallows the new grad the opportunity to learnin a safe environment.PVHC, in partnership with NWC, has developedan educational program to assist in the enculturationprocess. Each fall, the Vice President<strong>of</strong> Patient Care Services and the Float Pool Directorvisit the sophomore class at NWC to presentan employment opportunity. Students interestedin pursuing employment with PVHC can begintheir pr<strong>of</strong>essional journey even before they havefinished the nursing program.Following the application and interview process,hiring selections are made. <strong>The</strong>se job <strong>of</strong>fersinclude full time pay and benefits beginning withthe final semester as a nurse extern, followed by a12- week graduate nurse orientation period, thenas a registered nurse. As each level is achieved,additional pay is earned. <strong>The</strong> acceptance <strong>of</strong> thisjob <strong>of</strong>fer comes with a few commitments includingthe intention to work at PVHC for a minimum <strong>of</strong>two years, agreeing to obtain a bachelor <strong>of</strong> sciencedegree in nursing (BSN) within eight years <strong>of</strong> hireand fulfilling the nurse extern requirements. Oncethe job <strong>of</strong>fer is accepted, the student is requiredto enroll in the nurse extern course <strong>of</strong>fered by theNWC Workforce Alliance. This semester longclass provides the students with the opportunity towork as a nurse extern in a precepted student role.It is during these shifts, in combination with theclinical shifts, that the students begin to learn theprocesses unique to PVHC and build relationshipswith staff who will soon be their peers. In additionto the work experience, the students meet weeklyto discuss issues that arise, seek advice in networking,and learn about how they fit into the culture<strong>of</strong> PVHC. <strong>The</strong> materials for the nurse externcourse that have been selected by PVHC and approvedby the NWC Workforce Alliance Trainingand Development Programs Manager are: “Now,Discover Your Strengths” by Marcus Buckinghamand Donald Clifton and “If Disney Ran Your Hospital,9 ½ Things You Would Do Differently” byFree Lee.In this vulnerable learning time, the strengthsdiscovery process builds confidence as it highlightsthat each student has innate strengths to bring tothe bedside. Following the discussions, studentswrite a self reflection paper outlining how theycan leverage their strengths as they begin theirnew career. As the course progresses, the studentsare tasked to examine the cultural philosophy usedat PVHC which is based on Fred Lee’s work. Eachweek, through journal entries and discussions, thestudents explore the expectations and behaviorsthat are exhibited in the culture <strong>of</strong> which they arebecoming a part.As the semester comes to a close and the studentsare preparing to take their next step up theladder to becoming graduate nurses, it is our hopethat the experiences and learning that has takenplace throughout the nurse extern period laid thefoundation for their future success in our organization.This program sets the stage to foster aculture <strong>of</strong> collaboration by identifying and sharingstrengths, not necessarily to improve individualweaknesses, but to enhance our collective practice.ReferencesBuckingham, M. & Clifton, D. (2001). Now, discoveryour strengths. New York: Simon & Schuster,Inc.Grochow, D. (2008). From novice to expert: Transitioninggraduate nurses, Nursing Management,39(3), 10-12.Lee, F. (2004). If Disney ran your hospital: 9 ½things you would do differently. Bozeman, MT: SecondRiver Healthcare Press.Wy o m i n g Nu r s e Re p o r t e r 15
April 2009NCSBN’s Transition to Practice Model: Frequently Asked Questions1. Q. Why should Boards <strong>of</strong> Nursing consider regulating transition to practice?A. Please see our Fact Sheet, which outlines the compelling argument that transition to practice programsshould be implemented through regulation: https://www.ncsbn.org/363.htm. As background to this work,NCSBN studies in the early 2000s found that new graduates and employers cited transition to practice as aproblem. For example, one NCSBN study reported that new nurses were expected to practice independentlyin a mean <strong>of</strong> eight days after the first day <strong>of</strong> hire. Other NCSBN studies found that fewer than 50% <strong>of</strong> theemployers reported that new graduates were prepared to practice safely and competently. In further studiesNCSBN found that well-planned, post-hire transition programs had better outcomes than pre-graduation clinicalimmersion programs and were related to fewer practice errors and fewer risks for practice breakdown. In anextensive literature review NCSBN also found that post-hire transition programs were linked to fostering betterpractice outcomes and safer practice.2. Q. How was the model designed?A. NCSBN’s Transition to Practice Committee spent a year analyzing the available evidence from transition topractice programs, published and unpublished. Data were retrieved from international, national, and individualstudies and projects and were outlined in our Evidence Grid, available here: https://www.ncsbn.org/363.htm.<strong>The</strong> model was derived from the evidence and in concert with the Boards’ mission <strong>of</strong> public protection.3. Q. Are you seeing this as a failure <strong>of</strong> education and/or practice in nursing?A. Absolutely not! Health care delivery in the U.S. is becoming increasingly complex, necessitating the use <strong>of</strong>sophisticated technologies and the need for systems thinking in order for nurses to practice safely. Further,more than ever before nurses are caring for sicker, older, and more diverse patients with myriad chronic conditions.In order to keep up with this these changes, NCSBN is proposing that nursing needs to regulate thatcritical period between education and competent practice where the novice nurse needs practice experienceand support from competent nurses in order to develop pr<strong>of</strong>essionally.4. Q. Are the modules “re-teaching” didactic content that you are assuming the newly licensed nurses didnot effectively learn?A. No! <strong>The</strong> modules will not be designed as didactic courses. <strong>The</strong> modules will build on the nurse’s educationalexperiences, providing opportunities for deliberate practice. For example, there will be interactive practiceexercises designed for newly licensed nurses in areas that are critical for public protection, such as experienceswith: priority setting; delegating and supervising; making decisions in a fast paced environment; communicatingwith other healthcare pr<strong>of</strong>essionals; and implementing risk management principles.5. Q. What about cost?A. All published studies have shown positive return on investment for the workplace when well-planned transitionprograms are implemented. However, we recognize that the start-up <strong>of</strong> these programs might requiresome out-<strong>of</strong>-the-box thinking. We encourage partnerships between practice agencies, as well as betweenpractice and education, in developing a transition program that would meet the jurisdiction’s criteria. NCSBN16 Wy o m i n g Nu r s e Re p o r t e r
www.ncsbn.org 2is investigating the possibility <strong>of</strong> small start-up grants as well as federal funding for the employers. One <strong>of</strong> thepurposes <strong>of</strong> NCSBN’s pilot studies will be to investigate the cost/benefit ratio for employers as well as the costto Boards <strong>of</strong> Nursing.6. Q. How can this be implemented in rural areas?A. NCSBN is planning to develop online modules and online connections with preceptors that could be usedif the facility does not have the resources to develop a transition to practice program. <strong>The</strong> online connectionfor preceptors would also be valuable in those settings where there might be a paucity <strong>of</strong> preceptors, such ascorrectional institutions or schools.7. Q. What if an agency already has an excellent residency program?A. As long as it meets the criteria <strong>of</strong> our model, it would be acceptable. Many <strong>of</strong> the current models out theremeet our criteria. An underpinning <strong>of</strong> our model is that it was designed to be flexible (we won’t mandate theprogram to be used) and robust (inclusive <strong>of</strong> all settings and all education levels <strong>of</strong> nurses).8. Q. What about preceptor training?A. Our model has preceptor training built in. We will have set criteria for preceptor training, and we will developmodules for those agencies that do not have resources to train their preceptors. However, we absolutelythink it’s essential for preceptors to be adequately trained.9. Q. During the time <strong>of</strong> the 6-month preceptorship is the newly licensed nurse considered part<strong>of</strong> the work schedule?A. At the beginning <strong>of</strong> the relationship the preceptor will work very closely with the newly licensed nurse,providing much support and feedback. However, as the relationship develops (and this will be on an individualbasis), that newly licensed nurse will be supported to work more independently since the goal <strong>of</strong> this relationshipis to foster safe and competent practice by allowing for experiential learning.10. Q. Must it be a one-to-one preceptor relationship?A. While some research has found the one-to-one relationship between preceptor and newly licensed nurse tobe more effective than multiple preceptors, this might not always be feasible. Furthermore, new studies havefound that team preceptorships can be effective. <strong>The</strong>refore, a one-to-one preceptorship won’t be required; theworkplace should decide what works better for their situation.11. Q. Will NCSBN mandate transition to practice programs across all Boards <strong>of</strong> Nursing?A. No! Because <strong>of</strong> state’s rights, NCSBN does not have the authority to mandate regulation in the Boards <strong>of</strong>Nursing. If our members support this initiative, we will make the recommendation and will assist those Boardsthat want to implement transition to practice to do so.©2009 <strong>The</strong> National Council <strong>of</strong> State Boards <strong>of</strong> Nursing, Inc. (NCSBN) is a not-for-pr<strong>of</strong>it organization whosemembership comprises the boards <strong>of</strong> nursing in the 50 states, the District <strong>of</strong> Columbia and four U.S. territories.Mission: <strong>The</strong> National Council <strong>of</strong> State Boards <strong>of</strong> Nursing (NCSBN), composed <strong>of</strong> Member Boards, provides leadershipto advance regulatory excellence for public protection.For more information, please contact Nancy Spector, PhD, RN at 312.525.3657 or nspector@ncsbn.org.Wy o m i n g Nu r s e Re p o r t e r 17
Parish <strong>Nurse</strong> Health MinistryFlossie Vance, RNParish nursing is a unique, specialized practice<strong>of</strong> nursing that is a health promotion, diseaseprevention ministry based on the total healthhealing <strong>of</strong> a person – body, mind and spirit.<strong>The</strong> spiritual aspect is central to parish nursing.Although this is a new specialty in nursing onlyapproved by the American <strong>Nurse</strong>s Association in1997 it is based on old traditions <strong>of</strong> the Christianchurch to care for the sick and those in need. Itsroots are in many religious traditions, especiallyJesus’ healing ministry reflected in one fifth<strong>of</strong> the gospels. Parish nursing also reflects thecore philosophy <strong>of</strong> nursing which is to care forothers through teaching, counseling, advocating,referring and including family and others inthe provision <strong>of</strong> care. Parish nursing requiresadditional training after which the nurse iscommissioned and receives a certificate. This canbe done through the Wyoming Health Councilin cooperation with Carroll College in Helena,Montana. <strong>The</strong> parish nurse works in collaborationwith the pastor, priests, church staff and localresources to improve the health and wellness <strong>of</strong>the parish as well as the local community. <strong>The</strong>Parish nurse may also work under the guidance<strong>of</strong> a health ministry team. <strong>The</strong> team can consist<strong>of</strong> the pastor, pastoral, medical, nursing, socialwork, legal, business and lay members dedicatedto helping guide, direct, expand and evaluate theprogram.As a health educator and counselor, the parishnurse helps parishioners explore ways to cope withphysical problems, safety concerns, relationshipconcerns, and stressful life transitions (birth,retirement and loss). <strong>The</strong> nurse assists parishionersevaluate signs and symptoms <strong>of</strong> disease that mayneed to be acted on promptly and helps those inneed to understand their diagnosis, lab resultsand medications. Caregivers are also assisted witheducation and support. <strong>The</strong> parish nurse may writehealth articles for the Sunday bulletins as well asarrange or provide classes on health topics. <strong>The</strong>yalso conduct health fairs and health screenings.As health advocates, parish nurses helpparishioners to understand and navigate thehealth care system, help those in need access ahealth care provider or health care when medicalhelp is needed. <strong>The</strong> parish nurse can be a voicefor those who cannot act on their own behalfand a health resource for families in need. <strong>The</strong>ycan accompany parishioners to their healthcare provider visits and explain their concern orsituation to the health care provider if requested.<strong>The</strong>y can direct parishioners to resources forinsurance, medications or health care.As a referral person, the parish nurse canguide, refer and direct the parishioners to theresources in the community, when they don notknow where to go or what is there for them.<strong>The</strong>y can refer parishioners to health careproviders and community agencies and collaboratewith members <strong>of</strong> the health care system.<strong>The</strong> parish nurse meets with parishioners upontheir request or when referred by friends, family orparish staff in a variety <strong>of</strong> settings. <strong>The</strong>y visit in thehome, hospital, nursing home, rehab unit, parishbuilding and the <strong>of</strong>fice as well as communicate byphone, e-mail or regular mail depending on theneed <strong>of</strong> the parishioner. Many parish nurses doweekly rounds visiting parishioners while they arein the hospital.Today there are thousands <strong>of</strong> nurses in manydenominations working as parish nurses acrossthe country. <strong>The</strong>y are reclaiming the old tradition<strong>of</strong> health ministry in the church, to meet unmethealth needs and support the journey towardswholeness. <strong>The</strong> ultimate goal <strong>of</strong> parish nursing isto improve the whole person health <strong>of</strong> the parishand community and strengthen the awareness <strong>of</strong>the connection between faith and health. <strong>The</strong>emphasis <strong>of</strong> spiritual health care combined withother parish nurse roles <strong>of</strong>fers a unique service tothe parishioners not available anywhere else.Flossie Vance is a Catholic Community Parish<strong>Nurse</strong> in Cheyenne WyomingHEALTH CARE WITHOUT HARM AND NURSES ALL OVER THEWORLD PARTNER FOR AN ENVIRONMENTAL HEALTH CAREIn celebration <strong>of</strong> the International <strong>Nurse</strong>s Day,Health Care Without Harm and nurses all overthe world partner to create a cleaner, healthier andmore environment-friendly health care system.In the Philippines, HCWH-Southeast Asiaand the Philippine <strong>Nurse</strong>s Association (PNA)signed a memorandum <strong>of</strong> understanding detailingthe work to phase-out mercury in the health caresetting.According to Merci Ferrer, Executive Director<strong>of</strong> HCWH-SEA, “for so many years in the history<strong>of</strong> HCWH, the nurses have always been inthe forefront <strong>of</strong> environmental health campaigns.<strong>Nurse</strong>s are first to demand for occupational safetypractices in the hospitals and also the first to askthat mercury devices be phased-out.”“We are glad that in the Philippines, it is notjust individual nurses who are taking the lead forchange but the nurses as a collective, as an organization,”she added.As part <strong>of</strong> the MOU, PNA will join the MercuryFree Health Care Global Initiative led by theWorld Health Organization (WHO) and HCWH.This Initiative aims to substitute mercury-basedmedical devices with safer, accurate and affordableby 2017.“<strong>The</strong> mercury phase-out is number one issue,”said PNA President Tita Barcelo. “We haveAdministrative Order 21 which mandates thephasing-out <strong>of</strong> all mercury-containing devices inall hospitals by 2010 here in the Philippines. <strong>The</strong>PNA definitely support a global phase-out. This isfor the welfare <strong>of</strong> the patients who visit the hospitalsand the nurses and other health workers whospend 40 hours a week on duty.”PNA’s support to global mercury phase-outdoes not stop with the MOU. <strong>The</strong>y likewise aimfor a virtual elimination <strong>of</strong> mercury-based thermometersand sphygmomanometers over the nextdecade, substituting these items with accurate,economically viable alternatives and enjoiningall PNA members, chapters and affiliates in thecountry to help promote the advocacy to eliminatemercury in health care.PNA is also supporting the call for the Department<strong>of</strong> Environment and Natural Resources(DENR) to provide an intermediate storage areafor phased-out mercury devices from hospitals.“As for all items that are to be phased-out,there must be a corresponding storage area. Thus,we are urging the DENR to be dutiful enough andprovide a temporary storage,” Barcelo added.HCWH-SEA, on the other hand will organizemercury-free health care information and educationprograms to be disseminated to PNA regional<strong>of</strong>fices; national and local activities for nurses onthe promotion <strong>of</strong> mercury-free health care devices;and promote through its website and the nationalmedia the various activities done by the PNA andthe partnership.18 Wy o m i n g Nu r s e Re p o r t e rContinued on next page
Don’t riskAre you up to the challenge <strong>of</strong> coordinating and leading a newPractical Nursing Program? Eastern Wyoming College seeks aPractical Nursing Program Coordinator/ Instructor for its DouglasCampus.<strong>The</strong> Nursing Program Coordinator/ Instructor will:- oversee and establish a classroom-based curriculum consistentwith Board <strong>of</strong> Nursing guidelines- structure and implement a hands-on internship based program- recommend appropriate equipment and staffIf you feel you may have a substanceabuse problem, reach out to the WyomingPr<strong>of</strong>essional Assistance Program(WPAP). This program is <strong>of</strong>ficiallyrecognized by the Wyoming State Board<strong>of</strong> Nursing as an effective intervention,referral and monitoring program.Don’t face your addiction alone. Learnmore by calling, in confidence,307.472.1222 or wpapro@wyonet.net.This person will oversee a program that prepares students with theknowledge, skills, values, and attitudes essential to a successfulnursing career. Most <strong>of</strong> all, this person will exemplify the highstandards <strong>of</strong> compassion and care that are at the core <strong>of</strong>pr<strong>of</strong>essional nursing.REQUIREMENTS: Master’s degree in Nursing. Have, or obtain beforeemployment, a current Wyoming RN license. Supervisory experience,computer pr<strong>of</strong>iciency, excellent interpersonal and communicationskills a must. Submit letter <strong>of</strong> application, resume, three letters <strong>of</strong>reference, OFFICIAL graduate and undergraduate transcripts to thePersonnel Office 3200 West C St. Torrington, WY 82240Make a difference.For a more information contact:Tom McDowell, HR Director, 866.327.8996 orTom.McDowell@ewc.wy.edu.Visit www.ewc.wy.eduEASTERN WYOMING COLLEGE IS AN AFFIRMATIVEACTION/EQUAL OPPORTUNITY EMPLOYERFor advertisinginformation call or e-mailVictor Horne501.221.9986or 800.561.4686vhorne@pcipublishing.comYou Dreamed<strong>of</strong> Being a<strong>Nurse</strong>.Now Become the<strong>Nurse</strong> You Dreamed<strong>of</strong> Being.If someonecame to youASKINGABOUTADOPTION…WOULD YOUKNOW WHAT TO SAY?“This is what partnership entails. Each has itsown duty. You excel in the work assigned to you.You share resources. And when it’s harvest time,all the members reap the benefits,” said Ferrer.“In this case, it is not just the Philippine nursesand hospitals who will benefit but nurses, healthcare workers and practically every human all overthe world.”PNA has a membership <strong>of</strong> over 105,000.Health Care Without Harm (HCWH) is aglobal coalition <strong>of</strong> more than 400 organizations inmore than 50 countries working to protect healthby reducing pollution in health care sector. Formore information, visit www.noharm.org. (30)For other HCWH-nurses partnership projects,visit http://noharm.org/globalsoutheng/pressroom/latestNews.cfmOne <strong>of</strong> “America’s Best Colleges”U.S. News & World ReportEarn Your RNto BSN Online!RNs: Get 30Credits Free!Call 800-571-4934JacksonvilleU.com/PC© 2009 All Rights Reserved.Made Available by University Alliance ® –<strong>The</strong> Nation’s Leading Universities Online.SC: 191734zj1 | MCID: 2742Infant Adoption Training Initiative isa FREE half- or full-day training thatwill enhance your knowledge andexpertise <strong>of</strong> the adoption option. Visitwww.infantadoptiontraining.orgor call 1.888.201.5061 for moreinformation. Free CEUs arealso available.This project is funded through the Children’s Bureau<strong>of</strong> the Department <strong>of</strong> Health and Human Services.Wy o m i n g Nu r s e Re p o r t e r 19
Advanced Practice Registered <strong>Nurse</strong>in a Specialty clinic?Maria Kidner, DNP, FNP-BCI work in a cardiology practice whereI have privileges for in-patient care,noninvasive testing supervision andoutpatient clinical care; that is within myscope <strong>of</strong> practice. How can that be, sincemy training as a family nurse practitionerand a doctor <strong>of</strong> nursing practice was forbasic family care and care <strong>of</strong> chronicstable patients? However, a 37-year oldpatient with premature coronary arterydisease and post-operative pericarditis anda 78-year old patient with non-ischemiccardiomyopathy, apical ballooning andheart failure are two <strong>of</strong> the many wonderfulpatients for whom I provide care.Advanced Practice Registered <strong>Nurse</strong>s(APRNs) work in specialty clinicswithin their scope <strong>of</strong> practice. This isaccomplished by virtue <strong>of</strong> advanced andcontinuing education, communicationskills, teamwork, partnerships andinvesting time in building trust amongthe referring providers to the specialtyclinic. It is important to understandthat the unique paradigm <strong>of</strong> the APRNcompliments the care provided in specialtyclinics where sicker patients with greaterfears and a need for understanding comefor intense healthcare treatments. APRNslearn patient care through a bio-psychosocialparadigm (Bock, 2006; Kleiman,2004). Consider the 82-year old malewho presented to the ER with shortness<strong>of</strong> breath. He actually had severe coronaryartery disease which was treated by severalintracoronary stents, but later was found tohave a large abdominal aortic aneurysm.However, he developed renal failurebefore he could have a repair completed.<strong>The</strong> APRN must think <strong>of</strong> him not as all <strong>of</strong>those parts, but as a wonderfully delightfulfather and devoted husband who (inspite<strong>of</strong> everything) is feeling quite well andhappy. <strong>Nurse</strong>s think <strong>of</strong> the patient as aperson, whereas the medical paradigm wasbuilt upon theories developed by Platoand Hippocrates who studied specificparts <strong>of</strong> each problem (Bock, 2006). <strong>The</strong>APRN still comes up with a similar plan<strong>of</strong> care and still follows the guidelines...wejust do it differently. Ultimately, APRNsin specialty clinics take time to listen inorder to develop strong relationships andpatient trust. That trust must be extendedBe consistent, persistent, trustworthy, maintain integrity and always use anursing perspective by treating your patient as a person first and you will findworking in a specialty clinic immensely satisfying!to other providers in the specialty clinicand, ultimately, to the referring providers(truly the hardest to achieve) (Carroll,Rankin, & Cooper, 2007).At my place <strong>of</strong> employment,Cheyenne Cardiology Associates, thereis tremendous support for me as a Doctor<strong>of</strong> Nursing Practice (DNP) and for thePhysician’s Assistant (PA). We areteam members building a practice andfoundation <strong>of</strong> cardiovascular excellencefor our patients, their families and referringproviders. Through continuing educationwe have developed a sound understanding<strong>of</strong> cardiovascular care. Physicians in thispractice trust us to know when we need toseek their opinion and guidance in morecomplex care. <strong>The</strong> decision to seek peerconsultation and to refer appropriately isimportant. Understanding the limits <strong>of</strong>personal knowledge and skills are criticalin maintaining trust, relationships, andultimately, in preserving patient safety.In my opinion, the hardest part <strong>of</strong>being a team member in a specialty clinicas an APRN is developing a trustingrelationship with referring physicians.Could a physician be comfortable insending their complex and ill patients tothe APRN in a specialty clinic? Couldthe APRN know anything more thanthe referring physician! Well, yes, theAPRN can grow in skills and knowledgein a specialty clinic that is supported bya team <strong>of</strong> physician peers who are eagerto provide support and guidance (Carroll,Rankin & Cooper, 2007; Hooker, 2006).Again, yes we could, because we look atthe patient through a bio-psycho-socialmodel. APRNs alleviate fears, obtaina comprehensive history and physical,order appropriate diagnostic tests,provide individualized patient education,and develop a plan <strong>of</strong> care. All <strong>of</strong> thisconsultation needs to be articulatedconcisely, pr<strong>of</strong>essionally and promptlyto the referring provider. All <strong>of</strong> theseactivities are well within the scope <strong>of</strong>practice <strong>of</strong> APRNs. Remaining withinyour scope requires you to always knowyour limits. Be consistent, persistent,trustworthy, maintain integrity and alwaysuse a nursing perspective by treating yourpatient as a person first and you will findworking in a specialty clinic immenselysatisfying!Maria Kidner is the nurse practitionerfor Cheyenne Cardiology Associates,the President <strong>of</strong> District #1 Wyoming<strong>Nurse</strong>s Association, and is Wyomingrepresentative to the American Academy<strong>of</strong> <strong>Nurse</strong> Practitioners.ReferencesBlock, D. (2006). Healthcare outcomesmanagement: Strategies for planning andevaluation. Boston: Jones and BartlettPublishers.Carroll, D., Rankin, S. & Cooper, B.(2007). <strong>The</strong> effect <strong>of</strong> a collaborative peeradvisor/advanced practice nurse intervention:Cardiac rehabilitation participation andrehospitalization in older adults after a cardiacevent. Journal <strong>of</strong> Cardiovascular Nursing,22, 326-343.Hooker, R. (2006). Physician assistantsand nurse practitioners: <strong>The</strong> United Statesexperience. <strong>The</strong> Medical Journal <strong>of</strong> Australia,185 (1), 4-7.Kleiman, S. (2004). What is the nature<strong>of</strong> nurse practitioner’s lived experienceinteracting with patients? Journal <strong>of</strong> theAmerican Academy <strong>of</strong> <strong>Nurse</strong> Practitioners,16(6), 263-269.20 Wy o m i n g Nu r s e Re p o r t e r
Powell Valley HealthcareEmploymentOpportunitiesWe Treat YouLike FamilyRNs and LPNsLander <strong>of</strong>fers a variety and abundance<strong>of</strong> outdoor recreational opportunities,cultural activities and affordable housingin a beautiful setting. With over 250 days<strong>of</strong> brilliant blue skies, your adventuresare limitless.We are committed to five core values: High Quality Patient Care Excellent Workplace Supporting Physicians Providing community value Ensuring Fiscal responsibility$6,000 Sign-on/Retention BonusOpportunities- OR Circulating <strong>Nurse</strong>Great BenefitPackage!• Flexible Scheduling• Health Insurance, including dental & vision• Generous compensationBased on years <strong>of</strong> experience• Career Ladder that includes additionalcompensation for education, certifications,cross-training, quality, and mentorshipThis Big Horn Basin growing community’s climate iscomfortable with little moisture. Located near YellowstoneNational Park and surrounded by mountains,there is ample opportunity for outdoor recreation yeararound.Powell Valley Healthcare is a facility dedicated to providingan outstanding work environment for staff, andexceptional experiences for customers.• Paid time <strong>of</strong>f starting at 23 days• Life & Disability insurance• Differential for evenings & nights• Extended Illness Plan• Tuition & Student Loan Reimbursement• Retirement plan with employermatching contributionsTo interview us as your future employer, call:1-800-428-1398, Ext. 134Visit our web site atwww.pvhc.orgEqual Opportunity EmployerContact:Human ResourcesJanet.Morgan@lpnt.netLander Regional Hospital1320 Bishop Randall DriveLander, WY 82520307-335-6580Fax 307-335-6237To apply visit our Web sitewww.landerhospital.comWy o m i n g Nu r s e Re p o r t e r 21
Why all theConfusion aboutMidwives andHome Birth?Patti Gardner, CNM, MSN, PMHNP-BCIsn’t home birthillegal in Wyominganyway?IntroductionA friend <strong>of</strong> mine recently had a plannedhome birth. When she called the newspaper toask how she would go about getting the birthannouncement published, the person from thenewspaper <strong>of</strong>fice paused, cleared his throat andthen finally asked, “Well isn’t it illegal to haveyour baby at home anyway?” With so muchpublicity about home births and illegal midwiveslately, it seems as if much has been misunderstood.This article will highlight the history <strong>of</strong> midwiferyin America, the differences among the types <strong>of</strong>midwives and what research tells us about thesafety <strong>of</strong> homebirth. <strong>The</strong>n we will hear from afamily who just had their fourth baby at home,a Certified <strong>Nurse</strong> Midwife doing home births inWyoming and an Obstetrician and Gynecologist’s(OB/GYN) perspective on how we can keep homebirth safe in Wyoming.History <strong>of</strong> midwifery in AmericaEarly on in America, midwives were respectedas vital members <strong>of</strong> the community (Rooks, 1997).In fact, during the first 250 years <strong>of</strong> our history asa nation, midwives provided almost all the careto pregnant women (Rooks, 1997). Prior to 1760,childbirth was virtually never seen nor attendedby men (Leavitt, 1983). Midwives had littleeducation (Cassidy, 2006) and practiced underfew rules or regulations (Lit<strong>of</strong>f, 1982). This allchanged with the introduction <strong>of</strong> medicine.In the early seventeenth century, PeterChamberlain, a British surgeon, inventedforceps (Rooks, 1997, p. 15). At the end <strong>of</strong> the18 th century, medical schools banned womenstudents at the same time when the progress inscience would have promoted their competenceas midwives and physicians (Lit<strong>of</strong>f, 1982, p. 26).Forceps and opium for pain allowed physiciansinto the birth process (Rooks, 1997). By the turn<strong>of</strong> the twentieth century, physicians deliveredabout half <strong>of</strong> the nation’s babies (Leavitt, 1983).<strong>The</strong> pursuit to abolish midwives resulted in themidwife debates which occurred between 1910and 1935 (Rooks, 1997). <strong>The</strong> debates focusedon convincing the public that midwives wereincompetent, that pregnancy was a “dangerouscondition” which required care from physicians,and that allowing midwives to continue to beinvolved with childbirth hindered medicalprogress in obstetrics (Rooks, 1997, p. 24). In1912, Dr. Williams, an obstetrician, called for the“gradual abolition <strong>of</strong> midwives in large cities andtheir replacement by obstetric charities” (Rooks,1997, p. 25).<strong>The</strong> Children’s Bureau was formed in 1912 tocollect data about women’s and children’s healthin the United States (Rooks, 1997). <strong>The</strong> statisticsrevealed that America experienced maternal andinfant mortality rates that were higher than most<strong>of</strong> Europe (Rooks, 1997). <strong>The</strong> Maternity CenterAssociation (MCA), a non-pr<strong>of</strong>it voluntaryhealth agency was formed in Manhattan in 1918to improve maternal and child health in the city(Rooks, 1997). By 1920, MCA had public healthnurses working under physician supervision toprovide prenatal care and education to pregnantwomen and their families, mostly in their homes,in 30 neighborhood centers (Rooks, 1997, p. 38).MCA formed the Association for Promotion andStandardization <strong>of</strong> Midwifery in 1930 (Rooks,1997). <strong>The</strong> organization opened the first school<strong>of</strong> <strong>Nurse</strong>-Midwifery in the nation, the Lobenstine<strong>Nurse</strong>-Midwifery School, in 1931(Rooks, 1997).<strong>The</strong> school ran for 26 years, and attended 7,099births, mostly in the woman’s home (Rooks, 1997).<strong>The</strong> maternal mortality rates for these births wereten times lower than the nation’s average duringthis period (Rooks, 1997).In 1918, an American named Mary Breckinridgevolunteered to go to France to care for children inthe war torn country (Breckinridge, 1981). Sheobserved excellent training in midwifery in France,with a lack <strong>of</strong> nursing education; in America,the opposite existed (Breckinridge, 1981). Shemet British nurse-midwives during her work inFrance and her visits to London, who were bothnurses and midwives (Breckinridge, 1981). Shehad the epiphany that <strong>Nurse</strong>-Midwifery was theanswer to the health care needs in rural America(Breckinridge, 1981, p. 111).Breckinridge began to form a plan for whatwould become Frontier Nursing Services (FNS).She had spent much time in the mountains <strong>of</strong>Kentucky, and she knew the desolation <strong>of</strong> thosewho lived there (Breckinridge, 1981). Afterbecoming a nurse-midwife in England, andwith much preparation as well as fundraising,Breckinridge returned to Kentucky and startedFNS in 1925 (Breckinridge, 1981). <strong>The</strong> nursesworking for FNS rode on horseback to attendto pregnant and laboring women (Breckinridge,1981).With great foresight, Breckinridge hired theMetropolitan Life Insurance Company to keepstatistics for the service (Rooks, 1997). <strong>The</strong>statistics demonstrate the incredible quality <strong>of</strong>care provided (Rooks, 1997). As a testamentto this, Dr. Louis Dublin who worked for theinsurance company wrote that if the rest <strong>of</strong> thecountry implemented similar programs, the lives<strong>of</strong> thousands <strong>of</strong> women and children would besaved (Rooks, 1997).Breckinridge started the second nurse-midwiferyschool in the nation, the Frontier School <strong>of</strong>Midwifery and Family Nursing (FSMFN), in 1939(Breckinridge, 1981). FNS and FSMFN are stillin operation today, <strong>of</strong>fering distance education tonurses around the world.With nurse-midwives finding a niche inmultiple settings, the scope <strong>of</strong> nurse-midwifery hasexpanded. A 1994 survey <strong>of</strong> nurse-midwives foundthat some were performing many skills outside <strong>of</strong>their original training, as well as treating womenfor health problems unrelated to reproduction(Stone, 2000). To support the progress, theAmerican College <strong>of</strong> <strong>Nurse</strong> Midwives, foundedin 1955, issued a statement that Certified <strong>Nurse</strong>-Midwives are primary health care providers forwomen and newborns, and changed the CoreCompetencies’ for Basic Midwifery practice in1997 to include areas outside <strong>of</strong> reproduction(Stone, 2000). Certified <strong>Nurse</strong>-Midwives arealso required to complete continuing educationprograms to maintain their knowledge and skills(ACNM Web site, 2008).So…did I understand that there’s more than onekind <strong>of</strong> midwife?In part, the confusion over midwives is in thetitle. “Midwife,” meaning “with women” (ACNMwebsite, 2009) is in the title <strong>of</strong> four separate andvery distinct groups providing care for birthingwomen. To try and simplify, there are midwiveswho are nurses and midwives who are not nurses.Those who are NOT nurses are generally referredto as direct entry midwives. <strong>The</strong>re is muchmisinformation on the world wide web about thedifferences in midwives, the outcomes <strong>of</strong> midwivesand who is more qualified to do what and in whatsetting. I have tried to simplify for you here thetypes <strong>of</strong> midwives, primarily with informationavailable from the American College <strong>of</strong> <strong>Nurse</strong>Midwives (ACNM website, 2009).Certified nurse-midwives are master’s preparedregistered nurses who have graduated from anurse-midwifery education program accreditedby the American College <strong>of</strong> <strong>Nurse</strong>-Midwives andhave passed a national certification examinationto receive the pr<strong>of</strong>essional designation <strong>of</strong> certifiednurse-midwife. <strong>Nurse</strong>-midwives have beenpracticing in the U.S. since the 1920s and workin clinics, hospitals, birthing centers and attendhome births (ACNM website, 2009).Direct Entry Midwives: <strong>The</strong>re are three types<strong>of</strong> “direct entry” midwives; certified midwives,certified pr<strong>of</strong>essional midwives and lay midwives.Certified midwives, popular in Europe, areindividuals who have or receive a backgroundin a health related field other than nursing andgraduate from a midwifery education programaccredited by the ACNM. Graduates <strong>of</strong> anACNM accredited midwifery education program22 Wy o m i n g Nu r s e Re p o r t e r
take the same national certification examinationas CNMs but receive the pr<strong>of</strong>essional designation<strong>of</strong> certified midwife. Certified midwives workin clinics, hospitals, birthing centers and attendhome births (ACNM Web site, 2009).A Certified Pr<strong>of</strong>essional Midwife is a direct entrymidwife and independent midwifery practitionerwho has met the standards for certification setby the North American Registry <strong>of</strong> Midwives(NARM) and is qualified to provide the midwiferymodel <strong>of</strong> care. No college degree is required forthis designation. Certified pr<strong>of</strong>essional midwiveswork primarily in out <strong>of</strong> hospital settings.A Lay Midwife, sometimes called a “directentry” midwife, is an independent practitionerwho has learned midwifery through study orapprenticeship. A direct entry/lay midwife maywork to meet standards for certification set upby NARM and become a certified pr<strong>of</strong>essionalmidwife. No college degree is required for thisdesignation. Direct entry/lay midwives attendhome births.So what does all this mean? I’m still confused….Unfortunately, there seems to be confusionabout what’s legal and what’s not; from state tostate, and certainly within the state <strong>of</strong> Wyoming.It’s all very confusing and most people, even thosein health care and many midwives themselves,don’t know the differences. To simplify:• Certified <strong>Nurse</strong> Midwives are legally authorizedto practice in every state in the US and in theDistrict <strong>of</strong> Columbia.• Certified Midwives are currently legallyauthorized to practice in New York, NewJersey and Rhode Island.• Twenty six states now recognize direct-entrymidwives in statute, and 24 states licensedirect entry midwives. States with activedirect-entry midwifery licensure, certification,or registration at the time <strong>of</strong> this printingwere California, New York, South Carolina,Utah, Alaska, Colorado, Florida, NewHampshire, Oregon, Vermont, Wisconsin,Arizona, Louisiana, Montana, New Jersey,Tennessee, Virginia, Arkansas, Delaware,Minnesota, New Mexico, Rhode Island, Texas,Washington (ACNM Web site, 2009).<strong>The</strong> take home message, however, is simple.<strong>The</strong>re is one type <strong>of</strong> midwife that can legallypractice in the state <strong>of</strong> Wyoming: a Certified <strong>Nurse</strong>Midwife (CNM). All other types <strong>of</strong> midwifery areillegal in the state <strong>of</strong> Wyoming. Having a baby athome, however, is NOT illegal. But is it safe, youask? Let’s look at the research.Safety <strong>of</strong> Homebirth<strong>The</strong> debate over the safety <strong>of</strong> homebirth hasbeen argued in the literature for years. In morerecent years however, there have been severalhigh quality and controlled studies that haveestablished that home birth is safe, with thecorrect parameters in place. Home births generallyresult in fewer cesarean births, less narcotic andepidural analgesia use during labor and delivery,less electronic fetal monitoring, and reduced risk<strong>of</strong> amniotomy and episiotomy (Durrand, 1992;Janssen, Ryan, Etches, Klein and Reime, 2006;Olsen, 1997). Data from a large North Americanstudy demonstrates few differences in plannedhome births and planned hospital births withlower rates <strong>of</strong> medical intervention when selectioncriteria is used and physician consultation isavailable (Janssen et al, 2006).Why would someone want to have a baby athome?An interview with Michelle Swanson, married mother<strong>of</strong> four, recently delivered her fourth baby at home,Cheyenne, Wyoming.Tell me about your previous birth experiences.Michelle: My first birth (at a hospital), eightyears ago included every intervention except ac-section; I got an epidural, additional IV painmedication, an episiotomy and then a forcepsdelivery, despite my labor from start to finish,lasting less than four hours. <strong>The</strong> OB/GYN believedmy son to be in a dangerous situation with the cordaround his neck, so did everything in his powerto deliver him quickly. Unfortunately, I spent therecovery time vomiting in the bathroom because<strong>of</strong> the IV medication, instead <strong>of</strong> holding/nursing/bonding with my son during the first hour afterhis birth. It took much longer than the allottedsix week period to recover from that first birthexperience. I remember it as a very scary time, withover 10 strangers in the room during the exposedpushing stage, alarms and monitors screaming andterrible nausea because <strong>of</strong> all <strong>of</strong> the medication inmy body.My second birth was an induction because <strong>of</strong>kidney trouble (stones and a never ending kidneyinfection). My labor again was very quick and mydaughter was caught by a nurse in the room becauseno one else was there. While I enjoyed the fastlabor (it was over quickly) I was worried for thenurse, knowing that she could get in trouble forcatching the baby, even though it would have beenunethical for her to leave the room to find a doctorwhile the baby was being delivered. Because mybaby didn’t spend much time in the birth canal,she was born with a lot <strong>of</strong> fluid still in her tummyand lungs. But because there were so many birthsthat day, she didn’t get “in to the system” and see adoctor until more than six hours after her birth. Iheld her in my arms and watched her gag and gaspfor breath for a long time. Even after bringing thisto the attention <strong>of</strong> several nurses, they said theycouldn’t do anything about it, until she was “inthe system” and we would just have to wait untilit was less busy to see a doctor. She was fine in theend, but we were definitely “just another number”during that hospital stay.My third and last hospital birth was the bestexperience <strong>of</strong> the three. My doctor knew that Ididn’t want any interventions, so she told thenurses to leave me alone, which they did, for thethree hours I labored at the hospital until mydaughter was born. <strong>The</strong> doctor made a hurtfulcomment though, as to the amount <strong>of</strong> noise I wasmaking during transition, and I’m still hurt bythat comment. After my baby was born and thedoctor was assessing for [perineal] tearing, she hada resident doctor with her, to whom I hadn’t beenintroduced. He was cleaning the area very roughly,when I startled in pain. She had to remind himthat I was not numb and he needed to be muchmore gentle. I was the first patient he had cared forwho had delivered a baby without an epidural. Wechecked out and went home only 18 hours afterher birth, so that I could rest! We had hospital staffin and out <strong>of</strong> our room, interrupting our resting,nursing or sleeping time, every 30 minutes or so;all wanting something else...to check a temp, toprick a heal, to get our supper meal order, to see ifwe needed a prayer, etc, etc, etc. It is impossible torecover from childbirth in a place where the mamaand the baby can’t bond and rest undisturbed.When did you decide you wanted a home birth foryour current pregnancy?Michelle: Before I conceived I knew I wantedto have a baby at home.What factors led you to seek a home birth?Michelle: <strong>The</strong>re were several factors I tookinto consideration; my previous hospital birthexperiences; the movie “<strong>The</strong> Business Of BeingBorn;” my work with counseling breastfeedingmothers and always talking to them about theimportance <strong>of</strong> a non-intervention birth and itseffects on breastfeeding; and the fact that a verygood friend had just had a safe and satisfying homebirth, here in Cheyenne, the previous summer.Who have you hired to attend your home birth?Michelle: My CNM Janet Schwab, and herlabor assistant, who is also a doula.What kind <strong>of</strong> research did you do to find a homebirth attendant?Michelle: I don’t think that I did any specificresearch about the safety <strong>of</strong> home births beforeI decided I wanted one. It was more like anintrinsic belief or understanding that home birthwas a safer, MORE NATURAL, form <strong>of</strong> birth,compared to the over-“medicalized” hospitalapproach to birth. Because I am a strong supporter/educator <strong>of</strong> breastfeeding and spend much <strong>of</strong> mytime emphasizing to mothers that breastfeeding isa normal, natural process, believing that birth too,is a normal and natural process is just an extension<strong>of</strong> those philosophies. While some births dorequire hospitalization and medical interventions,the majority <strong>of</strong> births does not and should notbe treated as though they do. I am familiar withIna May Gaskin and her books/research, plusthe overall outcome <strong>of</strong> home birth in othercountries, such as New Zealand, which furtheredmy convictions that the USA’s approach to birthand its overall health care system is a convolutedmess, driven by a fear <strong>of</strong> lawsuits. Money and feardo not contribute to a good overall quality <strong>of</strong> careand commitment to the patient and her needs,especially during such an emotional and climatictime as childbirth. I wanted someone attendingme who knew me as a person, as a friend, as awoman. Someone who knew the names <strong>of</strong> mychildren, who remembered (without looking atmy chart) the ups and downs <strong>of</strong> this pregnancy;someone who really wanted me to have the mostWy o m i n g Nu r s e Re p o r t e r 23
satisfying birth experience and believed that I wascompletely capable <strong>of</strong> delivering this baby safelyand at my own pace. That’s why I chose a homebirth and a midwife. If I wanted to be just anothernumber, just another insurance payment, justanother patient in the waiting room, then I wouldhave chosen a hospital birth.After our decision was made, it was just a matter<strong>of</strong> finding a midwife who could legally attenda home birth in Wyoming, and hoping that shewould be willing and able to travel to Cheyenneto do so. <strong>The</strong>re are only two CNMs within 100miles <strong>of</strong> Cheyenne.What have been the reactions <strong>of</strong> your family andfriends to your impending home birth?Michelle: Yes, in the very beginning <strong>of</strong> thehome birth discussions between my husband andme, he was concerned about safety, especiallybecause we had so many seemingly necessaryinterventions during our first birth. My husbandbelieved that had we not had those interventionswith my first pregnancy, the baby would have died.So we did a lot <strong>of</strong> talking about that first birth,and how one intervention led to another, then toanother and to another. <strong>The</strong> biggest interventionI received during that birth, was an epidural,which put me on my back for the rest <strong>of</strong> thedelivery. As a result I was unable to move into amore comfortable position, or one that could haveexpedited the delivery. This led to prolong pushing,additional strain on the baby, and the eventual use<strong>of</strong> forceps. Had I not been numb and flat on myback, I believe the birth would have been normaland safe. My husband was still concerned withthese ‘safety’ issues, so during our initial interviewwith our midwife, he was able to ask her questionsabout the overall safety <strong>of</strong> a home birth withmy history. My husband felt reassured by Janet’sanswers and by her credentials, and her ability touse medication during the delivery for both meand the baby, should the need arise. Had we beengiven the choice between a CNM and a CPM,we would have chosen the CNM because <strong>of</strong> theadditional training, credentials and availability <strong>of</strong>medications, especially because <strong>of</strong> my history <strong>of</strong>hemorrhaging.I would also like to mention the financial/insurance aspect. We have health insurance but westill do not know if my home birth will be coveredunder our insurance plan. Choosing a home birth,for us, was a financial burden and caused us bothstress. Janet requires her fee, <strong>of</strong> several thousanddollars, to be paid in full by 35 weeks. So we hadto withdraw that money from my husband’s 401Kaccount. Although a home birth overall, is far lesscostly than a hospital birth, it is harder to affordfor the average American family.My parents were both concerned about thesafety factor and my friends (outside <strong>of</strong> thebreastfeeding counseling world) have all beenuncomfortable with the thought <strong>of</strong> a home birth.Many think it is unsafe and illegal to have a homebirth in Wyoming.Whom do you plan to have present at your homebirth?Michelle: My husband, my sister (who hasacted as my doula at my previous births, like I havebeen for her at her births), Janet and her assistantand my two closest girlfriends.Do you have any concerns for your safety or that<strong>of</strong> your baby?Michelle: Janet and I have talked about thesethings. Because I have a history <strong>of</strong> heavy bleedingafter past deliveries, Janet will give me a shot <strong>of</strong>pitocin immediately after delivery and before theplacenta is delivered. She will also have the IVassembled and ready in case the pitocin shot is notenough.How much time has your midwife spent with youduring your pregnancy and where did these visitsoccur?Michelle: Janet came to my home everymonth for a prenatal appointment until week 28,when she came every two weeks, until week 34when her visits increased to weekly, the same asif I were seeing a traditional OB for my prenatalcare. Janet’s visits lasted between an hour anda half and two hours. We spent a lot <strong>of</strong> timediscussing, not just my physical preparation forchildbirth, but also my emotional and spiritualpreparation for childbirth. Janet’s concern was forme as a whole person, a whole woman, not justhow much weight I had gained or the size <strong>of</strong> mytummy at this prenatal visit. She supported meentirely, cared for my well-being completely, andgave me a type <strong>of</strong> care that I had never receivedwith any <strong>of</strong> my other pregnancies.After DeliveryMichelle: After I had the baby, she returned tocheck on us twice in those first few days followingthe birth. Janet’s fee covers also a day onepostpartum checkup for mom and baby and a daythree postpartum checkup for mom and baby, anda six week postpartum checkup for mom.Did your delivery go as you had hoped it would?Michelle: Yes. It was not what I planned orimagined, but it was more than I had hoped for!Each birth is different. Because Janet (as a midwife)does little or no unnecessary intervention, she didnot break my water during my labor. So my laborwas slowed, considerably, compared to my laborsat the hospital, where breaking a woman’s wateraround 5cm is a routine intervention. This allowedme to stay in control <strong>of</strong> the pain and contractions,despite the longer labor, because my bag <strong>of</strong> waterdidn’t break until my baby was crowning.Were there any complications or problems? If so,how do you feel things were handled?Michelle: My labor began during a blizzard,causing the Interstate to close and Janet to getsnowed in another client’s home, here in Cheyenne.It was very stressful to me. Janet remained in closephone contact with me, and kept me updatedabout when she expected to arrive at my house.Once she finally arrived though, my labor hadstalled out because <strong>of</strong> my fear and anxiety aboutthe blizzard. After staying the night on my s<strong>of</strong>a,Janet stripped my membranes the followingmorning and <strong>of</strong>fered to me a dose <strong>of</strong> Castor Oil toget labor started again. Both <strong>of</strong> those techniquesproved very effective, and I was in active labor lessthan two hours later.How do you feel about your home birth overall?Michelle: Despite the blizzard and the stalledlabor, I still LOVED my home birth and wouldnever deliver another child in a hospital unlessit was medically necessary. I labored in a birthingpool for three hours, while I was surrounded bycalm, supportive and loving people. <strong>The</strong>re wereno bright lights, beeping monitors or restrictionson eating (my husband made me a chicken broth- from scratch, to sip on during the last part <strong>of</strong>my labor, between contractions, to keep up mystrength and stamina). <strong>The</strong> curtains were closed,I was able to vocalize without fear <strong>of</strong> repercussion,and labored under the calming glow <strong>of</strong> candlelight,without interruptions or interventions. When mybaby was finally in my arms, she stayed there,learning to breathe, in peace and quiet untilthe cord stopped pulsating (about 10 minutes).Once I was out <strong>of</strong> the pool and had delivered theplacenta, Janet tucked me into my own bed andstepped back allowing me to nurse my daughterand bond with her for an hour, in peace and quiet.While I rested and bonded, my husband made mea fabulous meal. Janet and her assistant starteda load <strong>of</strong> laundry and cleaned up after the birth.Janet stayed for about three hours following thebirth, to make sure that my daughter and I werestable. I couldn’t have asked for more. It was theperfect end to a miraculous day!Where can I find someone to deliver my baby athome?An interview with Penelope Caldwell, Certified <strong>Nurse</strong>Midwife, attending home births in southeast, Wyoming.Have you delivered babies in hospitals duringyour career?Penelope: I delivered babies in hospitals, yes,large teaching hospitals, community hospitals,free standing birth centers for probably six yearsor more.How long have you being delivering babies athome?Penelope: I’ve been doing home births for10 years either working in a group with others orpracticing independently.How are institutional and home births differentfrom your perspective?Penelope: <strong>The</strong>re is a huge difference indoing institutional births and home births—it’simpossible to compare the two. <strong>The</strong> only thingthat’s the same is that a baby comes out. <strong>The</strong>reare no interventions usually in a home birth andthe chances <strong>of</strong> intervention are much less. <strong>The</strong>woman is at home in her environment whereshe is not inhibited, she can walk around, eat, benaked, tell people to leave; she has the people andthings she needs, there are no strangers present.Birth happens in a very normal way, it’s a verysacred space, its’ palpable. You don’t have thatsacred sense or energy in a hospital. You can’t.Hospitals are all about fixing things before theybreak, routine interventions, even if not needed orwanted. <strong>The</strong>re’s a lot <strong>of</strong> fear in the hospital, whichwill slow down labor or even stop it. <strong>The</strong>re’s justno comparison.As a midwife, birth centers are the happymedium; you can have shifts and share the work.You can let it go once your shift is over. Womencome to you, you don’t have to travel so much.<strong>The</strong>re’s a lot less time involved. <strong>The</strong> environmentis different but it feels safer than the hospital. Nostrangers, no lights, families move in and createtheir nest. People birth very well in birthingcenters. It’s a little easier for midwives to do thejob. Like a homebirth practice, there’s not muchmoney in birth centers either. Many birth centersdon’t make it financially.Would you ever go back into the hospitalsetting?Penelope: I would go back to hospital forfinancial reasons only. Homebirths do not pay thebills; it’s a labor <strong>of</strong> love. It’s very time consuming24 Wy o m i n g Nu r s e Re p o r t e r
and costs a lot in human hours. All the travel…one prenatal visit might take all afternoon. You’rethere for the whole labor and for several visitslater. And <strong>of</strong> course they never stop calling you.<strong>The</strong> relationship never ends, it’s not like it’s overonce the baby’s born. It’s a very different kind <strong>of</strong>career. It’s a very different kind <strong>of</strong> life. You’rejob is never finished when you’re a home birthmidwife. Historically, the midwife has always beenan integral part <strong>of</strong> the community, people come toher for advice, whether they are pregnant or not.It is still kind <strong>of</strong> like that.How can we keep home birth safe in Wyoming?An interview with Dr. Sharon Eskam, MD, Obstetricianand Gynecologist, Cheyenne Obstetrics andGynecology, Cheyenne, Wyoming.How do we make homebirth safe?Dr. Eskam: Some patients will choose a homebirth and face any possible risks, regardless <strong>of</strong>possible medical consequences, because they feelso strongly about a loss <strong>of</strong> personal autonomy.<strong>The</strong>se patients are <strong>of</strong>ten religiously, culturallyor personally motivated. Even though as anobstetrician I may not personally agree with thatchoice, I have an obligation to support theirdecision, and do anything that I can to maketheir delivery as safe as possible. Among the mostimportant things that I can do is to make sure theyare aware <strong>of</strong> any risk factors that they may haveand to plan for possible problems related to theserisks. Patients need to be made aware <strong>of</strong> any risksfactors as they may need to re-think their decisionif the risks are significant. <strong>The</strong>y also need to knowthat if they choose a home birth, the hospital willprovide any emergency treatment they may need ifa hospital delivery is necessary, without prejudiceto their previous decision.What is your vision <strong>of</strong> safe homebirth?Dr. Eskam: While the American College <strong>of</strong>Obstetricians and Gynecologists (ACOG) doesnot take a black/white approach to home birth,it does recognize that unexpected significantproblems may occur, making home birth inherentlymore risky than a hospital birth, although neithercan guarantee an absolute outcome. Certainly thebetter the training is for the home birth attendant,the better would be the possibly for avoidance <strong>of</strong>an adverse outcome by identifying risk issues asearly as possible.One <strong>of</strong> the issues that obstetricians havewith home birth is one <strong>of</strong> liability concern. Anexample <strong>of</strong> this would be if there was a hypoxicevent, which occurred at home during a homebirth attempt, and the patient was then broughtto the hospital. <strong>The</strong> hospital course could appearbenign, but if the baby were later diagnosed witha hypoxic encephlalopathy, it would be difficult toverify the timing <strong>of</strong> the event. This would probablymean a lawsuit for the obstetrician, as obstetriciansusually have more malpractice dollars available forrecovery than a home birth provider. A statewideprogram to provide recovery in the form <strong>of</strong> a birthinjury fund that would prohibit a lawsuit againstthe hospital or the obstetrician assuming care froma home birth attempt would go a long way towardsimproving the opinion <strong>of</strong> obstetricians regardinghome births.Things to PonderIn writing this article, I found manyinconsistencies and blatant errors in websites thatare primary resources for families to use duringpregnancy. I found several states with models <strong>of</strong>home birth and direct entry midwifery that areworking beautifully. For example, in Washingtonstate and Colorado, direct entry midwives arelicensed and regulated, just as physicians andnurses are, and they attend home births and arereimbursed by insurance and Medicaid. Everyonehas their niche and there are even some practiceswith physicians, nurse midwives and direct entrymidwives all working together in the same practice.It was amazing how well these systems are workingwell for everyone involved and how well everyoneseems to be working together. Home birth isn’tfor everyone, but it will always be the choicefor some. Wouldn’t it be great if we could worktogether and find a way to make Wyoming one <strong>of</strong>the best places to have a baby, regardless <strong>of</strong> whereyou wanted to deliver?Acknowledgments<strong>The</strong> author wishes to thank Gabrielle Scharp, BSN,RN, SNM for her contributions to the section titled“<strong>The</strong> History <strong>of</strong> Midwifery in America.”Continued on next pageWy o m i n g Nu r s e Re p o r t e r 25
Why all the Confusion about Midwivesand Home Birth? Isn’t home birthillegal in Wyoming anyway?Continued from page 25ReferencesBreckinridge, M. (1981). Wide neighborhoods: A story <strong>of</strong> the Frontier Nursing Service.Lexington, KY: University Press.Cassidy, T. (2006). Birth: <strong>The</strong> surprising history <strong>of</strong> how we are born. New York: AtlanticMonthly Press.Durand, M.A. (1992). <strong>The</strong> safety <strong>of</strong> home birth: the Farm study. American Journal <strong>of</strong>Public Health, 82(3), 450-453.Janssen, P., Ryan, E., Etches, D. J., Klein, M.C. and Reime, B. (2006). Outcomes <strong>of</strong>planned hospital birth attended by midwives compared with physicians in British Columbia.Birth 34(2), 140-47.Leavitt, J. (1983). “Science” enters the birthing room: Obstetrics in America since theeighteenth century. <strong>The</strong> Journal <strong>of</strong> American History, 70(2), 281-304.Lit<strong>of</strong>f, J. (1982). <strong>The</strong> midwife throughout history. Journal <strong>of</strong> <strong>Nurse</strong>-Midwifery, 27(6),3-11.Olsen, O (1997). Meta-analysis <strong>of</strong> the safety <strong>of</strong> home birth. Birth,24(1), 4-13.Rooks, J., Weatherby, N., Ernst, E., Stapleton, S., Rosen, D., & Rosenfield, A. (1989).Outcomes <strong>of</strong> care in birth centers: <strong>The</strong> national birth center study. New England Journal <strong>of</strong>Medicine, 321(26), 1804-1811.Rooks, J. (1997). Midwifery and childbirth in America. Philadelphia: Temple UniversityPress.Stone, S. (2000). <strong>The</strong> evolving scope <strong>of</strong> nurse-midwifery practice it the United States. Journal<strong>of</strong> Midwifery & Women’s Health, 45(6), 522-531.<strong>The</strong> American College <strong>of</strong> <strong>Nurse</strong>-Midwifery (2009). Retrieved April 23, 2009 from http://www.acnm.org/about.cfm and http://www.acnm.org/organization_history.cfmNursys® Update forNon-compact jurisdictionsEmployers/PublicIf you or your organization needs to increase your efficiency inverifying nurse licenses and/or checking a nurse’s discipline statusfor employment decisions, then look no further than the NationalCouncil <strong>of</strong> State Boards <strong>of</strong> Nursing’s secure, online verificationsystem, Nursys® (www.nursys.com). <strong>The</strong> nursys.com web sitecontains data obtained directly from the licensure systems <strong>of</strong> theboards <strong>of</strong> nursing through frequent, secured updates.Employers and the general public can now verify licenses andreceive a report within minutes, free <strong>of</strong> charge. This report willcontain the name, jurisdiction, license type, license number,license status, expiration date and any discipline against thelicense <strong>of</strong> the nurse being verified.<strong>Nurse</strong>sWhen a nurse applies for endorsement into a state, verification <strong>of</strong>existing or previously held licenses may be required. A nurse canuse Nursys.com to request verification <strong>of</strong> licensure from a Nursyslicensure participating board. A list <strong>of</strong> licensure participatingnursing boards can be found at Nursys.com.Verifications can be processed by completing the online Nursysverification process. <strong>The</strong> fee for this service is $30.00 per licensetype for each state board <strong>of</strong> nursing where the nurse is applying.Nursys license verification is sent to the endorsing boardimmediately. Please visit www.nursys.com for more details.For more information, email nursys@ncsbn.org, call 312.525.3780or visit www.nursys.comTargeted Networking<strong>The</strong> “NEW” ClassifiedsReach 11,000 nurses in Wyoming for as little as $260.limitedavailabilityCALL TODAYWork in Comfort!Your Wyoming source for scrubs,footware, compression hosiery andmore! Great assortment, mutliplebrand lines.Kimberly’s Uniforms(307) 235-3156Visit www.KimberlysUniforms.comContact Victor Hornevhorne@pcipublishing.com1-800-561-4686NURSEEDUCATORSRecruit TalentedFaculty HereVictor Horne(800) 561-4686RivertonMemorial HospitalSeekingFull-time ER/ICU RNFull-time OB RN$6,000 sign on, medical,dental, vision, Life, AD&D,STD, LTD, EAP, 401(k), PTO,EIB, and a competitive wage.Call 307-857-3465 oremail norma.atwood@lpnt.net.Wyoming<strong>Role</strong> <strong>of</strong> <strong>The</strong>Pr<strong>of</strong>essional <strong>Nurse</strong><strong>Role</strong> Differentiation:What’s the Problem?Thinkaboutitnursingscholarship funfund<strong>Nurse</strong>Vol. 5 number 2Summer 2009R E P O R T E RFocus on Practice:Nursing research clarifiesbest practices for blood pressuremeasurementAPPLYTODAY26 Wy o m i n g Nu r s e Re p o r t e r
<strong>The</strong> UMKC RN-BSNRural <strong>Nurse</strong> InitiativeAdvancement. Access. At your fingertips.Contact the University <strong>of</strong>Missouri-Kansas City School <strong>of</strong> Nursingat 1-800-499-8652 or visitwww.umkc.edu/nursingVIRTUALLY CONNECTINGBreathe new lifeinto your career.THERE IS OPPORTUNITYIN THE AIR.At Banner Health’s Wyoming facilities, weunderstand the vital role our nurses play inour success. We provide an environmentthat is rich in opportunities, <strong>of</strong>fers growthand development and is equipped with thelatest in life-saving technology. As a 2009Gallup Great Workplace Award recipient,our commitment to our employees is evident.We make a difference in our employees’ livesso they can make a difference in the lives<strong>of</strong> others.Opportunities availablefor the following positions:Director <strong>of</strong> Nursing – LTCand Patient Care ManagerPlatte County Memorial Hospital, WheatlandRegistered <strong>Nurse</strong> and LPNGoshen Care Center, TorringtonRegistered <strong>Nurse</strong> – OBWashakie Medical Center, WorlandBreathe new life into your career.Call 307-534-7157 or visit:jobs.BannerHealth.com/wynEOE/AA Banner Health supports a drug-free work environment.Memorial Hospital <strong>of</strong> Converse County is a state licensed,Medicare certified, 25 bed Critical Access Hospital locatednear downtown Douglas, Wyoming, surrounded by scenicLaramie Peak and Medicine Bow National Forest.•••••••••••Big Hospital Services - Small HospitalEnvironmentContinuous Opportunities for TrainingSafe Community to Live and WorkProven Successful Preceptor ProgramNo State Income TaxStrong Community EconomyHousing AssistanceTuition Reimbursement OptionsRelocation AssistanceFull Benefits availableGreat Opportunities!To Find Out More Information:www.ConverseHospital.comor call 307-358-1403Wy o m i n g Nu r s e Re p o r t e r 27
Disciplinary ActionsDorothy Barthel, CNAApril 9, 2009Voluntary SurrenderDorothy Barthel, CNA, voluntarily surrendered her certificate after she admitted having oralsex with an active client at an inpatient addiction recovery center.Grounds for Discipline: Chapter VII, Section 11(b) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (G) Boundary Violations, including sexual boundaries;(iv) Failure to conform to the standards <strong>of</strong> prevailing nursing practice, in which case actualinjury need not be established.Amanda Carubie, CNAApril 8, 2009Letter <strong>of</strong> ReprimandAmanda Carubie, CNA was issued a letter <strong>of</strong> reprimand for her conduct in photographing aresident <strong>of</strong> a residential nursing facility. <strong>The</strong> resident was nude from the waist down. AfterCarubie took the picture, she showed the picture to three (3) other coworkers and indicatedthat she intended to forward the picture to her husband. When told that the picture was“illegal”, she deleted it from her phone. In response to the Board’s investigation, Carubieadmitted her conduct and expressed regret.Grounds for Discipline: Chapter VII, Section 11(b) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (D) Client abuse, including sexual abuse; (F) Clientneglect; (G) Boundary violations, including sexual boundaries; (iv) Failure to conform to thestandards <strong>of</strong> prevailing nursing practice, in which case actual injury need not be established.Kevin Franke, RNApril 9, 2009Voluntary SurrenderKevin Franke, RN will voluntarily surrender his license as a result <strong>of</strong> his conduct in divertingFentanyl by June 30, 2009. An internal investigation revealed discrepancies in the PYXISand patient Medication Administration Records and the facility questioned Franke regardinghis withdrawals <strong>of</strong> Fentanyl from the PYXIS. Franke admitted he relapsed during this timewhich violated a previous conditional licensing agreement by handling narcotics and divertingFentanyl.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (iv) Failure toconform to the standards <strong>of</strong> prevailing nursing practice, in which case actual injury need notbe established.Tyana Giesler, CNAJanuary 5, 2009Letter <strong>of</strong> ReprimandTyana Giesler, CNA was issued a letter <strong>of</strong> reprimand for her conduct in “force feeding” aresident while the resident repeatedly told Giesler that she needed to use the restroom. Giesleradmitted that she was dismissive <strong>of</strong> the resident’s requests.Grounds for Discipline: Chapter VII, section 11(b) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (D) Client abuse, including sexual abuse; (F) Clientneglect; (H) Performance <strong>of</strong> unsafe client care; (iv) Failure to conform to the standards <strong>of</strong>prevailing nursing and nursing assistant/nurse aid practice, in which case actual injury neednot be established.Susanna Herrman, RNApril 9, 2009ConditionalSusanna Herrman, RN was granted a conditional license after her conduct in divertingDemerol from a medication cart. Ms. Herrman admitted to this conduct. Herrman enrolledin the Wyoming Pr<strong>of</strong>essional Assistance Program (WPAP) in August 2006 and signed aWPAP monitoring agreement.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (iv) Failure toconform to the standards <strong>of</strong> prevailing nursing practice, in which case actual injury need notbe established.Jill Johnson, RNApril 9, 2009Voluntary SurrenderJill Johnson, RN voluntarily surrendered her license as a result <strong>of</strong> her conduct in approachinga physician for a prescription <strong>of</strong> Ativan for a patient and after attempting to fill the prescriptionfor herself at the pharmacy. Johnson pleaded guilty to one count <strong>of</strong> Possession <strong>of</strong> ControlledSubstance by Fraud and was placed on three (3) years <strong>of</strong> supervised probation. In a writtenstatement provided to the Board <strong>of</strong>fice, Johnson admitted she had entered a plea agreementand received probation. Johnson also admitted to abuse <strong>of</strong> prescription medication and toaltering the Ativan prescription by adding her name, address, age and date on theprescription, though she denied any willful wrongdoing and attributed her alteration to a“miscommunication” she had with the prescribing physician. Though Johnson verbally agreedto participate in the Hawaii <strong>Nurse</strong> Association Peer Assistance Program in June 2007, shedid not sign a monitoring agreement with the program until May 2008.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (iv) Failure toonform to the standards <strong>of</strong> prevailing nursing practice, in which case actual injury need notbe established.Kelly Johnson, RNApril 9, 2009Voluntary SurrenderKelly Johnson, RN voluntarily surrendered her license as a result <strong>of</strong> her conduct in divertingnarcotics from the medication cart at a residential living center. Johnson was witnessed onseveral occasions crushing pills and then proceeding to the restroom for a period <strong>of</strong> time beforeleaving the restroom. Johnson was later charged in prescription fraud and was placed onprobation following conviction. Johnson admitted to the Board that she diverted medicationsand admitted to a substance abuse problem. During the course <strong>of</strong> the Board’s investigation,Johnson enrolled in the Wyoming Pr<strong>of</strong>essional Assistance Program (WPAP) which lateradvised that Johnson be restricted from direct patient care for a significant period <strong>of</strong> time. Alsoduring the Board’s investigation, Johnson voluntarily surrendered her Colorado registerednurse license.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (iv) Failure toconform to the standards <strong>of</strong> prevailing nursing practice, in which case actual injury need notbe established.James Judd, LPNApril 9, 2009ConditionalJames Judd, LPN was issued a conditional license as a result <strong>of</strong> his conduct in taking anOxycodone pill from a resident at a residential care center. Judd enrolled in the WyomingPr<strong>of</strong>essional Assistance Program (WPAP) and signed a monitoring agreement with WPAP.Judd was later convicted <strong>of</strong> acquiring a controlled substance by fraud or misrepresentationand possession <strong>of</strong> a controlled substance without a valid prescription. Judd was placed onsupervised probation for these convictions.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (iii) CriminalConviction; (iv) Failure to conform to the standards <strong>of</strong> prevailing nursing practice, in whichcase actual injury need not be established.Shellie Meyer, RNApril 9, 2009ConditionalShellie Meyer, RN was granted a conditional license after she was observed on video taperemoving a single dose vial <strong>of</strong> Morphine Sulfate from the emergency use box and returningit later. It was later discovered, on or about October 11, 2005, that the Morphine Sulfatesingle dose vial had been tampered with. Meyer was arrested for acquiring possession <strong>of</strong> acontrolled substance by deception or subterfuge and for omitting material information fromany document or record required to be kept or filed under the Wyoming Controlled SubstanceAct. Meyer pled guilty to the charge <strong>of</strong> “Acquire Possession <strong>of</strong> a Controlled Substance byFraud, Forgery, Deception or Subterfuge.” She was placed on three years <strong>of</strong> supervisedprobation. In Meyer’s response to the Board’s Notice <strong>of</strong> Complaint letter, she admitted shediverted Morphine Sulfate for her personal use.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (ii) Misappropriationor misuse <strong>of</strong> property; (iii) Criminal conviction.28 Wy o m i n g Nu r s e Re p o r t e r
Susanna Patterson, RNApril 9, 2009Letter <strong>of</strong> ReprimandSusanna Patterson, RN was issued a Letter <strong>of</strong> Reprimand as a result <strong>of</strong> her conduct inobtaining Lortab Elixer from the pharmacy without a physician’s order, without verifyingwhether a standing order existed, and later administering it to a patient.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rules andRegulations: (iv) Failure to conform to the standards <strong>of</strong> prevailing nursing practice, in whichcase actual injury need not be established.Jody Shine, RNApril 9, 2009ConditionalJody Shine, was granted a conditional license as a result <strong>of</strong> her conduct in removing Demerolon twenty-one (21) patients who did not have physician’s orders for Demerol. Shine had beenunder a monitoring agreement with the Wyoming Pr<strong>of</strong>essional Assistance Program (WPAP).In 2007, the monitoring agreement terminated, however, Shine voluntarily continues to bemonitored by WPAP.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (ii) Misappropriationor misuse <strong>of</strong> property.Genevieve Trogden, RNApril 8, 2009ConditionalGenevieve Trogden, RN was issued a conditional license for her conduct in testing positivefor cocaine metabolites. Trogden admitted trying cocaine at a party a couple days before thedrug screening. Subsequent drug screens were negative.Grounds for Discipline: Chapter III, section 4(a) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (B) Substance abuse/dependency; (iv) Failure toconform to the standards <strong>of</strong> prevailing nursing practice, in which case actual injury need notbe established.Kico Vasco, CNAApril 9, 2009Letter <strong>of</strong> ReprimandKico Vasco, CNA was issued a letter <strong>of</strong> reprimand as a result <strong>of</strong> his conduct in accompanyingseveral residents <strong>of</strong> a residential living center into a bar and adult entertainment facility inCasper following their attendance at a football game in Laramie.Grounds for Discipline: Chapter VII, Section 11(b) <strong>of</strong> the Board’s Administrative Rulesand Regulations: (i) Inability to function with reasonable skill and safety for the followingreasons, including but not limited to: (H) Performance <strong>of</strong> unsafe client care; (iv) Failure toconform to the standards <strong>of</strong> prevailing nursing practice, in which case actual injury need notbe established.Denials <strong>of</strong> Applicants Seeking Licensure or Certification<strong>The</strong> <strong>Nurse</strong> Practice Act, 33-21-146 identifies the following reasons that an application may be denied:“(a) <strong>The</strong> board <strong>of</strong> nursing may refuse to issue or renew,or may suspend or revoke the license, certificate ortemporary permit <strong>of</strong> any person, or to otherwise disciplinea licensee, upon pro<strong>of</strong> that the person:(i) Has engaged in any act inconsistent withuniform and reasonable standards <strong>of</strong> nursing practiceas defined by board rules and regulations;(ii) Has been found guilty by a court, has entered anAlford plea or has entered a plea <strong>of</strong> nolo contendereto a misdemeanor or felony that relates adversely tothe practice <strong>of</strong> nursing or to the ability to practicenursing;(iii) Has practiced fraud or deceit:(A) In procuring or attempting to procure a license topractice nursing;(B) In filing or reporting any health care information,including but not limited to client documentation,agency records or other essential health documents;(C) In signing any report or record as a registered nurseor as a licensed practical nurse;(D) In representing authority to practice nursing; or(E) In submitting any information or record to theboard.(iv) Is unfit or incompetent to practice nursing byreason <strong>of</strong> negligence, habits or other causes includingbut not limited to:(A) Being unable to practice nursing with reasonableskill and safety to patients by reason <strong>of</strong> physical ormental disability, or use <strong>of</strong> drugs, narcotics, chemicals orany other mind-altering material; or(B) Performance <strong>of</strong> unsafe nursing practice or failureto conform to the essential standards <strong>of</strong> acceptable andprevailing nursing practice, in which case actual injuryneed not be established.(v) Has engaged in any unauthorized possession orunauthorized use <strong>of</strong> a controlled substance as definedin the Wyoming Controlled Substances Act [§§ 35-7-1001 through 35-7-1057];(vi) Has had a license to practice nursing or topractice in another health care discipline in anotherjurisdiction, territory or possession <strong>of</strong> the UnitedStates denied, revoked, suspended or otherwiserestricted;(vii) Has practiced nursing within this state withouta valid current license or temporary permit or asotherwise permitted under this act;(viii) Has knowingly and willfully failed to report tothe board any violation <strong>of</strong> this act or <strong>of</strong> board rulesand regulations;(ix) Has been found by the board to have violatedany <strong>of</strong> the provisions <strong>of</strong> this act or <strong>of</strong> board rules andregulations; or(x) Has knowingly engaged in an act whichthe licensee knew was beyond the scope <strong>of</strong> theindividual’s nursing practice prior to committing theact, or performed acts without sufficient education,knowledge, or ability to apply nursing principles andskills; or(xi) Has failed to submit to a mental, physical ormedical competency examination following a properrequest by the board made pursuant to board rulesand regulations and the Wyoming AdministrativeProcedure Act.(b) Upon receipt from the department <strong>of</strong> family services<strong>of</strong> a certified copy <strong>of</strong> an order from a court to withhold,suspend or otherwise restrict a license issued by theboard, the board shall notify the party named in thecourt order <strong>of</strong> the withholding, suspension or restriction<strong>of</strong> the license in accordance with the terms <strong>of</strong> the courtorder. No appeal under the Wyoming AdministrativeProcedure Act shall be allowed for a license withheld,suspended or restricted under this subsection” (pg 12-13<strong>of</strong> 18).<strong>The</strong> following actions were taken on applications:Michael Bond, CNA ApplicantDenial Assault & Battery with Probation December 25, 2008Ekaterina Inanova, CNA ApplicantDenial DUI with Supervised Probation March 23, 2009Lacy Raney, CNA ApplicantDenial Drugs –Unlawful Possession <strong>of</strong> Controlled Substance February 22, 2009DUIJessica Tjaden, CNA ApplicantDenial Possession <strong>of</strong> a Controlled Substance April 16, 2009Minor in Possession-AlcoholKristi Tomich, RN ApplicantDenial 2005 & 2007 DUI Convictions April 16, 2009Denial <strong>of</strong> Licensure in CaliforniaWy o m i n g Nu r s e Re p o r t e r 29
NCSBN Unveils NewNursys.com Web Sitewith Enhanced <strong>Nurse</strong> Licensure Verification ToolsChicago - <strong>The</strong> National Council <strong>of</strong> StateBoards <strong>of</strong> Nursing’s (NCSBN) Nursys.com licenseverification Web site recently unveiled anew and improved verification process, whichmakes nurse license verification quicker, easierand free <strong>of</strong> charge to employers and the generalpublic.<strong>The</strong> Licensure QuickConfirm applicationallows employers and the general public to verifylicenses from a public access Nursys licensureparticipating board <strong>of</strong> nursing.* Withinminutes, a detailed report is generated, containingthe nurse’s name, jurisdiction, licensetype, license number, license status, expirationdates, as made available by the board <strong>of</strong> nursingfor all licenses held, and any discipline againstthe license.In addition, Nursys.com also enables nursesto verify their license(s) from a Nursys licensureparticipating board <strong>of</strong> nursing** when applyingfor endorsement into another state byusing the online <strong>Nurse</strong> Licensure Verificationapplication. <strong>Nurse</strong>s can verify their licenses bycompleting the Nursys verification process for$30.00 per license type, per each state board<strong>of</strong> nursing where the nurse is applying. <strong>The</strong>nurse’s license verification is available immediatelyto the endorsing board <strong>of</strong> nursing.“We feel that online nurse licensure verificationis extremely important, especially inthe evolving and <strong>of</strong>ten mobile world <strong>of</strong> healthcare,” said Kathy Apple, MS, RN, CAE,NCSBN CEO. “Nursys.com contains data obtaineddirectly from the licensure systems <strong>of</strong>the boards <strong>of</strong> nursing. This allows nurses andemployers to verify licenses in a secure mannerwhile boards <strong>of</strong> nursing continue to protect thepublic.”For those states participating in the <strong>Nurse</strong>Licensure Compact (NLC), which is a mutualrecognition model <strong>of</strong> nurse licensure thatallows a nurse to have one license (in his orher state <strong>of</strong> residency) to practice in multiplestates, Nursys.com can be used to verifya nurse’s NLC status (multistate/single state)and any discipline against privilege to practicefrom an NLC state. A nurse must legallyreside in an NLC state in order to be eligiblefor a multistate license in the NLC. An active,unencumbered, multistate license allowsthe nurse to practice in all 23 NLC*** jurisdictions.Questions about NLC eligibility andlegal residency can be directed to the state’sboard <strong>of</strong> nursing. Currently, Nursys.com is theonly verification tool available that providesthe status <strong>of</strong> a multistate license’s privilege topractice in NLC jurisdictions.<strong>The</strong> National Council <strong>of</strong> State Boards <strong>of</strong>Nursing (NCSBN) is a not-for-pr<strong>of</strong>it organizationwhose members include the boards <strong>of</strong>nursing in the 50 states, the District <strong>of</strong> Columbiaand four U.S. territories - American Samoa,Guam, Northern Mariana Islands and the VirginIslands. <strong>The</strong> College <strong>of</strong> Registered <strong>Nurse</strong>s<strong>of</strong> British Columbia is an associate member.Mission: <strong>The</strong> National Council <strong>of</strong> StateBoards <strong>of</strong> Nursing (NCSBN), composed <strong>of</strong>Member Boards, provides leadership to advanceregulatory excellence for public protection.*QuickConfirm Public Access LicensureParticipating Boards <strong>of</strong> Nursing as <strong>of</strong> May 1,2009Alaska, Arizona, Arkansas, Colorado, Delaware,District <strong>of</strong> Columbia, Florida, Idaho, Indiana,Iowa, Kentucky, Louisiana - RN, Maine,Maryland, Massachusetts, Minnesota, Mississippi,Nebraska, New Hampshire, New Jersey,New Mexico, North Carolina, North Dakota,Ohio, Oregon, Rhode Island, South Carolina,South Dakota, Tennessee, Texas, Utah, Vermont,Virgin Islands, Virginia, West Virginia- PN, Wisconsin, Wyoming**Nursys Licensure Participating Boards <strong>of</strong>Nursing as <strong>of</strong> May 1, 2009Alaska, Arizona, Arkansas, Colorado, Delaware,District <strong>of</strong> Columbia, Florida, Idaho,Indiana, Iowa, Kentucky, Louisiana - RN,We are Hiring!Jobs available now for<strong>Nurse</strong>s and <strong>Nurse</strong> ManagersGreat Pay,Great Benefits,Great People.Maine, Maryland, Massachusetts, Minnesota,Mississippi, Missouri, Montana, Nebraska,New Hampshire, New Jersey, New Mexico,North Carolina, North Dakota, Ohio, Oregon,Rhode Island, South Carolina, South Dakota,Tennessee, Texas, Utah, Vermont, Virgin Islands,Virginia, Washington, West Virginia -PN, Wisconsin, Wyoming**NLC Participating States as <strong>of</strong> May 1, 2009Arizona, Arkansas, Colorado, Delaware, Idaho,Iowa, Kentucky, Maine, Maryland, Mississippi,Nebraska, New Hampshire, New Mexico,North Carolina, North Dakota, Rhode Island,South Carolina, South Dakota, Tennessee,Texas, Utah, Virginia, WisconsinContact: Dawn M. KappelDirector, Marketing & Communications312.525.3667 direct312.279.1034 faxdkappel@ncsbn.org111 E. Wacker Drive, Suite 2900Chicago, IL 60601-4277312.525.3600 | http://www.ncsbn.org/International Calls: +1.312.525.3600Call or e-mail us for more details.www.WyomingMedicalCenter.com307.577.2669 • sstephens@wmcnet.orgCasper, WyomingEOE30 Wy o m i n g Nu r s e Re p o r t e r
Come join our exciting and innovative multidisciplinary treatment team. We are a modern, dynamic 90 bed growingJoint Commission accredited behavioral health hospital serving children, adolescents, and adults.• We believe that each patient who walks through our front door is unique.• Each experience a person has shapes their behavior.• Every patient receives a multi-disciplinary assessment.WE ARE LOOKING FOR NURSES WHO:• Strive for excellence• Value therapeutic, interpersonal relationships• Desire to search for patterns <strong>of</strong> unpredictable and risky behavior• Choose to pursue the development <strong>of</strong> their personal destiny• Possess compassionate hearts towards those who lead unstable livesCOMMITMENT TO SERVICE EXCELLENCE:• Treat everyone as a guest• Demonstrate pr<strong>of</strong>essionalism and a commitment excellence• Practice TeamworkWe <strong>of</strong>fer an excellent compensation/benefit packageCall Jon Barra / HR Director, Ph 800-457-9312, Fax 307-256-5525 oremail your cover letter and resume to jon.barra@uhsinc.comResumes may also be mailed to:Wyoming Behavioral Institute Attn: Jon Barra2521 E 15th Street, Casper, WY 82609Wyoming Behavioral Institute is owned by UHS (Universal Health Services),one <strong>of</strong> the largest providers <strong>of</strong> high-quality healthcare in the nation. www.uhsinc.com
Wy o m i n g St a t e Bo a r d o f Nu r s i n g1810 Pioneer Ave.Cheyenne, Wyoming 82002Presorted StandardU.S. Postage PaidMontezuma, IowaPermit No. 30Call to request a freeCD-Rom introducing youto Regional Health and thebeautiful Black Hills.1-800-865-2638Go on-line for currentopenings, job descriptions,and benefits atwww.regionalhealth.comIn the Black Hills, you’ll discover a great place to liveand a great place to work. We’ve invested our resourcesto create a career environment built upon a commitmentto excellence. You’ll find yourself putting compassion intopractice while you work with leading-edge technology.And after you’ve helped others, help yourself to the beauty <strong>of</strong>the Black Hills. Go for a drive. Marvel at the monuments. Ridea horse. Experience history. Take a hike. Climb a mountain orjust sit beside a waterfall and read a book. It’s all waiting inour backyard.Regional Health, a system <strong>of</strong> hospitals, clinics, and seniorcare facilities, <strong>of</strong>fers the best <strong>of</strong> both worlds to nurses:competitive pay and benefits presented with valuable opportunitiesfor career development in an atmosphere <strong>of</strong> respectwhere the sky is the limit. Inside and out.It’s no wonder our nurses find it hard to leave.Equal Opportunity Employer353 Fairmont Boulevard Rapid City, SD 57701CUSTER REGIONAL HOSPITAL • LEAD-DEADWOOD REGIONAL HOSPITAL • RAPID CITY REGIONAL HOSPITAL • SPEARFISH REGIONAL HOSPITAL •STURGIS REGIONAL HOSPITAL