
You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
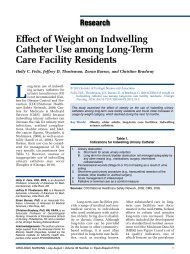
SERIES<strong>Managing</strong> a <strong>Pessary</strong> <strong>Business</strong>Katharine O’Dell, Leslie Saltzstein Wooldridge, and Shanna AtnipSPECIAL SERIES ON PESSARIESThis article discusses topicsimportant to developingan effective pessarypractice, includinga review of office managementoptions related to fitting, stocking,and maintaining pessaries,and compliance issues related toappropriate billing and coding.<strong>Pessary</strong> Fitting and StockingDecisionsTo initiate pessary services,providers must develop an overallplan for fitting and dispensingthese devices. Figure 1 offers anoverview of typical options thatwill need to be considered andtheir relationships to the devel-Katharine O’Dell, PhD, CNM, WHNP-BC,is an Assistant Professor of OB/GYN, theDivision of Pelvic Medicine andReconstructive Surgery, UMass MemorialMedical Center, Worcester, MA.Leslie Saltzstein Wooldridge, MSN, GNP,BCIA, F-AGS, is a Nurse Practitioner andthe Director the Bladder Control Center,Muskegon, MI.Shanna Atnip, MSN, WHNP-BC, is a NursePractitioner, the Division of Urogynecologyand Reconstructive Pelvic Surgery,Parkland Health & Hospital System, and theUniversity of Texas Southwestern MedicalCenter, Dallas, TX.Note: Objectives and CNE Evaluation Formappear on page 146.Statements of Disclosure: Leslie SaltzsteinWooldridge disclosed that she is on theConsultant/Presenters’ Bureau for AstellasUroplasty.Shanna Atnip and Katharine O’Dell had noactual or potential conflicts of interest inrelation to this continuing nursing educationactivity.This learning activity was partially fundedby an unrestricted educational grant fromCooperSurgical, Inc.© 2012 Society of Urologic Nurses and AssociatesO’Dell, K., Wooldridge, L.S., & Atnip, S. (2012). <strong>Managing</strong> a pessary business.Urologic Nursing, 32(3), 138-146.In this final article in a series of three, components of pessary fitting, provision,and follow up are reviewed from a business perspective related to supplies,patient flow, billing, and coding.Key Words:Pelvic organ prolapse, pessary, pelvic floor, billing and coding.Objectives:1. Describe the initiation and management of pessary services in a healthcare practice.2. Discuss the plan for fitting and dispensing of pessaries in a health carepractice.3. Explain the billing and coding system for pessary reimbursement.opment of a practice plan. Forexample, pessary fitting may beaccomplished by either usingactual pessaries or using fittingkits. Either way, it is common fora new user to try at least two orthree pessaries before finding onethat is comfortable and effective(Komesu et al., 2008). For thisreason, cleaning and sterilizationoptions for the chosen fittingdevice must be readily available.Providers are advised to checkwith the manufacturer of pessariesthey stock and follow therecommended guidelines. In theUnited States, many pessariesand fitting kits are autoclavablesilicone, making access to anautoclave an essential element ofthe pessary business plan. How -ever, for some air-filled pessaries,such as the Donut and the inflatablesilicone Donut, alternativesterilization options should beused (Bioteque of America, 2011).When the decision has beenmade to stock pessaries and/orfitting kits, the practice mustdecide which styles and sizes tostock. In terms of their clinicaluse, pessaries can generally bedivided into three categories:support pessaries that are re -Urologic Nursing Editorial Board Statements of DisclosureIn accordance with ANCC-COA governing rules Urologic Nursing Editorial Board statementsof disclosure are published with each CNE offering. The statements of disclosure forthis offering are published below.Susanne A. Quallich, ANP-BC, NP-C, CUNP, disclosed that she is on the Consultants’Bureau for Coloplast.All other Urologic Nursing Editorial Board members reported no actual or potentialconflict of interest in relation to this continuing nursing education activity.138 UROLOGIC NURSING / May-June 2012 / Volume 32 Number 3
Figure 1.Sample Decision Tree for <strong>Pessary</strong> Practice ManagementWill practice provide pessary care?NoKnow referral optionsYesFitting and follow upFitting kitsonlyPurchase at leastone kit from eachcategory. Checklocal pharmacies/medical equip -ment storesrelated to optionsfor patientpurchase.Will care include fitting or only follow up?Completearray ofpessariestypes andsizesPurchase stock; planstorage, inventory,ordering methodsLimited pessarystockFollow up onlySelect and purchasecommon sizes of atleast one type ofpessary from eachcategory. Knowreferral options.No special equipment ifsite provides women’shealth services; knowreferral options.SPECIAL SERIES ON PESSARIESComplete equipment checklist (see Table 1)tained by relatively intact pelvicmuscle integrity, support pessariesthat are somewhat selfretaining,and pessaries that offeradditional urethral support forwomen with stress urinary in -continence. Some large referralpractices may have sufficientvolume of potential pessary usersto justify stocking several stylesof each category of pessary, aswell as a complete range of sizesof each style. Smaller practiceshave several options for limitingtheir up-front purchasing costs.Table 1.Office Resources Necessary for <strong>Pessary</strong> ManagementAssorted pessaries and/or fitting rings<strong>Pessary</strong> cleaning plan prior to re-sterilizationAutoclave, cold, or alternate sterilizationAppropriate educational materialsFollow-up visit tracking systemAfter-hours contact and referral planGeneral pelvic examination equipment, including options for vaginitis and urinarytract infection screening<strong>Pessary</strong> cart or other storage areaInventory and re-order planUROLOGIC NURSING / May-June 2012 / Volume 32 Number 3 139
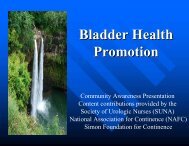
SERIESSPECIAL SERIES ON PESSARIESFigure 2.Sample Office Procedure for Cold Sterilization of Pessaries1. Cidex OPA ® is used to disinfect pessaries in the bladder control clinic.2. First, clean the pessaries with enzymatic detergent. Mix 15 mL of detergentwith 1 gallon of water. Soak pessaries for 5 minutes.3. Thoroughly clean and rinse the pessaries and pat dry.4. Test Cidex OPA with Cidex OPA test strips according to package directionsto make sure the solution meets minimum effective concentration, recordingdate, time, lot number of solution, test pass or fail, and staff member initialsin the monitoring log.5. If the solution passes, proceed to disinfecting the pessaries. If it does not,discard the solution, clean and dry the container, and put new solution in.Test this new solution to make sure it passes and meets the minimumeffective concentration, recording results in the monitoring log.6. After donning the appropriate personal protective equipment (gloves,goggles, and gown), place the pessaries in the Cidex OPA for 12 minutes forhigh level disinfection.7. After 12 minutes of soaking, remove the pessaries from the Cidex OPA andthoroughly rinse the pessaries with tap water. Dry and repackage thepessaries with the date and size of the pessary.For example, sterilizable fittingkits are now available for Ring,Cube, Incontinence Dish, Oval,and Gellhorn pessaries (Atnip &O’Dell, 2012; Bioteque of America,2011). Practice costs associatedwith fitting kits include the originalcost of the kit(s) and theirupkeep. Options for sterilizationafter cleaning include autoclaving,with specifications dependenton the type of autoclave used,or cold sterilization with a product,such as Cidex OPA ® orChloro phenyl ® , followed bythorough rinsing with water(Bioteque of America, 2001). Anexample of a written procedurefor cold sterilization for officeuse is presented in Figure 2.If fitting kits are used, a prescriptionfor the device is typicallyprovided to the potential user,who then obtains the devicethrough a pharmacy or medicalsupply store. In some cases,insurance may cover all or part ofthe cost of the device. Cost comparisonmay demonstrate an economicadvantage to the providerwhen fitting kits are utilized.However, practice decision-makersshould also consider patientsatisfaction, including potentialaggravation of delays in symptomrelief. This may be especiallyproblematic for women whorequire a subsequent change inpessary type or size after a trial ofdaily use.If actual pessaries are stocked,the number of types and sizes tokeep as inventory must be determined.In provider surveys, themost commonly used pessarystyles are variations of the Ringpessary (with and without a supportmembrane, and with andwithout an incontinence knob),and Gellhorn pessaries (Cundiff,Weidner, Visco, Bump, &Addison, 2000; Pott-Grinstein &Newcomer, 2001). The mostcommon sizes of Ring pessary are2 through 5 (whole numbers).Gellhorn pessaries are sized bythe dish diameter in quarter-inchincrements, with common sizesranging from 1.75 to 3.0 inches(CooperSurgical, 2011). Whenordering decisions are beingmade, limiting pessary styles tothose with drainage holes mayoffer an advantage by allowingnormal vaginal discharge to passfrom the vagina, rather than poolingas a potential culture medium.This may decrease infectionrisk but has not been well studied.When a decision is made tolimit the number of in-housestock, unusual sizes can be speciallyordered, or the patient canbe referred to specialty practice. Ifa referral is made, users can beoffered the option of returning tothe original practice for follow-upvisits once a satisfactory pessaryis identified for on-going use.Similarly, small practices maychoose to refer all potential usersfor pessary fitting, with theoption of seeing established pessaryusers for follow-up care only.Insurance reimbursement canbe expected to vary by region ofthe country. In making a businessplan, providers should obtainestimates of typical reimbursementsfor pessary-related visitsand supplies from establishedlocal providers, from local professionalorganizations, or directlyfrom third-party payers. Com -paring this information withanticipated purchase and overheadcosts can inform decisionmaking.While pessary practicemay not be lucrative, it should beseen as an important componentto offering a breadth of women’shealth care services. Taking timeto carefully consider stocking,sterilization, and referral optionsshould help maximize both userand provider satisfaction in termsof cost-effectiveness and timemanagement.Supply, Equipment, and ProceduralConsiderations for <strong>Pessary</strong> PracticeSeveral other practice-plancomponents should be considered(see Table 1). In the absenceof established national standards,pessary care can reasonably takeplace in a variety of practice settingsincluding urogynecology,urology, general gynecology, andprimary care. However, rare complicationscan be life-threatening(Atnip & O’Dell, 2012; O’Dell &Atnip, 2012). Designated pro -viders within any practice shouldhave demonstrated competence140 UROLOGIC NURSING / May-June 2012 / Volume 32 Number 3
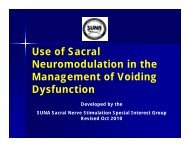
SERIESrelated to knowledge of comfortableand complete pelvic examination,normal and abnormalpelvic anatomy and function, pessaryindications and risks, andmanagement of complications.Written material and educationaldiagrams related to pelvicanatomy, pelvic floor dysfunctions,and specific pessary placementand care enhance patientteaching and should be availableonsite and in take-home format.Whenever possible, all materialshould be available in languagesthat meet the needs of womenseeking outpatient care. A samplepessary handout is presented inFigure 3. When women receiveboth manufacturer and providercare instructions, any discrepanciesshould be ex plained. Otheruseful educational handoutsinclude summaries of relatedtreatment options, such as vaginalestrogens, anticholinergicmedications, urethral bulkingagents, and/or vaginal moisturizersand acidification products.General equipment neededto provide pessary care includesmany items already present in awomen’s health setting, such asvaginal specula, proctologyswabs, straight catheters, lubricants,examination gloves, anditems for assessment of vaginaldischarge (such as pH paper,microscopy, cultures) and urine(such as containers and dipsticks).Cotton-tip applicators orcytology brushes are useful forcleaning pessary drainage holes.Items specific to pessary careinclude selected pessaries and/orfitting kits, written informationand anatomic diagrams, items forvaginal lavage (such as saline,provodine iodine, 10 to 60 ccsyringe), and an autoclave oralternate cleaning and sterilizationplan. A small storage cart onwheels may be useful for transportingequipment to variousexamination rooms (see Figure4). In addition, the office maywish to stock other pessary-relateditems, such as tubes of acidifyinggel (Trimosan TM ).Figure 3.Sample Patient Handout – <strong>Pessary</strong> Care InstructionsWhy do I need a pessary?A pessary is a silicone support device used to support the vagina in womenwho have prolapse (dropping of the pelvic organs) or some kind of urine loss.Pessaries come in many sizes, shapes, and variations. For example, some aredesigned for self-removal, but some are not; some can be worn during sexualintercourse; some will only stay in place if a woman still has strong vaginalmuscles. A pessary can be a comfortable, safe way for many women to controlpelvic problems for a short time or for years.How often does a pessary need to be removed for cleaning?This varies. Some women remove their pessary every night and put it backin the next morning, others remove their pessary occasionally or to have sex,while others only have their pessary removed at an office visit every few months.The best plan for you depends on the type of pessary that works for you and whatyou prefer. Even if you remove and clean your own pessary, you still need to beseen regularly for follow-up care because pessaries can cause painless butserious pressure sores in the vagina.How do I care for my own pessary?If you have a pessary, you can remove it easily and then replace yourself, orwe will work with you in the office to be sure you can:• Remove your pessary.• Wash it with warm water and soap.• Rinse it well.• Reinsert your pessary, often with a special cream we may prescribe.Your pessary is called a ________________________________ pessary, size___________.• To Insert: Wash your hands,lubricate your vagina. Wash/dry yourhands again. Fold the pessary.Insert.• To remove: Wash your hands. Insertone finger into your vagina. Hookyour finger through the finger hole,loop, or above the top of the pessary,and pull out and downwards.What should I expect if I use a pessary?While you use a pessary, you should be seen regularly to be sure thepessary is not causing painless sores in your vagina. Between visits, call if younotice any changes, especially pain, bleeding, increasing odor, or problemspassing your urine or bowels. At each visit, your pessary will be removed andcleaned, your vagina will be examined for irritation, and if everything is okay, yourpessary will be reinserted. Here is our plan for your care.[Insert your plan of care.]Do I need any creams or treatments?We may advise you to use a vaginal estrogen with your pessary. Thesepreparations can be an important way to prevent infection and injury becausethey can increase blood supply and elasticity. This may also make pessaryremoval and insertion more comfortable. Other treatments, such as a gel calledTrimosan ® , can make the vagina more pH-balanced (acidic), and decrease riskof odor or infection. DO NOT use petroleum jelly (Vaseline ® ) or other oil-basedlubricants with your pessary.If you have problems or questions, please call us any time at [insert yourcontact plan].SPECIAL SERIES ON PESSARIESUROLOGIC NURSING / May-June 2012 / Volume 32 Number 3 141
SERIESSPECIAL SERIES ON PESSARIESFigure 4.<strong>Pessary</strong> Storage CartNote: A pessary storage cart may facilitatetransporting pessaries, supplies,and educational materials to variedexamination rooms.An important part of pessaryinitiation is a trial of the pessaryas the woman performs a facsimileof her typical activities, suchas walking, sitting, climbingstairs, bending, and sitting on atoilet to urinate and defecate.Including this type of trial periodat the office-fitting visit is likelyto preempt problems, such as urinaryretention or return urgentvisits for pain or expulsion. Thetrial period in the office area mayincrease non-billable visit time,and patient flow to facilitaterelaxed assessment should becarefully considered before fittingappointments are scheduled.<strong>Pessary</strong> complications aremore common when pessariesare forgotten or neglected (Arias,Ridgeway, & Barber, 2008). Forthis reason, several safe guardsshould be in place. First, a trackingsystem should be developedto insure that women who misspessary return visits are quicklycontacted and rescheduled.Some clinicians advise all wo -men, and in particular, wo menwith memory impairment, towear medical alert bracelets,identifying them as a pessaryuser. Others require a new pessaryuser to sign an informedconsent form acknowledgingunder standing of pessary risksand warning signs, and responsibilitiesduring follow up. Addi -tionally, if pessary providers arenot always available, pessaryusers should be aware of a planof obtaining care at any hour incases of urgent or emergent problems.Ordering PessariesSeveral companies distributepessaries in the U.S., and potentialproviders should check costsof supplies and delivery to theirarea. Table 2 lists a sample of distributorsand their Internet-accessibleservices. Providers can ac -cess several other important servicesfrom pessary distributors ortheir representatives, includingproduct fitting and care advice,and assistance with purchasingand reimbursement information(Artisan Medical, 2011; Biotequeof America, 2011; CooperSurgical,2011; Personalmed, 2012). Pes -sary distribution may changeownership, and providers willneed to reassess their purchasingoptions intermittently.Table 2.Examples of <strong>Pessary</strong> Resources in the United StatesCompany Web Site <strong>Pessary</strong>-Related Products Other Web-Based ServicesArtisan Medical www.artisanmed.com Wide range of pessaries Online orderingBioteque of America www.bioteque.com Bioteque pessaries; Fittingkits for Ring, Oval, Cube,Gellhorn, Incontinence Dish.<strong>Pessary</strong> removersVaginal dilatorsOnline ordering;downloadable pessaryselection chart, patienteducation brochure, productinformationCooperSurgical www.coopersurgical.com Milex pessaries; Fitting kitsfor Ring pessaries; Trimosanacidifying gelPersonalmed www.personalmed.com EvaCare pessaries; vaginalcones, electrical stimulationunitsOnline ordering;downloadable documents,including pessary materialinformation sheet andMagnetic ResonanceImaging recommendationsOnline ordering142 UROLOGIC NURSING / May-June 2012 / Volume 32 Number 3
SERIESBilling and Coding for <strong>Pessary</strong>ReimbursementTable 3.Commonly Used Billing CodesStandards and guidelines forbilling offer providers the opportunityto receive appropriate compensationand continue their work,and they offer payers the securityof assuring that charges reflectactual services provided. Manyprivate third-party payers followregulations developed by theCenters for Medicare & MedicaidServices (CMS). Information forproviders is available at the CMSWeb site (www.cms.gov), with specificeducational material availablefree of charge through the affiliatedMedicare Learning Network (MLN)(www.cms.gov/MLNGenInfo). ForMedicare purposes, both physiciansand advanced practice registerednurses are fee-for-servicebillers. Providers should regularlyreview changes in standards andguidelines as they become availablethrough the CMS Web site.As part of the billing process,providers designate codes to identify1) either the complexity of thevisit or the time spent with thepatient, if that is unusual related tothe expected complexity of thevisit; 2) specific procedures performedduring the visit; and 3)diagnoses demonstrating at leastprimary and possibly secondaryindications for the care provided(CMS, 2011a). Table 3 lists somecommon codes used for pessaryrelatedbilling. Typically, only oneservice can be billed per office day.In certain circumstances, whenseparate services are provided onthe same day, or a patient receivesservices from separate providerson the same day, a codingModifier may be appropriate toidentify this exception (CMS,2011b). Provider documentationin the medical record justifyingcoding selections is essential toretrospective audit of appropriatebilling. Because the billing pro cessmay not always be straightforward,professional organizationsoften offer Web-based assistance tohelp members, and in some cases,non-members, understand regulationsin a specific field. For exam-Type of Code Description CodeUterovaginal prolapse618.3completeCurrent ProceduralTerminology (CPT)Diagnostic CodeUterovaginal prolapse618.2incompleteCystocele (anterior618.01compartment prolapse)Stress urinary incontinence 625.6Urinary retention 788.20Unspecified non-inflammatory 623.9disorder of the vaginaVulvar atrophy 624.1Vaginitis/vulvitis616.10unspecifiedVaginitis, postmenopausal627.3atrophicVaginal stenosis 623.2Vaginal discharge 623.5Procedure Codes <strong>Pessary</strong> fitting and insertion 057160Vaginal irrigation 57150Supplies Non-rubber pessary (silicone) A4562<strong>Pessary</strong>, rubber, any typeA4561Evaluation andManagement (E&M)Modifier Codesple, the American Congress ofObstetricians and Gynecologists(www.acog.org), the AmericanUrological Association (www.auanet.org), and the AmericanUrogynecologic Society (www.augs.org) offer this type of memberNew patient to practice (novisits in past 3 years), codeselection based oncomplexity OR time.Established patient, codeselection based oncomplexity OR time.Same day: Separate serviceand procedure/sameproviderSame day: Separate service/different provider99203 (Detailed OR30 minutes)99204(Comprehensive OR45 minutes)99212 (ProblemfocusedOR 10minutes)99213 (Expandedproblem-focused OR15 minutes)99214 (Detailed OR25 minutes)Modifier-25Modifier-HOservice. Professional developmentrelated to billing and coding is alsooften included at annual professionalmeetings, such as thosesponsored by the Society ofUrologic Nurses and Associates(www.suna.org).SPECIAL SERIES ON PESSARIESUROLOGIC NURSING / May-June 2012 / Volume 32 Number 3 143
SERIESSPECIAL SERIES ON PESSARIESTable 4.Examples of <strong>Pessary</strong> Types and SizesType Size Variations AvailableRing Available: 0 to 13, in wholenumbers (equal to 1 ¾ to 5Ring with or without centralsupport membrane.inches)Ring with incontinence knobCommon: 2 through 5with or without supportmembrane.DonutInflatableDonutAvailable: 2 to 3 ¾ inches, in ¼inch incrementsCommon: 2 to 3Available: 2, 2.25, 2.50, 2.75inchesGellhorn Sized by the dish diameter:Available: 1 ½ to 3 ¾ inches, in¼ inch increments.Common: 1 ¾ to 3 inchesCube Available: Sizes 0 to 7 (1 to 2¼ inches)Common: 1 to 4Marcia is a 66-year-old woman seen for a routine bi-annualgynecology visit by a new provider who is an enrolledMedicare supplier. The purpose of her original visit meets thecriteria for a preventive visit. During a comprehensive interview,she reports feeling something new coming out of her vagina,with increasing pelvic pressure in the afternoon and evening. Acomprehensive physical examination (PE) confirms incompleteuterovaginal prolapse. Marcia is shown anatomical drawings tohelp her understand what is happening, and her options forcare are reviewed. She decides to try a vaginal support pessary,(see Table 4) and is easily fitted with a Ring pessary. Shefinds it very comfortable during a 20-minute pessary trial performinggeneral activities, such as walking in the office hallway.She verbalizes understanding of the importance of regular followup, typical expectations related to wearing a pessary, andwarning signs that would indicate she should call her provider.Marcia leaves with the pessary in place, written informationabout pessary care, and an appointment to return in two weeksfor a review of her satisfaction with the pessary, examination forpessary-related mechanical injury, and instruction related topessary self-removal and reinsertion.The provider documents the findings of the history andPE, reporting that during the 90-minute visit, 30 minutes werespent completing the preventative history and PE; 25 minutesinvolved face-to-face patient education related to pelvic prolapseand treatment options, and 15 minutes were spent fittingthe pessary. The remainder of the 90 minutes, while Marciatested the pessary by walking in the hall and going to the bathroom,was not face-to-face time with the provider, and that timeis not included in the coding documentation.When preparing the bill for this visit, the provider includescodes for a Preventive Visit for a new patient over the age of 65(Code 099387), with related diagnostic codes, such asGynecologic Examination Routine (V72.31) with CervicalRoutine Pap (V76.2); a modifier for Separate Evaluation andManagement and Procedure, Same Day, Same ProviderSilicone Inflato-Donut or latexInflato-BallLong stem or short stemChoose option with drainageholes. Compressibility will varyby manufacturer.Figure 5.Case Example: <strong>Pessary</strong> Billing and CodingFigure 5 describes a caseexample of billing and commoncodes used during a hypotheticalpatient’s pessary care. However,the information in this article canonly serve as an introduction tothis complex topic. Regulationschange, and the ultimate responsibilityfor conforming to regulationsrests with the provider.ConclusionVaginal support pessaries arean important treatment optionfor women who report symptomsrelated to loss of pelvic support.Careful consideration of pessarypractice options combined withknowledgeable billing practicesshould allow providers in a varietyof settings to offer pessary fittingand follow up as an essential,cost-effective component ofwomen’s pelvic health care.(Modifier-25); a Procedure code for <strong>Pessary</strong> Fitting andInsertion (057160); a Supply code for <strong>Pessary</strong>, Non-Rubber(A4562), and the Current Procedural Terminology (CPT) diagnosticcode for uterovaginal prolapse incomplete (618.2).Marcia calls to ask some questions in the next two weeks.Later, she forgets her appointment and has to be called to berescheduled. During that call, the rationale and importance ofregular follow up is re-addressed. The provider does not submita bill for the 25 minutes spent during these two phone interactionsbecause they are not billable, face-to-face patient education.When Marcia returns, she reports de novo stress incontinence,and the decision is made to change the pessary. Thesesymptoms and the refitting are documented, along with thecontent and time spent for patient education. Because a refittingis required, a billing decision must be made based eitheron procedure (such as a pessary fitting) or time spent (such asusing an appropriate Evaluation and Management code).<strong>Pessary</strong> follow-up visits typically range between 15 to 25 minutesdepending on patient status and complexity (099213 or099214). In this case, the refitting was not complex, and theprovider decided not to reuse the pessary fitting proceduralcode. She discarded the used, unsatisfactory pessary, billed forthe new pessary as a supply, and added the CPT code forstress urinary incontinence (625.6) as a secondary code.If Marcia later returns with a problem, additional secondarydiagnostic coding would be added (vaginitis/vulvitis[616.10], atrophic vaginitis [627.3], vaginal discharge [623.5],postmenopausal bleeding [627.1], urine retention [788.20],mechanical complication of genitourinary device [996.39], andurinary tract infection [599.0]). Specific treatments clinically indicatedby the new diagnosis would be included (irrigation of thevagina [057150], endometrial biopsy [058100], insertion of nonindwellingbladder catheter [051701]), with supply codes ifappropriate. Procedures done at routine visits for additionaldiagnoses would continue to be designated with a Modifier-25.144 UROLOGIC NURSING / May-June 2012 / Volume 32 Number 3
SERIESReferencesArias, B.E., Ridgeway, B., & Barber, M.D.(2008). Complications of neglectedvaginal pessaries: Case presentationand literature review. InternationalUrogynecology Journal and PelvicFloor Dysfunction 19(8), 1173-1178.doi:10.1007/s00192-008-0574-2Artisan Medical. (2011). Artisan Medical.Retrieved from http://www.artisanmed.com/index.htmlAtnip, S., & O’Dell, K. (2012). Vaginalsupport pessaries: Indications foruse and fitting strategies. UrologicNursing, 32(3), 114-125.Bioteque of America. (2001). FS 1000<strong>Pessary</strong> Fitting Set. Retrieved fromhttp://pessary.net/pessaries/<strong>Pessary</strong>_Fitting_Set.htmlBioteque or America. (2011). Literaturedownload center. Retrieved fromhttp://www.bioteque.com/downloads/index.phpCenters for Medicaid and MedicareServices (CMS). (2011a). HealthcareCommon Procedure Coding System(HCPCS) overview. Retrieved fromhttp://www.cms.gov/MedHCPCSGenInfoCenters for Medicaid and MedicareServices (CMS). (2011b). Nationalcorrect coding initiative policy manualfor Medicare services. Retrievedfrom http://www.cms.gov/NationalCorrectCodInitEdCopperSurgical. (2011). Products for thepelvic floor: Pessaries. Retrieved fromhttp://www.coopersurgical.com/ourproducts/incontinence/pessaries/Pages/csland.aspx?LC=Pessar%20MainCundiff, G.W., Weidner, A.C., Visco, A.G.,Bump, R.C., & Addison, W.A. (2000).A survey of pessary use by membersof the American UrogynecologicSociety. Obstetrics & Gynecology,95(6), 931-935.Komesu, Y.M., Rogers, R.G., Rode, M.A.,Craig, E.C., Schrader, R.M., Gallegos,K.A., & Villareal, B. (2008). Patientselectedgoal attainment for pessarywearers: What is the clinical relevancy?American Journal of Obstetrics &Gynecology, 198, 577.e1-577.e5. doi:10.1016/j.ajog.2007.12.033O’Dell, K., & Atnip, S. (2012). <strong>Pessary</strong>care: Follow up and management ofcomplications. Urologic Nursing,32(3), 126-137, 145.Personalmed. (2012). Management withEva Care ® flexible silicone pessaries.Retrieved from http://www.personalmed.com/pessaries.phpPott-Grinstein, E., & Newcomer, J.R.(2001). Gynecologists’ patterns ofprescribing pessaries. Journal ofReproductive Medicine, 46(3), 205-208.Additional ReadingAmerican Congress of Obstetricians andGynecologists (ACOG). (2010).Coding and billing for pessaries. Re -trieved from http://www.acog.org/About_ACOG/ACOG_Departments/Coding_and_Nomenclature/Coding_and_Billing_for_PessariesSPECIAL SERIES ON PESSARIESUROLOGIC NURSING / May-June 2012 / Volume 32 Number 3 145