Mind the Gap - MAKO Surgical Corp.
Mind the Gap - MAKO Surgical Corp.
Mind the Gap - MAKO Surgical Corp.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Mind</strong> <strong>the</strong> <strong>Gap</strong> – Achieving aNaturally Balanced andAligned Knee Following UKAwith <strong>the</strong> <strong>MAKO</strong>plasty ®ProcedureMichael Conditt, Ph.D.Director of Clinical Research<strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>.Robert Van Vorhis, Ph.D.Principal Scientist<strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>.
<strong>Mind</strong> <strong>the</strong> <strong>Gap</strong> – Achieving aNaturally Balanced andAligned Knee Following UKAwith <strong>the</strong> <strong>MAKO</strong>plasty ®ProcedureThere are distinct differences in <strong>the</strong>philosophies of post-operative limbalignment between total knee arthroplastyand medial unicompartmentalarthroplasty. The goal of TKA is typicallyto align <strong>the</strong> post-operative knee inneutral, thus loading both compartmentsevenly or in slight valgus. 1-3 It has beengenerally accepted that this is <strong>the</strong> mostimportant variable predicting survival of<strong>the</strong> implant. 4 This long-standing goal ofTKA has actually been questionedrecently, perhaps because <strong>the</strong> normalknee loads <strong>the</strong> medial side more than<strong>the</strong> lateral side. 5Figure 1: Medial compartment osteoarthritis results in narrowing of <strong>the</strong> medial joint space due to <strong>the</strong>loss of articular cartilage.femoral deficitslack medial collateralcollapsed medial compartmentMLtibial deficitWith medial UKA, <strong>the</strong> desired postoperativelimb alignment is still unclear.Overcorrection has been implicated as acause of progression of <strong>the</strong> disease to<strong>the</strong> opposite compartment, 6,7 howeverundercorrection has also been identifiedas leading to accelerated wear of <strong>the</strong>polyethylene. 8 With <strong>the</strong> minimallyinvasive nature of both <strong>the</strong> <strong>MAKO</strong>plasty ®procedure and <strong>the</strong> all polyethylene tibialinlay component, <strong>the</strong> alignment goal ofeach component is to match <strong>the</strong> naturalanatomy, thus simply replacing <strong>the</strong>worn joint surface and restoring <strong>the</strong>mechanical axis to its position before<strong>the</strong> onset of degenerative changes. 9-13<strong>MAKO</strong>plasty ® provides a method fordetermining where this relative positionwas before <strong>the</strong> onset of osteoarthritis.Then, three-dimensional planning of<strong>the</strong> implant position to achieve thisalignment and precise preparation of<strong>the</strong> bones enables achievement of thisalignment post-operatively.A preliminary plan for <strong>the</strong> position andorientation of <strong>the</strong> components is createdfrom a three-dimensional reconstructionof a pre-operative CT scan of <strong>the</strong> patient’sleg and CAD models of <strong>the</strong> implantedcomponents. This preliminary plan isbased primarily on <strong>the</strong> geometry of <strong>the</strong>individual bones. During <strong>the</strong> surgicalprocedure, standard navigation markersare placed in <strong>the</strong> femur and <strong>the</strong> tibia andare also mounted on a robotic arm.A registration procedure consisting ofkinematically determining <strong>the</strong> center ofrotation of <strong>the</strong> hip and digitization ofvarious bony landmarks allows <strong>the</strong> correlationof <strong>the</strong> previously reconstructedmodels of <strong>the</strong> bones along with <strong>the</strong>ircorresponding component plans to <strong>the</strong>current three-dimensional space of <strong>the</strong>operating room. Motions of <strong>the</strong> bonesand <strong>the</strong> robot are continuously monitoredin real time.Once <strong>the</strong> registration has been completed,osteophytes interfering with medialcollateral ligament function are removedand capsular adhesions interfering withknee function are relieved (Figure 1).As two of <strong>the</strong> indications for a UKA area correctable deformity and functioningACL, removal of <strong>the</strong>se impedimentsmakes it possible to achieve correct legkinematics and tissue tension duringpassive manipulation throughout <strong>the</strong> fullrange of motion with an applied valgusFigure 2: Manual application of a valgus stress to <strong>the</strong>knee opens <strong>the</strong> medial compartment and allows <strong>the</strong>planning of <strong>the</strong> placement of <strong>the</strong> components to fill<strong>the</strong> articular gap left by <strong>the</strong> loss of articular cartilage.(force via pelvis)taught medialcollateralopen medialcompartmentexternallyinducedvalgusmoment
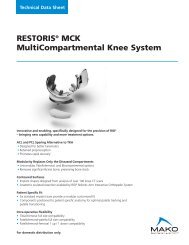
Figure 3: Graph used in planning implant placement at different flexion angles during which <strong>the</strong> desired limb alignment was captured. The graph displaysgap/overlap of <strong>the</strong> femoral and tibial components. Each component can <strong>the</strong>n be fine-tuned in all 6 degrees of freedom, upon which <strong>the</strong> graph is immediatelyupdated. This allows <strong>the</strong> three-dimensional adjustment of implant placement to optimize <strong>the</strong> desired joint laxity throughout flexion.0ºloose4.0<strong>Gap</strong> Between Articular Surfaces (mm)3.02.01.00.0-1.0tight-2.00 45 90ExtensionFlexion90º4 poses captured 4 “gap” values at posesstress (Figure 2). Correct leg kinematicsand soft tissue tension should represent<strong>the</strong> relative positioning of <strong>the</strong> femur and<strong>the</strong> tibia before <strong>the</strong> loss of cartilage. Thecamera system captures <strong>the</strong> positions of<strong>the</strong> femur and <strong>the</strong> tibia during manipulationof <strong>the</strong> knee through a range ofmotion with <strong>the</strong> disease induced varusdeformity corrected with an externallyapplied valgus stress. It should be notedthat applying a pure valgus stressbecomes more difficult with increasingknee flexion as <strong>the</strong>re is tendency forrotation at <strong>the</strong> hip. These capturedthree-dimensional positions represent<strong>the</strong> appropriate spacing within <strong>the</strong> jointwith <strong>the</strong> medial collateral ligamentproperly tensioned. While variability willexist in <strong>the</strong> manual application of <strong>the</strong>valgus moment, <strong>the</strong> high stiffness of <strong>the</strong>MCL attenuates <strong>the</strong> manifestation ofthis variability in <strong>the</strong> medial joint spaceopening provided <strong>the</strong> force is largeenough to create a taught collateral.The planned positions of <strong>the</strong> femoraland tibial components can <strong>the</strong>n befine-tuned such that <strong>the</strong> joint articularsurfaces are placed to fill <strong>the</strong> gap leftby <strong>the</strong> disease process throughout <strong>the</strong>flexion arc (Figure 3). The philosophybeing that after resection and componentimplantation, knee mechanics will beproperly restored throughout <strong>the</strong> rangeof motion.This final planned position <strong>the</strong>n defines<strong>the</strong> volume of bone to be resected by<strong>the</strong> high speed burr attached to <strong>the</strong>robotic arm. While inside <strong>the</strong> volume ofbone to be resected, <strong>the</strong> robotic armoffers no resistance. As <strong>the</strong> burrapproaches <strong>the</strong> boundary, <strong>the</strong> roboticarm resists that motion and keeps <strong>the</strong>burr only within <strong>the</strong> accepted volume.The effectiveness of this process isdifficult to quantify. A surrogatevariable indicative of success is <strong>the</strong>number of soft tissue releases performedand <strong>the</strong> number of times <strong>the</strong>planned insert thickness is not changedintra-operatively. Eighty-nine percent of<strong>MAKO</strong>plasty ® procedures result in <strong>the</strong>use of <strong>the</strong> planned insert thickness*,*Data on file.
<strong>Mind</strong> <strong>the</strong> <strong>Gap</strong> - Achieving a Naturally Balanced and Aligned Knee Following UKA with <strong>the</strong> <strong>MAKO</strong>plasty ® Procedure6mm, which is <strong>the</strong> thinnest possibleinsert. This three-dimensional planningmethod, which is a combination ofpre- and intra-operative planning,empowers <strong>the</strong> robotic arm to effectivelyact as a virtual instrument set thatprecisely assists <strong>the</strong> surgeon to execute<strong>the</strong> plan to create an appropriately,naturally balanced and aligned knee.References1. Insall, J. N.; Binazzi, R.; Soudry, M.; and Mestriner,L. A.: Total knee arthroplasty. ClinicalOrthopaedics And Related Research, (192):13-22, 1985.2. Ritter, M. A.; Faris, P. M.; Keating, E. M.; andMeding, J. B.: Postoperative alignment of totalknee replacement. Its effect on survival. ClinicalOrthopaedics And Related Research, (299):153-6, 1994.3. Hsu, H. P.; Garg, A.; Walker, P. S.; Spector, M.; andEwald, F. C.: Effect of knee component alignmenton tibial load distribution with clinical correlation.Clinical Orthopaedics And Related Research,(248): 135-44, 1989.4. Moreland, J. R.: Mechanisms of failure in totalknee arthroplasty. Clinical Orthopaedics AndRelated Research, (226): 49-64, 1988.5. Parratte, S.; Pagnano, M. W.; Trousdale, R. T.; andBerry, D. J.: The mechanical axis may be <strong>the</strong>wrong target in computer assisted TKA In 75thAnnual Meeting of <strong>the</strong> American Academy ofOrthopaedic Surgeons. Edited, San Francisco, CA,2008.6. Laskin, R. S.: Unicompartmental tibiofemoralresurfacing arthroplasty. The Journal of Bone andJoint Surgery, American, 60(2): 182-5, 1978.7. Scott, R. D.; Cobb, A. G.; McQueary, F. G.; andThornhill, T. S.: Unicompartmental kneearthroplasty. Eight- to 12-year follow-upevaluation with survivorship analysis. ClinicalOrthopaedics And Related Research, (271):96-100, 1991.8. Barrett, W. P., and Scott, R. D.: Revision of failedunicondylar unicompartmental knee arthroplasty.The Journal of Bone and Joint Surgery, American,69(9): 1328-35, 1987.9. Cartier, P., and Deschamps, G.: <strong>Surgical</strong> principlesof unicompartmental knee replacement. InUnicompartmental Knee Arthroplasty. Edited byCartier, P.; Epinette, J. A.; Deschamps, G.; andHernigou, P., Paris, Expansion ScientifiqueFrancaise, 1977.10.Keene, G.; Simpson, D.; and Kalairajah, Y.: Limbalignment in computer-assisted minimally-invasiveunicompartmental knee replacement. The Journalof Bone and Joint Surgery, British, 88(1): 44-8,2006.11.Repicci, J. A.: Mini-invasive knee unicompartmentalarthroplasty: bone-sparing technique.<strong>Surgical</strong> Technology International, 11: 282-6,2003.12.Repicci, J. A., and Eberle, R. W.: Minimallyinvasive surgical technique for unicondylar kneearthroplasty. Journal of <strong>the</strong> Sou<strong>the</strong>rn OrthopaedicAssociation, 8(1): 20-7; discussion 27, 1999.13.Emerson, R. H., Jr.; Head, W. C.; and Peters, P. C.,Jr.: Soft-tissue balance and alignment in medialunicompartmental knee arthroplasty. The Journalof Bone and Joint Surgery, British, 74(6): 807-10,1992.© <strong>MAKO</strong> <strong>Surgical</strong> <strong>Corp</strong>. 203027 r00 09/09 www.makosurgical.com