Axillary Dissection vs No Axillary Dissection in Women With Invasive ...
Axillary Dissection vs No Axillary Dissection in Women With Invasive ...
Axillary Dissection vs No Axillary Dissection in Women With Invasive ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ORIGINAL CONTRIBUTION<strong>Axillary</strong> <strong>Dissection</strong> <strong>vs</strong> <strong>No</strong> <strong>Axillary</strong> <strong>Dissection</strong><strong>in</strong> <strong>Women</strong> <strong>With</strong> <strong>Invasive</strong> Breast Cancerand Sent<strong>in</strong>el <strong>No</strong>de MetastasisA Randomized Cl<strong>in</strong>ical TrialArmando E. Giuliano, MDKelly K. Hunt, MDKarla V. Ballman, PhDPeter D. Beitsch, MDPat W. Whitworth, MDPeter W. Blumencranz, MDA. Marilyn Leitch, MDSukamal Saha, MDL<strong>in</strong>da M. McCall, MSMonica Morrow, MDAXILLARY LYMPH NODE DISSECtion(ALND) has been part ofbreast cancer surgery s<strong>in</strong>ce thedescription of the radical mastectomy.1 ALND reliably identifies nodalmetastases and ma<strong>in</strong>ta<strong>in</strong>s regional control,2,3 but the contribution of localtherapy to breast cancer survival is controversial.4,5 The Early Breast Cancer Trialists’Collaborative Group synthesizedf<strong>in</strong>d<strong>in</strong>gs from 78 randomized controlledtrials, conclud<strong>in</strong>g that local controlof breast cancer was associated withimproved disease-specific survival. 6ALND, as a means for achiev<strong>in</strong>g localdisease control, carries an <strong>in</strong>disputableand often unacceptable risk of complicationssuch as seroma, <strong>in</strong>fection, andlymphedema. 7-9 Sent<strong>in</strong>el lymph nodedissection (SLND) was therefore developedto accurately stage tumordra<strong>in</strong><strong>in</strong>gaxillary nodes with less morbiditythan ALND. 10 SLND alone is theaccepted management for patients whoseFor editorial comment see p 606.Context Sent<strong>in</strong>el lymph node dissection (SLND) accurately identifies nodal metastasisof early breast cancer, but it is not clear whether further nodal dissection affectssurvival.Objective To determ<strong>in</strong>e the effects of complete axillary lymph node dissection (ALND)on survival of patients with sent<strong>in</strong>el lymph node (SLN) metastasis of breast cancer.Design, Sett<strong>in</strong>g, and Patients The American College of Surgeons Oncology GroupZ0011 trial, a phase 3 non<strong>in</strong>feriority trial conducted at 115 sites and enroll<strong>in</strong>g patientsfrom May 1999 to December 2004. Patients were women with cl<strong>in</strong>ical T1-T2 <strong>in</strong>vasivebreast cancer, no palpable adenopathy, and 1 to 2 SLNs conta<strong>in</strong><strong>in</strong>g metastases identifiedby frozen section, touch preparation, or hematoxyl<strong>in</strong>-eos<strong>in</strong> sta<strong>in</strong><strong>in</strong>g on permanentsection. Targeted enrollment was 1900 women with f<strong>in</strong>al analysis after 500 deaths,but the trial closed early because mortality rate was lower than expected.Interventions All patients underwent lumpectomy and tangential whole-breast irradiation.Those with SLN metastases identified by SLND were randomized to undergo ALNDor no further axillary treatment. Those randomized to ALND underwent dissection of 10or more nodes. Systemic therapy was at the discretion of the treat<strong>in</strong>g physician.Ma<strong>in</strong> Outcome Measures Overall survival was the primary end po<strong>in</strong>t, with a non<strong>in</strong>ferioritymarg<strong>in</strong> of a 1-sided hazard ratio of less than 1.3 <strong>in</strong>dicat<strong>in</strong>g that SLND aloneis non<strong>in</strong>ferior to ALND. Disease-free survival was a secondary end po<strong>in</strong>t.Results Cl<strong>in</strong>ical and tumor characteristics were similar between 445 patients randomizedto ALND and 446 randomized to SLND alone. However, the median numberof nodes removed was 17 with ALND and 2 with SLND alone. At a median follow-upof 6.3 years (last follow-up, March 4, 2010), 5-year overall survival was 91.8%(95% confidence <strong>in</strong>terval [CI], 89.1%-94.5%) with ALND and 92.5% (95% CI, 90.0%-95.1%) with SLND alone; 5-year disease-free survival was 82.2% (95% CI, 78.3%-86.3%) with ALND and 83.9% (95% CI, 80.2%-87.9%) with SLND alone. The hazardratio for treatment-related overall survival was 0.79 (90% CI, 0.56-1.11) withoutadjustment and 0.87 (90% CI, 0.62-1.23) after adjust<strong>in</strong>g for age and adjuvant therapy.Conclusion Among patients with limited SLN metastatic breast cancer treated withbreast conservation and systemic therapy, the use of SLND alone compared with ALNDdid not result <strong>in</strong> <strong>in</strong>ferior survival.Trial Registration cl<strong>in</strong>icaltrials.gov Identifier: NCT00003855JAMA. 2011;305(6):569-575Author Affiliations: John Wayne Cancer Institute atSa<strong>in</strong>t John’s Health Center, Santa Monica, California(Dr Giuliano); M. D. Anderson Cancer Center, Houston,Texas (Dr Hunt); Mayo Cl<strong>in</strong>ic Rochester, Rochester,M<strong>in</strong>nesota (Dr Ballman); Dallas Surgical Group,Dallas, Texas (Dr Beitsch); Nashville Breast Center,Nashville, Tennessee (Dr Whitworth); Morton PlantHospital, Clearwater, Florida (Dr Blumencranz); Universityof Texas Southwestern Medical Center, Dallaswww.jama.com(Dr Leitch); McLaren Regional Medical Center, MichiganState University, Fl<strong>in</strong>t (Dr Saha); American Collegeof Surgeons Oncology Group, Durham, <strong>No</strong>rth Carol<strong>in</strong>a(Ms McCall); and Memorial Sloan-Ketter<strong>in</strong>gCancer Center, New York, New York (Dr Morrow).Correspond<strong>in</strong>g Author: Armando E. Giuliano, MD, JohnWayne Cancer Institute at Sa<strong>in</strong>t John’s Health Center,2200 Santa Monica Blvd, Santa Monica, CA 90404(giulianoa@jwci.org).©2011 American Medical Association. All rights reserved. (Repr<strong>in</strong>ted) JAMA, February 9, 2011—Vol 305, <strong>No</strong>. 6 569Downloaded From: http://jama.jamanetwork.com/ on 05/27/2012
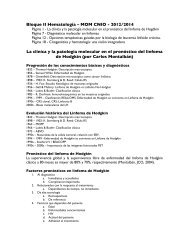
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCERFigure 1. Study Flow445 Randomized to receive ALND420 Received ALND asrandomized25 <strong>With</strong>drew prior to surgery92 Lost to follow-up2 Discont<strong>in</strong>ued <strong>in</strong>tervention1 Refused after randomizationbut prior to surgery1 Consent obta<strong>in</strong>ed afterpatient registered420 Included <strong>in</strong> primary analysis25 Excluded (withdrew prior to surgery)sent<strong>in</strong>el lymph nodes (SLNs) are histologicallyfree of tumor, while ALND rema<strong>in</strong>sthe standard of care for patientswhose SLNs conta<strong>in</strong> metastases. 11Cancer biology is much better understoodnow than it was when ALND was<strong>in</strong>troduced. Biological factors may affectthe predilection of some malignant cellsto selectively <strong>in</strong>vade lymph nodes ratherthan visceral organs, just as certa<strong>in</strong> tumortypes metastasize to certa<strong>in</strong> organsand not others. 12 Recognition of the complexityof tumor biology has changedcancer treatment, with more liberal useof systemic therapy to treat occult cancercells wherever they may be <strong>in</strong> thebody. Consequently, the decision to adm<strong>in</strong>istersystemic therapy is <strong>in</strong>fluencedby a variety of patient- and tumorrelatedfactors, with lymph node tumorstatus <strong>in</strong>fluenc<strong>in</strong>g 13,14 but not necessarilydictat<strong>in</strong>g the use of chemotherapy. 15-18Other factors, such as early cancer detectionby screen<strong>in</strong>g mammography,have led to earlier <strong>in</strong>tervention <strong>in</strong> breastcancer, reduc<strong>in</strong>g the <strong>in</strong>cidence of nodalmetastases and even the number of tumor-<strong>in</strong>volvedlymph nodes. 19These evolv<strong>in</strong>g concepts have called<strong>in</strong>to question the need for ALND. 20,21 Avariety of algorithms have been developedto help cl<strong>in</strong>icians decide which patientswould benefit from ALND. 22-24 Reviewof Surveillance, Epidemiology, andEnd Results data has shown that the useof ALND for SLN metastases has decreased<strong>in</strong> recent years. 25 <strong>No</strong> study has891 Patients randomized446 Randomized to receive SLND alone436 Received SLND aloneas randomized10 <strong>With</strong>drew prior to surgery74 Lost to follow-up3 Discont<strong>in</strong>ued <strong>in</strong>tervention2 Refused after randomizationbut prior to surgery1 Opted for alternative therapy436 Included <strong>in</strong> primary analysis10 Excluded (withdrew prior to surgery)ALND <strong>in</strong>dicates axillary lymph node dissection; SLND, sent<strong>in</strong>el lymph node dissection.conclusively demonstrated a survivalbenefit or detriment for omitt<strong>in</strong>g ALNDwhen metastatic breast cancer is identifiedby SLND. In the late 1990s, theAmerican College of Surgeons OncologyGroup designed and began the multicenterZ0011 trial. The primary aim ofthis study was to determ<strong>in</strong>e the effectsof ALND on overall survival <strong>in</strong> patientswith SLN metastases treated <strong>in</strong> the contemporaryera with lumpectomy, adjuvantsystemic therapy, and tangentialfieldradiation therapy.METHODSPatient CharacteristicsThis multicenter, randomized phase 3trial was registered with the NationalCancer Institute and approved by the <strong>in</strong>stitutionalreview boards of participat<strong>in</strong>gcenters. All patients provided written<strong>in</strong>formed consent. Adult womenwith histologically confirmed <strong>in</strong>vasivebreast carc<strong>in</strong>oma cl<strong>in</strong>ically 5 cm or less,no palpable adenopathy, and an SLNconta<strong>in</strong><strong>in</strong>g metastatic breast cancerdocumented by frozen section, touchpreparation, or hematoxyl<strong>in</strong>-eos<strong>in</strong> sta<strong>in</strong><strong>in</strong>gon permanent section were eligiblefor participation. Patients with metastasesidentified <strong>in</strong>itially or solely with immunohistochemicalsta<strong>in</strong><strong>in</strong>g were <strong>in</strong>eligible.Treatment with lumpectomy tonegative marg<strong>in</strong>s (no tumor at <strong>in</strong>k) wasrequired. <strong>Women</strong> were <strong>in</strong>eligible if theyhad 3 or more positive SLNs, mattednodes, or gross extranodal disease, or ifthey had received neoadjuvant hormonaltherapy or chemotherapy.Study Design and TreatmentBefore randomization, all women underwentSLND and were stratified accord<strong>in</strong>gto age (50 and 50 years), estrogen-receptorstatus, and tumor size(1cm,1cmand2cm,or2cm).Eligible women were randomly assignedto ALND or no further axillaryspecific<strong>in</strong>tervention—specifically, nothird-field nodal irradiation. ALND wasdef<strong>in</strong>ed as an anatomical level I and II dissection<strong>in</strong>clud<strong>in</strong>g at least 10 nodes. Allwomen were to receive whole-breastoppos<strong>in</strong>g tangential-field radiationtherapy. The use of adjuvant systemictherapy was determ<strong>in</strong>ed by the treat<strong>in</strong>gphysician and was not specified <strong>in</strong> theprotocol.Patients most commonly entered thestudy post-SLND follow<strong>in</strong>g identificationof metastases on f<strong>in</strong>al pathology report.However, of the 891 registered patients,287 were registered pre-SLNDand assigned to treatment after <strong>in</strong>traoperativedocumentation of SLN metastases.Patients <strong>in</strong> this group subsequentlyfound to have 3 or more tumor-<strong>in</strong>volvedlymph nodes were <strong>in</strong>cluded <strong>in</strong> the analysis.Patients were assessed for disease recurrenceaccord<strong>in</strong>g to standard cl<strong>in</strong>icalpractice. History and physical exam<strong>in</strong>ationwere performed every 6 months forthe first 36 months and yearly thereafter.Annual mammography was required;other test<strong>in</strong>g was based on symptomsand <strong>in</strong>vestigator preference.Study End Po<strong>in</strong>tsThe primary end po<strong>in</strong>t was overall survival,def<strong>in</strong>ed as the time from randomizationuntil death from any cause. Ashort-term primary end po<strong>in</strong>t was occurrenceof surgical morbidities. Thestudy plan was to report surgical morbiditiesfollow<strong>in</strong>g the completion of accrualand prior to overall survival report<strong>in</strong>gafter receiv<strong>in</strong>g permission fromthe data and safety monitor<strong>in</strong>g committee.These morbidities have beenreported. 10A secondary end po<strong>in</strong>t was diseasefreesurvival, def<strong>in</strong>ed as the time from570 JAMA, February 9, 2011—Vol 305, <strong>No</strong>. 6 (Repr<strong>in</strong>ted) ©2011 American Medical Association. All rights reserved.Downloaded From: http://jama.jamanetwork.com/ on 05/27/2012
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCERrandomization to death or first documentedrecurrence of breast cancer.Breast cancer recurrence was categorizedas locoregional disease (tumor <strong>in</strong>the breast or ipsilateral supraclavicular,subclavicular, <strong>in</strong>ternal mammary,or axillary nodes) or distant metastases.Disease-free survival and its components(locoregional disease and distantmetastases) are reported <strong>in</strong>stead ofthe protocol-specified secondary endpo<strong>in</strong>t (eg, distant disease–free survival)to facilitate comparison withother studies.Statistical AnalysisThe primary end po<strong>in</strong>t was overall survivalas a measure of non<strong>in</strong>feriority ofno further axillary specified <strong>in</strong>terventions(SLND-alone group) comparedwith the ALND group. Based on the literatureat the time of study design, wehypothesized that overall survival was80% at 5 years for optimally treatedwomen with positive nodes. 26-28 Cl<strong>in</strong>icalnon<strong>in</strong>feriority was def<strong>in</strong>ed as theSLND-alone group hav<strong>in</strong>g a 5-year survivalof not less than 75% of that observed<strong>in</strong> the ALND group. <strong>No</strong>n<strong>in</strong>feriorityof the SLND-alone treatment wasalso considered if the hazard ratio (HR)for mortality was less than 1.3 whencompared with ALND. An estimated 500deaths were needed for the study to have90% power to confirm non<strong>in</strong>feriority ofSLND alone compared with ALND, withthe use of a 2-sided 90% confidence <strong>in</strong>terval(CI) for the HR from a Cox regressionmodel. 29 Specifically, if the90% CI for the HR was below 1.3, thiswould <strong>in</strong>dicate that patients undergo<strong>in</strong>gSLND alone do not have an unacceptablyworse overall survival than patientsundergo<strong>in</strong>g SLND plus ALND.The use of a 2-sided 90% CI correspondsto a 1-sided significance level of.05. 30 The enrollment of 1900 patients <strong>in</strong>4yearswitham<strong>in</strong>imumfollow-upperiodof 5 years was <strong>in</strong>itially planned. Fourformal <strong>in</strong>terim analyses and 1 f<strong>in</strong>al analysiswere planned for overall survival, andthe O’Brien-Flemm<strong>in</strong>g -spend<strong>in</strong>g strategywas used to generate stopp<strong>in</strong>gboundaries for each planned analysis.The overall study significance was ma<strong>in</strong>ta<strong>in</strong>edat .05. However, none of theplanned <strong>in</strong>terim analyses were performedbefore the study was closed basedon the recommendation of the data andsafety monitor<strong>in</strong>g committee. Because ofthis, a s<strong>in</strong>gle term<strong>in</strong>al hypothesis test withan of .05 is applied to the data, whichmakes it consistent with the plannedoverall significance level of .05 <strong>in</strong> theorig<strong>in</strong>al study plan.Ineligible patients were reta<strong>in</strong>ed <strong>in</strong>all analyses (ie, both the <strong>in</strong>tent-totreatanalyses and the treatmentreceivedanalyses). Kaplan-Meier survivalcurves for overall survival werecompared by log-rank test. The unadjustedHR (and 90% CI) was calculatedus<strong>in</strong>g a Cox regression analysis,and non<strong>in</strong>feriority P values are reported.As a secondary analysis, knownprognostic factors <strong>in</strong>clud<strong>in</strong>g adjuvanttreatment were <strong>in</strong>cluded <strong>in</strong> the Cox regressionmodel to generate an adjustedHR for overall survival (with a90% CI and non<strong>in</strong>feriority P values).Disease-free survival was analyzed us<strong>in</strong>gKaplan-Meier curves and univariableand multivariable Cox regression analyseswith 95% CIs. The fact that therewere only 94 deaths limited the numberof variables that could be used <strong>in</strong> amultivariable model without affect<strong>in</strong>gmodel stability. We created a basemodel that <strong>in</strong>cluded the treatmentgroup (SLND alone <strong>vs</strong> ALND), age(50 <strong>vs</strong> 50 years), and whether thepatient received adjuvant therapy (yes<strong>vs</strong> no) and added prognostic variablesto this model <strong>in</strong>dividually. Only variablesobta<strong>in</strong>ed on 90% or more of thepatients were <strong>in</strong>cluded <strong>in</strong> the multivariableanalysis. Locoregional recurrencerates were compared with theFisher exact test. Each analysis, otherthan analysis for the primary end po<strong>in</strong>tof overall survival, was performed with2-sided P values, 5% significance, anda 95% CI; all analyses were performedus<strong>in</strong>g SAS release 9.1 (SAS Institute Inc,Cary, <strong>No</strong>rth Carol<strong>in</strong>a).RESULTSPatient CharacteristicsThe first patient was enrolled <strong>in</strong> May1999, and accrual closed <strong>in</strong> DecemberTable 1. Basel<strong>in</strong>e Patient and TumorCharacteristics by Study Group<strong>No</strong>. (%)ALND SLND AloneCharacteristic (n = 420) (n = 436)Age, median (range), y 56 (24-92) 54 (25-90)Miss<strong>in</strong>g 7 10Cl<strong>in</strong>ical T stageT1 284 (67.9) 303 (70.6)T2 134 (32.1) 126 (29.4)Miss<strong>in</strong>g 2 7Tumor size, median 1.7 (0.4-7.0) 1.6 (0.0-5.0)(range), cmMiss<strong>in</strong>g 6 14Receptor statusER/PR 256 (66.8) 270 (68.9)ER/PR− 61 (15.9) 54 (13.8)ER−/PR 3(0.8) 4(1.0)ER−/PR− 63 (16.5) 64 (16.3)Miss<strong>in</strong>g 37 44LVIYes 129 (40.6) 113 (35.2)<strong>No</strong> 189 (59.4) 208 (64.8)Miss<strong>in</strong>g 102 115Modified Bloom-Richardson score1 71(22.0) 81(25.6)2 158(48.9) 148(46.8)3 94(29.1) 87(27.5)Miss<strong>in</strong>g 97 120Tumor typeInfiltrat<strong>in</strong>g ductal 344 (82.7) 356 (84.0)Infiltrat<strong>in</strong>g lobular 27 (6.5) 36 (8.5)Other 45 (10.8) 32 (7.5)Miss<strong>in</strong>g 4 12Lymph nodemetastases0 4(1.2) 29(7.0)1 199(58.0) 295(71.1)2 68(19.8) 76(18.3)3 25(7.3) 11(2.7)4 47(13.7) 4(1.0)Miss<strong>in</strong>g 77 21Abbreviations: ALND, axillary lymph node dissection; ER, estrogenreceptor; LVI, lymphovascular <strong>in</strong>vasion; PR, progesteronereceptor; SLND, sent<strong>in</strong>el lymph node dissection.2004 based on a recommendation of the<strong>in</strong>dependent data and safety monitor<strong>in</strong>gcommittee because of concerns regard<strong>in</strong>gthe extremely low mortalityrate. Even if the trial had accrued thetargeted 1900 patients, it would havetaken more than 20 years of follow-upto observe 500 deaths at the realizedevent rate. At the time of the decisionto term<strong>in</strong>ate the study there had beenno formal analysis compar<strong>in</strong>g the survivalexperience between the 2 groups;the decision was based solely on the ob-©2011 American Medical Association. All rights reserved. (Repr<strong>in</strong>ted) JAMA, February 9, 2011—Vol 305, <strong>No</strong>. 6 571Downloaded From: http://jama.jamanetwork.com/ on 05/27/2012
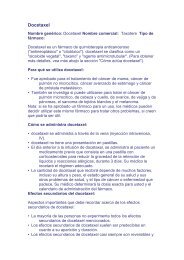
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCERFigure 2. Survival of the ALND Group Compared <strong>With</strong> SLND-Alone GroupSurvival, %1009080706050403020100<strong>No</strong>. at riskALND 420SLND alone 4361408421ALNDSLND alone23984113 4 5Years391403Alive378387Log-rank P = .25313326served mortality rate for pooled datafrom the 2 groups. The date of last follow-upfor this analysis was March 4,2010.Patients were enrolled from 115 <strong>in</strong>stitutions,which <strong>in</strong>cluded affiliates of theCancer Trials Support Unit and the<strong>No</strong>rth Central Cancer Treatment Group.Of 891 patients, 445 were randomly assignedto the ALND group and 446 tothe SLND-alone group (FIGURE 1).Thirty-five patients were excluded afterwithdraw<strong>in</strong>g consent prior to surgery.The 103 <strong>in</strong>eligible patients were<strong>in</strong>cluded <strong>in</strong> the analyses reported here.Because this was a non<strong>in</strong>feriority trial,a more conservative analysis was performedon the treatment-receivedsample (n=813 patients); 32 patients<strong>in</strong> the ALND group did not have ALND,and 11 patients <strong>in</strong> the SLND-alonegroup had ALND. <strong>No</strong> qualitativedifferences were observed betweentreatment-received sample and <strong>in</strong>tentto-treatsample analyses, so only <strong>in</strong>tentto-treatresults are reported. Diseasecharacteristics at basel<strong>in</strong>e were well balancedbetween the 2 groups (TABLE 1).Treatment ResultsThere was an expected differencebetween ALND and SLND-alone treatmentgroups <strong>in</strong> total number of removedlymph nodes and total number oftumor-<strong>in</strong>volved nodes; the median totalnumber of nodes removed was 17 (<strong>in</strong>terquartilerange [IQR], 13-22) <strong>in</strong> theALND group and 2 (IQR, 1-4) <strong>in</strong> theSLND-alone group. 31 The median total6223226714114287474100908070605040302010042043613693952335363310337ALND <strong>in</strong>dicates axillary lymph node dissection; SLND, sent<strong>in</strong>el lymph node dissection.Alive and Disease-Free3 4 5Years286307Log-rank P = .14226231number of nodes with histologicallydemonstrated tumor <strong>in</strong>volvement (<strong>in</strong>clud<strong>in</strong>gSLNs) <strong>in</strong> the ALND group andSLND-alone group was equal (1 [IQR,1-2] for both groups). Hematoxyl<strong>in</strong>eos<strong>in</strong>–sta<strong>in</strong>edtumor deposits no largerthan 2 mm were def<strong>in</strong>ed as micrometastasesand were identified <strong>in</strong> SLNs of137 of 365 patients (37.5%) <strong>in</strong> theALND group compared with 164 of 366(44.8%) <strong>in</strong> the SLND-alone group(P=.05).IntheALNDgroup,97of355patients (27.3%) had additional metastasis<strong>in</strong> lymph nodes removed by ALND,<strong>in</strong>clud<strong>in</strong>g 10% of patients with SLNmicrometastasis who had macroscopically<strong>in</strong>volved non-SLNs removed. Totalnodal <strong>in</strong>volvement is summarized <strong>in</strong>Table 1; 21.0% of patients undergo<strong>in</strong>gALND had 3 or more <strong>in</strong>volved nodescompared with 3.7% undergo<strong>in</strong>g SLNDalone. Four or more <strong>in</strong>volved nodeswere seen <strong>in</strong> 13.7% of patients receiv<strong>in</strong>gALND and 1.0% of those receiv<strong>in</strong>gSLND alone.Adjuvant systemic therapy was deliveredto 403 women (96.0%) <strong>in</strong> theALND group and 423 women (97.0%)<strong>in</strong> the SLND-alone group. 31 <strong>No</strong> differences<strong>in</strong> the proportion of women receiv<strong>in</strong>gendocr<strong>in</strong>e therapy, chemotherapy,or both were observed. Thetype of chemotherapy adm<strong>in</strong>istered wassimilar <strong>in</strong> the 2 groups; anthracycl<strong>in</strong>eandtaxane-based comb<strong>in</strong>ation regimenswere the most common. The majorityof the women (n=605) receivedwhole-breast radiation therapy: 263of 296 (88.9%) <strong>in</strong> the ALND group61521477838183736and 277 of 309 (89.6%) <strong>in</strong> the SLNDalonegroup.Overall SurvivalAt a median follow-up of 6.3 years (IQR,5.2-7.7), there were 94 deaths (SLNDalonegroup, 42; ALND group, 52). Theuse of SLND alone compared with ALNDdid not appear to result <strong>in</strong> statistically<strong>in</strong>ferior survival (FIGURE 2)(P=.008fornon<strong>in</strong>feriority). The unadjusted HRcompar<strong>in</strong>g overall survival between theSLND-alone group and the ALND groupwas 0.79 (90% CI, 0.56-1.10), whichdid not cross the specified boundary of1.3 (FIGURE 3). The 5-year overall survivalrates were 92.5% (95% CI, 90.0%-95.1%) <strong>in</strong> the SLND-alone group and91.8% (95% CI, 89.1%-94.5%) <strong>in</strong> theALND group. This was substantiallygreater than the 80% anticipated at protocoldesign. The HR for overall survivaladjust<strong>in</strong>g for adjuvant therapy(chemotherapy, endocr<strong>in</strong>e therapy,and/or radiation therapy) and age forthe SLND-alone group compared withthe ALND group was 0.87 (90% CI,0.62-1.23). The adjusted HRs compar<strong>in</strong>gthe SLND-alone group with theALND group <strong>in</strong> the other multivariablemodels ranged from 0.86 to 0.92(TABLE 2), all similar to the unadjustedrate of 0.79. An exploratoryanalysis revealed that treatment withALND <strong>vs</strong> SLND alone produced no statisticallysignificant difference <strong>in</strong> outcomeamong patients grouped by receptorstatus of the primary tumor (ER/PR or ER−/PR−).Disease-Free SurvivalDisease-free survival (Figure 2) did notdiffer significantly between treatmentgroups. The 5-year disease-free survivalwas 83.9% (95% CI, 80.2%-87.9%) forthe SLND-alone group and 82.2% (95%CI, 78.3%-86.3%) for the ALND group(P=.14). The unadjusted HR compar<strong>in</strong>gthe SLND-alone group with theALND group was 0.82 (95% CI, 0.58-1.17), and the HR adjusted for adjuvanttreatment and age was 0.88 (95% CI,0.62-1.25) (TABLE 3). The adjusted HRscompar<strong>in</strong>g the SLND-alone group withthe ALND group <strong>in</strong> the other multivari-572 JAMA, February 9, 2011—Vol 305, <strong>No</strong>. 6 (Repr<strong>in</strong>ted) ©2011 American Medical Association. All rights reserved.Downloaded From: http://jama.jamanetwork.com/ on 05/27/2012
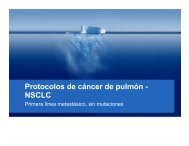
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCERable models ranged from 0.84 to 0.89(Table 3), all similar to the unadjustedrate of 0.82. Locoregional recurrence andits correlates have been previouslyreported. 31 The 5-year rates of local recurrencewere 1.6% (95% CI, 0.7%-3.3%)<strong>in</strong> the SLND-alone group and 3.1% (95%CI, 1.7%-5.2%) <strong>in</strong> the ALND group(P=.11). Locoregional recurrence–freesurvival at 5 years was 96.7% (95% CI,94.7%-98.6%) <strong>in</strong> the SLND-alone groupand 95.7% (95% CI, 93.6%-97.9%) <strong>in</strong> theALND group (P=.28).Surgical MorbiditiesParesthesias, shoulder pa<strong>in</strong>, weakness,lymphedema, and axillary web syndromeare recognized morbidities ofALND. 7-9 As previously reported, 10 therate of wound <strong>in</strong>fections, axillary seromas,and paresthesias among patients <strong>in</strong>the Z0011 trial was higher for the ALNDgroup than for the SLND-alone group(70% <strong>vs</strong> 25%, P.001). Lymphedema <strong>in</strong>the ALND group was significantly morecommon by subjective report (P.001)and also tended to be higher by objectiveassessment of arm circumference.These f<strong>in</strong>d<strong>in</strong>gs are <strong>in</strong> accordance withother randomized comparisons of SLNDwith <strong>vs</strong> without ALND. 32,33COMMENTIn the American College of SurgeonsOncology Group Z0011 randomizedtrial, ALND did not significantly affectoverall or disease-free survival ofpatients with cl<strong>in</strong>ical T1-T2 breast cancerand a positive SLN who were treatedwith lumpectomy, adjuvant systemictherapy, and tangential-field wholebreastradiation therapy. These survivalf<strong>in</strong>d<strong>in</strong>gs are consistent with thoseof the National Surgical Adjuvant Breastand Bowel Project B04 trial, <strong>in</strong> whichwomen with cl<strong>in</strong>ically negative nodeswere randomized to treatment by radicalmastectomy, total mastectomy plusnodal irradiation, or total mastectomywith delayed ALND if nodal recurrencewas observed. 4 Initially and ateach <strong>in</strong>terim analysis for up to 25 yearsof follow-up, no statistically significantsurvival differences were observedbetween any of the groups. For patientstreated <strong>in</strong> the modern era, the relevanceof the B04 study, which <strong>in</strong>cludedpatients with larger tumors undergo<strong>in</strong>gmastectomy without adjuvant systemictherapy, is uncerta<strong>in</strong>, because anaxillary recurrence after SLND <strong>in</strong>patients with a lower risk of death fromdistant disease might negatively affectsurvival. The f<strong>in</strong>d<strong>in</strong>gs from Z0011 documentthe high rate of locoregional controlachieved with modern multimodalitytherapy, even without ALND.In contrast to B04, <strong>in</strong> which about 40%of patients <strong>in</strong> the radical mastectomygroup were node-positive and the samenumber <strong>in</strong> the total mastectomy groupwere assumed to be node-positive and5-year overall survival was only about60%, 100% of patients <strong>in</strong> Z0011 hadnodal <strong>in</strong>volvement; yet the 5-year over-Figure 3. Hazard Ratios Compar<strong>in</strong>g OverallSurvival Between the ALND and SLND-AloneGroups0.5FavorsSLND AloneUnadjustedAdjustedFavorsALND1.0 1.3Hazard Ratio (90% CI)for Overall Survival2.0Blue dashed l<strong>in</strong>e at hazard ratio=1.3 <strong>in</strong>dicates non<strong>in</strong>ferioritymarg<strong>in</strong>; blue-t<strong>in</strong>ted region to the left of hazardratio=1.3 <strong>in</strong>dicates values for which SLND alonewould be considered non<strong>in</strong>ferior to SLND plus ALND.ALND <strong>in</strong>dicates axillary lymph node dissection; CI, confidence<strong>in</strong>terval; SLND, sent<strong>in</strong>el lymph node dissection.Table 2. Adjusted Hazard Ratios for Overall Survival Compar<strong>in</strong>g SLND-Alone <strong>vs</strong> ALND GroupsModel VariablesTreatment group (SLND alone <strong>vs</strong> ALND), age (50 <strong>vs</strong> 50 y),adjuvantly treated (yes <strong>vs</strong> no)Patients<strong>No</strong>.EventsAdjusted HR(90% CI)<strong>No</strong>n<strong>in</strong>feriorityP Value839 92 0.87 (0.62-1.23) .03Variables <strong>in</strong> row 1 primary tumor size (per 1 cm, cont<strong>in</strong>uous) 818 92 0.89 (0.62-1.25) .03Variables <strong>in</strong> row 1 estrogen receptor status (negative <strong>vs</strong> positive) 778 87 0.92 (0.64-1.30) .05Variables <strong>in</strong> row 1 modified Bloom-Richardson score (1 <strong>vs</strong> 2 <strong>vs</strong> 3) 839 92 0.86 (0.61-1.21) .02Variables <strong>in</strong> row 1 tumor type (ductal <strong>vs</strong> lobular <strong>vs</strong> other) 839 92 0.88 (0.63-1.25) .03Abbreviations: ALND, axillary lymph node dissection; CI, confidence <strong>in</strong>terval; HR, hazard ratio; SLND, sent<strong>in</strong>el lymph node dissection.Table 3. Adjusted Hazard Ratios for Disease-Free Survival Compar<strong>in</strong>g SLND-Alone <strong>vs</strong> ALND GroupsModel VariablesTreatment group (SLND alone <strong>vs</strong> ALND), age (50 <strong>vs</strong> 50 y),adjuvantly treated (yes <strong>vs</strong> no)Patients<strong>No</strong>.EventsAdjusted HR(95% CI) P Value839 127 0.88 (0.62-1.25) .47Variables <strong>in</strong> row 1 primary tumor size (per 1 cm, cont<strong>in</strong>uous) 818 125 0.86 (0.60-1.22) .40Variables <strong>in</strong> row 1 estrogen receptor status (negative <strong>vs</strong> positive) 778 117 0.84 (0.58-1.20) .33Variables <strong>in</strong> row 1 modified Bloom-Richardson score (1 <strong>vs</strong> 2 <strong>vs</strong> 3) 839 127 0.87 (0.61-1.23) .43Variables <strong>in</strong> row 1 tumor type (ductal <strong>vs</strong> lobular <strong>vs</strong> other) 839 127 0.89 (0.62-1.27) .52Abbreviations: ALND, axillary lymph node dissection; CI, confidence <strong>in</strong>terval; HR, hazard ratio; SLND, sent<strong>in</strong>el lymph node dissection.©2011 American Medical Association. All rights reserved. (Repr<strong>in</strong>ted) JAMA, February 9, 2011—Vol 305, <strong>No</strong>. 6 573Downloaded From: http://jama.jamanetwork.com/ on 05/27/2012
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCERall survival was more than 90%. Furthermore,a 19% rate of axillary first failurewas observed <strong>in</strong> B04, 4 whereas the axillarynodal recurrence rate was only 0.9%<strong>in</strong> the SLND-alone group <strong>in</strong> Z0011. 31 Theexcellent local and distant outcomes <strong>in</strong>this study highlight the effects of multiplechanges <strong>in</strong> breast cancer managementdur<strong>in</strong>g the <strong>in</strong>terval between the 2studies. These changes, which <strong>in</strong>cludeimproved imag<strong>in</strong>g, more detailed pathologicalevaluation, improved plann<strong>in</strong>g ofsurgical and radiation approaches, andmore effective systemic therapy, emphasizethe need for ongo<strong>in</strong>g reevaluationof “standard” local therapy.The well-documented morbidityfrom ALND has led other <strong>in</strong>vestigatorsto explore alternative methods ofaxillary treatment <strong>in</strong> patients with cl<strong>in</strong>icallynegative nodes, <strong>in</strong>clud<strong>in</strong>g radiation,systemic therapy, and axillaryobservation. These have consistentlydemonstrated low axillary failure rates,with no significant differences <strong>in</strong> survival.34,35 The International Breast CancerStudy Group trial of ALND <strong>vs</strong> observationis noteworthy because more thanhalf of the patients did not receive breastor axillary radiotherapy. In women 60years and older receiv<strong>in</strong>g adjuvanttamoxifen but no axillary treatment, therate of axillary recurrence was only 3%,and overall survival was 73% at a medianfollow-up of 6.6 years. 36The low rates of locoregional recurrenceat 5 years and the nearly identicaloverall and disease-free survival betweentreatment groups <strong>in</strong> Z0011would suggest that differences <strong>in</strong> survivalbetween study groups are unlikelyto emerge with longer followup,because ALND would only affectsurvival by virtue of improved locoregionalcontrol. In the Early Breast CancerTrialists’ Collaborative Group overview,statistically significant survivaldifferences between treatments at 15years were seen only when differences<strong>in</strong> locoregional recurrence betweentreatments were greater than 10% at 5years. 6 <strong>Axillary</strong> recurrence is usually anearly event, occurr<strong>in</strong>g at a median of14.8 months <strong>in</strong> B04; <strong>in</strong> that trial, only7 of 68 axillary recurrences occurredmore than 5 years after study entry. 4Greco et al 37 reported that median timeto axillary recurrence was 30.6 monthsfor 401 patients who underwent breastconserv<strong>in</strong>gprocedures and radiationtherapy with no axillary surgery. Recentreports of long-term follow-up <strong>in</strong>randomized trials confirm these f<strong>in</strong>d<strong>in</strong>gs.38,39 Because the total locoregionalrecurrence rate <strong>in</strong> the Z0011SLND-alone group at 5 years is only2.5% compared with 3.6% <strong>in</strong> the ALNDgroup, it is unlikely that further follow-upwould result <strong>in</strong> enough additionalrecurrences to generate a cl<strong>in</strong>icallymean<strong>in</strong>gful survival differencebetween groups. The absolute difference<strong>in</strong> 5-year overall survival betweenthe treatment groups <strong>in</strong> Z0011is 0.7%, numerically favor<strong>in</strong>g the SLNDalonegroup. The HR for overall survivalcompar<strong>in</strong>g the SLND-alone groupwith the ALND group was 0.79 (90%CI, 0.56-1.10). The worst HR (1.10) isless than 1.3, which was hypothesizedas the <strong>in</strong>feriority marg<strong>in</strong> threshold. Inessence, this means that the 5-year overallsurvival for the SLND-alone groupmight be as low as 90.3% if the true5-year overall survival for the ALNDgroup was 91.8% and the HR as highas 1.10. Most importantly, there is nosuggestion that rates of locoregional recurrence,the mechanism by whichvariations <strong>in</strong> local therapy result <strong>in</strong> survivaldifferences, differ between groupsto the extent needed to produce survivaldifferences or are likely to do so<strong>in</strong> the future. Taken together, this suggeststhat contemporary women maysusta<strong>in</strong> the morbidity of ALND withoutany mean<strong>in</strong>gful improvement <strong>in</strong>survival rates. Limitations of the study,such as failure to achieve target accrualand possible randomization imbalancefavor<strong>in</strong>g the SLND-alone group,must be considered. However, even <strong>in</strong>high-risk women (ER−/PR−) <strong>in</strong> Z0011,prelim<strong>in</strong>ary analysis suggests no effectof elim<strong>in</strong>ation of ALND on survival.Despite limitations of the Z0011 trial,its f<strong>in</strong>d<strong>in</strong>gs could have important implicationsfor cl<strong>in</strong>ical practice. Exam<strong>in</strong>ationof the regional nodes with SLND canidentify hematoxyl<strong>in</strong>-eos<strong>in</strong>–detected metastasesthat would <strong>in</strong>dicate a higher riskfor systemic disease and the need for systemictherapy to reduce that risk. Resultsfrom Z0011 <strong>in</strong>dicate that womenwith a positive SLN and cl<strong>in</strong>ical T1-T2tumors undergo<strong>in</strong>g lumpectomy with radiationtherapy followed by systemictherapy do not benefit from the additionof ALND <strong>in</strong> terms of local control,disease-free survival, or overall survival.The only additional <strong>in</strong>formationga<strong>in</strong>ed from ALND is the number ofnodes conta<strong>in</strong><strong>in</strong>g metastases. This prognostic<strong>in</strong>formation is unlikely to changesystemic therapy decisions and is obta<strong>in</strong>edat the cost of a significant <strong>in</strong>crease<strong>in</strong> morbidity. 10 The only rationalefor ALND <strong>in</strong> these patients wouldbe if the f<strong>in</strong>d<strong>in</strong>g of additional nodal metastaseswould result <strong>in</strong> changes <strong>in</strong> systemictherapy. Because current guidel<strong>in</strong>esdo not support differences <strong>in</strong>adjuvant systemic therapy based on thenumber of positive lymph nodes, except<strong>in</strong> some uncommon select subgroups,40 ALND does not appear to bewarranted <strong>in</strong> this patient population.The Z0011 trial did not <strong>in</strong>clude patientsundergo<strong>in</strong>g mastectomy, thoseundergo<strong>in</strong>g lumpectomy without radiotherapy,those treated with partialbreastirradiation, those receiv<strong>in</strong>g neoadjuvanttherapy, and those receiv<strong>in</strong>gwhole-breast irradiation <strong>in</strong> the proneposition, <strong>in</strong> which the low axilla is nottreated. In those patients, ALND rema<strong>in</strong>sstandard practice when SLNDidentifies a positive SLN. However,ALND may no longer be justified forwomen who have cl<strong>in</strong>ical T1-T2 breastcancer and hematoxyl<strong>in</strong>-eos<strong>in</strong>–detected metastasis <strong>in</strong> the SLN and whoare treated with breast-conserv<strong>in</strong>g surgery,whole-breast irradiation, and adjuvantsystemic therapy. Implementationof this practice change wouldimprove cl<strong>in</strong>ical outcomes <strong>in</strong> thousandsof women each year by reduc<strong>in</strong>gthe complications associated withALND and improv<strong>in</strong>g quality of lifewith no dim<strong>in</strong>ution <strong>in</strong> survival.Author Contributions: Dr Giuliano had full access toall of the data <strong>in</strong> the study and takes responsibility forthe <strong>in</strong>tegrity of the data and the accuracy of the dataanalysis.Study concept and design: Giuliano.574 JAMA, February 9, 2011—Vol 305, <strong>No</strong>. 6 (Repr<strong>in</strong>ted) ©2011 American Medical Association. All rights reserved.Downloaded From: http://jama.jamanetwork.com/ on 05/27/2012
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCERAcquisition of data: Giuliano, Beitsch, Whitworth,Blumencranz, Leitch, Saha, Morrow.Analysis and <strong>in</strong>terpretation of data: Giuliano, Hunt,Ballman, Whitworth, Leitch, McCall, Morrow.Draft<strong>in</strong>g of the manuscript: Giuliano, Ballman, Beitsch,Whitworth, Morrow.Critical revision of the manuscript for important<strong>in</strong>tellectual content: Giuliano, Hunt, Ballman, Beitsch,Whitworth, Blumencranz, Leitch, Saha, McCall,Morrow.Statistical analysis: Ballman, McCall.Adm<strong>in</strong>istrative, technical, or material support: Giuliano,Hunt, Whitworth, Leitch, Saha.Study supervision: Giuliano, Whitworth.Conflict of Interest Disclosures: All authors have completedand submitted the ICMJE Form for Disclosureof Potential Conflicts of Interest and none were reported.Fund<strong>in</strong>g/Support: This study was supported by NationalCancer Institute grant U10 CA 76001 to theAmerican College of Surgeons Oncology Group(ACOSOG).Role of the Sponsor: The National Cancer Institute hadno role <strong>in</strong> the design and conduct of the study; thecollection, analysis, and <strong>in</strong>terpretation of the data; orthe preparation, review, or approval of the manuscript.Additional Contributions: We thank the ACOSOGstaff, <strong>in</strong> particular the leadership of Heidi Nelson, MD(Mayo Cl<strong>in</strong>ic, Rochester, M<strong>in</strong>nesota), David Ota, MD(Duke University, Durham, <strong>No</strong>rth Carol<strong>in</strong>a), and SamuelA. Wells Jr, MD (National Cancer Institute, Bethesda,Maryland). All 3 of these <strong>in</strong>dividuals contributed tostudy design, manuscript review, or both; none receivedcompensation for their contributions. We alsothank all of the <strong>in</strong>vestigators and their site researchteams. Lastly, we wish to thank the brave patients withbreast cancer who participated <strong>in</strong> this study and theircaregivers.REFERENCES1. Halsted WS. The results of radical operations forthe cure of carc<strong>in</strong>oma of the breast. Ann Surg.1907;46(1):1-19.2. Fisher B, Wolmark N, Bauer M, Redmond C,Gebhardt M. The accuracy of cl<strong>in</strong>ical nodal stag<strong>in</strong>g andof limited axillary dissection as a determ<strong>in</strong>ant of histologicnodal status <strong>in</strong> carc<strong>in</strong>oma of the breast. SurgGynecol Obstet. 1981;152(6):765-772.3. Graversen HP, Blichert-Toft M, Andersen JA, ZedelerK. Breast cancer: risk of axillary recurrence <strong>in</strong> nodenegativepatients follow<strong>in</strong>g partial dissection of theaxilla. Eur J Surg Oncol. 1988;14(5):407-412.4. Fisher B, Jeong JH, Anderson S, Bryant J, FisherER, Wolmark N. Twenty-five-year follow-up of a randomizedtrial compar<strong>in</strong>g radical mastectomy, total mastectomy,and total mastectomy followed by irradiation.NEnglJMed.2002;347(8):567-575.5. Orr RK. The impact of prophylactic axillary nodedissection on breast cancer survival—a Bayesianmeta-analysis. Ann Surg Oncol. 1999;6(1):109-116.6. Clarke M, Coll<strong>in</strong>s R, Darby S, et al; Early Breast CancerTrialists’ Collaborative Group (EBCTCG). Effects ofradiotherapy and of differences <strong>in</strong> the extent of surgeryfor early breast cancer on local recurrence and15-year survival: an overview of the randomised trials.Lancet. 2005;366(9503):2087-2106.7. Yeoh EK, Denham JW, Davies SA, Spittle MF. Primarybreast cancer: complications of axillarymanagement. Acta Radiol Oncol. 1986;25(2):105-108.8. Lotze MT, Duncan MA, Gerber LH, Wolter<strong>in</strong>g EA,Rosenberg SA. Early versus delayed shouldermotion follow<strong>in</strong>g axillary dissection: a randomizedprospective study. Ann Surg. 1981;193(3):288-295.9. Ivens D, Hoe AL, Podd TJ, Hamilton CR, Taylor I,Royle GT. Assessment of morbidity from completeaxillary dissection. Br J Cancer. 1992;66(1):136-138.10. Lucci A, McCall LM, Beitsch PD, et al; AmericanCollege of Surgeons Oncology Group. Surgical complicationsassociated with sent<strong>in</strong>el lymph node dissection(SLND) plus axillary lymph node dissection comparedwith SLND alone <strong>in</strong> the American College ofSurgeons Oncology Group trial Z0011. JCl<strong>in</strong>Oncol.2007;25(24):3657-3663.11. Lyman GH, Giuliano AE, Somerfield MR, et al;American Society of Cl<strong>in</strong>ical Oncology. American Societyof Cl<strong>in</strong>ical Oncology guidel<strong>in</strong>e recommendationsfor sent<strong>in</strong>el lymph node biopsy <strong>in</strong> early-stagebreast cancer. JCl<strong>in</strong>Oncol.2005;23(30):7703-7720.12. Fidler IJ. The pathogenesis of cancer metastasis:the “seed and soil” hypothesis revisited. Nat RevCancer. 2003;3(6):453-458.13. Abrams JS. Adjuvant therapy for breast cancer—results from the USA consensus conference. BreastCancer. 2001;8(4):298-304.14. Goldhirsch A, Glick JH, Gelber RD, Senn HJ. Meet<strong>in</strong>ghighlights: International Consensus Panel on theTreatment of Primary Breast Cancer. JNatlCancerInst.1998;90(21):1601-1608.15. Sørlie T, Perou CM, Tibshirani R, et al. Gene expressionpatterns of breast carc<strong>in</strong>omas dist<strong>in</strong>guish tumorsubclasses with cl<strong>in</strong>ical implications. Proc Natl AcadSci U S A. 2001;98(19):10869-10874.16. van de Vijver MJ, He YD, van’t Veer LJ, et al. Agene-expression signature as a predictor of survival<strong>in</strong> breast cancer. NEnglJMed.2002;347(25):1999-2009.17. Alba<strong>in</strong> KS, Barlow WE, Shak S, et al; Breast CancerIntergroup of <strong>No</strong>rth America. Prognostic and predictivevalue of the 21-gene recurrence score assay<strong>in</strong> postmenopausal women with node-positive, oestrogen-receptor-positivebreast cancer on chemotherapy:a retrospective analysis of a randomised trial.Lancet Oncol. 2010;11(1):55-65.18. Paik S, Tang G, Shak S, et al. Gene expression andbenefit of chemotherapy <strong>in</strong> women with nodenegative,estrogen receptor-positive breast cancer.JCl<strong>in</strong>Oncol.2006;24(23):3726-3734.19. Swedish Organised Service Screen<strong>in</strong>g EvaluationGroup. Effect of mammographic service screen<strong>in</strong>g onstage at presentation of breast cancers <strong>in</strong> Sweden.Cancer. 2007;109(11):2205-2212.20. Fisher B, Montague E, Redmond C, et al. Comparisonof radical mastectomy with alternativetreatments for primary breast cancer: a first reportof results from a prospective randomized cl<strong>in</strong>icaltrial. Cancer. 1977;39(6)(suppl):2827-2839.21. Rutgers EJ. Sent<strong>in</strong>el node biopsy: <strong>in</strong>terpretationand management of patients with immunohistochemistry-positivesent<strong>in</strong>el nodes and those withmicrometastases. JCl<strong>in</strong>Oncol.2008;26(5):698-702.22. van la Parra RF, Ernst MF, Bevilacqua JL, et al. Validationof a nomogram to predict the risk of nonsent<strong>in</strong>ellymph node metastases <strong>in</strong> breast cancer patientswith a positive sent<strong>in</strong>el node biopsy: validationof the MSKCC breast nomogram. Ann Surg Oncol.2009;16(5):1128-1135.23. Amanti C, Lombardi A, Maggi S, et al. Is completeaxillary dissection necessary for all patients withpositive f<strong>in</strong>d<strong>in</strong>gs on sent<strong>in</strong>el lymph node biopsy? validationof a breast cancer nomogram for predict<strong>in</strong>g thelikelihood of a non-sent<strong>in</strong>el lymph node. Tumori.2009;95(2):153-155.24. Coutant C, Olivier C, Lambaudie E, et al. Comparisonof models to predict nonsent<strong>in</strong>el lymph nodestatus <strong>in</strong> breast cancer patients with metastatic sent<strong>in</strong>ellymph nodes: a prospective multicenter study.JCl<strong>in</strong>Oncol.2009;27(17):2800-2808.25. Rescigno J, Zampell JC, Axelrod D. Patterns of axillarysurgical care for breast cancer <strong>in</strong> the era of sent<strong>in</strong>ellymph node biopsy. Ann Surg Oncol. 2009;16(3):687-696.26. Fisher B, Redmond C, Poisson R, et al. Eightyearresults of a randomized cl<strong>in</strong>ical trial compar<strong>in</strong>gtotal mastectomy and lumpectomy with or withoutirradiation <strong>in</strong> the treatment of breast cancer. NEnglJMed. 1989;320(13):822-828.27. Early Breast Cancer Trialists’ Collaborative Group.Systemic treatment of early breast cancer by hormonal,cytotoxic, or immune therapy: 133 randomisedtrials <strong>in</strong>volv<strong>in</strong>g 31,000 recurrences and 24,000deaths among 75,000 women. Lancet. 1992;339(8785):71-85.28. Early Breast Cancer Trialists’ Collaborative Group.Systemic treatment of early breast cancer by hormonal,cytotoxic, or immune therapy: 133 randomisedtrials <strong>in</strong>volv<strong>in</strong>g 31,000 recurrences and 24,000deaths among 75,000 women. Lancet. 1992;339(8784):1-15.29. Rub<strong>in</strong>ste<strong>in</strong> LV, Gail MH, Santner TJ. Plann<strong>in</strong>g theduration of a comparative cl<strong>in</strong>ical trial with loss to follow-upand a period of cont<strong>in</strong>ued observation.JChronicDis.1981;34(9-10):469-479.30. Kaji AH, Lewis RJ. Are we look<strong>in</strong>g for superiority,equivalence, or non<strong>in</strong>feriority? ask<strong>in</strong>g the rightquestion and answer<strong>in</strong>g it correctly. Ann Emerg Med.2010;55(5):408-411.31. Giuliano AE, McCall L, Beitsch P, et al. Locoregionalrecurrence after sent<strong>in</strong>el lymph node dissectionwith or without axillary dissection <strong>in</strong> patients withsent<strong>in</strong>el lymph node metastases: the American Collegeof Surgeons Oncology Group Z0011 randomizedtrial. Ann Surg. 2010;252(3):426-433.32. Fleissig A, Fallowfield LJ, Langridge CI, et al. Postoperativearm morbidity and quality of life: results ofthe ALMANAC randomised trial compar<strong>in</strong>g sent<strong>in</strong>elnode biopsy with standard axillary treatment <strong>in</strong> themanagement of patients with early breast cancer.Breast Cancer Res Treat. 2006;95(3):279-293.33. Veronesi U, Paganelli G, Viale G, et al. A randomizedcomparison of sent<strong>in</strong>el-node biopsy with rout<strong>in</strong>eaxillary dissection <strong>in</strong> breast cancer. NEnglJMed.2003;349(6):546-553.34. Veronesi U, Orecchia R, Zurrida S, et al. Avoid<strong>in</strong>gaxillary dissection <strong>in</strong> breast cancer surgery: a randomizedtrial to assess the role of axillary radiotherapy.Ann Oncol. 2005;16(3):383-388.35. Martelli G, Boracchi P, De Palo M, et al. A randomizedtrial compar<strong>in</strong>g axillary dissection to no axillarydissection <strong>in</strong> older patients with T1N0 breast cancer:results after 5 years of follow-up. Ann Surg.2005;242(1):1-9.36. Rudenstam CM, Zahrieh D, Forbes JF, et al; InternationalBreast Cancer Study Group. Randomizedtrial compar<strong>in</strong>g axillary clearance versus no axillaryclearance <strong>in</strong> older patients with breast cancer: first resultsof International Breast Cancer Study Group Trial10-93. JCl<strong>in</strong>Oncol.2006;24(3):337-344.37. Greco M, Agresti R, Casc<strong>in</strong>elli N, et al. Breast cancerpatients treated without axillary surgery: cl<strong>in</strong>icalimplications and biologic analysis. Ann Surg. 2000;232(1):1-7.38. Martelli G, Miceli R, Daidone MG, et al. <strong>Axillary</strong>dissection versus no axillary dissection <strong>in</strong> elderly patientswith breast cancer and no palpable axillary nodes:results after 15 years of follow-up [published onl<strong>in</strong>eahead of pr<strong>in</strong>t July 23, 2010]. Ann Surg Oncol.2010.doi:10.1245/s10434-010-1217-7.39. Veronesi U, Viale G, Paganelli G, et al. Sent<strong>in</strong>ellymph node biopsy <strong>in</strong> breast cancer: ten-year resultsof a randomized controlled study. Ann Surg. 2010;251(4):595-600.40. Goldhirsch A, Ingle JN, Gelber RD, Coates AS,Thürlimann B, Senn HJ; Panel Members. Thresholdsfor therapies: highlights of the St Gallen InternationalExpert Consensus on the primary therapy of early breastcancer 2009. Ann Oncol. 2009;20(8):1319-1329.©2011 American Medical Association. All rights reserved. (Repr<strong>in</strong>ted) JAMA, February 9, 2011—Vol 305, <strong>No</strong>. 6 575Downloaded From: http://jama.jamanetwork.com/ on 05/27/2012