Care home pain assessment chart
Care home pain assessment chart Care home pain assessment chart
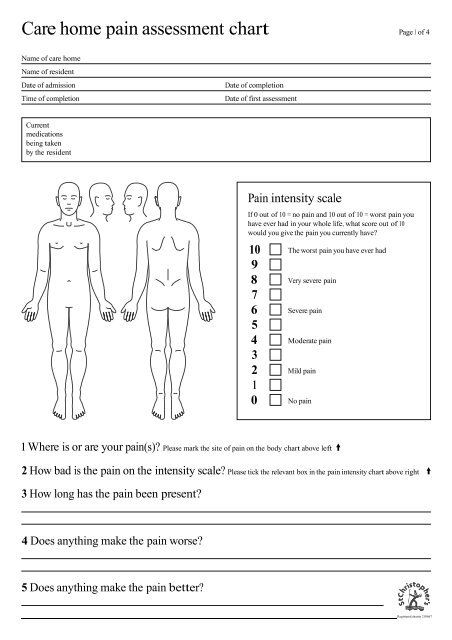
Care home pain assessment chart Page 1 of 4Name of care homeName of residentDate of admissionTime of completionDate of completionDate of first assessmentCurrentmedicationsbeing takenby the residentPain intensity scaleIf 0 out of 10 = no pain and 10 out of 10 = worst pain youhave ever had in your whole life, what score out of 10would you give the pain you currently have?10 The worst pain you have ever had98 Very severe pain76 Severe pain54 Moderate pain32 Mild pain10 No pain1 Where is or are your pain(s)? Please mark the site of pain on the body chart above left2 How bad is the pain on the intensity scale? Please tick the relevant box in the pain intensity chart above right3 How long has the pain been present?4 Does anything make the pain worse?5 Does anything make the pain better?Registered charity 210667
- Page 2 and 3: Page 2 of 4PLEASE USE THE FOLLOW
- Page 4: Pain assessment CONTINUED Page 4 of
<strong>Care</strong> <strong>home</strong> <strong>pain</strong> <strong>assessment</strong> <strong>chart</strong> Page 1 of 4Name of care <strong>home</strong>Name of residentDate of admissionTime of completionDate of completionDate of first <strong>assessment</strong>Currentmedicationsbeing takenby the residentPain intensity scaleIf 0 out of 10 = no <strong>pain</strong> and 10 out of 10 = worst <strong>pain</strong> youhave ever had in your whole life, what score out of 10would you give the <strong>pain</strong> you currently have?10 The worst <strong>pain</strong> you have ever had98 Very severe <strong>pain</strong>76 Severe <strong>pain</strong>54 Moderate <strong>pain</strong>32 Mild <strong>pain</strong>10 No <strong>pain</strong>1 Where is or are your <strong>pain</strong>(s)? Please mark the site of <strong>pain</strong> on the body <strong>chart</strong> above left2 How bad is the <strong>pain</strong> on the intensity scale? Please tick the relevant box in the <strong>pain</strong> intensity <strong>chart</strong> above right3 How long has the <strong>pain</strong> been present?4 Does anything make the <strong>pain</strong> worse?5 Does anything make the <strong>pain</strong> better?Registered charity 210667
Page 2 of 4PLEASE USE THE FOLLOWING ASSESSMENT CHART WHEN A PERSON IS UNABLE TO ACCURATELY DESCRIBE THEIR PAIN Pain Assessment in Advanced Dementia (PAINAD) Scale Items 0 1 2 ScoreBreathingindependentof vocalizationNormalOccasional labored breathing.Short period ofhyperventilation.Noisy labored breathing.Long period ofhyperventilation. Cheyne-Stokes respirations.NegativevocalizationNoneOccasional moan or groan.Low-level speech with anegative or disapprovingquality.Repeated troubled callingout. Loud moaning orgroaning. Crying.FacialexpressionSmiling orinexpressiveSad. Frightened. Frown.Facial grimacing.Body language Relaxed Tense. Distressed pacing.Fidgeting.Rigid. Fists clenched.Knees pulled up. Pulling orpushing away. Striking out.ConsolabilityNo need toconsoleDistracted or reassured byvoice or touch.Unable to console, distractor reassure.Total****Total scores range from 0 to 10 (based on a scale of 0 to 2 for five items), with a higher scoreindicating more severe <strong>pain</strong> (0="no <strong>pain</strong>" to 10="severe <strong>pain</strong>").NBOnce you have ‘scored’ the <strong>pain</strong> make sure you document the necessarymanagement on the next page
Pain <strong>assessment</strong> Page 3 of 4Name of residentCurrentmedicationsbeing takenby the residentRegularity of <strong>assessment</strong> DAILY (10am medicine round) WEEKLY (10am medicine round)PAIN INTENSITY QUESTION If 0 out of 10 = no <strong>pain</strong> and 10 out of 10 = worst <strong>pain</strong> you haveever had in your whole life, what score out of 10 would you give the <strong>pain</strong> you currently have?Date Time PainintensityPAINADscoreAction takenTimebowelslastopenedSignatureandreviewdate/timeOutcome
Pain <strong>assessment</strong> CONTINUED Page 4 of 4PAIN INTENSITY QUESTION If 0 out of 10 = no <strong>pain</strong> and 10 out of 10 = worst <strong>pain</strong> you haveever had in your whole life, what score out of 10 would you give the <strong>pain</strong> you currently have?Date Time PainintensityPAINADscoreAction takenTimebowelslastopenedSignatureandreviewdate/timeOutcome


