Total Hip Replacement - UPMC Beacon Hospital
Total Hip Replacement - UPMC Beacon Hospital
Total Hip Replacement - UPMC Beacon Hospital

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
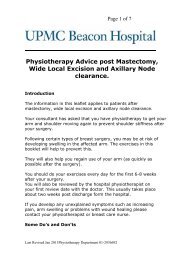
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>4What is a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>?A total hip replacement (THR)is designed to replace a hipjoint that has been damagedby arthritis.The hip is a ball and socketjoint formed by the headof the femur or thigh bone,sitting into the acetabulumor socket in the side of thepelvis. Normally the surfacesare covered by a smoothSocket(acetabulum)Ball(femoralhead)SmoothcartilageThighbone(femur)substance known as articular cartilage or gristle. Dueto arthritis, part or all of this cartilage may wear away,exposing the underlying bone, thus causing roughening ofthe joint surfaces, stiffness and painful movement. A limpwill usually develop and the leg may become shorter andalso thinner due to muscle wasting.A THR replaces the worn head of the femur with a metalball on a stem, which is inserted into the centre of thefemur. A THR also re-lines the socket (acetabulum) with acup made of special plastic or metal.A THR is principally designed to relieve pain and restorejoint movement. It will also aim to correct the shorteningeffect of arthritis. It is important to note that it is notalways possible to make both legs equal in length.What can I expect from an artificial hip?Pain should no longer be a concern – that is the majorbenefit of surgery. You will usually notice the benefitalmost immediately after the operation, although you willof course have pain from the surgery to start with. Youshould have greater mobility and a better quality of life.But it is important to remember that an artificial hip is notas good as a natural hip. It does have some limitations,which are summarised later in this booklet.Preparing for Admission ChecklistSmoking: It is advisable to give up smoking, or at leastto reduce the number of cigarettes you smoke a day, assmoking interferes with wound healing. It also impairsbone growth and repair and will delay or even preventhealing of the joint after surgery.Clothing: Loose comfortable clothing isadvised eg. long shorts, tracksuit bottomsor loose three-quarter length trousers.Back on shoeFootwear: Slip-on shoes with a low heeland a rear counter (back) are recommended. Elastic shoelaces can turn your laced shoes into slip-on shoes.5
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>Cardinal RulesIn order to avoid dislocating your new hip, you must notstress the joint (for the next three months post surgeryor until your surgeon says otherwise) in the extremes ofits motions. This can be done if you keep in mind thefollowing precautions:RIGHTRIGHTRIGHTWRONGWRONGWRONGAvoid bendingpast 90 degreesAvoid twistingyour leg in or outAvoid crossingyour legsPhysiotherapyThe aims of physiotherapy are:• To restore independence by being able to walk byyourself with a walking aid and be able to use stairs.• To regain movement, strength and control around thehip.• To encourage a gradual return to normal activities suchas work and all your usual hobbies.The physiotherapist will help to get you moving freely andadvise you on exercises to strengthen your muscles.ExercisesBefore being allowed to get out of bed for the first time, itis important to do the following exercises. These exerciseswill aid recovery by promoting muscle healing and byhelping to develop strong muscles around the new hip.The benefits of these exercises are as follows:• Minimise the risk of blood clot formation.• Strengthen muscles and keep joints mobile.• Prepared the operated leg for improved walkingtechnique.1011
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>The ExercisesYou should ensure that you have had adequate painmedication prior to seeing the physiotherapist –please discuss your pain with the nursing staff.The physiotherapist will teach you hip exercises postsurgerythat are to be practised whilst lying and standing tobuild up the musculature around the hip joint and ensurethat the affected joints do not become stiff post-surgery.These exercises should be performed within a comfortablerange and should not lead to excessive pain or discomfort.Perform the exercises on the following pages 15 timeseach, three times daily.Bed Exercises1Ankle Pumps• With your legs straight, bend yourankles up and down, towards andaway from your face.• Repeat 15 times• Continue this exercise until you arefully recovered and all ankle andlower-leg swelling has subsided.23Quadriceps Contraction• With your leg straight out in front of you, tightenthe muscles at the front of your thigh, pushingthe back of your knee down into the bed.• The result should be straightening of the knee.• Hold the contraction for 5 seconds.• Repeat 15 times.Gluteal Contraction• Lie on your back with your legs straight and incontact with the bed.• Tighten buttocks.• Hold the contraction for 5 seconds.• Repeat 15 times.1213
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>8 Active Extension in Standing• Step your operated leg backwards slowly.• Try to keep your back andknee straight – hold for 2seconds.• Return your foot to startposition.• Repeat 15 times.9 Active Flexion in Standing• Lift your operated leg in front of you slowly.• Remember not to bring yourknee higher than the level ofyour hip.• Try to keep your back straight.Return your foot to the floor.• Repeat 15 times.It is important to follow your physiotherapist’s instructionscarefully and to only perform the movements taught toyou.WalkingIn most cases, after an uncomplicated first hipreplacement (primary total hip replacement) you will beencouraged, when using crutches for support, to put yourfull weight through the operated leg.Your consultant will advise you when you can reduce yoursupport to one crutch or progress to a stick in the oppositehand.If you have had a complicated primary total hipreplacement or a revision total hip replacement, you willbe instructed to reduce the amount of weight bearingon your leg. In such a case you will be given specificinstructions on how to proceed.Walking Pattern with Crutches:1) Stand in the middle of your crutches.2) Place crutches in front of you. They should be acomfortable arm’s length away3) Push down on the hand grips. Step forward to thecrutches with your operated (weaker) leg.1617
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>4) Step past the crutches with your unoperated (stronger)leg.5) Repeat the same sequence.Strong footWeak footCrutchPositionUsing Chairs and StairsSitting and getting in and out of chairsYou must sit in a firm high chair with arms – you will betaught to do so safely by your physiotherapist.Sitting down• The back of your legs must touch the chair before sitting.• Leave the crutches/frame aside or held in one hand.• Reach both hands back to feel the arm of the chair.• As you sit down, in the early post-operative days slideyour operated leg forward straight out in front of youand sit into the chair. As time progresses, you will not berequired to slide your leg out in front to sit down.• To move back in the chair, slide your bottom back.Getting out of a chair• In the early post-operative days ensure your operatedleg is straight out in front of you. As time progresses,you may stand up as normal.• Move out to the edge of the seat.• Position your walking aid correctly.• Push down on the arms of the chair with your hands andlean on your unoperated leg to stand up.• Do not lean too far forward.• Straighten up and grip your walking aid.Chair: Choose an upright chair with a firm seat andarmrest. Ensure the seat allows your hips to stay higherthan your knees. Sit up straight or lean backwards.Toilets: As most toilets may be too low, you will require araised toilet seat. There will be a raised toilet seat in yourhospital room. Please do not use a commode during yourhospital stay as the seat is too low for your new hip. Avoidstraight-backchair18arm rest19
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>20twisting or bending on the toilet. Keep toilet paper within easyreach or take some before you sit down. Turn your whole bodyaround to flush the toilet.Stairs TechniqueGoingupstairsGoingdownstairsGoing upstairs• Maintain crutches/walking stick on the step below.• Lead with the unoperated (good) leg up onto the step above.• Take your weight onto the unoperated leg by pushing oncrutches/walking stick and banister.• Follow with the crutch/walking stick onto the samestep.Going downstairs• Put crutch/walking stick down onto the step below.• Follow with the operated leg.• Take weight onto the operated leg using the crutchesand banister for support.• Follow with the unoperated leg onto the same step.Hint: The good leg goes up the stairs first and bad leggoes down the stairs first.Rehabilitation Goals<strong>Hip</strong> <strong>Replacement</strong> – Goals of CareThe goals on the following pages have been developed toassist you in understanding your patient journey and alsoto outline your physiotherapy goals, as a patient in <strong>UPMC</strong><strong>Beacon</strong> <strong>Hospital</strong>. Your goals are divided into two areas,Nursing and Physiotherapy, and these start right after yoursurgery so you have some goals that remain the samefrom day one, with new goals added each day.21
<strong>Hip</strong> <strong>Replacement</strong> Goals of CareNursing GoalsNursing GoalsYour Physiotherapy Goals22Day ofProcedureDay OneYou will:• receive adequate pain relief• be started on intravenous (IV) antibiotics. These will be continued until dayone and then stopped unless you are told otherwise.• depending on the time of day you return from theatre, you will be givensomething light to eat and drink• may have an x-ray of your new joint completed on this day or day one• commence medications to prevent clots from occurring on this day or onday one• have the wound dressing checked to ensure it is intact• have an abduction pillow placed between your legs at all times when youare resting in bed.Nursing GoalsYou will:• receive adequate pain relief• be started on medications to preventclots and be given IV antibiotics• have bloods taken to check your ironlevels after surgery• have a wash and get dressed withassistance• have ice packs applied to your hip aminimum of three times per day• be encouraged to drink plenty off luids• have the wound dressing checked toensure it is intact• have an abduction pillow placedbetween your legs at all times when youare resting on the bed.Your Physiotherapy Goals• Complete hip exercisesunder the supervision of thephysiotherapist• Get out of bed with the helpof the physiotherapist• Walk a short distance with aframe• Sit out for a short period oftime - maximum of 1.5 hours• Understand cardinal rulesafter hip replacement surgery• Participate in a secondphysiotherapy treatmentsession of exercises andwalking practice.Day TwoDayThreeDayFourYou will:• receive adequate pain relief• be given medications to prevent clots• have your wound dressing checked toensure it is intact• have a wash and get dressed withassistance• have ice packs applied to your hip threetimes per day• ensure the abduction pillow present at alltimes when you are resting on the bed• mobilise with an appropriate aid (Zimmerframe or crutches) under the supervisionof the nurse or healthcare assistant.You will:• receive adequate pain relief• be given medications to prevent clots• be checked by your nurse to ensure yourbowels have returned to normal function• have your wound checked to ensure it isclean and dressing intact• have resumed a normal diet• have your Discharge Plan reviewed byyour nurse• ensure the abduction pillow present at alltimes when you are resting on the bed• be encouraged to mobilise withappropriate aid.You will:• receive adequate pain relief• be given medications to prevent clots• be checked by your nurse to ensure yourbowels have returned to normal function• have your wound checked to ensure it isclean and dressing intact• have your Discharge Plan reviewedby your nurse and implement anyarrangements• be encouraged to mobilise.• Walk outside of your patientroom with a frame• Complete exercises withphysiotherapist• Complete exerciseindependently throughoutthe day• Sit out for a longer period oftime• Progress to walking with twoelbow crutches if able.• Walk longer distancesoutside of your patient roomwith elbow crutches• Learn how to climb stairswith the physiotherapist• Complete exerciseindependently 3 timesthroughout the day• Sit out during the day.• Walk safely andindependently• Independent and safe onstairs using elbow crutches• Independent in completionof your exercise programme• Understand the importanceof rehabilitation and followup outpatient physiotherapy• Ensure you have thenecessary equipment foryour rehabilitation.23
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>24Occupational TherapyThe occupational therapist’s role is to assess a patient’shome circumstances, looking at the physical environmentand assisting patients in maintaining independence witheveryday activities. If necessary, adaptive equipment canbe prescribed as well as advice on alternative methodsof performing everyday tasks while adhering to your hipprecautions, ensuring safety with your new hip joint.DressingComfortable, loose clothing is best. Do not bend from thehips to pick up objects from the floor. A‘helping-hand’ (long handled reacher)will be issued to you from the ward toassist with this.Gather whatever items you need andkeep them within close reach. Sit onthe edge of the bed or a high chair.Dress your operated leg first using the‘helping-hand’ and shoe horn to assistwith getting shoes/slippers on and off.Be careful not to bend forward or liftyour knees above your hip. To put on adress or skirt, slip this over your head.A sock aid can assist with getting your socks on and offwhile avoiding bending at the hip.When undressing, remove your trousers or underwear fromyour non-operated side first.WashingThe safest method of washing after your hip replacementis sitting at the wash basin on a suitable high chair orperching stool. Or you can sit on the edge of your bed andhave someone bring you a basin of water to be placeddirectly in front of you. Use the long handled aids to washand dry your feet or ask for assistance.Showering/BathingA shower usually has a small step in and care should betaken getting in and out. A shower chair, non-slip mattand grab rail will maximise your safety if you choose touse the shower.We would advise that no bath transfers are completedas the hip position can be compromised with too muchflexion occurring. Sitting while washing at a sink orusing a family member’s shower are also useful methodsof bathing. If a bath transfer must be completed thanassistance of family member/carers, as well as the useof assistive equipment would be required. The website25
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>26www.assistireland.ie is a useful resource for informationand local suppliers of assistive equipment for showering/bathing. If you require more specific advice in relation tobathing the Occupational Therapist can assist you.Kitchen ActivityYou are likely to require help from your family and friendswith shopping, meal preparation and cleaning tasks. Youmade need to reorganise your kitchen so that all items/objects are placed at waist level and within easy reach. Aperching stool can be used in the kitchen for basic snackand drink prep at the work top.General Safety Advice for HomePlease be aware of the hazards in your home as this willmake your recovery easier and safer.• Move electrical cords, phone lines and ensure clearpathways.• Store items within easy reach, specifically in the kitchenand bathroom areas. You will not be able to bend downto lower cupboards.• Remove rugs including bath mats and entrance mats.• Be careful with pets and children.• Be aware of water spills, slippery floors and always thinkbefore you move.• Pace yourself and take your time.General RecommendationsSleepingWhile in hospital some patients find it harder to sleepfor various reasons, e.g. different bed and environment. Ifyou find that you are having this problem please let thenursing staff know as you may require something to helpyou sleep. You will have to sleep on your back for at least6 weeks until reviewed by your consultant.NauseaSome of the medications you may be prescribed cancause nausea. Please inform the nursing staff if you feelsick or are getting sick. Your medications may need tobe changed/adjusted and the nursing staff can also get amedication prescribed to help relieve this nausea.Pain MedicationOn discharge from hospital, you will be prescribed somemedications. At least one of the medications will be forpain. Plan to take your pain medication 30 minutes beforeyour exercises. Preventing pain is easier than chasing pain.If pain control continues to be a problem, contact yourGeneral Practitioner.27
Guidelines for Patients Having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>Nutritionyour hospital stay.Leg SwellingSwelling can occur for 6 -12 weeks post surgery or longer,and can also affect the ankle and foot.BruisingBruising can affect the entire operated limb and may bepresent for a few weeks after the surgery.Driving28Aim to follow a well balanced diet which includesprotein, fats and carbohydrates. It is important to be wellnourished to promote wound healing, so eat well and donot attempt to lose weight at this time.The following nutrients are particularly important topromote wound healing:• Protein – found in meat, fish, eggs, milk, cheese,yoghurt, beans and pulses.• Vitamin A – found in liver, fortified milk, carrots,turnips, and leafy green vegetables.• Vitamin C – found in citrus fruits, potatoes and leafygreen vegetables.• Iron – found in liver, red meat and leafy greenvegetables.• Zinc – found in fortified breakfast cereals, red meat andleafy green vegetables.If you are on a special diet or have any queries, pleasediscuss with your doctor, nurse or dietician.Bowel CareA high fibre diet is recommended after surgery. You mayalso be prescribed laxatives (i.e. Lactalose, Senokot) duringYour consultant will tell you whenyou are allowed to drive again afteryour operation. In order to be safedriving a motor vehicle, you must bein control of the pedals effectively.It is recommended that you notdrive a motor vehicle until youhave complete control over yourleg. This does not normally occur until at least 6 weeksafter your surgery. When you do become capable ofhandling a motor vehicle, it is recommended to completea trial period in an empty car park to accustom yourselfto your new hip. Please check with your motor insurerprior to your return to driving. There may be additionalrequirements or restrictions to follow after your surgery.pillow29
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>30Car TransfersWhen travelling in the car, you should sit in the frontpassenger seat. It can be difficult getting in and out of alow car seat so please ensure you are following your hipprecautions. It is important that you avoid long journeysif possible.Your family or carer should bring a cushion or pillowto place on the passenger seat, raising the height andensuring your hips are kept above your knees, keepingthe seat reclined back as far as possible.When getting into the car, lead with your bottom. Standwith your back to the car; lower yourself keeping youroperated leg straight in front of you. Slide back on toseat and let your driver assist with your legs, keepingboth legs together and your knees lower then your hips.Please ensure you are not twisting.When getting out of the car, lift your legs out of the carfirst with assistance from your driver. Slide towards theedge of the seat and stand up keeping your operated legstretched out in front of you.TravelProlonged periods of sitting on airlines may predisposeto leg swelling and deep venous thrombosis, and it isrecommended to avoid this until 6 weeks after yoursurgery. If you must travel, wear your stockings and keepyour leg elevated as much as possible.StockingsYour consultant may wish for you to go home withelasticated stockings. These can be an important partof preventing the development of deep vein thrombosis(blood clots in the legs). It is recommended to wear thesefor 6 weeks after surgery.AntibioticsFollowing hip replacement surgery there can be a greaterrisk of developing an infection in the hip with someprocedures. Antibiotics to prevent the development ofan infection in the hip should be taken when havinga bladder catheter inserted, urinary surgery (e.g.prostatectomy) or when having infected teeth removed.Always tell your dentist that you have had a total hipreplacement.ActivitiesDuring the first 6 weeks after your surgery, it isrecommended limiting your activities to walking with thesupport. Sexual activity may be resumed at 4-6 weeks,when you are physically and mentally ready and whenyou have a clear understanding of the precautions to befollowed to protect the new joint.31
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>32We recommend that you refrain from more strenuousactivities such as golf and social tennis for a period of 3months.Discharge InstructionsAssuming no complications arise after your operation, andonce your physiotherapist considers you independentlymobile, you will be discharged from hospital. This isusually about day four or day five of your stay. Somepeople go straight home, others require some time in aconvalescent home. When you leave the hospital youwill be given an appointment to see your consultant,usually around 6 weeks after the operation. This is for aroutine check-up which will make sure you are progressingsatisfactorily and x-rays may be taken. It is important tostill bring your old x-rays with you at this time. Subsequentappointments may be at 6 months, 1 year, or 2 years aftersurgery.You will be advised to attend outpatient Physiotherapywithin two to three weeks of discharge. You can eitherattend a private physiotherapist in the hospital or aphysiotherapist more local to your home. If you wouldprefer to exercise in a group setting, <strong>UPMC</strong> <strong>Beacon</strong><strong>Hospital</strong> provides weekly group exercise classes for totalhip replacement patients. Your physiotherapist will provideyou with the details of these classes. You will need tocontinue your physiotherapy for 2-3 months after yoursurgery. Your physiotherapists will advice you after yoursurgery regarding your requirements.Wound CareYou will leave the hospital with a simple surgical wound.Before leaving the hospital your dressing will be changedand the wound site checked. Keep the wound dressingclean and dry for 72 hours. You may then remove thedressing after showering and apply a fresh dressing.Please check with your nurse prior to discharge regardingyour consultant’s specific wound care instructions, andinstructions regarding removal of clips or stitches.Infection may occur despite your very best efforts. If any ofthe symptoms below occur then you will need to see yourGP or liaise with the Centre for Orthopaedics for advice andpossibly antibiotics.Signs of InfectionIf you develop any of the following signs of infection, itis important to report them to your doctor. The signs ofinfection include:• Redness around the wound site• Increased pain in the wound33
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>• Swelling around the wound• Heat at the wound site• Discharge of fluid – may be green or yellow• Odour or smell from the wound• Feeling of being generally unwell• Fever or temperatureMost people will have sutures (stitches) that will need tobe removed approximately 10-14 days after surgery. Thismay be done by the GP, Dressing Clinic, consultant or inthe convalescence centre.Individual Patient NotesConsultant Name:Date of Surgery:Weight Bearing Status:Walking Device:Date for Removal of Sutures (Stitches):Other Recommendations:Make sure you receive a copy of the Patient Wound CareDischarge Instructions prior to your discharge.34ConclusionWe hope that you have found this booklet useful and thatit has helped to relieve some of your fears and anxietiesregarding your surgery.During your hospital stay, your medical team will beavailable to discuss anything mentioned in this booklet orto answer any other queries you may have.We look forward to meeting you soon.35
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>Exercise Diary Following <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong> SurgeryDay Post Operation: Day 1 Day 2 Day 3 Day 4 Day 5Time of Day: Morning Afternoon Evening Morning Afternoon Evening Morning Afternoon Evening Morning Afternoon Evening Morning Afternoon EveningTarget Volume(Repetitions x Sets)1. Ankle Pumps2. QuadricepsContraction3. Gluteal Contraction4. Inner RangeQuadriceps5. Active <strong>Hip</strong> & KneeFlexion6. Active Abduction7. Active Abduction inStanding8. Active Extension inStanding9. Active Flexion inStanding36Instructions: The exercise programme will begin the first day afteryour surgery and the physiotherapist will teach you the exercisesthe first time you perform them. Following this you should recordthe number of repetitions of each exercise that you complete inthe boxes in the table above. The aim is to perform three exercisesets per day (morning, afternoon and evening).37
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>38AppendixPotential Complications of <strong>Hip</strong> <strong>Replacement</strong> SurgeryIncidence: THE MAJORITY OF PATIENTS WHO UNDERGO HIPREPLACEMENT SURGERY HAVE A PLEASANT EXPERIENCE WITHOUTANY COMPLICATIONS. OF ALL PATIENTS WHO UNDERGO TOTALHIP REPLACEMENTS MORE THAN 96% HAVE NO COMPLICATIONS.THE FOLLOWING IS A COMPREHENSIVE LIST OF ALL PROBLEMSTHAT COULD POTENTIALLY OCCUR. FOR INFORMED CONSENT IT ISIMPORTANT THAT YOU KNOW OF THESE PROBLEMS BUT PLEASEBE REASSURED THAT THE VAST MAJORITY OF PATIENTS SUFFER NOCOMPLICATIONS.PainThe hip area will be sore after the operation. If I am in pain, Iunderstand that it is important to tell staff so that medications canbe given. Pain will improve with time. Rarely, pain will be a longterm problem but may be due to altered leg length or any othercomplications listed, or sometimes, for no obvious reason.BleedingThis is usually small and can be stopped during the operation.However patients with large amounts of blood loss may need ablood transfusion or iron tablets. Sometimes a blood clot may formor a large bruise may be noticed at the wound site, which maybecome painful and require surgery to remove it.Deep Vein Thrombosis (DVT)A DVT is a blood clot in the vein. This may present as red, painfuland swollen legs (usually). The risks of a DVT are greater afterany surgery and especially bone surgery. Although not a problemthemselves, a DVT can pass in the blood stream and be depositedin the lungs (a pulmonary embolism/PE). This is a very seriouscondition, which affects your breathing. Your consultant willprescribe medication to limit the risk of a DVT forming. Starting towalk and mobilising after surgery is one of the best ways to preventclots from forming.Discrepancy in Leg LengthWith arthritis, your leg may have shortened. If you have bilateralarthritis both legs may be shorter than they once were. The aim ofjoint replacement surgery is to correct the deformity and restore thenormal length. After a total hip replacement the leg will feel longerdue to the swelling in the joint (functional lengthening) and it maytake up to 3 months for this to resolve. Occasionally it is necessaryto lengthen a leg by a few millimetres to achieve stability andprevent dislocation. This rarely requires a further operation or shoeimplants to correct the difference.Dislocation of <strong>Hip</strong>If this occurs the joint can usually be put back into place without theneed for surgery; however you may need an anaesthetic or sedationto relax your muscles. Sometimes this is not possible, and anoperation is required, followed by the application of a hip brace or,if the hip keeps dislocating, a revision operation may be necessary.The patient can help prevent dislocation by strictly adhering tothe guidelines governing sitting, bending and sleeping. These areoutlined in this booklet.Intra-operative/Post-operative FractureDuring and post the surgery there is a possibility that bonemay fracture. If this occurs the fracture will be treated but maytemporarily alter the amount of weight that can be put on theaffected leg after surgery. This complication can occur after ahip replacement if the bone is weak, especially in the first twomonths after surgery. Sometimes it is caused by a fall or stumble.39
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>40Periprosthetic femoral fracture causes thigh pain with weightbearing and may cause shortening and rotation of the limb.Loosening/Wear of the ProsthesisModern operating techniques and new implants mean that mosthip replacements last over 15 years. In some cases this can besignificantly less. Although wearing down of the bearing surfacemay occur, it is usually minimal. Wear may contribute to looseningand may require corrective surgery if it is excessive. The reasonis often unknown. Implants can wear with overuse. There is stilla debate as to which material is the strongest. The reason forloosening is also unknown. Sometimes it is secondary to infection.Loosening of the prosthesis (total joint replacement) causes painand, if the loosening is significant, a second joint replacementmay be needed or performed. This operation is significantly morecomplicated than the original joint replacement.InfectionAntibiotics are given just before and after the operation and theprocedure will be performed in an operating theatre with sterileequipment. Despite this, infection may still occur. The wound sitemay become red, hot and painful. There may also be a discharge offluid or pus. This is usually treated with antibiotics and an operationto wash out the joint may be necessary. In rare cases, the implantsmay be removed and replaced at a later date. The infection cansometimes lead to sepsis (blood infection) and strong antibioticsmay be required.Late InfectionSpread of infection from another part of the body to a jointreplacement can occur, sometimes years after the operation. Toprevent such infections, persons with a joint replacement aregenerally given antibiotics with extensive dental procedures, urinarytract infections or surgery as well as before other types of surgery.If an infection occurs anywhere in the body it must be treatedpromptly with antibiotics.Heterotropic OssificationThere is a small risk of developing ossification or calcification in themuscle tissue around the hip after surgery. In the majority of cases,this involves small islands of bone that do not cause any functionalrestriction and are only noticeable on x-rays. Rarely, in less than 1%of cases there may be more extensive ossification that may causestiffness and pain. This can be corrected by surgical removal butonly after 12 months or more have passed since the surgery.Vascular Injury/DamageThere are several blood vessels that are located near the hip joint.In rare cases injury to the vessels may occur during surgery and aredealt with during the operation by repairing the vessel. In extremelyrare cases, this could result in loss of limb or life.Nerve Injury/DamageThere are several nerves located near the hip joint. In rare cases,these may be injured during surgery due to direct damage fromsurgical instruments, or indirect damage due to stretching as thehip joint is manipulated (a neuropraxia). Most injuries are temporaryand may resolve with no permanent damage. In rare cases, thenerve injury may be permanent. The nerve most at risk is the sciaticnerve that runs in the buttock just behind the hip joint. If thisnerve is damaged during surgery, upon returning to the ward thepatient may complain of altered sensation in the foot or, in moresevere cases, inability to move their foot (foot drop). Fortunately,the majority of these neuropraxias resolve over a period of time(sometimes months). In a very small minority the damage may bepermanent, resulting in loss or heightened sensation and decreased41
Guidelines for Patients having a <strong>Total</strong> <strong>Hip</strong> <strong>Replacement</strong>motor (muscle) function to the leg.Blood/Pulmonary Embolism (PE)A PE is a consequence of a DVT (Deep Vein Thrombosis). It is ablood clot that breaks away and can travel to the lungs and canmake breathing difficult. A PE can be treated but can also be fatal.Stroke (CVA)/Sudden DeathAlthough these complications can occur during any surgery theyare extremely rare following joint replacements.Notes:4243
<strong>UPMC</strong> <strong>Beacon</strong> Centre for Orthopaedics<strong>UPMC</strong> <strong>Beacon</strong> <strong>Hospital</strong>SandyfordDublin 18Tel: 01 293 7575Email: orthoclinic@beaconhospital.iewww.orthopaedics.ie<strong>UPMC</strong> <strong>Beacon</strong> Physiotherapy DepartmentTel: 01 293 6692Email: physiotherapy@beaconhospital.iewww.beaconhospital.ieScan with your smartphoneto visitour websiteto downloadour free appVersion 2