© 2006 - The Charles H. Tweed International Foundation
© 2006 - The Charles H. Tweed International Foundation
© 2006 - The Charles H. Tweed International Foundation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
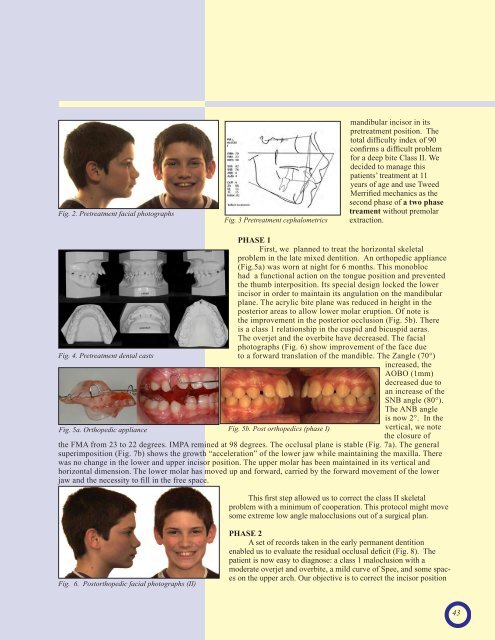
Fig. 2. Pretreatment facial photographsFig. 3 Pretreatment cephalometricsmandibular incisor in itspretreatment position. <strong>The</strong>total difficulty index of 90confirms a difficult problemfor a deep bite Class II. Wedecided to manage thispatients’ treatment at 11years of age and use <strong>Tweed</strong>Merrified mechanics as thesecond phase of a two phasetreament without premolarextraction.Fig. 4. Pretreatment dental castsFig. 5a. Orthopedic appliancePHASE 1First, we planned to treat the horizontal skeletalproblem in the late mixed dentition. An orthopedic appliance(Fig.5a) was worn at night for 6 months. This monoblochad a functional action on the tongue position and preventedthe thumb interposition. Its special design locked the lowerincisor in order to maintain its angulation on the mandibularplane. <strong>The</strong> acrylic bite plane was reduced in height in theposterior areas to allow lower molar eruption. Of note isthe improvement in the posterior occlusion (Fig. 5b). <strong>The</strong>reis a class 1 relationship in the cuspid and bicuspid aeras.<strong>The</strong> overjet and the overbite have decreased. <strong>The</strong> facialphotographs (Fig. 6) show improvement of the face dueto a forward translation of the mandible. <strong>The</strong> Zangle (70°)increased, theAOBO (1mm)decreased due toan increase of theSNB angle (80°).<strong>The</strong> ANB angleFig. 5b. Post orthopedics (phase I)is now 2°. In thevertical, we notethe closure ofthe FMA from 23 to 22 degrees. IMPA remined at 98 degrees. <strong>The</strong> occlusal plane is stable (Fig. 7a). <strong>The</strong> generalsuperimposition (Fig. 7b) shows the growth “acceleration” of the lower jaw while maintaining the maxilla. <strong>The</strong>rewas no change in the lower and upper incisor position. <strong>The</strong> upper molar has been maintained in its vertical andhorizontal dimension. <strong>The</strong> lower molar has moved up and forward, carried by the forward movement of the lowerjaw and the necessity to fill in the free space.This first step allowed us to correct the class II skeletalproblem with a minimum of cooperation. This protocol might movesome extreme low angle malocclusions out of a surgical plan.Fig. 6. Postorthopedic facial photographs (II)PHASE 2A set of records taken in the early permanent dentitionenabled us to evaluate the residual occlusal deficit (Fig. 8). <strong>The</strong>patient is now easy to diagnose: a class 1 maloclusion with amoderate overjet and overbite, a mild curve of Spee, and some spaceson the upper arch. Our objective is to correct the incisor position43