

Better Sooner More Convenient Primary Care - New Zealand Doctor
Better Sooner More Convenient Primary Care - New Zealand Doctor
Better Sooner More Convenient Primary Care - New Zealand Doctor

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
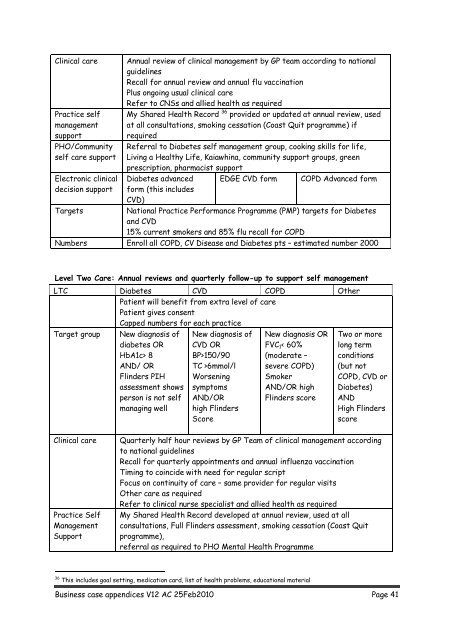
Clinical care<br />
Practice self<br />
management<br />
support<br />
PHO/Community<br />
self care support<br />
Electronic clinical<br />
decision support<br />
Targets<br />
Annual review of clinical management by GP team according to national<br />
guidelines<br />
Recall for annual review and annual flu vaccination<br />
Plus ongoing usual clinical care<br />
Refer to CNSs and allied health as required<br />
My Shared Health Record 36 provided or updated at annual review, used<br />
at all consultations, smoking cessation (Coast Quit programme) if<br />
required<br />
Referral to Diabetes self management group, cooking skills for life,<br />
Living a Healthy Life, Kaiawhina, community support groups, green<br />
prescription, pharmacist support<br />
Diabetes advanced EDGE CVD form COPD Advanced form<br />
form (this includes<br />
CVD)<br />
National Practice Performance Programme (PMP) targets for Diabetes<br />
and CVD<br />
15% current smokers and 85% flu recall for COPD<br />
Numbers Enroll all COPD, CV Disease and Diabetes pts – estimated number 2000<br />
Level Two <strong>Care</strong>: Annual reviews and quarterly follow-up to support self management<br />
LTC Diabetes CVD COPD Other<br />
Patient will benefit from extra level of care<br />
Patient gives consent<br />
Capped numbers for each practice<br />
Target group<br />
<strong>New</strong> diagnosis of<br />
diabetes OR<br />
HbA1c> 8<br />
AND/ OR<br />
Flinders PIH<br />
assessment shows<br />
person is not self<br />
managing well<br />
<strong>New</strong> diagnosis of<br />
CVD OR<br />
BP>150/90<br />
TC >6mmol/l<br />
Worsening<br />
symptoms<br />
AND/OR<br />
high Flinders<br />
Score<br />
<strong>New</strong> diagnosis OR<br />
FVC 1 < 60%<br />
(moderate –<br />
severe COPD)<br />
Smoker<br />
AND/OR high<br />
Flinders score<br />
Two or more<br />
long term<br />
conditions<br />
(but not<br />
COPD, CVD or<br />
Diabetes)<br />
AND<br />
High Flinders<br />
score<br />
Clinical care<br />
Practice Self<br />
Management<br />
Support<br />
Quarterly half hour reviews by GP Team of clinical management according<br />
to national guidelines<br />
Recall for quarterly appointments and annual influenza vaccination<br />
Timing to coincide with need for regular script<br />
Focus on continuity of care – same provider for regular visits<br />
Other care as required<br />
Refer to clinical nurse specialist and allied health as required<br />
My Shared Health Record developed at annual review, used at all<br />
consultations, Full Flinders assessment, smoking cessation (Coast Quit<br />
programme),<br />
referral as required to PHO Mental Health Programme<br />
36 This includes goal setting, medication card, list of health problems, educational material<br />
Business case appendices V12 AC 25Feb2010 Page 41














