

SPECIAL EDUCATION REFERRAL FORM REASON FOR ...
SPECIAL EDUCATION REFERRAL FORM REASON FOR ...
SPECIAL EDUCATION REFERRAL FORM REASON FOR ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
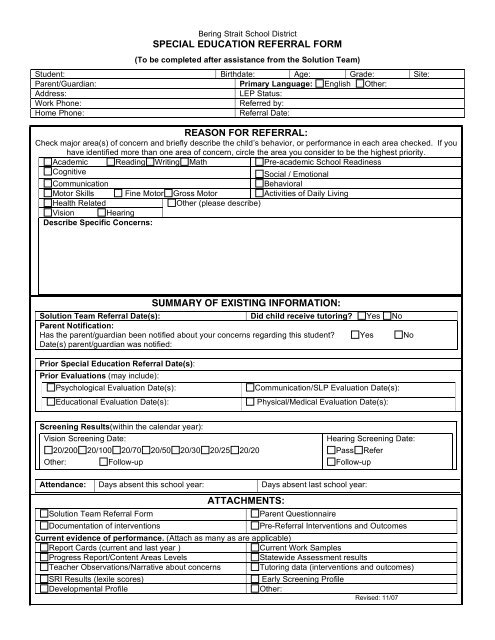
Bering Strait School District<br />
<strong>SPECIAL</strong> <strong>EDUCATION</strong> <strong>REFERRAL</strong> <strong><strong>FOR</strong>M</strong><br />
(To be completed after assistance from the Solution Team)<br />
Student: Birthdate: Age: Grade: Site:<br />
Parent/Guardian: Primary Language: English Other:<br />
Address:<br />
LEP Status:<br />
Work Phone:<br />
Referred by:<br />
Home Phone:<br />
Referral Date:<br />
<strong>REASON</strong> <strong>FOR</strong> <strong>REFERRAL</strong>:<br />
Check major area(s) of concern and briefly describe the child’s behavior, or performance in each area checked. If you<br />
have identified more than one area of concern, circle the area you consider to be the highest priority.<br />
Academic Reading Writing Math Pre-academic School Readiness<br />
Cognitive<br />
Social / Emotional<br />
Communication<br />
Behavioral<br />
Motor Skills Fine Motor Gross Motor Activities of Daily Living<br />
Health Related<br />
Other (please describe)<br />
Vision Hearing<br />
Describe Specific Concerns:<br />
SUMMARY OF EXISTING IN<strong><strong>FOR</strong>M</strong>ATION:<br />
Solution Team Referral Date(s): Did child receive tutoring? Yes No<br />
Parent Notification:<br />
Has the parent/guardian been notified about your concerns regarding this student? Yes No<br />
Date(s) parent/guardian was notified:<br />
Prior Special Education Referral Date(s):<br />
Prior Evaluations (may include):<br />
Psychological Evaluation Date(s):<br />
Educational Evaluation Date(s):<br />
Communication/SLP Evaluation Date(s):<br />
Physical/Medical Evaluation Date(s):<br />
Screening Results(within the calendar year):<br />
Vision Screening Date:<br />
20/200 20/100 20/70 20/50 20/30 20/25 20/20<br />
Other:<br />
Follow-up<br />
Hearing Screening Date:<br />
Pass Refer<br />
Follow-up<br />
Attendance: Days absent this school year: Days absent last school year:<br />
ATTACHMENTS:<br />
Solution Team Referral Form<br />
Parent Questionnaire<br />
Documentation of interventions<br />
Pre-Referral Interventions and Outcomes<br />
Current evidence of performance. (Attach as many as are applicable)<br />
Report Cards (current and last year )<br />
Current Work Samples<br />
Progress Report/Content Areas Levels<br />
Statewide Assessment results<br />
Teacher Observations/Narrative about concerns Tutoring data (interventions and outcomes)<br />
SRI Results (lexile scores)<br />
Early Screening Profile<br />
Developmental Profile<br />
Other:<br />
Revised: 11/07
Bering Strait School District<br />
SOLUTION TEAM INTERVENTIONS<br />
Date Started __________Date Ended________<br />
Target Behavior/Learning Need: __________________________________________________<br />
Describe Intervention: ___________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
Outcome: data of outcome; rate of success __________________________________________<br />
______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
Date Started __________Date Ended_________<br />
Target Behavior/Learning Need: __________________________________________________<br />
Describe Intervention: ___________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
Outcome: data of outcome; rate of success __________________________________________<br />
_______________________________________________________________________________<br />
______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
Date Started __________Date Ended_________<br />
Target Behavior/Learning Need: __________________________________________________<br />
Describe Intervention: ___________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
Outcome: data of outcome; rate of success __________________________________________<br />
______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
**Include additional pages as needed.













