TRICARE Overseas Program Provider Manual
TRICARE Overseas Program Provider Manual
TRICARE Overseas Program Provider Manual

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>TRICARE</strong> overseas <strong>Program</strong><br />
<strong>Provider</strong> <strong>Manual</strong><br />
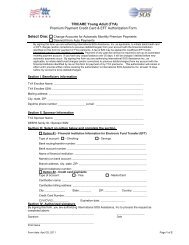
Part 4: <strong>Provider</strong>’s Details<br />
The ‘Federal Tax ID Number’ is the<br />
<strong>Provider</strong>’s <strong>TRICARE</strong> ID Number<br />
(or TEPRV). Please enter this here.<br />
Always indicate ‘Yes’ here. This<br />
ensures that payment goes to the<br />
<strong>Provider</strong>.<br />
If the patient has OHI, it will be the primary payer<br />
for the claim. After the OHI has processed the<br />
claim, indicate here how much they have paid.<br />
Also include any payments the patient has made<br />
towards the claim. If <strong>TRICARE</strong> is the patient’s only<br />
health insurance plan, leave this field blank.<br />
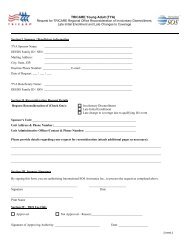
This must be signed and<br />
dated by the <strong>Provider</strong>.<br />
This does not<br />
necessarily have to be<br />
the attending physician,<br />
but can be signed by an<br />
authorized person.<br />
Note: The <strong>Provider</strong><br />
‘Signature on File’<br />
procedure can be<br />
used here.<br />
Please enter the<br />
patient’s account<br />
number. This is<br />
generated by the<br />
<strong>Provider</strong> and<br />
should not be<br />
longer than 18<br />
digits long.<br />
Please enter<br />
the <strong>Provider</strong>’s<br />
name and full<br />
physical<br />
address.<br />
Fields highlighted in green<br />
can be left blank<br />
Please enter the<br />
<strong>Provider</strong>’s full billing<br />
address if different to<br />
the physical address.<br />
SECTIoN 5<br />
<strong>Provider</strong> Claims Information<br />
63