TRICARE Overseas Program Provider Manual
TRICARE Overseas Program Provider Manual
TRICARE Overseas Program Provider Manual

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>TRICARE</strong> overseas <strong>Program</strong><br />
<strong>Provider</strong> <strong>Manual</strong><br />
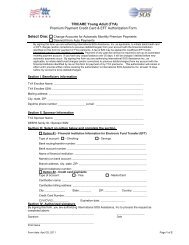
Part 1: Patient’s and Sponsor’s Details<br />
Always choose the<br />
<strong>TRICARE</strong> option.<br />
Please enter the patient’s<br />
DOB using the format<br />
MM DD YY and tick M or F to<br />
indicate the patient’s gender.<br />
Enter the sponsor’s ID number (10-digit DOD<br />
Benefit or 9-digit Social Security Number (SSN))<br />
and name using the format Last Name, First<br />
Name, Middle Initial. This information will appear<br />
on the patient’s Military ID Card.<br />
Enter the patient’s name,<br />
using the format Last Name,<br />
First Name, Middle Initial and<br />
the patient’s full physical<br />
address including post code.<br />
Enter the patient’s relationship<br />
to the sponsor.<br />
Fields highlighted in green<br />
can be left blank<br />
Enter the sponsor’s<br />
full address if different than<br />
the patient’s.<br />
If the patient has OHI enter<br />
the name of the insured party<br />
using the format Last Name,<br />
First Name, Middle Initial, the<br />
policy number and in field 9d<br />
enter the name of the<br />
insurance plan.<br />
<strong>TRICARE</strong> is always the secondary<br />
payer. If the patient has OHI policy,<br />
tick ‘YES’ here and then<br />
complete 9, 9a and 9d.<br />
If the patient does not have OHI<br />
policy, section 9 can be left blank.<br />
Enter the sponsor’s DOB,<br />
using the format MM DD YY<br />
and indicate the sponsor’s<br />
gender marking either M for<br />
Male or F for Female.<br />
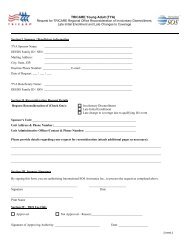
SECTIoN 5<br />
<strong>Provider</strong> Claims Information<br />
Fields highlighted in green<br />
can be left blank<br />
59