(echs) application form - Bureau of Naviks
(echs) application form - Bureau of Naviks
(echs) application form - Bureau of Naviks

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
11/1<br />
SAMPLE FOR AFFIDAVIT<br />
AFFIDAVIT ON RS. 10/- NON JUDICIAL STAMP PAPER AND TO BE ATTESTED BY MAGISTRATE/NOTARY<br />
PUBLIC DECLARATION<br />
DECLARATION<br />
I, Service No. ………………….. Rank …………… Name …………………………..<br />
<strong>of</strong> unit Indian Coast Guard solemnly affirm and declare as follows :-<br />
or<br />
I, ……………………………………. Wife/father/mother/daughter/son <strong>of</strong> Service No………………..<br />
Rank……………………………. Name………………………………..<strong>of</strong> (Unit) …………………………………. Solemnly affirm<br />
and declare as follows<br />
1. Than I am/will be drawing pension vide PCDA Pension Payment Order No.<br />
…………………………………………………………….. dated ………………..
11/2<br />
2. That I have the following legal dependent(s) whose photographs(s) is/are affixed below on this<br />
Affidavit :-<br />
Name :<br />
Photo<br />
Date <strong>of</strong> Birth :<br />
Relationship :<br />
Identification Mark :<br />
Name :<br />
Photo<br />
Date <strong>of</strong> Birth :<br />
Relationship :<br />
Identification Mark: .<br />
Name :<br />
Photo<br />
Date <strong>of</strong> Birth :<br />
Relationship :<br />
Identification Mark :<br />
Name :<br />
Photo<br />
Date <strong>of</strong> Birth :<br />
Relationship :<br />
Identification Mark :<br />
(Photograph(s) to be pasted and signed by the applicant)
11/3<br />
3. (a) That the combined monthly income (from all sources including income accruing from<br />
house/other immovable property /fixed deposit etc) <strong>of</strong> my dependent father and /or<br />
dependent mother is less than Rs. 3500/-.<br />
(b) That it is hereby certified that my parents (father/mother or both) do not draw any pension<br />
from Central Govt/State Govt/PSUs/ any Private Organisation and are physically residing with me.<br />
4. That my child/children is/are dependent on me and is /are NOT earning more than Rs. 3500/-<br />
per month & that my daughter(s) is /are NOT married.<br />
5. I shall in<strong>form</strong> the ECHS immediately <strong>of</strong> his /her/their employment <strong>of</strong> earning more than Rs.<br />
3500/- P.M.<br />
6. That in case <strong>of</strong> any change in the status <strong>of</strong> my dependents (due to death, marriage,<br />
employment), I will in<strong>form</strong> Station Headquarters, ECHS Cell at the earliest and will stop use <strong>of</strong> ECHS<br />
facilities. I will refund, in full, the cost <strong>of</strong> any treatment that my dependent may have received after<br />
he/she become ineligible. I shall be liable for civil/criminal action should I fail to do so.<br />
7. (a) That I am NOT a member <strong>of</strong> any other medical scheme funded by Central Govt, PSU or any<br />
other Govt undertaking. I will immediately in<strong>form</strong> Stn HQ if I am re-employed in the Army/Coast<br />
Guard and I am aware that my membership will remain suspended during reemployment.<br />
(b)<br />
That my spouse is NOT a member <strong>of</strong> CGHS or any other Govt Scheme.<br />
8. I understand that in case I have submitted any incorrect in<strong>form</strong>ation, or if any<br />
ECHS Membership Card is misused or used by any unauthorized person, my membership will be cancelled<br />
without any notice or further hearing. In addition, I will forfeit my contribution and I will pay the entire cost<br />
<strong>of</strong> expenditure incurred on such unauthorized person(s). I will forfeit my contribution and I will pay the entire<br />
cost <strong>of</strong> expenditure incurred on such unauthorized person(s) I will also be liable for legal action by the ECHS<br />
Organisation. I will also immediately report the loss <strong>of</strong> my ECHS membership card to the nearest Station<br />
Headquarters.<br />
9. That in case <strong>of</strong> any misuse <strong>of</strong> Smart Card(s) or tampering with bills or attempt to defraud, once I<br />
became a member, I will forfeit my membership automatically.<br />
10. I undertake that in case <strong>of</strong> any misbehavior, on my part with Polyclinic staff, my membership may be<br />
suspended/cancelled/terminated.<br />
11. I understand that the contribution I am making is a onetime token amount and is not refundable even<br />
if I do not make use <strong>of</strong> any ECHS facility or opt out <strong>of</strong> ECHS Scheme.<br />
Signature <strong>of</strong> Deponent
11/4<br />
VERIFICATION<br />
I, the deponent above named, do hereby solemnly declare and verify that contents <strong>of</strong> the<br />
above affidavit are true to the best <strong>of</strong> my knowledge and belief, and nothing material has been<br />
concealed or suppressed there from. Verified at(place) ……………………….. On this (date) …….………<br />
Day <strong>of</strong> month) ……………Year…………………….<br />
Signature <strong>of</strong> deponent<br />
ATTESTATION<br />
Certified that the above statement is declared before me at (Place) …………….……….on this …………day<br />
<strong>of</strong> (Month) ……………. Year ……….. by Deponent Name………………………..…………………… Service No.………….<br />
Rank………………… Who is identified by Name ………………………………… S/o ………………………….. and witnessed<br />
by Name…………………………… S/o……………………………….. And Name…………………………………….. S/o<br />
…………………………………..<br />
WITNESS<br />
Signature <strong>of</strong> Witness No. 1<br />
Signature <strong>of</strong> Witness No.2<br />
(Name in Block Capitals)<br />
(Full postal address)<br />
(Name in Block Capitals)<br />
(Full postal address)<br />
ATTESTED BY MAGISTRATE/NOTARY PUBLIC
MILITARY RECEIVABLE ORDER<br />
Bank's Counterfoil(To be forwarded to the CDA)<br />
(To be filled by MRO issuing authority)<br />
Received a sum <strong>of</strong> Rs.<br />
Total(Rs in words)<br />
___Crores _____Lakhs ____ Thousands ____Hundred _____Tens ___ units<br />
From ………………………………………………………………………………………………. (Name/Rank/P.No. <strong>of</strong> the individual)<br />
By Cash/Cheque No. ………….Date…………….. Bank …………… for credit to PCDA(WC) CHANDIGARH (Code No: 4013000004) on<br />
account <strong>of</strong> "EX-SERVICEMEN CONTRIBUTORY HEALTH SCHEME (ECHS)”<br />
MAJOR HEAD : 0076, MINOR HEAD: 107, COMPLIABLE TO CODE HEAD: 0/405/01<br />
BSR Code DD MM YY Serial No.<br />
Bank Seal<br />
Signature <strong>of</strong> Pensioner/Issuing Authority<br />
Depositor's Counterfoil-1 (To be retained by the Depositor)<br />
(To be filled up by Treasury/RBI/SBI Bank)<br />
Treasury/RBI/Bank …………………………….. Dated :‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐<br />
Received a sum <strong>of</strong> Rs…………………(Rupees …………………………………………………….. only) from ……………………………………………………………………..<br />
………..(Individual/Unit/Officer) on account <strong>of</strong> "EX-SERVICEMEN CONTRIBUTORY HEALTH SCHEME (ECHS)” for credit to<br />
PCDA(WC) CHANDIGARH as Defence Receipts<br />
MAJOR HEAD : 0076, MINOR HEAD: 107, COMPLIABLE TO CODE HEAD: 0/405/01<br />
o<br />
BSR Code DD MM Serial No.<br />
YY<br />
Bank Seal<br />
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐<br />
Depositor's Counterfoil-2 (To be forwarded to PCDA/CDA)<br />
(To be filled up by Treasury/RBI/SBI Bank)<br />
Treasury/RBI/Bank …………………………….. Dated :‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐<br />
Received a sum <strong>of</strong> Rs………………… (Rupees …………………………………………………….. only) from ________________________________________<br />
………………….. (Individual/Unit/Officer) on account <strong>of</strong> "EX-SERVICEMEN CONTRIBUTORY HEALTH SCHEME (ECHS)” for credit to<br />
PCDA(WC) CHANDIGARH as Defence Receipts<br />
MAJOR HEAD : 0076, MINOR HEAD: 107, COMPLIABLE TO CODE HEAD: 0/405/01<br />
BSR Code DD MM YY Serial No.<br />
Bank Seal<br />
………………………………………………………………………………………………………………………….…………………………………………………………<br />
Depositor's Counterfoil-3 (To be retained by Stn. HQ/Regional Centre)<br />
(To be filled up by Treasury/RBI/SBI Bank)<br />
Treasury/RBI/Bank …………………………….. Dated :‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐<br />
Received a sum <strong>of</strong> Rs…………………(Rupees ………………………………………..………………………… only) from …………………………………………………<br />
…………………………… (Individual/Unit/Officer) on account <strong>of</strong> "EX-SERVICEMEN CONTRIBUTORY HEALTH SCHEME (ECHS)” for credit<br />
to PCDA(WC) CHANDIGARH as Defence Receipts<br />
MAJOR HEAD : 0076, MINOR HEAD: 107, COMPLIABLE TO CODE HEAD: 0/405/01<br />
BSR Code DD MM YY Serial No.<br />
Bank Seal
14<br />
BANKER’S CERTIFICATE<br />
Certified that following :<br />
Name ………………………………………………………… Service No. ………………. Rank ………………<br />
Pension Account No ……………………………. <strong>of</strong> this bank is drawing pension as follow :<br />
(a) Uncommuted Basic Pension Rs. ……………….<br />
Including 50% Dearness Pension<br />
(b) DA Rs. ……………….<br />
(c) Fixed Medical Allowance Rs. .……………<br />
------------------<br />
Total :<br />
Rs<br />
His Pension Payment Order No. is ………………………………………………….<br />
Fixed Medical Allowance has been stopped w.e.f. (date)………………………<br />
------------------<br />
(Authority for discontinuation <strong>of</strong> FMA, CGDA New Delhi Circular No. 5601/AT – P/Paytt dated 17 Jun 05<br />
and GOI, MOD letter No. 2(a)/01/US(WE)/D (Res) dated 30 Dec 2002)<br />
Date :<br />
PDA/Bank Manager/I/C DPDO<br />
(With Official Stamp)
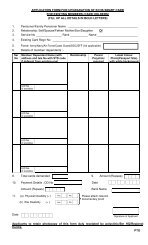
BUREAU OF NAVIKS<br />
GENERAL INSTRUCTIONS FOR FILLING-UP THE ECHS APPLICATION FORM<br />
1. Application to be filled up in capital letter with ball point pen, ink pen not to be used. No overwriting is<br />
allowed.<br />
2. While filling up the <strong>form</strong>, leave one box blank after each completed word.<br />
3. Applicant must sign/thumb impression should be clear without any overwriting with black ink within<br />
the boxes proved on the pages 1 & 4 (part-IV).<br />
4. The boxes provided at the end <strong>of</strong> pages 1, 3 and 4 (part V) in the <strong>form</strong> are to be left blank for Record<br />
Officer’s signature and stamp.<br />
5. Abbreviations such as Mr.Mrs.& Shri..etc NOT to be written before the name in the boxes.<br />
6. Copy <strong>of</strong> Pension Payment Order (PPO), duly attested by Bank from where pension is being<br />
drawn to be enclosed.<br />
7. Bankers Certificate to be made as per page no.14. Stoppage date <strong>of</strong> Fixed Medical Allowance to be<br />
mentioned (if mentioned in PPO).<br />
8.. UID Number <strong>of</strong> Aadhar Card to be mentioned in <strong>application</strong> and duly attested photo copy<br />
<strong>of</strong> the same must be enclosed.<br />
9. Recent colour(CLEAR AND SHARP) passport size photographs (Red Background) <strong>of</strong> self and the<br />
dependants are to be pasted in the appropriate boxes provided in the Application <strong>form</strong> without signing on<br />
them. Scanned/ computerized/small and poor image quality photos are not permitted.<br />
10. A single demand draft <strong>of</strong> the total amount @ Rs. 135/- per member ‘x’ number <strong>of</strong> smart cards,<br />
required to be made in favour <strong>of</strong> REGIONAL CENTRE, ECHS, DELHI CANTT” payable at DELHI, (The<br />
individual’s Name, Rank & No. to be written on the reverse side <strong>of</strong> the DD) having validity <strong>of</strong> 2-3 months at<br />
the time <strong>of</strong> reaching ECHS Cell, <strong>Bureau</strong> <strong>of</strong> <strong>Naviks</strong>.<br />
11. ECHS Contribution be made through MRO at RBI/SBI in favour <strong>of</strong> PCDA (WC) Chandigarh, on<br />
account <strong>of</strong> “Ex-servicemen Contributory Health Scheme (ECHS)”. Two copies (in original) <strong>of</strong> the<br />
same to be enclosed with <strong>application</strong>.<br />
12. Affidavit to be filled up on Rs.10/- NON JUDICIAL STAMP PAPER as per the sample and duly<br />
attested by the Magistrate/Notary with the round stamp and signature having the following: -<br />
(i) Para 1 to 11<br />
(ii) Photographs signed across by the Applicant<br />
(iii) Date <strong>of</strong> Birth, Relation and Identification mark <strong>of</strong> all the members to be written (as per the<br />
service document) below the photograph, DOB should strictly match with the Application from.<br />
(iv) Attestation to be filled correctly. i.e. particulars <strong>of</strong> Identifier and 02 witnesses.<br />
(v) Signature and full postal address <strong>of</strong> two witnesses.<br />
13. Lab report <strong>of</strong> Blood Group for self and dependent must be enclosed.<br />
14. Parent polyclinic to be filled in <strong>application</strong> must be nearest to the residential address <strong>of</strong> each member.<br />
List <strong>of</strong> polyclinics is at page no.13.<br />
15. Additional photo copy <strong>of</strong> fully filled and updated <strong>application</strong> to be enclosed.