A comparative study of tension band wiring and reconstruction ...
A comparative study of tension band wiring and reconstruction ...
A comparative study of tension band wiring and reconstruction ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Khanna et al<br />
Severely comminuted fractures were given preference for<br />
internal fixation with plate. Cases were classified as per Horne<br />
<strong>and</strong> Tanzer’s Classification 6 (Table-1)<br />
Type-1<br />
Type-2<br />
Type-3<br />
Table 1<br />
Showing the classification <strong>of</strong> Olecranon<br />
Transverse intra-articular fractures on the proximal third<br />
<strong>of</strong> the articular surface <strong>of</strong> the olecranon fossa or oblique<br />
extra-articular fracture <strong>of</strong> the olecranon<br />
Oblique or transverse fractures on the middle third <strong>of</strong> the<br />
articular surface <strong>of</strong> the olecranon fossa.<br />
Oblique or transverse fractures on the middle third<strong>of</strong> the<br />
articular surface <strong>of</strong> the olecranon fossa.<br />
Transverse or oblique fractures on the distal third <strong>of</strong>the<br />
olecranon fossa.<br />
3 rd generation cephalosporins plus aminoglycosides were given<br />
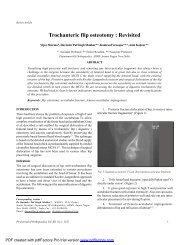
for 72 hours.X-rays were taken on 1 st post-operative dayto<br />
confirm the fixation <strong>and</strong> reduction. Wound site was checked<br />
on 3 rd post-op day. Stitches were removed on 12th post-op<br />
day.<br />
The patients were examined on 3rd, 6th, 9th, 12th week<br />
<strong>and</strong> at six weekly intervals after that. On every visit patients<br />
were examined clinically <strong>and</strong> X-rays <strong>of</strong> the elbow taken in<br />
anteroposterior <strong>and</strong> lateral view. Movements <strong>of</strong> elbow were<br />
recorded. During the period <strong>of</strong> follow up, only active exercises<br />
in physiotherapy centre or at home were advocated.<br />
Every patient <strong>of</strong> each group then is graded during his<br />
follow-up for clinical <strong>and</strong> radiological results as per criteria laid<br />
by Rogers et al 8 . (Table-2)<br />
Surgical steps:<br />
Exposure: General Anesthesia or brachial block was preferred<br />
<strong>and</strong> tourniquet was used in all cases. Posterior midline incision,<br />
extending 2.5 cm proximal <strong>and</strong> 10 cm distal to the olecranon<br />
was usedfor both groups <strong>and</strong> fracture site was exposed 7 .<br />
ORIF with TBW: A hole was drilled transversely in the ulna<br />
about 5-7 cm distal to fracture site. A Stainless steel wire No.20<br />
was passed through this hole. Two parallel 2.00 mm K-wires<br />
were drilled from the tip <strong>of</strong> the olecranon through the proximal<br />
fragment in slight oblique anterior direction to engage the<br />
anterior cortex <strong>of</strong> the distal fragment <strong>of</strong> ulna. The loop <strong>of</strong> wire<br />
was crossed over the posterior surface <strong>of</strong> the olecranon in<br />
figure <strong>of</strong> eight fashion <strong>and</strong> passed around the protruded K-<br />
wires under the triceps tendon. The wire was tightened <strong>and</strong><br />
secured with a twist. Range <strong>of</strong> movements checked. K-wires<br />
were cut <strong>and</strong> bended end was rotated posteriorly <strong>and</strong> impacted<br />
in the olecranon under the triceps. Wound was stitched in<br />
layers <strong>and</strong> was sealed <strong>and</strong> compression <strong>b<strong>and</strong></strong>age applied.<br />
ORIF with 3.5 mm Reconstruction plate: After reduction<br />
<strong>of</strong> fragments, the fracture was temporarily fixed <strong>and</strong> aligned<br />
with 2.00 mm K-wire passed from the tip into the medullary<br />
canal <strong>of</strong> distal ulna. After necessary contouring <strong>of</strong> the plate, it<br />
was applied subperiosteally on the posterior or posteromedial<br />
surface <strong>of</strong> ulna, using 3.5mm cortical <strong>and</strong> 4.0mm cancellous<br />
screws. K-wire was not removed in some cases so as to maintain<br />
the fixation <strong>and</strong> alignment. Wound was closed in layers <strong>and</strong><br />
dressing was applied.<br />
POSTOPERATIVE MANAGEMENT & FOLLOW UP<br />
The operated limb was kept elevated for 48 hours. Intravenous<br />
RESULTS<br />
Table 2<br />
SHOWING BASIS OF GRADING<br />
Grade Loss <strong>of</strong> Loss <strong>of</strong> Union<br />
movement supination <strong>and</strong><br />
at elbow pronation<br />
Excellent