Intraarticular fractures: Past, present and future? - Punjab ...
Intraarticular fractures: Past, present and future? - Punjab ...
Intraarticular fractures: Past, present and future? - Punjab ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Review Article<br />
<strong>Intraarticular</strong> <strong>fractures</strong>: <strong>Past</strong>, <strong>present</strong> <strong>and</strong> <strong>future</strong><br />
Bhavuk Garg*, Rajesh Malhotra**<br />
*Assistant Professor, ** Professor<br />
Department of Orthopaedics<br />
AIIMS, New Delhi<br />
INTRODUCTION<br />
<strong>Intraarticular</strong> <strong>fractures</strong>, if not properly h<strong>and</strong>led, inevitably<br />
lead to stiffness, pain or osteoarthritis (posttraumatic) 1 . Sir<br />
John Charnley advocated non-operative management of<br />
intraarticular <strong>fractures</strong> in his famous book on conservative<br />
management of <strong>fractures</strong> entitled “The Closed Treatment of<br />
Common Fractures” 2 . Several other authors including Neer et<br />
al 3 <strong>and</strong> Stewart et al 4 also advocated the same. Unavailability<br />
of proper internal fixation devices as well as lack of proper<br />
underst<strong>and</strong>ing of orthopedic surgical principles was the main<br />
reason for this favor for conservative management.<br />
After foundation of AO group in 1958, a lot of<br />
improvements in orthopedic internal fixation devices as well as<br />
an improved underst<strong>and</strong>ing of orthopedic surgical principles<br />
prevailed. AO/ASIF group reported better outcome of<br />
intraarticular <strong>fractures</strong> with open reduction <strong>and</strong> internal fixation 5 .<br />
Several other authors echoed similar results 6, 7 . It was also<br />
observed that intraarticular <strong>fractures</strong> that underwent ORIF as<br />
well as immobilization had much more stiffness <strong>and</strong> worse<br />
outcome than <strong>fractures</strong>, which were either, underwent ORIF<br />
<strong>and</strong> early motion or immobilization alone 8 . AO group also<br />
advocated that intraarticular <strong>fractures</strong> behave in a different<br />
biological <strong>and</strong> functional manner as compared to diaphyseal<br />
<strong>fractures</strong>.<br />
PRINCIPLES OF INTRAARTICULAR FRACTURE<br />
MANAGEMENT<br />
Mitchell <strong>and</strong> Shepard 9 reported that articular cartilage<br />
regenerate after intraarticular <strong>fractures</strong> provided anatomical<br />
reduction <strong>and</strong> absolute stability. Salter et al 10 showed that<br />
continuous passive motion stimulates articular cartilage healing<br />
as well as regeneration. Schatzker et al 11 pointed out following<br />
principles of intraarticular fracture treatment:<br />
1. Immobilization of intraarticular <strong>fractures</strong> leads to stiffness<br />
of joint.<br />
2. Immobilization combined with ORIF of intraarticular<br />
<strong>fractures</strong> causes much more stiffness.<br />
3. Depressed <strong>and</strong> impacted articular fragments will not reduce<br />
by closed manipulation or ligamentotaxis.<br />
4. Big articular defects do not fill by fibrocartilage, resulting<br />
in instability due to their displacement.<br />
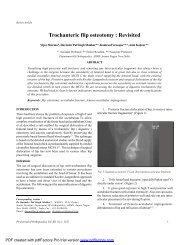
5. Anatomical reduction <strong>and</strong> as well as absolute stability is<br />
vital to the optimum healing of articular <strong>fractures</strong>. (Fig. 2)<br />
6. Metaphyseal voids should be bone grafted (Fig. 3)<br />
(however with use of current locking plates, this has<br />
become controversial).<br />
7. Any metaphyseal <strong>and</strong> diaphyseal displacements should<br />
be reduced to prevent extra load on the joint (This reduction<br />
need not to be anatomical)<br />
8. More important is to restore the joint congruity as well as<br />
axial alignment.<br />
Corresponding Author :<br />
Dr Bhavuk Garg,<br />
Assistant Professor,<br />
Department of Orthopaedics,<br />
AIIMS, New Delhi-110029<br />
Email: drbhavukgarg@gmail.com<br />
Pb Journal of Orthopaedics Vol-XIII, No.1, 2012<br />
Fig 2. A depressed intra-articular fracture of proximal tibia<br />
managed by anatomical reduction, stable fixation <strong>and</strong> early<br />
c motion. Patient had excellent functional result<br />
25
Garg <strong>and</strong> Malhotra<br />
Fig 4. CT gives much detailed description of intraarticular<br />
fracture anatomy<br />
Fig 3. Bone grafting should be done in cases of metaphyseal voids,<br />
particularly in osteoporotic bones<br />
9. Early motion is essential for optimal healing of articular<br />
cartilage <strong>and</strong> best outcome. Stable internal fixation is a<br />
must for this.<br />
BASIC SCIENCES FACTS ABOUT INTRAARTICULAR<br />
FRACTURES<br />
Articular cartilage is an aneural structure with no blood or<br />
lymphatic supply <strong>and</strong> is dependent upon diffusion from<br />
surrounding tissues for nutrition.Relationship between articular<br />
cartilage injury <strong>and</strong> subsequent development of osteoarthritis<br />
is a complex phenomenon. Articular cartilage healing leads to<br />
formation of fibrocartilage, however it does not restore the<br />
structural <strong>and</strong> mechanical properties of a normal articular<br />
cartilage 12 . Larger the defect, larger is the alteration of<br />
mechanical properties; larger is the risk of progression to<br />
osteoarthritis. 12 . Marsh et al 13 reported that development of<br />
posttraumatic osteoarthritis correlate with the severity of<br />
articular damage. Several other authors have also reported the<br />
same findings 14, 15 .<br />
The thickness of articular cartilage varies from joint to<br />
joint <strong>and</strong> is also variable at different sites in a single joint 16<br />
(Ankle 1.0 - 1.62mm, Knee 1.69 - 2.55mm, Patella 1.76 - 2.59mm).<br />
Articular cartilage step-offs do remodel but have limited<br />
capability 17 . Articular step-offs that exceeds the full thickness<br />
of articular cartilage usually do not remodel completely. These<br />
step offs lead to localized <strong>and</strong> altered mechanical peak pressures,<br />
leading to rapid progression of osteoarthritis 18 . Usually a stepoff<br />
of less than 2 mm is acceptable 12 . Extra-articular deformities<br />
also affect the development of osteoarthritis after intraarticular<br />
<strong>fractures</strong> by virtue of altered mechanical axis <strong>and</strong> eccentric<br />
joint loading 19 . Management of soft tissue surrounding joint<br />
is also very important in determining the optimal outcome<br />
following intraarticular <strong>fractures</strong> 20, 21 . Joint immobilization<br />
causesraised joint pressure( leading to loss of nutrition <strong>and</strong><br />
chondrocyte death. There is also liberation of several enzymes<br />
like proteases, which lead to articular surface degeneration.<br />
Motion promoteshealing of full thickness articular cartilage<br />
defects with hyaline articular “cartilage like” material.<br />
IMAGING OF INTRAARTICULAR FRACTURES<br />
A detailed radiographic workup is essential to underst<strong>and</strong> the<br />
fracture anatomy of intraarticular <strong>fractures</strong>. AP <strong>and</strong> lateral x-<br />
rays alone are usually not sufficient. Computed tomography is<br />
very useful for delineating the fracture configuration <strong>and</strong> has<br />
proved invaluable in current planning <strong>and</strong> management of<br />
intraarticular <strong>fractures</strong> (Fig. 4). This is more important in certain<br />
complex <strong>fractures</strong> like acetabular <strong>fractures</strong>, distal humerus<br />
<strong>fractures</strong>, distal tibia <strong>fractures</strong> etc.CT gives detailed description<br />
of articular gap <strong>and</strong> step offs 22, 23 . According to a study by<br />
Pb Journal of Orthopaedics Vol-XIII, No.1, 2012<br />
26
<strong>Intraarticular</strong> Fractures<br />
Fig 6. Travelling temporary fixator<br />
Fig 5. Infection <strong>and</strong> wound healing problems are common<br />
if surgery is done early through traumatic soft tissue envelope<br />
Fig 7a. AP <strong>and</strong> lateral X-rays of intraarticular radial head fracture<br />
Fig 7b. Exposure of fracture<br />
Tornetta 24 , surgical plan changed in 64% cases after CT <strong>and</strong><br />
additional information was available in 82% cases.<br />
Recently intraoperative 3-D fluoroscopy has been<br />
introduced, which usually provide inferior quality images than<br />
intraoperative CT but is much cheaper but has similar clinical<br />
value. Several studies 26-27 have proved the usefulness of this<br />
investigation <strong>and</strong> have led the surgeons to change their implant<br />
placement during surgery.<br />
TIMING TO OPERATE<br />
<strong>Intraarticular</strong> <strong>fractures</strong> rarely require urgent ORIF except in open<br />
<strong>fractures</strong>, <strong>fractures</strong> with neurovascular complications,<br />
associated compartment syndrome <strong>and</strong> irreducible fracture<br />
dislocations. Proper management of intraarticular <strong>fractures</strong><br />
requiresappreciation of fracture anatomy as well as soft tissue<br />
injury. (Fig. 5). So it is prudent to wait for soft tissue healing<br />
before embarking upon the surgery. This can vary from days to<br />
weeks 11 . In between the time, one can use bridging external<br />
fixators also known as travelling fixators (Fig. 6) with definitive<br />
fixation later on. Several indirect reduction techniques <strong>and</strong><br />
biological fixation concepts have also come to reduce trauma<br />
to soft tissue envelope.<br />
It is also important to assess the resources of surgeon as<br />
well as of the institution <strong>and</strong> cases should be referred to higher<br />
centers if facilities are inadequate.<br />
SURGICAL PRINCIPLES (FIG 7)<br />
An atraumatic surgical approach should be used. Both<br />
minimally invasive <strong>and</strong> open approaches are available, however<br />
all articular fragments must be reduced anatomically <strong>and</strong><br />
Pb Journal of Orthopaedics Vol-XIII, No.1, 2012<br />
27
Garg <strong>and</strong> Malhotra<br />
Fig 7c. Reduction of articular surface<br />
Fig 7d. Provisional fixation of fracture with K wires<br />
motion in intraarticular <strong>fractures</strong>. Active assisted exercises are<br />
preferable, muscles & joints both are rehabilitated. Continuous<br />
passive motion (CPM) does not prevent muscle atrophy<br />
(however still a useful tool in the management of intraarticular<br />
<strong>fractures</strong>. Sometimes stability of fixation can be of concern.<br />
Some sort of additional stability can be provided with ROMsplints.<br />
Plaster immobilization should not be used after ORIF<br />
of intraarticular <strong>fractures</strong> as it leads to more stiffness. Patients<br />
are kept non-weight bearing until articular fracture is healed.<br />
Fig 7e. Postop x-rays showing definitive fixation<br />
with plates <strong>and</strong> screws<br />
preferably under vision. Ligamentotaxis will only work for<br />
fragments with ligament attachment ( i.e. some split <strong>fractures</strong><br />
of the tibial plateau.<br />
Surgical reconstruction begins with anatomical reduction<br />
of articular surface.<br />
Sometimes depressed fragments need to be elevated. Bone<br />
graft or bone substitute is used to support this elevated<br />
fragment if necessary. This articular reduction is then secured<br />
with K-wires or screws <strong>and</strong> then this articular block is fixed to<br />
the metaphysis with the help of definitive implant. Now a day,<br />
periarticular anatomical locking plates have become<br />
indispensable in the management of these <strong>fractures</strong>. All<br />
measures are taken to minimize trauma to the surrounding soft<br />
tissue.<br />
POSTOPERATIVE REHABILITATION<br />
Several studies 29-31 have reported beneficial effects of early<br />
EMERGING TECHNOLOGIES<br />
T1-rho MRI mapping, which measure relaxation times in cartilage<br />
can assess specific components of articular cartilage<br />
biochemistry <strong>and</strong> ultra-structure. It has shown to be more<br />
sensitive to cartilage degradation than conventional MRI<br />
techniques 32-34 .<br />
Recently virtual operative plan can be made preoperatively<br />
with the help of electronic templating. Electronic templating is<br />
also useful in planning of implant needs as well as positioning<br />
over the bone fragments. Superior softwares are being<br />
introduced to improve the efficacy as well as extent of<br />
application of this technology. 35<br />
Navigation is another important breakthrough which helps<br />
in the management of complex intraarticular <strong>fractures</strong> like<br />
acetabular <strong>fractures</strong>. Both CT based as well as fluoroscopy<br />
36, 37<br />
based navigations are available in today’s world.<br />
New technologies are being added to orthopedics day by<br />
day. Some technologies like nanotechnology have the potential<br />
to change the current orthopedic practice completely.<br />
REFERENCES<br />
1. Muller ME, Allgower M, Schneider K, Willenegger H (1979) Manual<br />
of internal fixation, 2 nd edn. Springer, Berlin Heidelberg, New York.<br />
Pb Journal of Orthopaedics Vol-XIII, No.1, 2012<br />
28
<strong>Intraarticular</strong> Fractures<br />
2. Charnley J (1961) The closed treatment of common <strong>fractures</strong>.<br />
Livingstone, Edinburgh.<br />
3. Neer C, Graham SA, Shelton ML (1967). Supracondylar fracture of<br />
the adult femur. J Bone Joint Surg 49 A: 591-613<br />
4. Stewart M, Sisk D, Wallace SL (1966) Fractures of the distal third<br />
of the femur. J Bone Joint Surg 48 A: 784-807<br />
5. Wenzl H, Casey PA, Hebert P, Belin J (1970) Die operative<br />
Beh<strong>and</strong>lung der distalenFemurfraktur. AO Bulletin, Bern<br />
6. Mize RD, Bucholz RW, Grogan DP (1982) Surgical treatment of<br />
displaced comminuted <strong>fractures</strong> of distal end of femur. J Bone Joint<br />
Surg 64A: 871-879<br />
7. Schatzker J, Lampert DC (1979) Supracondylar <strong>fractures</strong> of the<br />
femur. Clin Orthop 138:77-83<br />
8. Schatzker J, McBroom R, Bruce D (1979) The tibial plateau<br />
fracture: the Toronto experience. Clin Orthop 138:94-104<br />
9. Mitchell N, Shepard N (1980) Healing of articular cartilage in<br />
intraarticular <strong>fractures</strong> in rabbits. J Bone Joint Surg 62A: 628-634<br />
10. Salter RB et al (1980). The biological effects of continuous passive<br />
motion on the healing of full thickness defects in articular cartilage:<br />
an experimental investigation in the rabbit. J Bone Joint Surg 62A:<br />
1232-1251<br />
11. Schatzker J, Tile M (2005) The rationale of Operative Fracture<br />
Care, 3rd edn, Springer, Berlin Heidelberg, New York<br />
12. Dirschl DR, Marsh L, Buckwalter JA et al. Articular <strong>fractures</strong>. J Am<br />
AcadOrthopSurg 2004; 12:416-423<br />
13. Marsh JL, Buckwalter J, Brown T, et al: Articular <strong>fractures</strong>: Does an<br />
anatomic reduction really change the result J Bone Joint Surg Am<br />
2002; 84:1259-1271.<br />
14. Crutchfield EH, Seligson D, Henry SL, Warnholtz A: Tibialpilon<br />
<strong>fractures</strong>: A comparative clinical study of management techniques<br />
<strong>and</strong> results. Orthopedics 1995; 18:613-617.<br />
15. S<strong>and</strong>ers R, Fortin P, DiPasquale T, Walling A: Operative treatment<br />
in 120 displaced intraarticular calcaneal <strong>fractures</strong>: Results using a<br />
prognostic computed tomography scan classification. Clin Orthop<br />
1993; 290:87-95.<br />
16. Shepherd DET, Seedhom BB. Thickness of human articular cartilage<br />
in joints of the lower limb. Ann Rheum Dis 1999; 58:27-34<br />
17. Lovász G, Llinás A, Benya PD, Park SH, Sarmiento A, Luck JV Jr:<br />
Cartilage changes caused by a coronal surface stepoff in a rabbit<br />
model. Clin Orthop 1998;354:224-234.<br />
18. Brown TD, Anderson DD, Nepola JV, Singerman RJ, Pedersen DR,<br />
Br<strong>and</strong> RA: Contact stress aberrations following imprecise reduction<br />
of simple tibial plateau <strong>fractures</strong>. J Orthop Res 1988;6:851-862<br />
19. Rasmussen PS: Tibial condylar frac- tures as a cause of degenerative<br />
arthritis. ActaOrthopSc<strong>and</strong> 1972;43:566-575.<br />
20. McFerran MA, Smith SW, Boulas HJ, Schwartz HS: Complications<br />
encountered in the treatment of pilon <strong>fractures</strong>. J Orthop Trauma<br />
1992;6:195-200.<br />
21. Blauth M, Bastian L, Krettek C, Knop C, Evans S: Surgical options<br />
for the treatment of severe tibialpilon <strong>fractures</strong>: A study of three<br />
techniques. J Orthop Trauma 2001;15:153-160.<br />
22. S<strong>and</strong>ers R, Fortin P, DiPasquale T, Walling A: Operative treatment<br />
in 120 displaced intraarticular calcaneal <strong>fractures</strong>: Results using a<br />
prognostic computed tomography scan classification. Clin Orthop<br />
1993;290:87-95.<br />
23. Cole RJ, Bindra RR, Evanoff BA, Gilula LA, Yamaguchi K, Gelberman<br />
RH. Ra- diographic evaluation of osseous displacement following<br />
intra-articular <strong>fractures</strong> of the distal radius: Reliability of plain<br />
radiography versus computerized tomography. J H<strong>and</strong> Surg [Am]<br />
1997;22:792-800.<br />
24. Tornetta P, Gorup J. Axial computed tomography of pilon <strong>fractures</strong>.<br />
Clin Orthop Relat Res. 1996 Feb; (323):273-6.<br />
25. Kendoff D, Citak M, Gardner MJ, Stübig T, Krettek C, Hüfner T.<br />
Intraoperative 3D imaging: value <strong>and</strong> consequences in 248 cases. J<br />
Trauma. 2009 Jan;66(1):232-8.<br />
26. Kendoff D, Citak M, Gardner M, Kfuri M Jr, Thumes B, Krettek C,<br />
Hüfner T. Three-dimensional fluoroscopy for evaluation of articular<br />
reduction <strong>and</strong> screw placement in calcaneal <strong>fractures</strong>. Foot Ankle<br />
Int. 2007 Nov;28(11):1165-71.<br />
27. Kendoff D, Gardner MJ, Citak M, Kfuri M Jr, Thumes B, Krettek<br />
C, Hüfner T. Value of 3D fluoroscopic imaging of acetabular <strong>fractures</strong><br />
comparison to 2D fluoroscopy <strong>and</strong> CT imaging. Arch Orthop<br />
Trauma Surg. 2008 Jun;128(6):599-605.<br />
28. Kendoff D, Pearle A, Hüfner T, Citak M, Gösling T, Krettek C.<br />
First clinical results <strong>and</strong> consequences of intraoperative threedimensional<br />
imaging at tibial plateau <strong>fractures</strong>. J Trauma. 2007 Jul;<br />
63(1): 239-44.<br />
29. Salter RB. Continuous passive motion: from origination to research<br />
to clinical applications. J Rheumatol. 2004 Nov;31(11):2104-5.<br />
30. Salter RB. History of rest <strong>and</strong> motion <strong>and</strong> the scientific basis for<br />
early continuous passive motion. H<strong>and</strong> Clin. 1996 Feb;12(1):1-11.<br />
31. Salter RB. The physiologic basis of continuous passive motion for<br />
articular cartilage healing <strong>and</strong> regeneration. H<strong>and</strong> Clin. 1994<br />
May;10(2):211-9<br />
32. Souza RB, Stehling C, Wyman BT, Hellio Le Graver<strong>and</strong> MP, Li X,<br />
Link TM, Majumdar S. The effects of acute loading on T1rho <strong>and</strong><br />
T2 relaxation times of tibiofemoral articular cartilage. Osteoarthritis<br />
Cartilage. 2010 Dec;18(12):1557-63.<br />
33. Zarins ZA, Bolbos RI, Pialat JB, Link TM, Li X, Souza RB, Majumdar<br />
S. Cartilage <strong>and</strong> meniscus assessment using T1rho <strong>and</strong> T2<br />
measurements in healthy subjects <strong>and</strong> patients with osteoarthritis.<br />
Osteoarthritis Cartilage. 2010 Nov;18(11):1408-16.<br />
34. Bolbos RI, Ma CB, Link TM, Majumdar S, Li X. In vivo T1rho<br />
quantitative assessment of knee cartilage after anterior cruciate<br />
ligament injury using 3 Tesla magnetic resonance imaging. Invest<br />
Radiol. 2008 Nov;43(11):782-8.<br />
35. Pilson HT, Reddix RN Jr, Mutty CE, Webb LX. The long lost art of<br />
preoperative planning—resurrected Orthopedics. 2008<br />
Dec;31(12).<br />
36. Hoffmann M, Schröder M, Lehmann W, Kammal M, Rueger JM,<br />
HerrmanRuecker A. Next generation distal locking for<br />
intramedullary nails using an electromagnetic X-ray-radiation-free<br />
real-time navigation system. J Trauma Acute Care Surg. 2012<br />
Jul;73(1):243-8.<br />
37. Oberst M, Hauschild O, Konstantinidis L, Suedkamp NP, Schmal H.<br />
Effects of three-dimensional navigation on intraoperative<br />
management <strong>and</strong> early postoperative outcome after open reduction<br />
<strong>and</strong> internal fixation of displaced acetabular <strong>fractures</strong>. J Trauma<br />
Acute Care Surg. 2012 Jun 14. [Epub ahead of print]<br />
Pb Journal of Orthopaedics Vol-XIII, No.1, 2012<br />
29