Role of primary bipolar arthroplasty or total hip arthroplasty - Punjab ...
Role of primary bipolar arthroplasty or total hip arthroplasty - Punjab ...
Role of primary bipolar arthroplasty or total hip arthroplasty - Punjab ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Walia et al<br />
Surgery was done under general <strong>or</strong> spinal anaesthesia<br />
depending upon the choice <strong>of</strong> anaesthesiologist. All patients<br />
were operated in lateral decubitus via posterolateral<br />
approach. The fascia was incised in line with the skin incision.<br />
After blunt dissection <strong>of</strong> gluteus maximus the gluteus medius<br />
was retracted to expose the sh<strong>or</strong>t external rotat<strong>or</strong> muscles <strong>of</strong><br />
the <strong>hip</strong>. The abduct<strong>or</strong>-greater trochanter-vastus lateralis<br />
complex was kept intact. Sh<strong>or</strong>t external rotat<strong>or</strong>s were divided<br />
close to their insertion and an inverted T shaped incision was<br />
made on the joint capsule. The fem<strong>or</strong>al neck was osteotomised<br />
and the fem<strong>or</strong>al head was removed. Patients were subjected to<br />
either hemi<strong>arthroplasty</strong>, with cemented <strong>bipolar</strong> prosthesis, <strong>or</strong><br />
<strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> depending upon condition <strong>of</strong> the<br />
acetabulum<br />
Hemi<strong>arthroplasty</strong> - Once the head-neck fragment has been<br />
removed the medullary canal <strong>of</strong> the femur is readily accessible.<br />
The canal was rasped with an appropriately sized broach and<br />
trial prosthesis was inserted. A helpful guide used f<strong>or</strong> the<br />
appropriate height <strong>of</strong> calcar reconstruction is the relations<strong>hip</strong><br />
between the centre <strong>of</strong> fem<strong>or</strong>al head and tip <strong>of</strong> the greater<br />
trochanter: It should be essentially coplanar. Although this<br />
may be difficult to assess in presence <strong>of</strong> trochanteric fracture,<br />
usually, the greater trochanter fragments are still somewhat<br />
attached and can be used as a gross guide f<strong>or</strong> evaluating the<br />
appropriate level f<strong>or</strong> prosthesis. Following an acceptable trail<br />
fit, leg length and <strong>hip</strong> stability are assessed. The head was redislocated<br />
and a permanent <strong>bipolar</strong> prosthesis was cemented<br />
into the femur at the proper level. After reduction the movements<br />
<strong>of</strong> the <strong>hip</strong> were checked.<br />
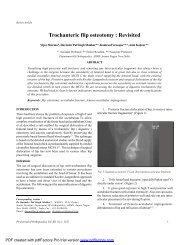
Figure 1: Pre and post operative X-ray <strong>of</strong> <strong>bipolar</strong> case<br />
Total Hip Replacement - The acetabulam was prepared by<br />
excising the ligamentum teres and removing the articular<br />
cartilage with acetabular reamer till raw cancellous bleeding<br />
bone was exposed. The fitting <strong>of</strong> the acetabular component<br />
was checked. Acetabular cup was placed in a position <strong>of</strong> 45-55 0<br />
abduction and 10-15 0 anteversion. Fem<strong>or</strong>al preparation was<br />
done as already mentioned above f<strong>or</strong> <strong>bipolar</strong> hemi<strong>arthroplasty</strong>.<br />
Trail reduction was done and s<strong>of</strong>t tissue tension<br />
checked. Following an acceptable trail fit, leg length and <strong>hip</strong><br />
stability are assessed. The head was re-dislocated and a<br />
permanent prosthesis was cemented into the femur at the<br />
proper level. After reduction the movements <strong>of</strong> the <strong>hip</strong> were<br />
checked.<br />
Figure 2: Pre and post operative X-ray <strong>of</strong> THR case<br />
Trochanteric reconstruction: Displaced trochanter was<br />
fixed acc<strong>or</strong>dingly as per geometry, comminution <strong>of</strong> fracture with<br />
the help <strong>of</strong> SS Wire <strong>or</strong> vicryl numbrt 1 reinf<strong>or</strong>ced with bone<br />
cement. Fem<strong>or</strong>al head was used f<strong>or</strong> reconstructing the medial<br />
bone loss wherever required.<br />
After reattachment <strong>of</strong> capsule and sh<strong>or</strong>t external rotat<strong>or</strong>s,<br />
closure in layers was done over drain.<br />
Physiotherapy was started on the first postoperative day.<br />
On the second postoperative day, patients were allowed<br />
to sit on the side <strong>of</strong> the bed <strong>or</strong> upright in a chair. Gait training<br />
was begun and weight-bearing was permitted earliest, as<br />
tolerated. As all the patients were elderly, they required a walker<br />
f<strong>or</strong> balance during gait training.<br />
Patients were discharged 5-12 days after surgery and were<br />
advised to continue physiotherapy until they could return to<br />
independent living.<br />
Patients were evaluated clinically acc<strong>or</strong>ding to the Harris<br />
<strong>hip</strong> sc<strong>or</strong>e 5 and Salvati-Wilson <strong>hip</strong> sc<strong>or</strong>e 6 in out-patient facilities<br />
at follow-ups.<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XII, No.1, 2011<br />
6<br />
PDF created with pdfFact<strong>or</strong>y Pro trial version www.pdffact<strong>or</strong>y.com