Role of primary bipolar arthroplasty or total hip arthroplasty - Punjab ...
Role of primary bipolar arthroplasty or total hip arthroplasty - Punjab ...
Role of primary bipolar arthroplasty or total hip arthroplasty - Punjab ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Original Article<br />
<strong>Role</strong> <strong>of</strong> <strong>primary</strong> <strong>bipolar</strong> <strong>arthroplasty</strong> <strong>or</strong> <strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> f<strong>or</strong><br />
the treatment <strong>of</strong> intertrochanteric fracture femur in elderly<br />
Jaswinder Pal Singh Walia*, Dheeraj Sansanwal**, Sonam Kaur Walia**,<br />
Sargun Singh***, Avinash Chander Gupta****<br />
*Pr<strong>of</strong>ess<strong>or</strong>, **Juni<strong>or</strong> Resident, ***Undergraduate, ****Associate Pr<strong>of</strong>ess<strong>or</strong><br />
Department <strong>of</strong> Orthopaedics,<br />
Govt. Medical College and Rajindra Hospital, Patiala, <strong>Punjab</strong>.<br />
ABSTRACT<br />
Extracapsular fractures <strong>of</strong> femur in elderly patients are associated with high rate <strong>of</strong> m<strong>or</strong>bidity and m<strong>or</strong>tality.<br />
Primary cemented <strong>hip</strong> <strong>arthroplasty</strong> is a very useful procedure f<strong>or</strong> the unstable comminuted intertrochanteric<br />
fractures with osteop<strong>or</strong>otic bone in elderly patients. The procedure markedly improved the clinical as well as<br />
functional status <strong>of</strong> the patients. The present study was conducted on 50 cases <strong>of</strong> extra capsular fractures <strong>of</strong><br />
femur above the age group <strong>of</strong> 50 years. Out <strong>of</strong> the 50 cases, 25 were those in whom cemented <strong>bipolar</strong><br />
prosthesis was used while in other 25, <strong>total</strong> <strong>hip</strong> replacement <strong>arthroplasty</strong> was done. There was no significant<br />
difference between two f<strong>or</strong>ms <strong>of</strong> <strong>arthroplasty</strong> (Bipolar hemi-replacement <strong>or</strong> Total Hip replacement) in terms<br />
<strong>of</strong> hospital stay, time period required f<strong>or</strong> partial <strong>or</strong> complete weight bearing, and functional results. Though<br />
<strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> appears to provide slightly better results regarding pain and mobility; its instability<br />
in addition to impaired reflexes, cognitive impairment, and weaker musculature in elderly shows higher<br />
dislocation rates. This can lead to increased hospital stay <strong>or</strong> revision surgery. This complication was not<br />
seen by us in hemi<strong>arthroplasty</strong> group.So we are <strong>of</strong> the opinion that although it may appear to be equally<br />
good results in both groups, in elderly patients, however, the choice should fall f<strong>or</strong> <strong>bipolar</strong> hemi-<strong>arthroplasty</strong><br />
than f<strong>or</strong> <strong>total</strong> <strong>hip</strong> replacement.It should however be noted that a larger randomized trial, with higher number<br />
<strong>of</strong> patients, <strong>or</strong> multi-centric trial can improve the interpretation <strong>of</strong> the results.<br />
Keyw<strong>or</strong>ds: Inter-trochanteric fem<strong>or</strong>al fractures, <strong>primary</strong> <strong>bipolar</strong> <strong>arthroplasty</strong>, <strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong>,<br />
elderly fem<strong>or</strong>al fractures.<br />
INTRODUCTION<br />
Hip fracture is a devastating injury, incidence <strong>of</strong> which has<br />
increased because <strong>of</strong> increased life expectancy 1 . Disability<br />
frequently results from persistent pain and limited physical<br />
mobility in <strong>hip</strong> fractures and is associated with substantial<br />
m<strong>or</strong>bidity and m<strong>or</strong>tality. F<strong>or</strong> the health care system and to<br />
society in general, intertrochanteric fractures and femur neck<br />
fracture represents an epidemic disease 2 .<br />
In elderly, osteop<strong>or</strong>otic bones, a trivial fall is the cause <strong>of</strong><br />
90% <strong>of</strong> <strong>hip</strong> fractures 3 .<br />
C<strong>or</strong>responding Auth<strong>or</strong> :<br />
Dr. JPS Walia<br />
Pr<strong>of</strong>ess<strong>or</strong> <strong>of</strong> Orthopaedics<br />
19, Phulkian enclave, Patiala, <strong>Punjab</strong>.<br />
E-mail : doc_jpswalia@yahoo.co.in<br />
A typical patient with <strong>hip</strong> fracture is characterized by old<br />
age, severe osteop<strong>or</strong>osis and significant co-m<strong>or</strong>bid diseases.<br />
Primary aim <strong>of</strong> treatment should be to perf<strong>or</strong>m a surgery that<br />
provides the individual with greatest opp<strong>or</strong>tunity f<strong>or</strong> early<br />
ambulation 4 . This requirement is fulfilled to a great extent by<br />
use <strong>of</strong> a <strong>primary</strong> prosthetic replacement implant with <strong>or</strong> without<br />
cement. This technique allows early ambulation, thus avoids<br />
recumbency and its associated complications.<br />
We studied the results <strong>of</strong> 50 cases <strong>of</strong> extra capsular fracture<br />
neck femur in elderly patients treated with <strong>primary</strong> cemented<br />
<strong>bipolar</strong> <strong>arthroplasty</strong> <strong>or</strong> <strong>total</strong> <strong>hip</strong> replacement <strong>arthroplasty</strong><br />
(25 cases each).<br />
MATERIAL AND METHODS<br />
This study was conducted on 50 cases <strong>of</strong> extra capsular fractures<br />
<strong>of</strong> femur above the age group <strong>of</strong> 50 years.<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XII, No.1, 2011<br />
5<br />
PDF created with pdfFact<strong>or</strong>y Pro trial version www.pdffact<strong>or</strong>y.com
Walia et al<br />
Surgery was done under general <strong>or</strong> spinal anaesthesia<br />
depending upon the choice <strong>of</strong> anaesthesiologist. All patients<br />
were operated in lateral decubitus via posterolateral<br />
approach. The fascia was incised in line with the skin incision.<br />
After blunt dissection <strong>of</strong> gluteus maximus the gluteus medius<br />
was retracted to expose the sh<strong>or</strong>t external rotat<strong>or</strong> muscles <strong>of</strong><br />
the <strong>hip</strong>. The abduct<strong>or</strong>-greater trochanter-vastus lateralis<br />
complex was kept intact. Sh<strong>or</strong>t external rotat<strong>or</strong>s were divided<br />
close to their insertion and an inverted T shaped incision was<br />
made on the joint capsule. The fem<strong>or</strong>al neck was osteotomised<br />
and the fem<strong>or</strong>al head was removed. Patients were subjected to<br />
either hemi<strong>arthroplasty</strong>, with cemented <strong>bipolar</strong> prosthesis, <strong>or</strong><br />
<strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> depending upon condition <strong>of</strong> the<br />
acetabulum<br />
Hemi<strong>arthroplasty</strong> - Once the head-neck fragment has been<br />
removed the medullary canal <strong>of</strong> the femur is readily accessible.<br />
The canal was rasped with an appropriately sized broach and<br />
trial prosthesis was inserted. A helpful guide used f<strong>or</strong> the<br />
appropriate height <strong>of</strong> calcar reconstruction is the relations<strong>hip</strong><br />
between the centre <strong>of</strong> fem<strong>or</strong>al head and tip <strong>of</strong> the greater<br />
trochanter: It should be essentially coplanar. Although this<br />
may be difficult to assess in presence <strong>of</strong> trochanteric fracture,<br />
usually, the greater trochanter fragments are still somewhat<br />
attached and can be used as a gross guide f<strong>or</strong> evaluating the<br />
appropriate level f<strong>or</strong> prosthesis. Following an acceptable trail<br />
fit, leg length and <strong>hip</strong> stability are assessed. The head was redislocated<br />
and a permanent <strong>bipolar</strong> prosthesis was cemented<br />
into the femur at the proper level. After reduction the movements<br />
<strong>of</strong> the <strong>hip</strong> were checked.<br />
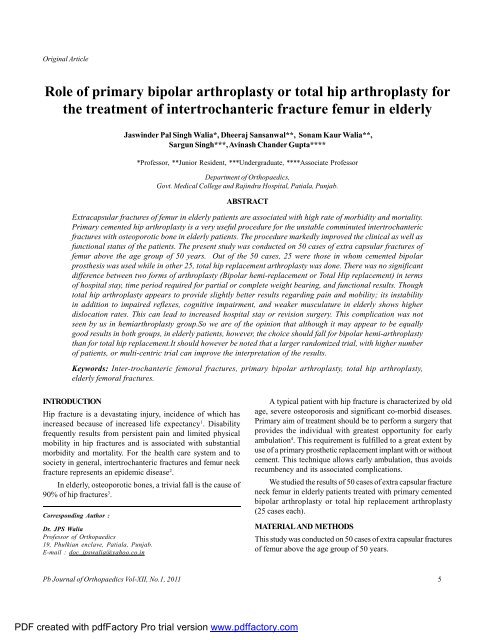
Figure 1: Pre and post operative X-ray <strong>of</strong> <strong>bipolar</strong> case<br />
Total Hip Replacement - The acetabulam was prepared by<br />
excising the ligamentum teres and removing the articular<br />
cartilage with acetabular reamer till raw cancellous bleeding<br />
bone was exposed. The fitting <strong>of</strong> the acetabular component<br />
was checked. Acetabular cup was placed in a position <strong>of</strong> 45-55 0<br />
abduction and 10-15 0 anteversion. Fem<strong>or</strong>al preparation was<br />
done as already mentioned above f<strong>or</strong> <strong>bipolar</strong> hemi<strong>arthroplasty</strong>.<br />
Trail reduction was done and s<strong>of</strong>t tissue tension<br />
checked. Following an acceptable trail fit, leg length and <strong>hip</strong><br />
stability are assessed. The head was re-dislocated and a<br />
permanent prosthesis was cemented into the femur at the<br />
proper level. After reduction the movements <strong>of</strong> the <strong>hip</strong> were<br />
checked.<br />
Figure 2: Pre and post operative X-ray <strong>of</strong> THR case<br />
Trochanteric reconstruction: Displaced trochanter was<br />
fixed acc<strong>or</strong>dingly as per geometry, comminution <strong>of</strong> fracture with<br />
the help <strong>of</strong> SS Wire <strong>or</strong> vicryl numbrt 1 reinf<strong>or</strong>ced with bone<br />
cement. Fem<strong>or</strong>al head was used f<strong>or</strong> reconstructing the medial<br />
bone loss wherever required.<br />
After reattachment <strong>of</strong> capsule and sh<strong>or</strong>t external rotat<strong>or</strong>s,<br />
closure in layers was done over drain.<br />
Physiotherapy was started on the first postoperative day.<br />
On the second postoperative day, patients were allowed<br />
to sit on the side <strong>of</strong> the bed <strong>or</strong> upright in a chair. Gait training<br />
was begun and weight-bearing was permitted earliest, as<br />
tolerated. As all the patients were elderly, they required a walker<br />
f<strong>or</strong> balance during gait training.<br />
Patients were discharged 5-12 days after surgery and were<br />
advised to continue physiotherapy until they could return to<br />
independent living.<br />
Patients were evaluated clinically acc<strong>or</strong>ding to the Harris<br />
<strong>hip</strong> sc<strong>or</strong>e 5 and Salvati-Wilson <strong>hip</strong> sc<strong>or</strong>e 6 in out-patient facilities<br />
at follow-ups.<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XII, No.1, 2011<br />
6<br />
PDF created with pdfFact<strong>or</strong>y Pro trial version www.pdffact<strong>or</strong>y.com
Bipolar <strong>or</strong> <strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> f<strong>or</strong> intertrochanteric fracture<br />
RESULTS<br />
A <strong>total</strong> <strong>of</strong> 50 elderly patients with intertrochanteric fractures<br />
underwent <strong>arthroplasty</strong> between 2008 and 2010. Mean followup<br />
duration was 21.8 months (range, 7-34months). No m<strong>or</strong>tality<br />
was noted. Mean age <strong>of</strong> patients was 69.04 years. Maximum<br />
number <strong>of</strong> patients was in the age group <strong>of</strong> 60-79 years<br />
comprising <strong>of</strong> 80% <strong>of</strong> <strong>total</strong> patients. In the <strong>bipolar</strong> group average<br />
age was 67.44 years, while in THR group average age was 70.64<br />
years. There were 38% female patients and 62% male patients.<br />
Patterns were similar in both the groups.<br />
In our Series 66% <strong>of</strong> intertrochanteric fractures were caused<br />
by min<strong>or</strong> trauma in the f<strong>or</strong>m <strong>of</strong> stumbling <strong>or</strong> fall on uneven<br />
surface and rest 34% cases by severe trauma in the f<strong>or</strong>m <strong>of</strong><br />
vehicular mot<strong>or</strong> accidents. Patterns were similar in two groups<br />
with min<strong>or</strong> trauma as cause in 60% in <strong>bipolar</strong> group and 72% in<br />
THR group.<br />
In present study, 64% cases were operated within 7 days<br />
<strong>of</strong> admission, 26% cases with in 8 to 15 days <strong>of</strong> admission and<br />
10% cases were operated after 15 days <strong>of</strong> admission in the<br />
hospital. The delay was mostly because <strong>of</strong> associated medical<br />
conditions. Hypertension was most common associated<br />
disease.<br />
The mean operative time in <strong>bipolar</strong> group was 50 minutes<br />
(range, 45-70 minutes). Average intraoperative blood loss<br />
was 120 ml (range, 90-25 0 ml) while in THR group mean<br />
operative time was 74 minutes (range, 60-100 minutes).<br />
Average intraoperative blood loss was 154 ml (range, 100-300<br />
ml).<br />
In Bipolar group 88% patients were allowed partial weight<br />
bearing within 7-14 days <strong>of</strong> operation 8% in third week and it<br />
was delayed till fourth week in one patient. In THR group 64%<br />
patients were allowed partial weight bearing within 7-14 days<br />
<strong>of</strong> operation 24% in third week and it was delayed till fourth<br />
week in 3 patients. Delayed weight bearing was due to<br />
comminution <strong>of</strong> fracture.<br />
In THR group 22 patients 88(%) were allowed full weight<br />
bearing within 4-6 weeks <strong>of</strong> operation. While in BIPOLAR group<br />
24 patients 96(%) were allowed full weight bearing within 4-6<br />
weeks <strong>of</strong> operation.<br />
At last follow-up in <strong>bipolar</strong> group, 3 cases (12%) had limp<br />
while walking. In THR group, only 2 cases (8%) had limp while<br />
walking.<br />
In THR series 2 cases had dislocations (8%), one happened<br />
after 2 weeks when patient slipped and fell; while in another<br />
case m<strong>or</strong>e than one year later in a road accident. Both were<br />
treated by closed reduction. This was followed by a 2-3 weeks<br />
period <strong>of</strong> immobilization with traction followed by guarded<br />
weight bearing. There were no dislocations in <strong>bipolar</strong> group.<br />
In our study <strong>of</strong> 50 cases outcome was excellent to good in<br />
all the cases as per Salvati and Wilson <strong>hip</strong> sc<strong>or</strong>e. Functional<br />
sc<strong>or</strong>es were slightly better in THR group (mean 34.16/40) when<br />
compared to <strong>bipolar</strong> group (33.60/40) but difference was not<br />
statistically significant (p value > 0.05).<br />
Mean Harris <strong>hip</strong> sc<strong>or</strong>e at final follow up was 82 in <strong>bipolar</strong><br />
group and 84.4 in THR group.<br />
DISCUSSION<br />
Hip fracture injuries are one <strong>of</strong> the most serious health care<br />
problems affecting elderly patients. There were an estimated<br />
1.66 million <strong>hip</strong> fractures w<strong>or</strong>ld-wide in 1990, this w<strong>or</strong>ldwide<br />
annual number will rise to 6.26 million by the year 2050 7,8 .<br />
In elderly the coexistence <strong>of</strong> unstable comminuted fracture<br />
with osteop<strong>or</strong>osis w<strong>or</strong>sen the prognosis 9,10 , which is attributed<br />
to presence <strong>of</strong> various co-m<strong>or</strong>bid conditions, which are<br />
exacerbated by immobility, bed rest and delayed weight<br />
bearing. In osteop<strong>or</strong>otic fractures, maintenance <strong>of</strong> reduction<br />
can be a maj<strong>or</strong> problem. Unsatisfact<strong>or</strong>y surgical outcome is<br />
common in elderly patients with intertrochanteric fractures;<br />
medical illness, osteop<strong>or</strong>osis, and fracture instability are<br />
contributing fact<strong>or</strong>s.<br />
The <strong>or</strong>thopaedic literature concerning the treatment<br />
and results <strong>of</strong> comminuted intertrochanteric fractures <strong>of</strong> the<br />
<strong>hip</strong> by Massie (1962) 11 , Holt (1963) 12 and Dimon (1973) 13 have<br />
shown outstanding w<strong>or</strong>k in an attempt to change an unstable<br />
fracture to a stable one and fix it with a specific device until it<br />
heals.<br />
Davis et al (1990) 9 studied the causes <strong>of</strong> mechanical<br />
failure in a series <strong>of</strong> 230 intertrochanteric fractures which had<br />
been internally fixed with either sliding <strong>hip</strong> screw <strong>or</strong> Kuntscher<br />
y-nail. The overall rate <strong>of</strong> mechanical failure was 16.5%.<br />
Kyle et al (1979) 14 rep<strong>or</strong>ting on a series <strong>of</strong> 74 unstable<br />
intertrochanteric fractures, had a post nailing complication rate<br />
<strong>of</strong> 6% to 8% and they could not ambulate their patients as late<br />
as four to six weeks due to the unstable nature <strong>of</strong> the implant<br />
bone construct. Hayward et al (1983) 15 rep<strong>or</strong>ted a failure rate <strong>of</strong><br />
35% using a nail plate combination and a failure rate <strong>of</strong> 37.5%<br />
using Enders nails.<br />
Kim et al (2001) 16 reviewed 178 intertrochanteric fractures<br />
treated by dynamic <strong>hip</strong> screw (DHS) fixation followed f<strong>or</strong> a<br />
minimum <strong>of</strong> one year. Unstable fractures with osteop<strong>or</strong>osis<br />
had a failure rate <strong>of</strong> m<strong>or</strong>e than 50%. They concluded in such<br />
cases, DHS should not be the first choice f<strong>or</strong> treatment.<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XII, No.1, 2011<br />
7<br />
PDF created with pdfFact<strong>or</strong>y Pro trial version www.pdffact<strong>or</strong>y.com
Walia et al<br />
Reoperation rates have been rep<strong>or</strong>ted as high as 8-16%<br />
with internal fixation in intertrochanteric fractures 17,18 .<br />
Furtherm<strong>or</strong>e, repeat surgery in these patients carries with it a<br />
high incidence <strong>of</strong> medical complications and post operative<br />
dislocation <strong>of</strong> the prosthesis has also been shown to be<br />
somewhat m<strong>or</strong>e common 19 .<br />
From the above review <strong>of</strong> literature, it is evident that<br />
although the use <strong>of</strong> internal fixation has decreased the m<strong>or</strong>tality<br />
rate, the rate <strong>of</strong> complication still ranges from 4-50% 16 and<br />
walking with full weight bearing bef<strong>or</strong>e the fracture has healed<br />
is <strong>of</strong>ten impossible.<br />
There is no doubt that the general consensus would be to<br />
use internal fixation devices in stable intertrochanteric fractures<br />
in younger patients as they can tolerate immobilization and if<br />
needed, reoperation, quite well. However this is not so in elderly,<br />
debilitated patients who sustain an unstable intertrochanteric<br />
fracture.<br />
Primary <strong>arthroplasty</strong> has been advocated in elderly patients<br />
with a view to make the rehabilitation early and to lessen the<br />
incidence <strong>of</strong> complications <strong>of</strong> prolonged immobilization which<br />
are frequently encountered in the treatment with various f<strong>or</strong>ms<br />
<strong>of</strong> internal fixation devices e.g. venous thrombosis, pulmonary<br />
embolism, atelactasis and allied complications. The maj<strong>or</strong><br />
advantage <strong>of</strong> treatment with cemented endoprosthesis is the<br />
early weight bearing and the rehabilitation <strong>of</strong> these elderly<br />
patients to their pre-fractures level m<strong>or</strong>e quickly than is achieved<br />
with various fixation devices.<br />
Multiple studies 20,21,22 showed that unstable three <strong>or</strong> four<br />
part <strong>hip</strong> fractures can be treated with a standard fem<strong>or</strong>al stem<br />
prosthesis and circlage wiring <strong>of</strong> the trochanters. This technique<br />
allows safe early weight bearing on the injured <strong>hip</strong> and had a<br />
relatively low rate <strong>of</strong> complications.<br />
A maj<strong>or</strong> complication associated with <strong>arthroplasty</strong> is high<br />
rate <strong>of</strong> dislocation 23 . Associated with the dislocations was a<br />
much higher incidence <strong>of</strong> pressure s<strong>or</strong>es and pulmonary<br />
complications 24 . But use <strong>of</strong> <strong>bipolar</strong> <strong>arthroplasty</strong> instead <strong>of</strong><br />
<strong>total</strong> <strong>hip</strong> replacements can reduce this complication to an<br />
acceptable rate 25 . Haentjens et al 26 and Geiger et al 27 separately<br />
rep<strong>or</strong>ted results <strong>of</strong> <strong>arthroplasty</strong> in intertrochanteric fractures.<br />
In their studies dislocation rate in the patient group who<br />
underwent <strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> was significantly higher<br />
(12% to 44.5%) than those who had <strong>bipolar</strong> <strong>arthroplasty</strong><br />
(0 to 3.3%).<br />
In our study, there was no significant difference between<br />
two f<strong>or</strong>ms <strong>of</strong> <strong>arthroplasty</strong> (<strong>bipolar</strong> hemi-replacement <strong>or</strong> <strong>total</strong><br />
<strong>hip</strong> replacement) in terms <strong>of</strong> hospital stay, time period required<br />
f<strong>or</strong> partial <strong>or</strong> complete weight bearing, and functional<br />
results.<br />
Though <strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> appears to provide slightly<br />
better results regarding pain and mobility;however, its<br />
instability in addition to impaired reflexes, cognitive impairment,<br />
and weaker musculature in elderly patients shows higher<br />
dislocation rates (8%). This leads to increased hospital stay <strong>or</strong><br />
revision surgery. This complication was not seen with <strong>bipolar</strong><br />
hemi-<strong>arthroplasty</strong>.<br />
So we are <strong>of</strong> opinion that although at the outset, it may<br />
appear that the results are equally good in both the groups, in<br />
elderly patients choice should fall f<strong>or</strong> <strong>bipolar</strong> hemi-<strong>arthroplasty</strong><br />
than f<strong>or</strong> Total <strong>hip</strong> replacement.<br />
REFERENCES<br />
1. Melton LJ, 3rd. Epidemiology <strong>of</strong> <strong>hip</strong> fractures: implications <strong>of</strong> the<br />
exponential increase with age. Bone 1996; 18:121s-125s.<br />
2. Melton LJ, 3rd. Hip fractures: A w<strong>or</strong>ldwide problem today and<br />
tom<strong>or</strong>row. Bone 1993; 14 Suppl 1: s1-8.<br />
3. Alffram PA. An epidemiologic study <strong>of</strong> cervical and trochanteric<br />
fractures <strong>of</strong> the femur in an urban population with special reference<br />
to etiologic fact<strong>or</strong>s. Acta Orthop Scand 1964; 65: 9-109.<br />
4. Stern MB and goldstein TB. The use <strong>of</strong> leinbach prosthesis in<br />
intertrochantric fractures <strong>of</strong> <strong>hip</strong>. Clin Orthop 1977; 128; 325-9.<br />
5. Harris WH. Traumatic arthritis <strong>of</strong> the <strong>hip</strong> after dislocation and<br />
acetabular fractures: treatment by mold <strong>arthroplasty</strong>. An end-result<br />
study using a new method <strong>of</strong> result evaluation. J Bone Joint Surg<br />
Am. 1969 Jun; 51(4):737-55.<br />
6. Salvati EA, Wilson PD (1973) long term results <strong>of</strong> fem<strong>or</strong>al head<br />
replacement. J Bone Joint Surg Am 55a:516-524<br />
7. Parker M, Johansen A. Clinical review. Hip fracture. Bmj. 2006;<br />
333: 27-30.<br />
8. Kannus P, Parkkari J, Sievänen H, heinonen A, Vu<strong>or</strong>i I, Järvinen M.<br />
Epidemiology <strong>of</strong> <strong>hip</strong> fractures. Bone. 1996 Jan; 18(1 Suppl):<br />
57s-63s.<br />
9. Davis TR, Sher JL, H<strong>or</strong>sman A et al (1990) intertrochanteric fem<strong>or</strong>al<br />
fractures. Mechanical failure after internal fixation. J Bone Joint<br />
Surg Br 72:26-31.<br />
10. Mariani EM and Rand JA. Non-union <strong>of</strong> intertrochanteric fractures<br />
<strong>of</strong> femur following open reduction and internal fixation <strong>of</strong><br />
intertrochanteric and subtrochanteric fractures in the elderly patient.<br />
Acta Orthop Belg 1994; 60 (1): 11-3...<br />
11. Massie WK. Extra capsular fractures <strong>of</strong> the <strong>hip</strong> treated by impaction<br />
using sliding nail plate fixation. Clin Orthop 1962; 22:180.<br />
12. Holt EP JR. Hip fractures <strong>of</strong> the trochanteric region; treatment<br />
with a strong nail and early weight bearing. J Bone Joint Surg 1963;<br />
45:687.<br />
13. Dimon JH. The unstable intertrochanteric fracture. Clin Orthop<br />
1973; 92:100-107.<br />
14. Davis TR, Sher JL, H<strong>or</strong>sman A et al (1990) intertrochanteric fem<strong>or</strong>al<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XII, No.1, 2011<br />
8<br />
PDF created with pdfFact<strong>or</strong>y Pro trial version www.pdffact<strong>or</strong>y.com
Bipolar <strong>or</strong> <strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> f<strong>or</strong> intertrochanteric fracture<br />
fractures. Mechanical failure after internal fixation. J Bone Joint<br />
Surg Br 72:26-31.<br />
15. Kyle RF, Gustiolo RB, Premer RF. Analysis <strong>of</strong> six hundred and<br />
twenty two intertrochanteric <strong>hip</strong> fractures. A retrospective and<br />
prospective study. J Bone Joint Surg 1979; 61:219-221.<br />
16. Hayward SJ, Lowe Lw, Tzeueleros S. Intertrochanteric fractures<br />
comparison between fixation with a two piece nail plate and enders<br />
nail. Int Orthop 1983; 7:153.<br />
17. Kim WY, Han CH, park JI, Kim JY (2001) failure <strong>of</strong><br />
intertrochanteric fracture fixation with a dynamic <strong>hip</strong> screw in<br />
relation to pre-operative fracture stability and osteop<strong>or</strong>osis. Int<br />
Orthop 25:360-362.<br />
18. Laros GS and Moo<strong>or</strong>e JF complications <strong>of</strong> fixation in joint fractures.<br />
Clin <strong>or</strong>thop 1947; 101: 110-9.<br />
19. Chapman MW, Bowman WE, Csongradi JJ et al. The use <strong>of</strong> enders<br />
pins in extracapsular fractures <strong>of</strong> the <strong>hip</strong>. J Bone Joint Surg 1981;<br />
65:14-28.<br />
20. Mehlh<strong>of</strong>f T, Landon GC, Tullos HS. Total <strong>hip</strong> <strong>arthroplasty</strong><br />
following failed internal fixation <strong>of</strong> <strong>hip</strong> fractures. Clin Orthop<br />
1991; 269:32-37.<br />
21. Zhang Q, Pang Q, Huang T, GE A, Tang T, Chen l. The clinical<br />
effect <strong>of</strong> <strong>bipolar</strong> long-stem prosthetic replacement on the treatment<br />
<strong>of</strong> comminuted intertrochanteric fracture <strong>of</strong> <strong>hip</strong> in the elderly<br />
osteop<strong>or</strong>otic patients. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi<br />
2005 Mar; 19(3):198-200.<br />
22. Van Loon CJ, De Wall Malefijt MC, Veth RP. Primary treatment <strong>of</strong><br />
unstable pertrochantric fem<strong>or</strong>al fracture using a head-neck<br />
prosthesis in elderly patients. Ned Tijdschr Geneeskd. 1994 Sept.<br />
3; 138(36):1810-3.<br />
23. Grimsrud C, Monzon RJ, Richman J, Ries MD. Cemented <strong>hip</strong><br />
<strong>arthroplasty</strong> with a novel cerclage cable technique f<strong>or</strong> unstable<br />
intertrochanteric <strong>hip</strong> fractures. J Arthroplasty 2005 Apr; 20(3):337-<br />
43.<br />
24. Haentjens P, Casteleyn P, Deboeck H. Treatment <strong>of</strong> unstable<br />
intertrchanteric and subtrochanteric fractures in elderly patientsprimay<br />
<strong>bipolar</strong> <strong>arthroplasty</strong> compared with internal fixation.<br />
J Bone Joint Surg 1989; 71A:1214-25.<br />
25. Haentjens P., G. Lamraski endoprosthetic replacement <strong>of</strong> unstable,<br />
comminuted intertrochanteric fracture <strong>of</strong> the femur in the elderly,<br />
osteop<strong>or</strong>otic patient: a review. Disability & rehabilitation Jan 2005,<br />
Vol. 27, No. 18-19:1167-1180.<br />
26. Rodop O, Kiral A, Kaplan H, Akmaz I (2002) Primary <strong>bipolar</strong><br />
hemiprosthesis f<strong>or</strong> unstable intertrochanteric fractures. Int Orthop<br />
26:233-237<br />
27. F. Geiger, M. Zimmermann-stenzel, C. Heisel, B. Lehner, W. Daecke<br />
trochanteric fractures in the elderly: the influence <strong>of</strong> <strong>primary</strong> <strong>hip</strong><br />
<strong>arthroplasty</strong> on 1-year m<strong>or</strong>tality Arch Orthop Trauma Surg (2007)<br />
127:959-966<br />
28. Haentjens P, Casteleyn PP, Opdecam P (1989) Primary <strong>bipolar</strong><br />
<strong>arthroplasty</strong> <strong>or</strong> <strong>total</strong> <strong>hip</strong> <strong>arthroplasty</strong> f<strong>or</strong> the treatment <strong>of</strong> unstable<br />
intertrochanteric and subtrochanteric fractures in elderly patients.<br />
Acta Orthop Belg 60(Suppl 1):124-128<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XII, No.1, 2011<br />
9<br />
PDF created with pdfFact<strong>or</strong>y Pro trial version www.pdffact<strong>or</strong>y.com