Role of locking compression plate in long bone fractures in adults - a ...
Role of locking compression plate in long bone fractures in adults - a ...
Role of locking compression plate in long bone fractures in adults - a ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Role</strong> <strong>of</strong> <strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong> <strong>in</strong> <strong>long</strong> <strong>bone</strong> <strong>fractures</strong><br />
<strong>in</strong> <strong>adults</strong> - a study <strong>of</strong> 50 cases<br />
JPS Walia MS*, Av<strong>in</strong>ash Gupta MS**, Girish Sahni MS***, Gagandeep Gupta MBBS****,<br />
Sonam Kaur Walia MBBS*****<br />
*Pr<strong>of</strong>essor, **Associate Pr<strong>of</strong>essor, ***Senior Resident, ****Junior Resident, *****Intern<br />
Department <strong>of</strong> Orthopaedics,<br />
Government Medical College, Patiala<br />
ABSTRACT<br />
In the modern world with <strong>in</strong>crease <strong>in</strong> speed and fast mov<strong>in</strong>g vechicles, there has been a cont<strong>in</strong>ous upsurge<br />
<strong>in</strong> the number as well as the severity <strong>of</strong> high energy <strong>fractures</strong>. Implants like Lc-Dcp and more recently the<br />
<strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong> helps to achieve satisfactory results <strong>in</strong> these cases. The present study was conducted<br />
to evaluate the results <strong>of</strong> Lock<strong>in</strong>g Compression Plate <strong>in</strong> 50 cases <strong>of</strong> <strong>long</strong> <strong>bone</strong> <strong>fractures</strong>(25 femur , 15 tibia,<br />
10 humerus <strong>fractures</strong>) admitted at GMC, Raj<strong>in</strong>dra Hospital, Patiala. The age group <strong>of</strong> patients <strong>in</strong> the study<br />
varied between 18 – 70 years. The <strong>fractures</strong> were 60 % closed and 40 % open <strong>in</strong> nature. Patients were<br />
evaluated and <strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong> was done under general,sp<strong>in</strong>al,epidural anesthesia. The patients<br />
were evaluated periodically both cl<strong>in</strong>ically and radiologically. 72 % <strong>of</strong> our cases achieved excellent to<br />
good results.<br />
Keywords : Lock<strong>in</strong>g <strong>compression</strong> <strong>plate</strong>, <strong>long</strong> <strong>bone</strong> <strong>fractures</strong>.<br />
INTRODUCTION<br />
Conventional <strong>plate</strong> and screw osteosynthesis has proved to<br />
be very successful <strong>in</strong> fracture fixation. These techniques require<br />
<strong>compression</strong> <strong>of</strong> the <strong>plate</strong> to the <strong>bone</strong> and rely on friction at the<br />
<strong>bone</strong>-<strong>plate</strong> <strong>in</strong>terface. This biomechanical prerequisite <strong>of</strong><br />
conventional <strong>plate</strong>s is associated with biological pitfalls due<br />
to <strong>compression</strong> <strong>of</strong> periosteal blood supply and compromise <strong>of</strong><br />
the vascularity <strong>of</strong> the fracture. With <strong>in</strong>creas<strong>in</strong>g axial load<strong>in</strong>g<br />
cycles, the screws can beg<strong>in</strong> to toggle, which decreases the<br />
friction force and leads to <strong>plate</strong> loosen<strong>in</strong>g. If this occurs<br />
prematurely, fracture <strong>in</strong>stability will occur, lead<strong>in</strong>g to implant<br />
failure. Thus, the more difficult it is to achieve and<br />
ma<strong>in</strong>ta<strong>in</strong> tight screw fixation (as for example, <strong>in</strong> metaphyseal<br />
and osteoporotic <strong>bone</strong>), the more difficult it is to ma<strong>in</strong>ta<strong>in</strong><br />
stability 1 .<br />
A newer concept <strong>of</strong> <strong>in</strong>ternal fixation, the <strong>lock<strong>in</strong>g</strong><br />
<strong>compression</strong> <strong>plate</strong> (LCP) was <strong>in</strong>troduced to overcome the<br />
drawbacks <strong>of</strong> conventional plat<strong>in</strong>g systems. This system<br />
Correspond<strong>in</strong>g Author:<br />
Dr JPS Walia, Pr<strong>of</strong>essor<br />
Department <strong>of</strong> Orthopaedics,<br />
Government Medical College, Patiala.<br />
E-mail : doc_jpswalia@yahoo.co.<strong>in</strong><br />
provides angular stability through the use <strong>of</strong> <strong>lock<strong>in</strong>g</strong> screws . 2<br />
The LCP system consists <strong>of</strong> a range <strong>of</strong> anatomically shaped<br />
<strong>plate</strong>s with specially designed comb<strong>in</strong>ation holes. The unique<br />
design <strong>of</strong> these comb<strong>in</strong>ation holes allows the system to be<br />
used both as a conventional <strong>compression</strong> <strong>plate</strong> and as a locked<br />
<strong>in</strong>ternal fixator; it also allows <strong>in</strong>ternal fixation with a comb<strong>in</strong>ation<br />
<strong>of</strong> conventional and <strong>lock<strong>in</strong>g</strong> head screws 3 . This is particularly<br />
valuable <strong>in</strong> cases <strong>of</strong> epimetaphyseal <strong>fractures</strong>. The system<br />
therefore has a broad range <strong>of</strong> potential <strong>in</strong>dications, <strong>in</strong>clud<strong>in</strong>g<br />
<strong>compression</strong> fixation <strong>of</strong> simple <strong>fractures</strong> and bridg<strong>in</strong>g <strong>of</strong><br />
comm<strong>in</strong>uted <strong>fractures</strong> 4 .<br />
This paper is a prospective study <strong>of</strong> use <strong>of</strong> <strong>lock<strong>in</strong>g</strong><br />
<strong>compression</strong> <strong>plate</strong>s <strong>in</strong> <strong>long</strong> <strong>bone</strong> <strong>fractures</strong>, which would have<br />
been associated with high rates <strong>of</strong> failure us<strong>in</strong>g conventional<br />
plat<strong>in</strong>g techniques.<br />
MATERIAL AND METHODS<br />
The present prospective study was done on patients with <strong>long</strong><br />
<strong>bone</strong> <strong>fractures</strong> admitted <strong>in</strong> our hospital. All patients were<br />
evaluated cl<strong>in</strong>ically and radiographically at the time <strong>of</strong><br />
admission. Fracture patterns like comm<strong>in</strong>uted <strong>fractures</strong>,<br />
metaphyseal <strong>fractures</strong> and <strong>fractures</strong> <strong>in</strong> osteoporotic <strong>bone</strong>s were<br />
chosen for LCP fixation. Anterior/Anterolateral approach with/<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XI, No.1, 2009<br />
41
Walia et al<br />
without radial nerve exploration for humerus and lateral<br />
approach for fracture shaft femur was taken. Fracture tibia was<br />
approached anterolaterally. All the <strong>fractures</strong> were fixed with<br />
LCPs tak<strong>in</strong>g care to protect the periosteal blood supply. Bone<br />
graft<strong>in</strong>g was done <strong>in</strong> old ununited <strong>fractures</strong> and <strong>in</strong> fresh cases<br />
with fracture comm<strong>in</strong>ution <strong>of</strong> high grade. Internal fixation <strong>in</strong><br />
open <strong>fractures</strong> was carried out after thorough irrigation and<br />
debridement. Spl<strong>in</strong>tage and immobilization was applied as per<br />
fixation achieved. Early range <strong>of</strong> motion exercises were started<br />
where a stable construct was achieved.<br />
RESULT<br />
Table 1<br />
Fracture Location<br />
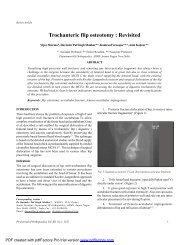
Fig. 1: LCP <strong>in</strong> tibia Preoperative and post-operative Xrays<br />
No. Fresh Non-union<br />
Closed Open<br />
Femur 25 19 4 2<br />
Tibia 15 6 5 4<br />
Humerus 10 5 1 4<br />
60% <strong>of</strong> cases were <strong>of</strong> closed nature. All 4 femur open <strong>fractures</strong><br />
were Gustillo Grade III open while 1 tibial and I humeral fracture<br />
was grade III. Four tibial <strong>fractures</strong> were grade 1 open. 20% <strong>of</strong><br />
cases were old ununited <strong>fractures</strong>.<br />
The age group <strong>of</strong> the patients <strong>in</strong> this study varied between<br />
18-70 years (average 53.1 years) with majority <strong>of</strong> the patients <strong>in</strong><br />
fifth to seventh decade <strong>of</strong> life.<br />
Follow-up <strong>in</strong> our series ranged from 6-24 months.<br />
All <strong>fractures</strong> united <strong>in</strong> this series without the need<br />
for any supplemental procedure. The average time for union <strong>in</strong><br />
fresh femur <strong>fractures</strong> was 16.4 weeks. 2 <strong>of</strong> the 4 open <strong>fractures</strong><br />
and 1 <strong>of</strong> 2 non-unions <strong>in</strong> femur took more than 20 weeks to<br />
unite.<br />
The average time for union <strong>of</strong> fresh tibial <strong>fractures</strong> was<br />
17.1 weeks while the non-unions united <strong>in</strong> an average <strong>of</strong> 17.75<br />
weeks. The average time <strong>of</strong> union for fresh humeral <strong>fractures</strong><br />
was 13.3 weeks. The union time <strong>in</strong> non unions ranged from 12<br />
to 20 weeks with a mean <strong>of</strong> 15.25 weeks<br />
Full weight bear<strong>in</strong>g <strong>in</strong> cases <strong>of</strong> fracture tibia and femur<br />
was done <strong>in</strong> 14 cases with<strong>in</strong> 12-16 weeks, 20 cases with<strong>in</strong> 17-20<br />
weeks and <strong>in</strong> 2 cases after 20 weeks.<br />
Range <strong>of</strong> motion at knee <strong>in</strong> femoral <strong>fractures</strong> was more<br />
than 90 degrees <strong>in</strong> 90% <strong>of</strong> the cases. Range <strong>of</strong> abduction was<br />
more than 140 degrees <strong>in</strong> 80 % <strong>of</strong> the cases with fracture shaft<br />
humerus and elbow flexion was more than 90 degrees <strong>in</strong> 85% <strong>of</strong><br />
the cases.<br />
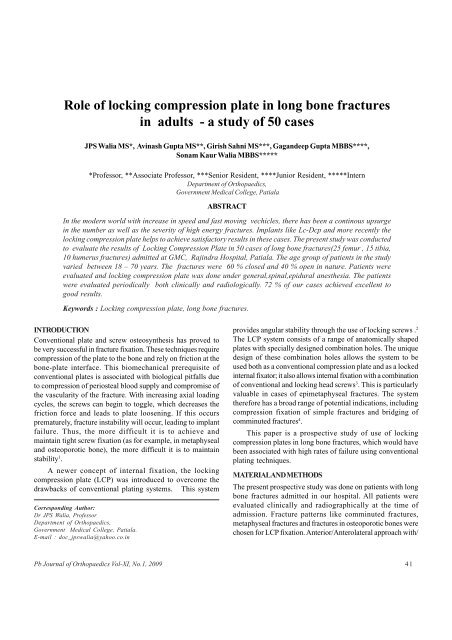
Fig. 2: LCP <strong>in</strong> femur pre and post operativeX rays<br />
Fig. 3: Three months follow up X ray <strong>of</strong> proximal humerus fracture<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XI, No.1, 2009<br />
42
<strong>Role</strong> <strong>of</strong> <strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong> <strong>in</strong> <strong>long</strong> <strong>bone</strong> <strong>fractures</strong> <strong>in</strong> <strong>adults</strong><br />
2 cases had wound <strong>in</strong>fection problems which healed with<br />
antibiotics and local wound care. Shorten<strong>in</strong>g was present <strong>in</strong><br />
one case that was operated more than 40 days after <strong>in</strong>jury with<br />
considerable fibrosis and overlapp<strong>in</strong>g <strong>of</strong> fragments; shorten<strong>in</strong>g<br />
was done <strong>in</strong> this case to achieve <strong>compression</strong> at the fracture<br />
site.<br />
Results were unsatisfactory <strong>in</strong> 2 cases <strong>of</strong> fracture humerus<br />
as both <strong>of</strong> them were hav<strong>in</strong>g concomitant <strong>in</strong>jury to the ipsilateral<br />
elbow, which hampered early rehabilitation.<br />
Evaluation <strong>of</strong> the results <strong>of</strong> fracture femur and tibia was<br />
done by Modified Mehrotra’s grad<strong>in</strong>g. Accord<strong>in</strong>g to this<br />
grad<strong>in</strong>g, 72% <strong>of</strong> the cases achieved excellent results, 20% fair<br />
and 8% poor. In case with humerus <strong>fractures</strong> achieved 80%<br />
satisfactory and 20% unsatisfactory.<br />
DISCUSSION<br />
Lock<strong>in</strong>g <strong>compression</strong> <strong>plate</strong>s have been designed to overcome<br />
the pitfalls <strong>of</strong> conventional <strong>plate</strong>s particularly when deal<strong>in</strong>g<br />
with difficult problems such as comm<strong>in</strong>uted, metaphyseal and<br />
osteoporotic <strong>fractures</strong>. Locked <strong>plate</strong>s have become an attractive<br />
alternative to conventional <strong>plate</strong>s as they can be used as “bridge<br />
<strong>plate</strong>s” to preserve fragmentary blood supply, they provide<br />
fixed angular stability with the potential for improved fixation<br />
<strong>in</strong> osteoporotic <strong>bone</strong>, and they reduce the risk <strong>of</strong> primary loss<br />
<strong>of</strong> reduction as exact <strong>plate</strong>-contour<strong>in</strong>g is not required 5<br />
Wagner(2003) <strong>in</strong> his paper on general pr<strong>in</strong>ciples for the<br />
cl<strong>in</strong>ical use <strong>of</strong> <strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong>, made comment that<br />
Internal fixator (A term used for <strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong>s) is<br />
a construct <strong>in</strong> which the screws (P<strong>in</strong>s/Bolts) are locked <strong>in</strong> the<br />
<strong>plate</strong> (Frame). Forces are transferred from the <strong>bone</strong> to the screw<br />
<strong>plate</strong> threaded connection. Rigid <strong>compression</strong> <strong>of</strong> the Plate on<br />
the <strong>bone</strong> is therefore not required to achieve stability. Lock<strong>in</strong>g<br />
the screw <strong>in</strong> the <strong>in</strong>ternal fixator <strong>in</strong>creases the stability, and the<br />
risk <strong>of</strong> loss <strong>of</strong> reduction due to the toggl<strong>in</strong>g <strong>of</strong> the screws is<br />
elim<strong>in</strong>ated 3 .<br />
Numerous case series have reported the successful use <strong>of</strong><br />
LCPs <strong>in</strong> a variety <strong>of</strong> cl<strong>in</strong>ical situations such as metaphyseal<br />
<strong>fractures</strong>, <strong>in</strong>traarticular <strong>fractures</strong>, <strong>fractures</strong> <strong>in</strong> osteoporotic<br />
<strong>bone</strong>s as well as difficult non-unuions 6-10.<br />
In our study, we found that the implant with <strong>lock<strong>in</strong>g</strong> head<br />
screw, when used <strong>in</strong> difficult <strong>fractures</strong> like type C3 provided<br />
good fixation. Even <strong>in</strong> osteoporotic <strong>bone</strong>s, the <strong>lock<strong>in</strong>g</strong> implant<br />
provided good anchorage. With locked fixation, a good<br />
purchase is achieved between the threaded <strong>plate</strong> and threaded<br />
screw head. The screws virtually act as pegs resist<strong>in</strong>g axial<br />
rotation, translation and bend<strong>in</strong>g, <strong>in</strong> porotic <strong>bone</strong> 10 . In our<br />
study we found that we could achieve union <strong>in</strong> all the nonunions<br />
and comm<strong>in</strong>uted <strong>fractures</strong>. This compares well to the<br />
reported results <strong>in</strong> literatures 11.12 .<br />
In conclusion, it can be said that, if biomechanical pr<strong>in</strong>ciples<br />
are followed, <strong>lock<strong>in</strong>g</strong> <strong>plate</strong>s provide excellent fixation <strong>in</strong> difficult<br />
situations like comm<strong>in</strong>uted <strong>fractures</strong>, osteoporotic <strong>fractures</strong><br />
and periarticular <strong>fractures</strong>.<br />
REFERENCES<br />
1. Smith WR, Ziran BH, Anglen JO and Stahel PF:Lock<strong>in</strong>g <strong>plate</strong>s: tips<br />
and tricks. J Bone Jo<strong>in</strong>t Surg Am 2007; 89:2298-2307<br />
2. Wagner,M. General pr<strong>in</strong>ciples for the cl<strong>in</strong>ical use <strong>of</strong> LCP. Injury<br />
2003; 34 suppl. 2; B 31-42.<br />
3. Frigg R. Lock<strong>in</strong>g <strong>compression</strong> <strong>plate</strong> (LCP). An osteosynthesis <strong>plate</strong><br />
based on the Dynamic Compression Plate and the Po<strong>in</strong>t Contact<br />
Fixator (PC-Fix). Injury. 2001; 32(suppl 2):63–66.<br />
4. Gautier E, Sommer C. Guidel<strong>in</strong>es for the cl<strong>in</strong>ical application <strong>of</strong> the<br />
LCP. Injury. 2003; 34(suppl 2):63–77.<br />
5. Kubiak EN, Fulkerson E, Strauss E and Egol KA : The Evolution <strong>of</strong><br />
Locked Plates: JBJS Am 2006 ;88:189-200.<br />
6. Bjorkenheim JM et al ,Internal fixation <strong>of</strong> proximal humeral<br />
<strong>fractures</strong> us<strong>in</strong>g <strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong>. Acta orthop scand:<br />
75(6)741-745 .<br />
7. Egol et al .Biomechanics <strong>of</strong> <strong>lock<strong>in</strong>g</strong> <strong>compression</strong> <strong>plate</strong>s. J orthop<br />
trauma2004;18;488-493.<br />
8. Fankhauser et al .A new <strong>lock<strong>in</strong>g</strong> <strong>plate</strong> for treatment <strong>of</strong> proximal<br />
humeral <strong>fractures</strong>. Cl<strong>in</strong>ical orthop related research 2005;430;176-<br />
181.<br />
9. Fulkerson et al;Fixation <strong>of</strong> the diaphyseal <strong>fractures</strong> with a segmental<br />
defect ; A biomechanical comparison between <strong>lock<strong>in</strong>g</strong> <strong>compression</strong><br />
<strong>plate</strong> and the conventional <strong>plate</strong>s;J orthop trauma2005;19;597-<br />
603.<br />
10. Shah Alam Khan, Prasoon Shamshery, Vikas Gupta,Vivek Trikha,<br />
Manish Kumar Varshney and Ashok Kumar :Lock<strong>in</strong>g Compression<br />
Plate <strong>in</strong> Long Stand<strong>in</strong>g ClavicularNonunions With Poor Bone Stock:<br />
J Trauma. 2008;64:439–441.<br />
11. R<strong>in</strong>g D, Kloen P, Kadzielski J, Helfet D, Jupiter JB. Lock<strong>in</strong>g<br />
<strong>compression</strong> <strong>plate</strong>s for osteoporotic nonunions <strong>of</strong> the diaphyseal<br />
humerus. Cl<strong>in</strong> Orthop Relat Res. 2004;425:50-4.<br />
12. Wenzl ME, Porte T, Fuchs S, Fasch<strong>in</strong>gbauer M, Jurgens C. Delayed<br />
and nonunion <strong>of</strong> the humeral diaphysis—<strong>compression</strong> <strong>plate</strong> or<br />
<strong>in</strong>ternal <strong>plate</strong> fixator Injury. 2004;35:55-60.<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XI, No.1, 2009<br />
43