NASSAU COMMUNITY COLLEGE
NASSAU COMMUNITY COLLEGE
NASSAU COMMUNITY COLLEGE

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
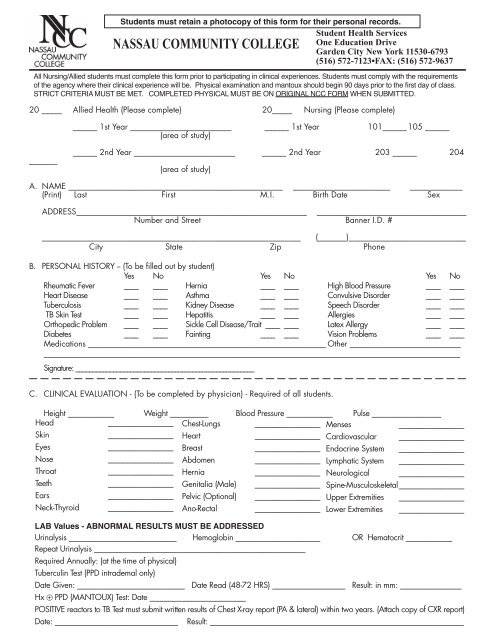
Students must retain a photocopy of this form for their personal records.<br />
Student Health Services<br />
One Education Drive<br />
Garden City New York 11530-6793<br />
(516) 572-7123•FAX: (516) 572-9637<br />
<strong>NASSAU</strong> <strong>COMMUNITY</strong> <strong>COLLEGE</strong><br />
All Nursing/Allied students must complete this form prior to participating in clinical experiences. Students must comply with the requirements<br />
of the agency where their clinical experience will be. Physical examination and mantoux should begin 90 days prior to the first day of class.<br />
STRICT CRITERIA MUST BE MET. COMPLETED PHYSICAL MUST BE ON ORIGINAL NCC FORM WHEN SUBMITTED.<br />
20 _____ Allied Health (Please complete) 20_____ Nursing (Please complete)<br />
______ 1st Year _________________________ ______ 1st Year 101______ 105 ______<br />
(area of study)<br />
_______<br />
______ 2nd Year _________________________ ______ 2nd Year 203 ______ 204<br />
(area of study)<br />
A. NAME _____________________________________________________ ________________________ _____________<br />
(Print) Last First M.I. Birth Date Sex<br />
ADDRESS_________________________________________________________ _____________________________________<br />
Number and Street Banner I.D. #<br />
________________________________________________________________ (_______)_____________________________<br />
City State Zip Phone<br />
B. PERSONAL HISTORY -- (To be filled out by student)<br />
Yes No Yes No Yes No<br />
Rheumatic Fever ____ ____ Hernia ____ ____ High Blood Pressure ____ ____<br />
Heart Disease ____ ____ Asthma ____ ____ Convulsive Disorder ____ ____<br />
Tuberculosis ____ ____ Kidney Disease ____ ____ Speech Disorder ____ ____<br />
⊕TB Skin Test ____ ____ Hepatitis ____ ____ Allergies ____ ____<br />
Orthopedic Problem ____ ____ Sickle Cell Disease/Trait ____ ____ Latex Allergy ____ ____<br />
Diabetes ____ ____ Fainting ____ ____ Vision Problems ____ ____<br />
Medications ____________________________________________________________ Other ____________________________<br />
________________________________________________________________________________________________________<br />
Signature: ____________________________________________________<br />
C. CLINICAL EVALUATION - (To be completed by physician) - Required of all students.<br />
Height ____________ Weight __________ Blood Pressure ____________ Pulse __________________<br />
Head<br />
_________________ Chest-Lungs _________________ Menses<br />
_________________<br />
Skin<br />
_________________ Heart<br />
_________________ Cardiovascular _________________<br />
Eyes<br />
_________________ Breast<br />
_________________ Endocrine System _________________<br />
Nose<br />
_________________ Abdomen _________________ Lymphatic System _________________<br />
Throat<br />
_________________ Hernia<br />
_________________ Neurological _________________<br />
Teeth<br />
_________________ Genitalia (Male) _________________ Spine-Musculoskeletal _________________<br />
Ears<br />
_________________ Pelvic (Optional) _________________ Upper Extremities _________________<br />
Neck-Thyroid _________________ Ano-Rectal _________________ Lower Extremities _________________<br />
LAB Values - ABNORMAL RESULTS MUST BE ADDRESSED<br />
Urinalysis ____________________________ Hemoglobin ______________________ OR Hematocrit ____________<br />
Repeat Urinalysis _______________________________________________________<br />
Required Annually: (at the time of physical)<br />
Tuberculin Test (PPD intrademal only)<br />
Date Given: ____________________________ Date Read (48-72 HRS) ___________________ Result: in mm: ________________<br />
Hx ⊕ PPD (MANTOUX) Test: Date _________________________<br />
POSITIVE reactors to TB Test must submit written results of Chest X-ray report (PA & lateral) within two years. (Attach copy of CXR report)<br />
Date: ________________________________ Result: __________________________________________________________________
NAME ____________________________________________________________<br />
Banner I.D. #________________________<br />
Required on Initial Physical Only: TITRES NEED TO BE DONE ONE TIME ONLY FOR INITIAL PHYSICAL<br />
*Attach Lab Reports to this Form (FOUR (4) TITRES MUST BE SUBMITTED) EQUIVOCAL TITRES ARE NOT ACCEPTABLE.<br />
NEGATIVE TITRES REQUIRE IMMUNIZATION. REPEAT TITRE WILL BE REQUIRED IN 30 DAYS.<br />
*Rubeola Titre (Value) __________ Date __________ Result: __________<br />
If negative, Vaccine administered:<br />
__________________<br />
(1) Date<br />
*Mumps Titre (Value) __________ Date __________ Result: __________ __________________<br />
(1) Date<br />
*Rubella Titre (Value) __________ Date __________ Result: __________ __________________<br />
(1) Date<br />
*Varicella Titre (Value) __________ Date __________ Result: __________ __________________ ______________<br />
(1) Date (2) Date<br />
*All dates must be filled in on this form each time you hand in the form.<br />
Polio Salk-Sabin (any history) Date: ___________________________________________<br />
Diphtheria/Tetanus Booster within ten years, Date: ________________________________<br />
Hepatitis B Vaccine: 1) Date _____________ 2) Date _______________ 3) Date __________________ Titre: ___________<br />
ALLIED HEALTH AND NURSING STUDENTS ARE ADVISED TO BE IMMUNIZED WITH HEPATITIS B VACCINE PRIOR TO THE<br />
BEGINNING OF CLINICAL PRACTICE OR MUST SIGN A DECLINATION STATEMENT.<br />
DECLINATION STATEMENT<br />
I understand that during my participation in my clinical internship, I may be exposed to blood or other potentially infectious<br />
materials and I may be at risk of acquiring Hepatitis B Virus (HBV) infection. I have been informed of the need<br />
to be vaccinated with Hepatitis B vaccine. However, I decline Hepatitis B vaccination at this time. I understand that by<br />
declining this vaccination, I continue to be at risk of acquiring Hepatitis B, a serious disease. I understand that Nassau<br />
Community College cannot mandate that I take this vaccination in order to continue my education in my chosen health<br />
science program. My failure to be immunized could jeopardize the successful fulfillment of the requirements of my program<br />
at Nassau Community College, which may preclude me from graduating. I further understand and agree that I<br />
cannot hold Nassau Community College responsible for any injury or illness arising from my activity and/or exposure<br />
to blood or other blood-borne pathogens in my program and clinical laboratories.<br />
Name (Print) ________________________________________________________<br />
Date: ____________________________________<br />
Student Signature ___________________________________________________<br />
PHYSICIAN'S CERTIFICATION -<br />
Above named patient is deemed to be free from any addictive substances (by visual inspection only).<br />
Is this the first time you have seen this patient Yes No<br />
Cleared<br />
Not Cleared<br />
________________________________________________________________________________________________________<br />
________________________________________________________________________________________________________<br />
________________________________________________________________________________________________________<br />
Physician's Signature __________________________________________<br />
Date ____________________________<br />
Physician's Name __________________________________________ License No. __________________________________<br />
(Please Print)<br />
Physician's Stamp ______________________________________________ Phone ( ) _____________________<br />
(Area Code) (Number)<br />
Address ________________________________________________________________________________________________<br />
SPS-4 (Rev. 09/08)<br />
(ALL INFORMATION IS CONFIDENTIAL)