CHN2617 Adult ICU Pain Orders.pdf - Carondelet
CHN2617 Adult ICU Pain Orders.pdf - Carondelet
CHN2617 Adult ICU Pain Orders.pdf - Carondelet

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
ADULT <strong>ICU</strong> PAIN ORDERS<br />
Physician Signature: Date Signed: Time Signed:<br />
STAT/NOW<br />
(Check Box to Left)<br />
* LIST ALL ALLERGIES: (Medication, food, latex and/or Contrast Dye) * Required on Admission <strong>Orders</strong><br />
1. Titrate to target pain: (Mild pain unless otherwise stated by patient)<br />
2. For patients pain select one of the following:<br />
NO RANGE ORDERS ALLOWED<br />
3. FentaNYL CONTINUOUS INFUSION:<br />
FentaNYL infusion at ___________ microgram/hour IV (e.g., 25-50 microgram/hour)<br />
• FentaNYL bolus at _________ microgram (e.g., 25 microgram) IV every 5 minutes p.r.n moderate pain<br />
• FentaNYL bolus at _________ microgram (e.g., 50 microgram) IV every 5 minutes p.r.n severe pain<br />
Repeat boluses until pain controlled<br />
If the patient requires more than 2 boluses in an hour, increase rate by _______ microgram/hour IV (e.g., 12.5-25<br />
microgram/hour) every hour<br />
Maximum dosage = ________ microgram/hour IV (e.g., 100-200 microgram/hour)<br />
Notify Physician if patient becomes hemodynamically unstable, for oversedation, or when pain control is not<br />
achieved at maximum dosage<br />
4. MORPHINE CONTINUOUS INFUSION (Avoid in patients with cardiovascular instability or renal impairment)<br />
Morphine infusion at _________ mg/hour IV (e.g., 2 - 4 mg/hour)<br />
• Morphine bolus at _________ mg (e.g., 2 mg) IV every 10 minutes p.r.n moderate pain<br />
• Morphine bolus at _________ mg (e.g., 4 mg) IV every 10 minutes p.r.n severe pain<br />
Repeat boluses until pain controlled<br />
If the patient requires more than 2 boluses in an hour, increase rate by __________ mg/hour IV (e.g., 1-2 mg/hour)<br />
every hour<br />
Maximum dose = ________ mg/hour IV (e.g., 10 mg/hour IV)<br />
Notify Physician if patient becomes hemodynamically unstable, for oversedation, or when pain control is not achieved<br />
at maximum dosage<br />
HYDROmorphone CONTINUOUS INFUSION<br />
HYDROmorphone infusion at _________ mg/hour IV (e.g., 0.4-0.8 mg/hour)<br />
• HYDROmorphone bolus at _________ mg (e.g., 0.4 mg) IV every 10 minutes p.r.n moderate pain<br />
• HYDROmorphone bolus at _________ mg (e.g., 0.8 mg) IV every 10 minutes p.r.n severe pain<br />
Repeat boluses until pain controlled<br />
If the patient requires more than 2 boluses in an hour, increase rate by _______ mg/hour IV (e.g., 0.2-0.4 mg/hour)<br />
every hour<br />
Maximum dose = ________ mg/hour IV (e.g., 3 mg/hour IV)<br />
Notify Physician if patient becomes hemodynamically unstable,, for oversedation, or when pain control is not achieved<br />
at maximum dosage<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 06/30/11 CSM – 06/30/11 CHC – 06/23/11 CHVI – 06/22/11<br />
<strong>CHN2617</strong> Expires – 06/2014<br />
Copy 05.02.13 Page 1 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
ADULT <strong>ICU</strong> PAIN ORDERS<br />
STAT/NOW<br />
(Check Box to Left)<br />
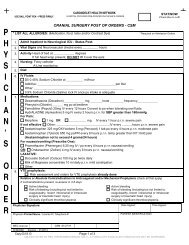
Critical Care <strong>Pain</strong> Observation Tool (CPOT)<br />
For non-communicative adults in critical care areas<br />
0 1 2 Score<br />
Facial Expression<br />
Relaxed, neutral; no<br />
muscular tension<br />
observed<br />
Tense; presence of<br />
frowning, brow lowering,<br />
orbit tightening, and<br />
levator contraction<br />
Grimacing; all facial<br />
movements for 1 plus<br />
eyelid tightly closed<br />
Body Movement<br />
Absence of movements;<br />
does not move at all<br />
(does not necessarily<br />
mean absence of pain)<br />
Protection; slow, cautious<br />
movements; touching or<br />
rubbing site; seeking<br />
attention through<br />
movement<br />
Restlessness; pulling<br />
tubes; attempting to sit<br />
up or get out of bed;<br />
moving limb/thrashing;<br />
not following<br />
commands; striking out<br />
Ventilator Compliance<br />
(intubated patients)<br />
OR<br />
Vocalization<br />
Tolerating ventilator or<br />
movement; alarms not<br />
activated; easy<br />
ventilation<br />
Talking in normal tone or<br />
no sound<br />
Coughing but tolerating;<br />
alarms stop spontaneously<br />
Sighing; moaning<br />
Fighting ventilator;<br />
asynchrony; blocking<br />
ventilation; alarms<br />
frequently activated<br />
Crying out; sobbing<br />
(extubated patients)<br />
Muscle Tension (evaluate<br />
by passive UE flexion and<br />
extension at rest or<br />
evaluate when turning<br />
patient)<br />
Relaxed; no resistance<br />
to passive movements<br />
Tense, rigid; resistance to<br />
passive movements<br />
Very tense or rigid;<br />
strong resistance to<br />
passive movements;<br />
inability to complete<br />
them<br />
Mild: 1-2 Moderate: 3-5 Severe: 6-8<br />
Total:<br />
(0-8)<br />
Visual Analog Scale (Communicative <strong>Adult</strong>s)<br />
Wong-Baker (Non-Communicative <strong>Adult</strong>s)<br />
Physician Signature: Date Signed: Time Signed:<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 06/30/11 CSM – 06/30/11 CHC – 06/23/11 CHVI – 06/22/11<br />
<strong>CHN2617</strong> Expires – 06/2014<br />
Copy 05.02.13 Page 2 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED