Medical Physicist Workforce Study - Health Workforce Australia
Medical Physicist Workforce Study - Health Workforce Australia
Medical Physicist Workforce Study - Health Workforce Australia

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Medical</strong> <strong>Physicist</strong><br />
<strong>Workforce</strong> <strong>Study</strong><br />
September 2012
© <strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong><br />
This work is copyright. It may be reproduced in whole<br />
or part for study or training purposes only, provided<br />
that the acknowledgment below is included.<br />
Any reproduction for purposes other than those<br />
indicated above, or otherwise not in accordance with<br />
the provisions of the Copyright Act 1968 or any other<br />
legal obligation, requires the written permission of<br />
<strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong> (HWA).<br />
ISBN: 978-0-9873201-8-6<br />
Enquiries concerning this report and its reproduction<br />
should be directed to:<br />
<strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong><br />
GPO Box 2098, Adelaide SA 5001<br />
T +61 8 8409 4500 F +61 8 8212 3841<br />
E hwa@hwa.gov.au<br />
www.hwa.gov.au<br />
Citation: <strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong> 2012: <strong>Medical</strong><br />
<strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong>
Contents<br />
1 Introduction ................................................................................................................................. 6<br />
2 <strong>Medical</strong> physicists – their role and responsibilities ................................................................. 7<br />
3 <strong>Workforce</strong> dynamics indicator methodology ........................................................................ 9<br />
4 <strong>Medical</strong> physicist workforce dynamics assessment ............................................................ 11<br />
5 Context for workforce assessment ......................................................................................... 22<br />
6 Potential paths forward ........................................................................................................... 28<br />
Appendix 1 – National Minimum Data Set ................................................................................... 31<br />
References ........................................................................................................................................ 32<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong><br />
iii
List of tables<br />
Table 1: <strong>Workforce</strong> dynamic indicators ........................................................................................................... 10<br />
Table 2: ROMPs and DIMPs – summary of workforce dynamics indicators .............................................. 12<br />
Table 3: Average age workforce dynamic rating assessment, ROMPs .................................................... 13<br />
Table 4: Average age workforce dynamic rating assessment, DIMPs ...................................................... 14<br />
Table 5: Training pathway, ROMPs ................................................................................................................... 15<br />
Table 6: Number of ROMPs intending to retire, 2009 .................................................................................... 15<br />
Table 7: Replacement rate workforce dynamic rating assessment, ROMPS ........................................... 15<br />
Table 8: Training pathway, DIMPs ..................................................................................................................... 16<br />
Table 9: Number of DIMPs intending to retire, 2011 ...................................................................................... 16<br />
Table 10: Replacement rate workforce dynamic rating assessment, DIMPs ........................................... 16<br />
Table 11: Vacancy rate, ROMPs, 2006 and 2009 ........................................................................................... 17<br />
Table 12: Vacancy rate workforce dynamic rating assessment, ROMPs ................................................. 18<br />
Table 13: Vacancy rate, DIMPs, 2006 and 2009 ............................................................................................. 19<br />
Table 14: Vacancy rate workforce dynamic rating assessment, DIMPs ................................................... 19<br />
Table 15: Origin of qualification by year of qualification, ROMPs .............................................................. 20<br />
Table 16: Dependence on ITPs workforce dynamic rating assessment, ROMPs ..................................... 20<br />
Table 17: Duration of training program workforce dynamic rating assessment, ROMPs and DIMPs .. 21<br />
Table 18: Employed ROMPs and DIMPs in <strong>Australia</strong>, 2006 and 2009 .......................................................... 22<br />
Table 19: Calculation of DIMP workforce trends with and without intakes .............................................. 26<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong><br />
iv
List of figures<br />
Figure 1: Professions survey – ROMPs (including registrars), age by sex, 2008 .......................................... 13<br />
Figure 2: DIMPs, age by sex, 2011 .................................................................................................................... 14<br />
Figure 3: ROMPs (including registrars), average weekly hours worked by sex, 2008 .............................. 23<br />
Figure 4: ROMP workforce projections to 2019............................................................................................... 25<br />
Figure 5: DIMP workforce trends with and without intakes ......................................................................... 26<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong><br />
v
1 Introduction<br />
In 2002, the Report of the radiation oncology inquiry: A vision for radiotherapy 1 was published. The<br />
aim of this inquiry was to ‘examine and make recommendations on <strong>Australia</strong>'s usage of radiation<br />
therapy as a cancer treatment modality with reference to current capacity, international best<br />
practice, clinical efficacy, as well as other cancer treatment modalities’. Within this, the role of<br />
radiation oncology medical physicists (along with radiation oncologists and radiation therapists)<br />
was examined. For radiation oncology medical physicists, the inquiry found existing workforce<br />
shortages, with increasing attrition rates. Recommendations in relation to the workforce included<br />
better career paths, competitive remuneration and the introduction of a formal training pathway<br />
(which was subsequently established).<br />
Since then, concerns have continued in relation to the radiation oncology medical physicist<br />
workforce. For example, in 2009, a Department of <strong>Health</strong> and Ageing commissioned review of the<br />
radiation oncology workforce 2 confirmed a shortage of radiation oncology medical physicists.<br />
Then, in 2010, the <strong>Health</strong> <strong>Workforce</strong> Principal Committee also highlighted a concern about a<br />
shortage of medical physicists, particularly of diagnostic imaging medical physicists. It was agreed<br />
that <strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong> (HWA) would consider this matter. This occurred at the same time<br />
as the implementation of the cancer care initiatives announced in the 2009 Federal Budget. In<br />
addition, HWA is concurrently developing a broader National Cancer <strong>Workforce</strong> Strategy, and the<br />
radiation oncology medical physicist workforce is incorporated within this work.<br />
The purpose of this report is to examine the radiation oncology and diagnostic imaging medical<br />
physicist workforces and highlight if there is cause for concern. Firstly, this report provides an<br />
overview of medical physics and the specialties within the profession. To examine the medical<br />
physicist workforces, an assessment is conducted against five separate workforce dynamics<br />
indicators – the indicators are first described and then the assessment against each is presented. It<br />
should be noted HWA did not conduct a new data collection to be able to undertake the<br />
assessments. Rather, existing information about the workforces was used. The assessment is followed<br />
by information on other key factors to assist in interpreting the significance of the assessment results.<br />
Finally, potential paths forward are presented.<br />
1<br />
Report of the radiation oncology inquiry: A vision for radiotherapy, Commonwealth of <strong>Australia</strong>, 2002.<br />
Accessed at http://www.health.gov.au/internet/main/publishing.nsf/Content/health-roi-inquiry-report.htm.<br />
2<br />
<strong>Health</strong>Consult. Radiation Oncology <strong>Workforce</strong> Planning. Final Report for Department of <strong>Health</strong> and Ageing.<br />
Sydney: <strong>Health</strong>Consult, November 2009.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 6
2 <strong>Medical</strong> physicists – their role and responsibilities<br />
The medical applications of x-rays and radioactivity have given rise to the discipline of medical<br />
physics. Accordingly, medical physicists are health professionals with specialised training in the<br />
medical applications of physics. Their work involves the use of: x-rays; gamma rays; electron and<br />
charged particle beams; neutrons; and radiations from sealed and unsealed radionuclide sources<br />
in the diagnosis and treatment of human diseases.<br />
There are three medical physicist specialties – radiation oncology, radiology and nuclear medicine.<br />
Radiation oncology medical physics pertains to the:<br />
• therapeutic application of x-ray, gamma rays, electron and charged particle beams,<br />
neutrons and radiations from sealed radionuclide sources<br />
• equipment associated with their production, use, measurement and evaluation<br />
• proper calibration and quality control of equipment used for therapeutic purposes and<br />
radiation dosimetry.<br />
Radiation oncology medical physicists (ROMPs), that is, people who practice radiation oncology<br />
medical physics, design and implement the quality assurance program in radiation oncology. Their<br />
primary roles are to ensure: therapy radiation doses are delivered accurately; radiation safety of<br />
patients, staff and the general public; and compliance with relevant regulations and standards.<br />
Radiology medical physics pertains to the:<br />
• diagnostic application of x-ray, gamma rays from sealed sources, ultrasound, radio<br />
frequency radiation and magnetic fields in medical imaging<br />
• equipment associated with the use of radiation for diagnostic imaging<br />
• quality of images and radiation dose associated with the use of imaging equipment.<br />
Nuclear medical physics pertains to the:<br />
• therapeutic and diagnostic application of radioactive isotopes for medical purposes<br />
• equipment associated with the production, use, measurement and evaluation of<br />
radioactive isotopes<br />
• quality of images and patient dose resulting from the use of radioactive isotopes.<br />
Collectively, radiology medical physicists and nuclear medical physicists are referred to as<br />
diagnostic imaging medical physicists (DIMPs). DIMPs play an important role in the quality<br />
assurance of imaging equipment and ensuring optimum image quality 3 , with the diagnostic<br />
parameters derived from images paramount in the management of patients’ treatment. 4 DIMPs<br />
also ensure that radiation exposure from radioactive sources, x-rays and other radiation emitters is<br />
measured or calculated appropriately for dosimetric and safety purposes. As with ROMPs, the role<br />
of DIMPs also encompasses the radiation safety of patients, staff and the general public, and<br />
ensuring compliance with relevant regulations and standards.<br />
Regulatory responsibilities<br />
The <strong>Australia</strong>n Radiation Protection and Nuclear Safety Agency (ARPANSA) is responsible for<br />
protecting the health and safety of people, and the environment, from the harmful effects of<br />
ionising and non-ionising radiation. ARPANSA developed the Code of Practice for Radiation<br />
3<br />
For further detail see www.acpsem.org.au.<br />
4<br />
Personal communication, John Cormac, September 2011. For further detail see<br />
www.chemphys.adelaide.edu.au/ medicalphysics.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 7
Protection in the <strong>Medical</strong> Applications of Ionizing Radiation (2008) (the Code), a regulatory<br />
document that covers the practices of radiotherapy, diagnostic and interventional radiology and<br />
nuclear medicine. The Code identifies that all health facilities using radiation must have access to a<br />
‘qualified expert’, this being a qualified medical physicist. Specifically, the qualified expert is<br />
defined as a person who:<br />
• is qualified in the application of the physics of therapeutic or diagnostic uses of ionizing<br />
radiation, and<br />
• has been recognised by the relevant regulatory authority as being able to perform the<br />
dosimetric calculations, radiation measurements and monitoring relevant to the person’s<br />
area of expertise. 5<br />
The qualified expert needs to be available for consultation on optimisation, dosimetry and quality<br />
assurance; and to give advice on matters relating to radiation protection in medical exposure. In<br />
addition, for radiotherapy the Code outlines that calibration, dosimetry and quality assurance<br />
requirements are conducted by, or under the supervision of, a qualified expert. This means each<br />
health facility using radiation must have access to a medical physicist who ensures that the<br />
radiation exposure from radioactive sources, x-rays and other radiation emitters is measured or<br />
calculated appropriately for dosimetric and safety purposes.<br />
5<br />
<strong>Australia</strong>n Radiation Protection and Nuclear Safety Agency, 2008.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 8
3 <strong>Workforce</strong> dynamics indicator methodology<br />
HWA has adapted <strong>Health</strong> <strong>Workforce</strong> New Zealand’s (HWNZ) medical discipline vulnerability ranking<br />
method to highlight aspects of the current workforce that may be of concern now and into the<br />
future. In this method, HWNZ use a traffic light approach to score workforces against four indicators<br />
(age and trainee numbers, dependence on general registrants, dependence on international<br />
medical graduates and level of vacancies). Scores against each indicator are then combined into<br />
an overall rating to demonstrate the vulnerability of the workforce. HWA renamed the method<br />
‘workforce dynamics indicator’ as the term ‘vulnerability’ has an implied meaning which was not<br />
appropriate for the assessment being made, and selected the following indicators for scoring.<br />
• Average age – workforces with a higher average age are of more concern due to the<br />
potential for higher exit rates (through retirement).<br />
• Replacement rate – this item calculated the ratio of newly accredited medical physicists to<br />
workforce exits in a given year. This indicates whether the number gaining accreditation is<br />
sufficient to replace those presently leaving the workforce. Note: this is an indicator for<br />
workforce dynamics assessment purposes only and is not intended to guide training<br />
numbers for the future.<br />
• Vacancy rate – workforces with a higher percentage of vacancies are of more concern<br />
due to the inability to fill existing workforce positions.<br />
• Dependence on internationally trained professionals (ITPs) – workforces with high<br />
percentages of ITPs are of greater concern due to their dependence on a less reliable<br />
supply stream (for example, changes in immigration policy may impact on supply, migrants<br />
may choose to settle in other countries).<br />
• Duration of training program – the greater the duration of training, the longer it takes to train<br />
a replacement workforce.<br />
The indicator range boundaries were selected as an extension of the HWNZ ranking method. In this<br />
initial development of the workforce dynamics indicator, the ranges for each indicator rating were<br />
set to be relatively equal, rather than being established using a statistical base.<br />
Unlike HWNZ, an overall rating is not generated in HWA’s scoring. This reflects the view that the<br />
focus should be on each individual indicator, and understanding the drivers of the results for those<br />
indicators, rather than on an amalgamated rating.<br />
To be able to score against the workforce dynamics indicators, an extensive range of data is<br />
required. Where a score cannot be allocated due to insufficient data, the indicator is not assessed.<br />
It should be noted this is a first iteration of the workforce dynamics indicator within HWA. The<br />
indicators used are basic measures only – ideally as data availability improves, more sophisticated<br />
measures can be developed.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 9
Table 1 summarises the workforce dynamics indicator and the score ranges.<br />
Table 1: <strong>Workforce</strong> dynamic indicators<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Average age of existing workforce
4 <strong>Medical</strong> physicist workforce dynamics assessment<br />
In this section, the ROMP and DIMP workforces are assessed against each workforce dynamic<br />
indicator. As noted earlier, HWA did not conduct a new data collection to obtain information on<br />
these workforces. Rather, the assessments have been based on existing information.<br />
For ROMPs, two key data sources were used.<br />
1. The Radiation Oncology <strong>Workforce</strong> Planning Final Report (prepared by <strong>Health</strong>Consult in<br />
2009). This was a review of the radiation oncology workforce commissioned by the<br />
Department of <strong>Health</strong> and Ageing, and included both primary data collection (with 80<br />
percent coverage of the ROMP workforce) and consultations with key stakeholders.<br />
2. The 2006 and 2009 Round Survey of the Australasian clinical medical physics and<br />
biomedical engineering workforce, which reviewed the profile, salary levels and number of<br />
vacant positions in the surveyed workforces.<br />
For DIMPs, the Round surveys were also key data sources, along with data made available to HWA<br />
from the Australasian College of Physical Scientists and Engineers in Medicine (ACPSEM).<br />
Summary of indicator results<br />
A summary of the indicator results for ROMPs and DIMPs is provided in Table 2. Reflecting the fact<br />
that data availability is greater for ROMPs, each indicator for ROMPs was able to be assessed. This is<br />
because of the greater focus on the ROMP workforce stemming from the 2002 Report of the<br />
radiation oncology inquiry: A vision for radiotherapy.<br />
The ROMP workforce has a low average age (less than 40) and more ROMPs being accredited<br />
than leaving the workforce (with retirement intentions used as a proxy for exits). Consequently both<br />
these indicators received the lowest rating in the workforce dynamics assessment, that is, they are<br />
areas of minimal concern. ROMPs had a vacancy rate of more than 10 percent (receiving the<br />
highest rating for this indicator, and therefore an area of significant concern), and a medium rating<br />
for dependence on internationally trained professionals (with approximately 40 percent of ROMPs<br />
receiving their qualification overseas).<br />
For DIMPs, one indicator (dependence on ITPs) was not assessed due to data availability. This<br />
suggests improved data collection is an area for future improvement for this workforce. Of the<br />
assessed indicators, the replacement rate received the highest rating (and is an area of significant<br />
concern), with no DIMP accreditations over the period 2006 to 2011. The average age (44 years)<br />
and vacancy rate (approximately seven percent) indicators both received medium ratings.<br />
With the majority of the workforce dynamics indicator assessments falling within the medium rating,<br />
this suggests areas of concern for both the ROMP and DIMP workforces.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 11
Table 2: ROMPs and DIMPs – summary of workforce dynamics indicators<br />
ROMPs<br />
DIMPs<br />
Average age of existing workforce<br />
Ratio of accreditations to workforce exits<br />
Vacancy rate<br />
Dependence on ITPs<br />
(ITPs as a percentage of employed practitioners)<br />
n.a.*<br />
Duration of training program (years)<br />
*n.a. not assessed<br />
As noted earlier, an extensive range of data is required to be able to conduct the indicator<br />
assessment. With one indicator not able to be assessed for DIMPs, the replacement rate indicator<br />
using a proxy data item (retirement intentions rather than actual exits) and key data sources for the<br />
ROMP and DIMP workforces being collected on a different basis, with different data items, there is<br />
scope for improved data collection. Improvements in data collected would allow for more robust<br />
and comparable assessments, as well as monitoring and planning. For information, Appendix 1<br />
contains the <strong>Australia</strong>n <strong>Health</strong> Ministers’ Advisory Council endorsed national minimum data set<br />
items along with a proposed data dictionary for medical physicists.<br />
Average age<br />
ROMPs<br />
Average age information was not directly available from either of the ROMP key data sources.<br />
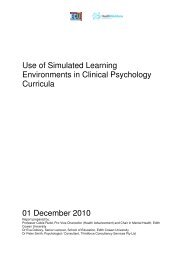
However, the 2009 <strong>Health</strong>Consult report provided an age and sex distribution of the ROMP<br />
workforce (Figure 1). This showed ROMPs have a relatively young age profile – more than half (54<br />
percent) were aged less than 40 years, with only 11 percent aged more than 55 years.<br />
On the basis of the age distribution, the average age of ROMPs in 2009 can be estimated to fall<br />
within the 35 to 39 year age bracket (the lowest range in the workforce dynamics indicator score,<br />
Table 3).<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 12
40<br />
35<br />
30<br />
Male<br />
Female<br />
Number<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65+<br />
Age Group (years)<br />
Figure 1: Professions survey – ROMPs (including registrars), age by sex, 2008<br />
Source: <strong>Health</strong>Consult, 2009<br />
Table 3: Average age workforce dynamic rating assessment, ROMPs<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Average age of existing workforce
Number<br />
10<br />
9<br />
8<br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
Male<br />
Female<br />
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65+<br />
Age Group (years)<br />
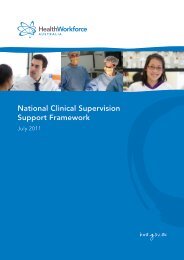
Figure 2: DIMPs, age by sex, 2011<br />
Source: Unpublished data, ACPSEM, November 2011<br />
With an average age of 44 years, the DIMP assessment for average age falls within the second<br />
rating.<br />
Table 4: Average age workforce dynamic rating assessment, DIMPs<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Average age of existing workforce
ROMPs<br />
Number of trainees and accreditations<br />
Table 5 provides an overview of the TEAP training pathway from 2006 to 2011 for ROMPs. New TEAP<br />
enrolments occurred each year over the period, along with an increasing (but relatively small)<br />
number of new accreditations. These data are consistent with the funding of fifteen ROMP registrars<br />
commencing their first year of training in 2010-11 under the Department of <strong>Health</strong> and Ageing<br />
Strengthening Cancer Care budget measure.<br />
Table 5: Training pathway, ROMPs<br />
2006 2007 2008 2009 2010 2011<br />
New TEAP enrolments 12 16 18 23 15 15<br />
Accreditations 0 0 3 2 8 6<br />
Source: Prof Eva Bezak, Personal communication October 2011<br />
<strong>Workforce</strong> exits<br />
As noted above, exit information was not available for the ROMP workforce. However, the 2009<br />
<strong>Health</strong>Consult survey collected data on ROMPs’ intention to retire, and in the absence of other<br />
information this measure is used as a proxy. Table 6 shows that at the time of the survey, 16 ROMPs<br />
(eight percent) intended to retire between 2009 and 2013, with a further 18 (or nine percent)<br />
intending to retire between 2014 and 2018. Assuming the retirements occur at an equal rate across<br />
those years, this equates to approximately three people exiting per annum.<br />
Table 6: Number of ROMPs intending to retire, 2009<br />
2009-2013 2014-2018 2019 and beyond<br />
<strong>Australia</strong> 16 18 143<br />
Note: Excluding registrars. Source: <strong>Health</strong>Consult, 2009<br />
Using an average of the accreditations over the period 2009 to 2011, the ratio of accreditations to<br />
workforce exits for ROMPs falls into the lowest rating bracket on the assessment scale (Table 7).<br />
Table 7: Replacement rate workforce dynamic rating assessment, ROMPS<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Proportion of accreditations to<br />
workforce exits<br />
130+%<br />
110-<br />
DIMPs<br />
Number of trainees and accreditations<br />
For DIMPs, there have only been a small number of nuclear medicine TEAP enrolments in recent<br />
years, with no enrolments for radiology. There have been no accreditations for DIMPs over the<br />
period 2006 to 2011 (Table 8).<br />
Table 8: Training pathway, DIMPs<br />
New TEAP enrolments<br />
2006 2007 2008 2009 2010 2011<br />
Radiology 0 0 0 0 0 0<br />
Nuclear medicine 2 0 0 4 2 1 (a)<br />
Total DIMPs 2 0 0 4 2 1 (a)<br />
(a) Enrolled in Diagnostic Imaging under the TEAP for DIMPs. Source: Prof Eva Bezak, Personal<br />
communication October 2011<br />
<strong>Workforce</strong> exits<br />
Table 9 provides information on DIMPs’ intentions to retire – with 11 DIMPs intending to retire in the<br />
next two years (from the time of the survey) and a further three in the next five years. Using the<br />
same process as was used for ROMPs, that is, assuming the retirements occur at an equal rate<br />
across those years, this equates to approximately three people exiting per annum.<br />
Table 9: Number of DIMPs intending to retire, 2011<br />
In the next 2 years In the next 5 years In the next 10 years<br />
<strong>Australia</strong> 11 3 1<br />
Source: Unpublished data, ACPSEM, November 2011<br />
With no accreditations, the replacement rate indicator is assessed at the highest rating bracket on<br />
the assessment scale (Table 10).<br />
Table 10: Replacement rate workforce dynamic rating assessment, DIMPs<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Proportion of accreditations to<br />
workforce exits<br />
130+%<br />
110-<br />
ROMPs<br />
Table 11 provides the vacancy rate for the ROMP workforce. Nationally, there was a relatively high<br />
proportion of vacancies for ROMPs in both 2006 (14 percent) and 2009 (11 percent). The vacancy<br />
rate varied substantially across states and territories, ranging from a low of approximately six<br />
percent in Western <strong>Australia</strong> to a high of 27 percent in the <strong>Australia</strong>n Capital Territory in 2009.<br />
Large variability in vacancy rates occurred within states and territories across survey years. For<br />
example, in the <strong>Australia</strong>n Capital Territory the vacancy rate increased from zero in 2006 to 27<br />
percent in 2009. This is because of the size of the ROMP workforce, where only a small change in<br />
the number of vacancies has a large percentage impact.<br />
ROMP services are provided remotely to the Northern Territory. This is reflected in Table 11 with the<br />
Northern Territory having no vacancies or positions.<br />
Table 11: Vacancy rate, ROMPs, 2006 and 2009<br />
2006 2009<br />
Vacancies<br />
Total<br />
positions (a)<br />
Vacancy<br />
rate<br />
Vacancies<br />
Total<br />
positions (a)<br />
Vacancy<br />
rate<br />
State/Territory FTE FTE % FTE FTE %<br />
NSW 17.0 100.0 17.0 12.0 116.7 10.3<br />
Vic 7.0 48.3 14.5 4.0 55.6 7.2<br />
Qld 4.0 31.9 12.5 6.0 44.4 13.5<br />
SA 0.0 17.8 0.0 3.5 26.5 13.2<br />
WA 2.0 15.4 13.0 1.0 17.4 5.7<br />
Tas 1.0 6.1 16.4 0.9 5.9 15.3<br />
ACT 0.0 4.5 0.0 2.0 7.3 27.3<br />
NT 0.0 0.0 –– 0.0 0.0 ––<br />
<strong>Australia</strong> 31.0 223.9 13.8 29.4 273.8 10.7<br />
(a) Including vacancies. Source: Round, 2007 and 2010<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 17
As an average across the two survey years, the ROMP vacancy rate was approximately 12<br />
percent. This falls into the highest range on the workforce dynamic rating scale (Table 12).<br />
Table 12: Vacancy rate workforce dynamic rating assessment, ROMPs<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Vacancy rate
Table 13: Vacancy rate, DIMPs, 2006 and 2009<br />
2006 2009<br />
Vacancies<br />
Total<br />
positions (a)<br />
Vacancy<br />
rate<br />
Vacancies<br />
Total<br />
positions (a)<br />
Vacancy<br />
rate<br />
State/Territory FTE FTE % FTE FTE %<br />
NSW 2.0 26.3 7.6 1.0 24.7 0.4<br />
Vic 0.0 7.1 0.0 0.0 9.5 0.0<br />
Qld 0.0 15.3 0.0 1.0 16.9 5.9<br />
SA 0.0 5.4 0.0 2.3 7.9 29.1<br />
WA 1.0 13.3 7.5 1.0 15.3 6.5<br />
Tas 0.1 0.7 14.3 0.0 0.0 ––<br />
ACT 1.0 1.1 90.9 1.1 1.7 64.7<br />
NT 0.0 0.0 –– 0.0 0.0 ––<br />
<strong>Australia</strong> 4.1 69.0 5.9 6.4 76.0 8.4<br />
(a) Including vacancies. Source: Round, 2007 and 2010<br />
As an average across the two survey years, the DIMP vacancy rate was approximately seven<br />
percent. This falls within the third bracket on the workforce dynamics rating scale (Table 14). Please<br />
note, advice from ACPSEM was that this rating should be at the highest level. They suggested longterm,<br />
unfilled positions have fallen off the vacancy list, leading to an under-estimation of the<br />
number of vacancies (and consequently a lower workforce dynamics indicator rating). They also<br />
suggested there is a shortfall in existing workforce numbers required to provide an appropriate<br />
quality service.<br />
Table 14: Vacancy rate workforce dynamic rating assessment, DIMPs<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Vacancy rate
Dependence on internationally trained professionals<br />
ROMPs<br />
The <strong>Health</strong>Consult survey identified that approximately 40 percent of ROMPs received their<br />
qualification overseas (Table 15). This proportion was relatively consistent across ROMPs regardless<br />
of workforce entry year. This indicates there is reliance in the workforce on internationally trained<br />
professionals.<br />
Table 15: Origin of qualification by year of qualification, ROMPs<br />
<strong>Workforce</strong> entry year<br />
Before 2000 2000-2004 2005-2009 Total<br />
Place of qualification no. % no. % no. % no. %<br />
<strong>Australia</strong> 51 63.8 24 57.1 29 56.9 104 60.1<br />
Overseas 29 36.2 18 42.9 22 43.1 69 39.9<br />
Total 80 100.0 42 100.0 51 100.0 173 100.0<br />
Note: Excludes registrars and 20 origin of qualification not stated. Source: <strong>Health</strong>Consult, 2009<br />
Based on the information in Table 15, the ROMP workforce falls within the third bracket on the<br />
workforce dynamics rating scale for dependence on ITPs (Table 16).<br />
Table 16: Dependence on ITPs workforce dynamic rating assessment, ROMPs<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Dependence on ITPs 0-14% 15-29% 30-44% 45-59% 60+%<br />
DIMPs<br />
Information was not available on ITPs for the DIMP workforce, therefore this indicator was not<br />
assessed. ACPSEM suggested this indicator would fall within the middle assessment ranges based<br />
on their workforce modelling.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 20
Duration of training program<br />
To become a medical physicist, a person must:<br />
• complete an undergraduate degree with a major in physics<br />
• obtain a training position at a clinical department<br />
• apply for a place as a registrar in the TEAP in one of three specialty areas (upon obtaining a<br />
training position), and<br />
• complete a post-graduate degree in medical physics, normally at Masters level<br />
(undertaken concurrently with TEAP completion). 7<br />
Upon successful completion of the above steps, the ACPSEM accredits a person as a medical<br />
physicist.<br />
For the purpose of this indicator, the assessment is based on the post-graduate training time (that is,<br />
the TEAP), not the entire training pathway. TEAP initially commenced for ROMPs in 2003. It was first<br />
developed as a response to the 2002 Report of the radiation oncology inquiry: A vision for<br />
radiotherapy, which recommended the introduction of a formal five-year training program for<br />
ROMPs. The program was expanded to encompass radiology and nuclear medicine (DIMPs). The<br />
ACPSEM website notes the TEAP ‘standard program is expected to take four to five years’. For this<br />
assessment the longest training time is assumed. Therefore, both the ROMP and DIMP rating falls in<br />
the third bracket on the assessment scale for this indicator.<br />
Table 17: Duration of training program workforce dynamic rating assessment, ROMPs and DIMPs<br />
Minimal<br />
concern<br />
Significant<br />
concern<br />
1 2 3 4 5<br />
Duration of training program (years)
5 Context for workforce assessment<br />
While the assessment in chapter 4 highlights a number of areas of concern in both the ROMP and<br />
DIMP workforces, it is important to understand other factors that may influence the interpretation of<br />
the assessment. Three additional aspects are presented for information in this chapter:<br />
• Size and other characteristics of the workforces<br />
• Demand for ROMPs and DIMPs<br />
• <strong>Workforce</strong> projections.<br />
Size and other characteristics<br />
Size<br />
The absolute size of a workforce is not necessarily a measure of concern in itself – how would the<br />
threshold below which a workforce is considered vulnerable be determined However, when<br />
combined with other indicators the size of a workforce can contribute to areas of concern. Table<br />
18 presents the size of the ROMP and DIMP workforces. ROMPs accounted for the majority of<br />
employed medical physicists in 2009 (78 percent or 244.4 FTE), with DIMPs accounting for the<br />
remaining 22 percent. The DIMP category was split almost equally between radiology medical<br />
physicists (32.4 FTE) and nuclear medicine medical physicists (37.2 FTE).<br />
As can be seen, both workforces (particularly the DIMP workforce) are very small. This means they<br />
are likely to be more affected by areas of significant concern (highlighted by the workforce<br />
dynamics indicator) than larger workforces. For example, the ROMP workforce has a high vacancy<br />
rating. In a sustained period of high vacancies, the impact on the ROMP workforce could be<br />
expected to be more significant when compared with a larger workforce. This is because the larger<br />
workforce would have some capacity to absorb high vacancies in the short-term, while<br />
interventions could be established.<br />
Table 18: Employed ROMPs and DIMPs in <strong>Australia</strong>, 2006 and 2009<br />
Employed (FTE)<br />
2006 2009<br />
Radiation Oncology (ROMPs) 192.9 244.4<br />
Diagnostic imaging medical physicists<br />
Radiology 25.4 32.4<br />
Nuclear Medicine 39.5 37.2<br />
Total DIMPs 64.9 69.6<br />
Total medical physicists 257.8 314.0<br />
Source: Round, 2007; Round, 2010<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 22
Average hours worked and gender distribution<br />
ROMPs<br />
Figure 3 presents average weekly hours worked by gender for ROMPs. The majority of ROMPs<br />
worked between 40-49 hours per week, with only small proportions working 50 or more hours per<br />
week (eight percent) and less than 30 hours per week (six percent). Almost half (49 percent) of<br />
female ROMPs worked less than 40 hours per week, compared with approximately one-third (32<br />
percent) of males.<br />
Figure 1 earlier in this report showed there are approximately equal numbers of male and female<br />
ROMPs in the younger age groups, with the older age groups dominated by males. Combined with<br />
the average hours worked results, this will likely have an impact on ROMP supply.<br />
100<br />
90<br />
80<br />
70<br />
Male<br />
Female<br />
Number<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70+<br />
Average Weekly Hours Worked<br />
Figure 3: ROMPs (including registrars), average weekly hours worked by sex, 2008<br />
Source: <strong>Health</strong>Consult, 2009<br />
DIMPs<br />
Average hours worked information was not available for DIMPs, however it can be assumed that a<br />
similar pattern of female and male average hours worked would exist, that is, female average<br />
weekly hours worked are lower than males. Similar to ROMPs, there are also approximately equal<br />
numbers of male and female DIMPs in the younger age groups (Figure 2, earlier in this report, noting<br />
also the very small numbers). A similar effect as described above may be expected, with an<br />
impact on DIMP workforce supply.<br />
So, being small workforces with increasing female participation (that may impact average weekly<br />
hours worked), the areas of concern highlighted by the workforce dynamics indicator could be<br />
expected to affect the ROMP and DIMP workforces more than workforces with greater absolute<br />
numbers.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 23
Demand for ROMPs and DIMPs<br />
If demand for the ROMP and DIMP workforces is not expected to continue, high workforce<br />
dynamics indicator ratings may be of less concern than if demand is expected to continue or<br />
grow. In the latter instance, high workforce dynamics ratings may indicate a need for workforce<br />
intervention. There are two key factors influencing the demand for the ROMP and DIMP workforces<br />
– increasing incidence of cancer and increasing cancer care infrastructure.<br />
Incidence of cancer<br />
According to the <strong>Australia</strong>n Institute of <strong>Health</strong> and Welfare, the number of new cancer cases more<br />
than doubled between 1982 (47,350 new cases) and 2007 (108,368 new cases). 8 The incidence rate<br />
for all cancers combined also increased (by 27 percent) – from 383 cases per 100,000 people in<br />
1982 to 485 cases per 100,000 people in 2007. 9<br />
Further to this, Cancer <strong>Australia</strong> noted in their 2010-11 Annual Report: ‘In 2010 about 115,000<br />
<strong>Australia</strong>ns were expected to be diagnosed with cancer, and by the age of 85 years, one in two<br />
men and one in three women will have been diagnosed with cancer in their life. Cancer is<br />
estimated to be the leading cause of burden of disease in <strong>Australia</strong>, accounting for approximately<br />
19 per cent of the total disease burden in 2010’.<br />
Similar concern over the demand for services has been expressed by Victoria with an expected<br />
increase of over 20 percent in cancer incidence over the next decade 10 .<br />
From such statements, it can be expected the incidence of cancer will continue, and<br />
consequently there will be a continuing, if not growing, demand for ROMP and DIMP services.<br />
Infrastructure<br />
The 2009-10 Federal Budget included a number of initiatives related to the Cancer Care System.<br />
New infrastructure announced included national centres at the Royal Prince Alfred Hospital in<br />
Sydney, the Parkville Comprehensive Cancer Centre in Melbourne and an expansion of the<br />
Garvan St Vincent’s Cancer Centre in Sydney, plus the building of a network of regional cancer<br />
centres. This increase in infrastructure will particularly impact on the demand for ROMPs, whose role<br />
encompasses ensuring that therapy radiation doses are accurately delivered. The impact on DIMPs<br />
will not be as great, however some increase in demand is expected, reflected in the funding of<br />
fifteen additional diagnostic imaging training positions.<br />
<strong>Workforce</strong> projections<br />
<strong>Workforce</strong> projections are a tool to assist with workforce planning. In the context of this report<br />
workforce projections can be used to highlight any significant anticipated changes to the future<br />
workforce that may impact on the workforce dynamics assessment.<br />
ROMPs<br />
In the 2009 <strong>Health</strong>Consult report, a workforce projection was conducted using 2009 as the baseline<br />
(by age profile), with expected recruitment and estimated attrition rates. Parameters and<br />
assumptions in the projection included:<br />
• there would be 97 new registrars in each five year period of the projections<br />
• 38 percent of <strong>Australia</strong>n patients diagnosed with cancer received radiation treatment (per<br />
the 2002 Report of the radiation oncology inquiry: A vision for radiotherapy)<br />
8<br />
http://www.aihw.gov.au/cancer/. Accessed 2 May 2012.<br />
9<br />
Ibid<br />
10<br />
Victorian Government. Department of Human Services, Victorian Radiotherapy Service Plan, July 2007.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 24
• a moderate target to aim to achieve was 45 percent treatment<br />
• the desired, or best practice treatment rate was 52.3 percent rate.<br />
Figure 4 presents the supply projection and estimated demand scenarios. In the short to medium<br />
term, the level of supply remained at the ’no change’ demand level of meeting approximately 38<br />
percent receiving treatment. This is substantially less than the moderate (45 percent) or best<br />
practice (52.3 percent) levels of treatment. In the longer term, the projection showed that<br />
workforce supply, with expected recruitment and estimated attrition, would be sufficient to meet<br />
the moderate level of treatment (but still below the best practice level of treatment).<br />
ROMP <strong>Workforce</strong> Projection<br />
500<br />
450<br />
400<br />
350<br />
300<br />
250<br />
Supply of ROMPs<br />
200<br />
Demand: Best Paractice (52.3% treatment)<br />
150<br />
Demand: Moderate (45% treatment)<br />
100<br />
50<br />
Demand: No change (38% treatment)<br />
0<br />
2009 2014 2019<br />
Figure 4: ROMP workforce projections to 2019<br />
Source: <strong>Health</strong>Consult, 2009<br />
DIMPs<br />
For DIMPs, a projection series was prepared (Cormack 2011) which provided a workforce supply<br />
trend if no intake is initiated, and the level of intake that would be required to increase the DIMP<br />
workforce to a fixed level. The tabulation used and the graphical presentation published in 2011<br />
are provided in Table 19 and Figure 5.<br />
This illustrative approach to projecting workforce supply to meet a fixed demand provides an<br />
indication of the magnitude of the injection of new registrars required (assuming nothing else<br />
changes). This assists in providing short and medium term directions in the estimation of the number<br />
of new registrars.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 25
Year<br />
Table 19: Calculation of DIMP workforce trends with and without intakes<br />
Effective<br />
workforce<br />
(current<br />
trend)<br />
<strong>Workforce</strong><br />
(required)<br />
Effective<br />
workforce (a)<br />
Effective<br />
registrar<br />
contribution<br />
intake 1 (b)<br />
Effective<br />
registrar<br />
contribution<br />
intake 2 (c)<br />
Effective<br />
registrar<br />
contribution<br />
ongoing (d)<br />
Intake of<br />
experienced<br />
DIMPs<br />
2010 64 104 68 4<br />
Attrition<br />
Rate<br />
2011 60 104 68 4 6.5%<br />
2012 56 104 74 7 4 6.5%<br />
2013 52 104 87 7 6.33 4 6.5%<br />
2014 49 104 98 7 6.33 4 6.5%<br />
2015 46 104 104 6.33 1.33 4 6.5%<br />
2016 43 104 102 2.66 4.0%<br />
2017 40 104 102 4 4.0%<br />
2018 37 104 102 4 4.0%<br />
2019 35 104 102 4 4.0%<br />
2020 33 104 102 4 4.0%<br />
(a) Effective workforce (with recruitment and training strategy)<br />
(b) Effective registrar contribution intake 1: 21 registrars, starting 2011<br />
(c) Effective registrar contribution intake 2: 20 registrars, starting 2012<br />
(d) Effective registrar contribution (ongoing): 4 new registrars per year, starting 2014<br />
Source: John Cormack, Personal communication May 2011<br />
Figure 5: DIMP workforce trends with and without intakes<br />
120<br />
Required level<br />
Effective workforce<br />
100<br />
80<br />
60<br />
40<br />
20<br />
With recruitment/training<br />
strategy<br />
Current trend<br />
0<br />
2008 2010 2012 2014 2016 2018 2020 2022<br />
Source: Cormack, 2011<br />
Limitations in the DIMP illustrative projections<br />
The projection series prepared by Cormack (2011) demonstrated a widening gap between the<br />
demand and supply of DIMP services. However there are a number of additional factors to<br />
consider in interpreting the projection series.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 26
• The impact of the number of new TEAP recruits on the existing workforce. Two major intakes<br />
of registrars included in the projection would have a major impact of the need for<br />
supervision from the reducing pool of experienced DIMPs. This would impact on the<br />
provision of DIMP services.<br />
• The impact in the changing proportion of female DIMPs. With approximately equal numbers<br />
of male and females in younger age groups, it can be anticipated that the FTE DIMP<br />
workforce would fall (due to females historically working less hours than males).<br />
• The assumption of a fixed level of demand. From recent studies it is evident that demand<br />
will increase with the expected increase in incidence of cancer and the increase in<br />
infrastructure. In addition, with changing technology it can be expected that there would<br />
be an increase in DIMP workload to both implement and maintain these new technologies.<br />
<strong>Health</strong>Consult (2009) identified that more complex technologies will require more staff.<br />
Notwithstanding the limitations outlined above, the projections suggest that the ROMP and DIMP<br />
workforces will not increase significantly – the ROMP projections suggest no change in the short to<br />
medium term and the DIMP projections suggest falling workforce numbers. This indicates the<br />
workforce dynamics indicator assessment conducted in this report are not likely to be impacted.<br />
That is, the areas of significant concern are not likely to reduce in the future compared with current<br />
with the current assessment.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 27
6 Potential paths forward<br />
The workforce dynamics indicator assessment, combined with the additional contextual<br />
information, suggests areas of concern now and into the future for both the ROMP and DIMP<br />
workforces. As such, consideration of future paths forward for the workforces is appropriate. In<br />
considering the future pathway, it is important to recognise what is sustainable, and to examine a<br />
range of options. Applying the response framework adopted for <strong>Health</strong> <strong>Workforce</strong> 2025 11 , there are<br />
four areas of consideration:<br />
1. <strong>Workforce</strong> reform and innovation<br />
2. Reform of training pathways<br />
3. Increased supply through immigration<br />
4. Increased supply through domestic training.<br />
It is likely a combination of all these areas would be required to sustainably move forward.<br />
<strong>Workforce</strong> reform and innovation<br />
<strong>Workforce</strong> reform and innovation can be used to improve flexibility, productivity and retention. The<br />
ROMP and DIMP workforces are small and highly specialised professions with a long training<br />
pathway. As such, it is important they are employed as far as possible on tasks for which only they<br />
have the training and capability to perform. Other tasks can be safely undertaken by less<br />
specialised workers, under appropriate guidance and supervision.<br />
In the case of the medical physicist workforces there is an existing model of this approach – DIMP<br />
services in Tasmania and the Northern Territory are provided by interstate-based DIMPs, who visit<br />
regularly to conduct quality control and audit on site technicians 12 . There are also some centres in<br />
<strong>Australia</strong> employing medical physics technicians to undertake defined tasks, with discussions also<br />
occurring more broadly on the role medical physics assistants or medical physics technicians could<br />
play in easing workforce issues. 13 This suggests there is scope to look at alternative models of<br />
workforce deployment (also enabled by an existing nationally consistent training program). This<br />
could reduce the need for the profession to directly undertake tasks, rather, enabling the<br />
professions to supervise an assistant workforce.<br />
Such alternative models could have a large potential impact on the requirement for ROMPs and<br />
DIMPs, and hence on their workforce dynamics rating assessment.<br />
There is also a high degree of specialisation within such a small overall workforce, with three distinct<br />
sub-specialties (radiation oncology, radiology and nuclear medicine). An examination of whether<br />
this degree of specialisation is required may be appropriate. An option could be a more generalist<br />
medical physicist role, which may be particularly applicable in an environment where the role of<br />
the medical physicist may be more supervisory than operational.<br />
The suggestions above encompass both the ROMP and DIMP workforces. The Radiation Oncology<br />
Reform Implementation Committee (RORIC), responsible for advising on reform initiatives to support<br />
sustainable access to radiotherapy services, has developed the RORIC <strong>Workforce</strong> Reform<br />
Framework. This framework is specific to radiation oncologists, radiation therapists and ROMPs. The<br />
framework specifies four key areas of reform, one of which is <strong>Workforce</strong> reform for more effective,<br />
efficient and accessible service delivery. This is focused on ‘improving the efficient and effective<br />
utilisation of available workforce, through business process improvements, effective application of<br />
11<br />
<strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong> 2012: <strong>Health</strong> <strong>Workforce</strong> 2025 – Doctors, Nurses and Midwives – Volume 1.<br />
12<br />
Personal communication, John Cormack, April 2012.<br />
13<br />
Communication with HWA, ACPSEM, May 2012.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 28
new technology, clinical practice improvements and role redesign.’ While there are no specific<br />
reforms outlined for ROMPs within this, proposals include more actively engaging with stakeholders<br />
to inform best practice models of care, and that innovative approaches are shared across<br />
jurisdictions.<br />
Under the <strong>Workforce</strong> capacity building and skills development area of reform, advanced practice<br />
and extended scope of practice are promoted as ways to expand workforce numbers – creating<br />
positions to perform less specialised tasks currently undertaken by skilled professionals. This is<br />
consistent with HWA’s suggestion above, and while the framework does not suggest specific<br />
reforms, it proposes RORIC will provide information on job redesign potential and examine the<br />
feasibility of the concept (if the proposal is supported). One example already in existence is<br />
advanced roles for radiation therapists, which included the development and evaluation of a<br />
radiation engineering assistant role (with the evaluation report currently being written).<br />
Reform of training pathways<br />
In line with an approach of a more generalist workforce as outlined above, the existing training<br />
pathway for medical physicists could be examined – particularly in terms of training posts which are<br />
currently specific to ROMP and DIMP roles. It should be noted some amalgamation of nuclear<br />
medicine and diagnostic radiology is already occurring, with the design of the DIMP TEAP taking<br />
this into account.<br />
The four to five year training pathway for medical physicists is also relatively long. In a situation<br />
where the profession is identified as potentially vulnerable it may be appropriate to examine<br />
whether it is possible to streamline training to reduce the overall length, while maintaining<br />
appropriate quality standards.<br />
This is consistent with the RORIC <strong>Workforce</strong> Reform Framework, which specifically mentioned<br />
streamlining existing training programs, and for the ROMP workforce in particular, it promoted the<br />
Queensland approach to training, which reduces the traditional ROMP training time by one year.<br />
Increased supply through immigration<br />
The ROMP workforce is already relatively reliant on ITPs (with no information available for the DIMP<br />
workforce). The continued or increased targeting of overseas supply may be useful in the short-term<br />
to fill supply gaps, while workforce and domestic training reforms are established. The medical<br />
physicist occupation is currently included on the general skilled migration skilled occupation list,<br />
which means overseas medical physicists can apply for a permanent visa in <strong>Australia</strong> without<br />
employer sponsorship, and it is also on the employer nomination scheme occupation list. By<br />
appearing on both these lists, the immigration of medical physicists into <strong>Australia</strong> is better enabled.<br />
Increased supply through domestic training<br />
For ROMPs, the replacement rate indicator is at the lowest workforce dynamics rating level, that is,<br />
of minimal concern. However for DIMPs, this indicator was at the highest workforce dynamics rating<br />
level (of significant concern). Therefore it may be appropriate to examine whether additional<br />
training positions should be created to meet long-term supply issues. Any increase in domestic<br />
training should only be considered in combination with the options outlined above. This is to ensure<br />
the opportunity for appropriate reform is not lost by simply taking a ‘more of the same’ approach,<br />
and that the option (or combination of options) chosen, results in a sustainable workforce and<br />
training pathway.<br />
Improved data collection<br />
In addition to the potential paths forward outlined above, there is scope for improved data<br />
collection on the medical physicist workforces, particularly for DIMPs. Reflecting the greater focus<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 29
on the ROMP workforce as a result of the 2002 Report of the radiation oncology inquiry: A vision for<br />
radiotherapy, all indicators for ROMPs were able to be assessed (recognising retirement intentions<br />
were used as a proxy for exits). A key data source on the ROMP workforce was a detailed data<br />
collection conducted as part of the 2009 <strong>Health</strong>Consult review of the radiation oncology<br />
workforce. However for DIMPs, no such data source exists and one of the five workforce dynamic<br />
indicators was not assessed due to data limitations (again also recognising retirement intentions<br />
were used as a proxy for exits). With key data sources for the ROMP and DIMP workforces also<br />
being collected on a different basis, with different data items, this indicates there is a need to<br />
improve the evidence base. Improved data collection would enable monitoring and planning,<br />
and a collection based on national health workforce data items (refer Appendix 1) would also<br />
enable comparability with other health professions.<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 30
Appendix 1 – National Minimum Data Set<br />
The table below provides the <strong>Australia</strong>n <strong>Health</strong> Ministers’ Advisory Council endorsed national<br />
minimum data set items. A proposed data dictionary for medical physicists for each of these data<br />
is included.<br />
Data item Collection Proposed Data Dictionary<br />
Sex One-off Male/ female<br />
Age Derived Month and year of birth<br />
State/Territory of birth One-off If <strong>Australia</strong>n born<br />
Country of birth One-off If overseas born, SACC (4 digit code) (a)<br />
Indigenous status One-off For <strong>Australia</strong>n born<br />
Residential address Annual Postcode, suburb/ locality<br />
Permanent residency status Annual If overseas born, No/Yes<br />
Visa type<br />
Annual<br />
1 st qualification One-off<br />
Year of 1 st qualification<br />
One-off<br />
If not permanent resident, category of Visa (or travel<br />
authority)<br />
First post-secondary qualification that enables working as<br />
<strong>Medical</strong> <strong>Physicist</strong><br />
Country of 1 st qualification One-off If overseas trained, SACC (4 digit code)*<br />
State/Territory of 1 st qualification One-off If <strong>Australia</strong>n trained<br />
Additional qualification<br />
Labour force status<br />
Hours worked by work location<br />
Hours worked by work sector<br />
Hours worked by principal area<br />
Hours worked by specialty area<br />
Annual<br />
Annual<br />
Annual<br />
Annual<br />
Annual<br />
Annual<br />
Employed in MP (including on leave for less 3 months)<br />
Employed in MP but on leave for 3+ months<br />
Not working in MP – o/s in MP/other employment<br />
Not working - unemployed /retired<br />
(If not working in MP in <strong>Australia</strong>)<br />
Looking for work in MP in <strong>Australia</strong> – Yes/No<br />
Work location – main / 2 nd Annual State/postcode/ suburb/ locality<br />
Work sector – main / 2 nd Annual Public/ private<br />
Principal role – main / 2 nd Annual Clinician/ Administrator/ Teaching/ Research<br />
Specialty area – main / 2 nd Annual Radiation oncology/ Radiology/ Nuclear medicine<br />
Work setting – main / 2 nd Annual Classification to be determined in consultation with ACPSEM<br />
Number years worked in MP<br />
Years intended to remain in in MP<br />
Annual<br />
Annual<br />
(a) ABS. Standard <strong>Australia</strong>n Classification of Countries, Second Edition. Cat. No. 1269.0: 2011<br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 31
References<br />
<strong>Australia</strong>n Radiation Protection & Nuclear Safety Agency. Radiation Protection Series No. 14. Code<br />
of Practice: Radiation Protection in the <strong>Medical</strong> Applications of Ionizing Radiation, 2008.<br />
Baume P. A Vision for Radiotherapy. Report of the Radiation Oncology Inquiry. Canberra:<br />
Department of <strong>Health</strong> and Ageing, June 2002.<br />
Cancer <strong>Australia</strong>. Cancer <strong>Australia</strong> Strategic Plan 2011-2014. Sydney: Cancer <strong>Australia</strong>, 2011.<br />
<br />
Cormack J. Editorial: the ACPSEM diagnostic imaging TEAP project. Australasian Physical &<br />
Engineering Sciences in Medicine 2011; 34: 173-8.<br />
<strong>Health</strong>Consult. Radiation Oncology <strong>Workforce</strong> Planning. Final Report for Department of <strong>Health</strong> and<br />
Ageing. Sydney: <strong>Health</strong>Consult, November 2009.<br />
<strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong>. <strong>Health</strong> <strong>Workforce</strong> 2025 – Doctors, Nurses and Midwives – Volume 1.<br />
Adelaide: HWA, 2012. <br />
Radiation Oncology Reform Implementation Committee. Radiation Oncology Reform<br />
Implementation Committee (RORIC) <strong>Workforce</strong> Reform Framework. Canberra: Department of<br />
<strong>Health</strong> and Ageing, 2011.<br />
Round WH. A survey of the Australasian clinical medical physics and biomedical engineering<br />
workforce. Australasian Physical & Engineering Sciences in Medicine 2007; 30: 13-24.<br />
Round WH. A 2009 survey of the Australasian clinical medical physics and biomedical engineering<br />
workforce. Australasian Physical & Engineering Sciences in Medicine 2010; 33: 153-62.<br />
Victorian Government. Victorian Radiotherapy Service Plan, July 2007. Victoria: Department of<br />
Human Services, 2008. < http://www.health.vic.gov.au/radiotherapy/radiotherapy-serviceplan06-11.pdf><br />
<strong>Medical</strong> <strong>Physicist</strong> <strong>Workforce</strong> <strong>Study</strong> 32
<strong>Health</strong> <strong>Workforce</strong> <strong>Australia</strong><br />
GPO Box 2098, Adelaide SA 5001<br />
T +61 8 8409 4500 F +61 8 8212 3841<br />
E hwa@hwa.gov.au<br />
Printed on 100% post-consumer recycled paper