CHN5140 Magnesium Sulfate for Preterm Labor.pdf - Carondelet
CHN5140 Magnesium Sulfate for Preterm Labor.pdf - Carondelet
CHN5140 Magnesium Sulfate for Preterm Labor.pdf - Carondelet

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
STAT/NOW<br />
(Check Box to Left)<br />
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
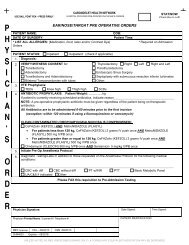
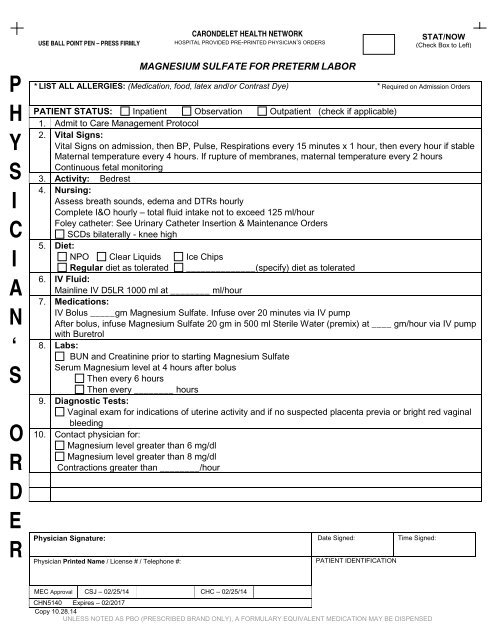
MAGNESIUM SULFATE FOR PRETERM LABOR<br />
* LIST ALL ALLERGIES: (Medication, food, latex and/or Contrast Dye) * Required on Admission Orders<br />
PATIENT STATUS: Inpatient Observation Outpatient (check if applicable)<br />
1. Admit to Care Management Protocol<br />
2. Vital Signs:<br />
Vital Signs on admission, then BP, Pulse, Respirations every 15 minutes x 1 hour, then every hour if stable<br />
Maternal temperature every 4 hours. If rupture of membranes, maternal temperature every 2 hours<br />
Continuous fetal monitoring<br />
3. Activity: Bedrest<br />
4. Nursing:<br />
Assess breath sounds, edema and DTRs hourly<br />
Complete I&O hourly – total fluid intake not to exceed 125 ml/hour<br />
Foley catheter: See Urinary Catheter Insertion & Maintenance Orders<br />
SCDs bilaterally - knee high<br />
5. Diet:<br />
NPO Clear Liquids Ice Chips<br />
Regular diet as tolerated ______________(specify) diet as tolerated<br />
6. IV Fluid:<br />
Mainline IV D5LR 1000 ml at ________ ml/hour<br />
7. Medications:<br />
IV Bolus _____gm <strong>Magnesium</strong> <strong>Sulfate</strong>. Infuse over 20 minutes via IV pump<br />
After bolus, infuse <strong>Magnesium</strong> <strong>Sulfate</strong> 20 gm in 500 ml Sterile Water (premix) at ____ gm/hour via IV pump<br />
with Buretrol<br />
8. Labs:<br />
BUN and Creatinine prior to starting <strong>Magnesium</strong> <strong>Sulfate</strong><br />
Serum <strong>Magnesium</strong> level at 4 hours after bolus<br />
Then every 6 hours<br />
Then every ________ hours<br />
9. Diagnostic Tests:<br />
Vaginal exam <strong>for</strong> indications of uterine activity and if no suspected placenta previa or bright red vaginal<br />
bleeding<br />
10. Contact physician <strong>for</strong>:<br />
<strong>Magnesium</strong> level greater than 6 mg/dl<br />
<strong>Magnesium</strong> level greater than 8 mg/dl<br />
Contractions greater than ________/hour<br />
Physician Signature: Date Signed: Time Signed:<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 02/25/14 CHC – 02/25/14<br />
<strong>CHN5140</strong> Expires – 02/2017<br />
Copy 10.28.14<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
STAT/NOW<br />
(Check Box to Left)<br />
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
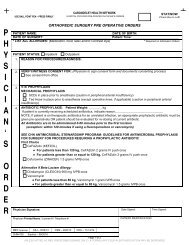
URINARY CATHETER INSERTION/MAINTENANCE ORDERS<br />
Urinary Catheter Insertion/Maintenance Options<br />
1. Urinary Catheter Insertion OR Urinary Catheter to Dependent Drainage<br />
Select urinary catheter indication:<br />
GU/GYN/Perineal Procedure<br />
Gross hematuria<br />
Acute urinary retention<br />
Bladder outlet obstruction<br />
Continuous IV infusion of diuretic<br />
Continuous IV infusion of paralytic<br />
Continuous IV infusion of vasopressor/inotropic<br />
Mechanical ventilation with order <strong>for</strong> deep sedation (RASS = -4 or -5)<br />
Prolonged immobility potentially related to unstable thoracic or lumbar spine, multiple traumatic injuries,<br />
hip fractures, etc<br />
End of life/com<strong>for</strong>t care<br />
Urinary catheter placed by urologist<br />
Urinary incontinence with Stage III or greater pressure ulcers<br />
Other: _______________________________________________________________<br />
Urinary Catheter Removal Options<br />
2. Discontinue Urinary Catheter if no indication <strong>for</strong> use per protocol<br />
Discontinue Urinary Catheter on Date: ______________ at Time: _____________<br />
Do Not Discontinue Urinary Catheter until further orders from provider<br />
When urinary catheter discontinued:<br />
Initiate Bladder Scan Protocol<br />
Per<strong>for</strong>m Bladder Scan 4 hours after removal if no void. Straight cath if volume greater than _____ mL.<br />
Nursing Tasks<br />
3. Assess and document Urinary Catheter Indication now and qshift (0900 and 2100) thereafter<br />
CSJ Only:<br />
If unable to place urinary catheter after one attempt, activate RN Foley Team and initiate protocol as needed<br />
Medications<br />
4. Lidocaine 2% gel transurethral.<br />
- Fill urethra 10 to 15 minutes prior to urinary catheter insertion. May repeat x 1.<br />
Physician Signature: Date Signed: Time Signed:<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
Approved 8/28/14<br />
CHN2212 Expires – 08/2017<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED