CHN4100 Orthopedic Surgery Pre Operative Orders.pdf - Carondelet
CHN4100 Orthopedic Surgery Pre Operative Orders.pdf - Carondelet
CHN4100 Orthopedic Surgery Pre Operative Orders.pdf - Carondelet

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
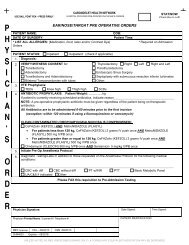
ORTHOPEDIC SURGERY PRE OPERATIVE ORDERS<br />
5. For documented High Risk MRSA:<br />
Vancomycin AND CeFAZolin (KEFZOL)<br />
• For patients less than 80 kg, Vancomycin 1 gram IVPB once<br />
• For patients greater than or equal to 80 kg, Vancomycin 1.5 grams IVPB once<br />
AND<br />
• For patients less than 120 kg, CeFAZolin (KEFZOL) 2 grams IV push once<br />
• For patients greater than or equal to 120kg, CeFAZolin (KEFZOL) 3 grams IV push once<br />
STAT/NOW<br />
(Check Box to Left)<br />
Vancomycin reasons: Must have physician/APN/PA documentation<br />
Beta-lactam (penicillin or cephalosporin) allergy<br />
MRSA colonization or infection<br />
High risk due to acute inpatient hospitalization within last year prior to admission<br />
High risk due nursing home or extended care facility within last year prior to admission<br />
Facility wide or operation-specific increased MRSA rate<br />
Chronic wound care or dialysis<br />
Continuous inpatient stay of more than 24 hours prior to principal procedure<br />
Transfer of patient following a 3-day inpatient hospitalization at another facility<br />
Other Reason_____________________________________________<br />
6. INITIATE PRE-OP ANESTHESIA PROTOCOL<br />
7. Diagnostic Testing/Labs in addition to those requested on the <strong>Pre</strong>-Op Anesthesia Protocol for the following<br />
medical conditions:<br />
1) ______________________________________________________________<br />
2) ______________________________________________________________<br />
8. Blood Draw<br />
CBC with diff<br />
BUN/Creatinine<br />
Liver Profile (BILI & BILC)<br />
Potassium<br />
Basic Metabolic Panel<br />
Comprehensive Metabolic Panel<br />
Type & Screen<br />
Blood Bank Hold Clot<br />
Type & Cross ______ units<br />
PT/INR day of surgery<br />
PTT<br />
HgbA1C<br />
POC<br />
Urine <strong>Pre</strong>gnancy Test<br />
Other<br />
UA, C&S if positive<br />
MRSA Swab<br />
CXR<br />
ECG<br />
9. For Total Joint Replacement <strong>Surgery</strong>: <strong>Pre</strong> Op Evaluation by CHN Surgical Nurse Practitioner, <strong>Pre</strong> <strong>Operative</strong><br />
Assessment Clinic<br />
10. For Total Joint Replacement <strong>Surgery</strong>: Schedule patient for Joint Camp through <strong>Orthopedic</strong> Unit coordinator<br />
11. Other <strong>Orders</strong>:<br />
Physician Signature: Date Signed: Time Signed:<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 8/22/13 CSM – 9/26/13 CHC – 11/14/14<br />
<strong>CHN4100</strong> Expires – 09/2016<br />
Page 2 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED