CHN4523 Spinal Surgery Pre-op Orders.pdf - Carondelet
CHN4523 Spinal Surgery Pre-op Orders.pdf - Carondelet
CHN4523 Spinal Surgery Pre-op Orders.pdf - Carondelet

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
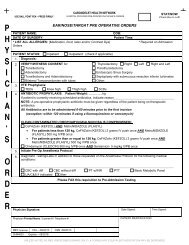
SPINAL SURGERY PRE OPERATIVE ORDERS<br />
Physician Signature: Date Signed: Time Signed:<br />
STAT/NOW<br />
(Check Box to Left)<br />
PATIENT NAME:<br />
DOB:<br />
DATE OF SURGERY: ________________________________________ Patient Time: _________________<br />
* LIST ALL ALLERGIES: (Medication, food, latex and/or Contrast Dye) * Required on Admission <strong>Orders</strong><br />
PATIENT STATUS: Inpatient Outpatient<br />
1. REASON FOR PROCEDURE:<br />
2. VERIFY/WITNESS CONSENT FOR:<br />
See consent from office<br />
3. Please instruct patient on use of incentive spirometry<br />
4. VTE PROPHYLAXIS:<br />
Thigh high TEDS OR Calf high TEDS<br />
• SCDs in place and functioning prior to anesthesia<br />
5. NPO except sips of water with BETA BLOCKER<br />
If patient is on a BETA BLOCKER at home, record time and date of last dose on med reconciliation form<br />
If patient is on a BETA BLOCKER and they have not taken in the last 24 hours, notify anesthesia ASAP<br />
6. ANTIBIOTIC PROPHYLAXIS: Patient Weight: ________kg<br />
If patient is currently receiving scheduled antibiotics, indicate reason____________________________<br />
NOTE: A pre-<strong>op</strong>erative pr<strong>op</strong>hylactic antibiotic must be given regardless of the patient being on therapeutic<br />
antibiotics.<br />
All Antibiotics are to be administered 0-60 minutes prior to the first incision<br />
(exception: within 120 minutes if using a fluoroquinolone or vancomycin)<br />
First Choice<br />
CeFAZolin (KEFZOL)<br />
• For patients less than 120 kg, CeFAZolin (KEFZOL) 2 grams IV push once<br />
• For patients greater than or equal to 120 kg, CeFAZolin (KEFZOL) 3 grams IV push once<br />
Cefuroxime (ZINACEF) 1.5 grams IVPB once<br />
7. Alternative if Beta Lactam Allergy<br />
Clindamycin (CLEOCIN) 900 mg IVPB once AND Gentamicin 5 mg/kg IVPB once<br />
Clindamycin (CLEOCIN) 900 mg IVPB once AND Ciprofloxacin (CIPRO) 400 mg IVPB once<br />
Vancomycin AND Gentamicin<br />
For patients less than 80 kg, Vancomycin 1 gram IVPB once AND Gentamicin 5 mg/kg IVPB once<br />
• For patients greater than or equal to 80 kg, Vancomycin 1.5 grams IVPB once AND Gentamicin 5 mg/kg<br />
IVPB once<br />
Vancomycin AND Ciprofloxacin<br />
For patients less than 80 kg, Vancomycin 1 gram IVPB once AND Ciprofloxacin (CIPRO) 400 mg IVPB<br />
once<br />
• For patients greater than or equal to 80 kg, Vancomycin 1.5 grams IVPB once AND Ciprofloxacin<br />
(CIPRO) 400 mg IVPB once<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 08/22/13 CSM – 09/26/13<br />
<strong>CHN4523</strong> Expires – 09/2016<br />
Page 1 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
SPINAL SURGERY PRE OPERATIVE ORDERS<br />
Physician Signature: Date Signed: Time Signed:<br />
STAT/NOW<br />
(Check Box to Left)<br />
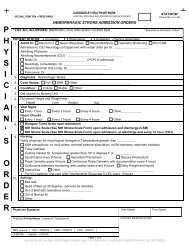
8. For documented High Risk MRSA<br />
Vancomycin AND CeFAZolin (KEFZOL)<br />
• For patients less than 80 kg, Vancomycin 1 gram IVPB once<br />
• For patients greater than or equal to 80 kg, Vancomycin 1.5 grams IVPB once<br />
AND<br />
• For patients less than 120 kg, CeFAZolin (KEFZOL) 2 grams IV push once<br />
For patients greater than or equal to 120kg, CeFAZolin (KEFZOL) 3 grams IV push once<br />
Note: Consider Vancomycin pr<strong>op</strong>hylaxis if anticipating extensive hardware placement and patient has risk factors<br />
Vancomycin reasons: Must have physician/APN/PA documentation<br />
MRSA colonization or infection<br />
High risk due to acute inpatient hospitalization within last year prior to admission<br />
High risk due to nursing home or extended care facility stay within last year prior to admission<br />
Facility wide or <strong>op</strong>eration-specific increased MRSA rate<br />
Chronic wound care or dialysis<br />
Continuous inpatient stay of more than 24 hours prior to principal procedure<br />
Transfer of patient following a 3-day inpatient hospitalization at another facility<br />
Other Reason: ___________________________________________________________<br />
Consider a pre-<strong>op</strong>erative prescription for Mupirocin ointment BID intranasally for 5 days prior to surgery<br />
and a Hibiclens shower.<br />
9. Initiate Anesthesia Protocol and perform Labs and ECG per protocol<br />
10. Surgeon requests the following Diagnostic Testing/Labs for the following medical conditions:<br />
___________________________________________________________________________________________<br />
STUDIES: ECG CXR<br />
LABS:<br />
11. Other <strong>Orders</strong>:<br />
CBC with diff<br />
CMP<br />
BMP<br />
Liver Profile (BILI & BILC)<br />
PT/INR<br />
PTT<br />
HgbA1C<br />
Type & Screen<br />
Blood Bank Hold Clot<br />
Type & Cross ______ units of PRBC<br />
UA, C&S if positive<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 08/22/13 CSM – 09/26/13<br />
<strong>CHN4523</strong> Expires – 09/2016<br />
Page 2 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
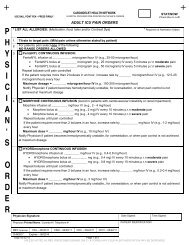
TREATMENT PROTOCOL – PRE OP ANESTHESIA (CSJ/CSM)<br />
1 Order to initiate <strong>Pre</strong>Op Anesthesia Protocol was previously given by a Licensed Independent Practitioner and signed on<br />
a separate <strong>Orders</strong> page unless box below is checked.<br />
Initiate <strong>Pre</strong>Op Anesthesia Protocol – checkmark here requires physician signature, date, time on bottom of page<br />
2 NPO Status: Per table on page 2<br />
3 Medications: Take all prescription medications on day of surgery with a sip of water EXCEPT:<br />
• Metformin (Gluc<strong>op</strong>hage) and other oral diabetic<br />
medications<br />
• Any medication that needs to be taken with food<br />
4 Other Special Medications:<br />
• Anticoagulants as per surgeon, cardiologist or PCP<br />
• Aspirin and Cl<strong>op</strong>idogrel (Plavix) should be taken up to the<br />
day of surgery unless specifically instructed by physician<br />
• Insulin; unless given specific instructions by PCP,<br />
attending or Hospitalist<br />
• Diuretics<br />
• Herbals, vitamins and supplements, and weight loss drugs:<br />
Should be st<strong>op</strong>ped 2 weeks prior to surgery<br />
• Diabetics: If AM blood glucose low, may take clear liquids<br />
with sugar<br />
5. If patient is on a BETA BLOCKER at home, record time and date of last dose in Medication history<br />
If patient is on a BETA BLOCKER and they have not taken it in the last 24 hours, notify anesthesia ASAP<br />
6. Start IV in pre-<strong>op</strong> holding, Lactated Ringers at 25 mL/hour (TKO)<br />
If renal dialysis and/or renal failure patient: Start IV with 0.9% Sodium Chloride at 25 mL/hour (TKO)<br />
(may use 0.5 mL 1% Lidocaine for skin wheal)<br />
Note: All testing must be based on known medical conditions, either documented in a physician’s H & P or the medical<br />
record, or reported by a patient as an established diagnosis. Contact the anesthesiologist directly for any testing not indicated<br />
by the protocol.<br />
7. LAB: Lab testing may be obtained through Laboratory analysis, Point of Care, or Fingerstick testing<br />
A checkmark in the box indicates that Lab test was done after Protocol was initiated<br />
K+ (Potassium) within one week prior to surgery if on Digoxin or Diuretics<br />
K+ (Potassium) day of surgery if renal dialysis and/or renal failure patient<br />
PT/INR day of surgery if on Warfarin (COUMADIN) within the last 7 days prior to surgery<br />
<strong>Pre</strong>gnancy test if female of child bearing years (onset of menses to no menses for 1 year) and no hysterectomy<br />
Hgb/Hct within one week (day of surgery with active bleeding) in patients with documented history of liver disease,<br />
anemia or bleeding disorder or if indicated by type/invasiveness of surgery (see page 2).<br />
Blood bank orders (if indicated on page 2): Hold Clot Type and screen Type and Cross 2 units PRBC’s<br />
Blood glucose within 2 hours of surgery for diabetic patients<br />
FOR CARDIOTHORACIC SURGERY ONLY:<br />
ACT if patient is on Heparin infusion<br />
Platelet Works if patient received Plavix or ASA within 1 week before cardiac surgery<br />
8. ECG: Needed within 90 days for the following patients:<br />
a) Patients undergoing cardiac or vascular surgical procedures<br />
b) Patients with a pacemaker or AICD except those undergoing intraocular or endosc<strong>op</strong>ic procedures<br />
c) Patients with any of the following cardiovascular risk factors undergoing INPATIENT surgical procedures:<br />
• coronary artery disease<br />
(MI/PCI/stents/history of arrhythmia)<br />
• cerebrovascular disease (TIA/CVA)<br />
• diabetes mellitus<br />
• peripheral artery disease<br />
• heart failure<br />
• renal insufficiency or failure<br />
9. NOTIFY: Anesthesiologist of record, or on-call anesthesiologist, for abnormal values or for clarification of protocol<br />
• K+ level less than 3.0 mmol/L or greater than 5.0 mmol/L<br />
• INR greater than 1.5<br />
• Positive pregnancy test<br />
• Hgb less than 10 gram/dL or greater than 19 gram/dL<br />
• Blood Glucose less than 60 mg/dL or greater than 200 mg/dL<br />
10. CHG: 2% Chlorhexidine Gluconate (CHG) wipes per policy<br />
CSM Only: 0.12% CHG mouthwash (PERIDEX) 15 mL to brush teeth, then 1 minute swish and spit<br />
Nurse Signature per physician order: Nurse Printed Name: Date Signed: Time Signed:<br />
Physician’s Signature if #1 box is checked Physician’s Printed Name if #1 box is checked PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 06/26/14 CSM – 06/26/14<br />
CHN8215 Expires – 06/2017<br />
C<strong>op</strong>y 08.11.14 Page 1 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
TREATMENT PROTOCOL – PRE OP ANESTHESIA (CSJ/CSM)<br />
WILL BE APPENDED TO THE FOLLOWING PREPRINTED ORDERS THAT REFERENCE “ANESTHESIA PROTOCOL”:<br />
SHOCK WAVE LITHOTRIPSY, GENERAL SURGERY PRE OPERATIVE ORDERS – CSJ / CSM, SLEEVE GASTRECTOMY PRE OPERATIVE ORDERS,VASCULAR SURGERY<br />
PRE-OP ORDERS, PERI-OPERATIVE EXCISION OF PTERYGIUM ORDERS, PRE OPERATIVE E.N.T ORDERS, PRE-OP ORTHOPEDIC SURGERY ORDERS, RETINA<br />
PERIOPERATIVE ORDERS – CSJ, TRABECULECTOMY PERI-OPERATIVE ORDERS,PODIATRY PERIOPERATIVE ORDERS, EAR/NOSE/THROAT (ENT) PERIOPERATIVE<br />
ORDERS –CSJ, OPHTHALMOLOGY PERIOPERATIVE ORDERS-CSJ, GYN PREOPERATIVE ORDERS – CSJ<br />
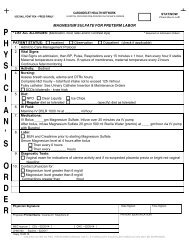
NPO Status Instructions to Patient Minimum Period<br />
Clear liquids (black coffee, apple juice, grape juice) Up to 4 hours pre-<strong>op</strong> 2 hours<br />
Breast milk Up to 4 hours pre-<strong>op</strong> 4 hours<br />
Infant formula Up to 6 hours pre-<strong>op</strong> 6 hours<br />
Light meal (Dry toast and clear liquids) None after midnight 6 hours<br />
Fried or fatty food and meat (includes milk products) None after midnight 8 hours<br />
Solids in high risk patients (e.g.: diabetes, pregnancy, obesity) None after midnight 8 hours<br />
PRE-OPERATIVE HGB/HCT and BLOOD BANK REQUIREMENTS<br />
<strong>Surgery</strong><br />
MAJOR ABDOMINAL:<br />
Whipple<br />
Splenectomy<br />
Gastrectomy<br />
Abdominal perineal resection<br />
Bleeding ulcer<br />
Adrenalectomy<br />
Es<strong>op</strong>hagogastrectomy<br />
Hysterectomy<br />
Colectomy<br />
VASCULAR:<br />
AAA, <strong>op</strong>en abdominal<br />
AAA, endovascular<br />
Any bypass case<br />
Any endarterectomy<br />
Aneurysmal repairs<br />
Repair/excision of infected grafts<br />
BKA/AKA<br />
CARDIOTHORACIC:<br />
Cardiac Surgeries<br />
Thoracic Surgeries<br />
ORTHOPAEDIC:<br />
Total Hip/Knee Arthr<strong>op</strong>lasty<br />
Hip Fracture/Revision<br />
Spine surgery (2 or more levels)<br />
Other Total Joints<br />
UROLOGICAL:<br />
Nephrectomy<br />
Cystectomy<br />
Prostatectomy<br />
TURP<br />
NEUROLOGIC:<br />
Craniotomy<br />
Spine surgery (2 or more levels)<br />
Aneurysm repair/clipping<br />
PLASTICS:<br />
TRAM<br />
<strong>Pre</strong>ssure ulcers<br />
Type & Cross<br />
2 units PRBCs<br />
And HGB/HCT<br />
X<br />
X<br />
X<br />
Type & Screen<br />
And HGB/HCT<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
X<br />
HGB/HCT & Hold Clot<br />
(if HGB/HCT