CHN4104 Hip Fracture Admission Orders.pdf - Carondelet
CHN4104 Hip Fracture Admission Orders.pdf - Carondelet
CHN4104 Hip Fracture Admission Orders.pdf - Carondelet

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
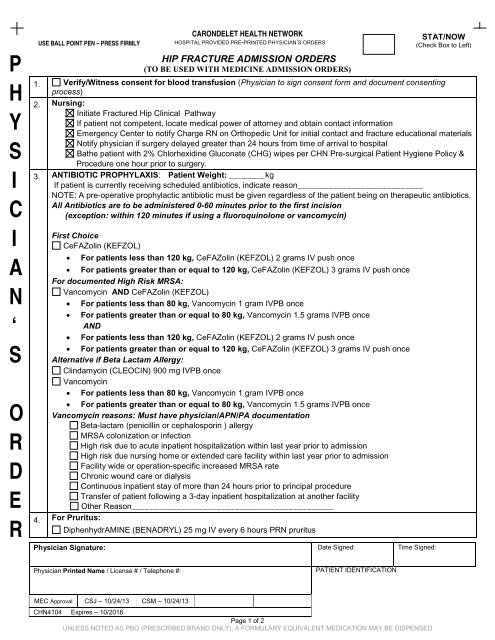
HIP FRACTURE ADMISSION ORDERS<br />
(TO BE USED WITH MEDICINE ADMISSION ORDERS)<br />
Physician Signature: Date Signed: Time Signed:<br />
STAT/NOW<br />
(Check Box to Left)<br />
1. Verify/Witness consent for blood transfusion (Physician to sign consent form and document consenting<br />
process)<br />
2. Nursing:<br />
Initiate <strong>Fracture</strong>d <strong>Hip</strong> Clinical Pathway<br />
If patient not competent, locate medical power of attorney and obtain contact information<br />
Emergency Center to notify Charge RN on Orthopedic Unit for initial contact and fracture educational materials<br />
Notify physician if surgery delayed greater than 24 hours from time of arrival to hospital<br />
Bathe patient with 2% Chlorhexidine Gluconate (CHG) wipes per CHN Pre-surgical Patient Hygiene Policy &<br />
Procedure one hour prior to surgery.<br />
3. ANTIBIOTIC PROPHYLAXIS: Patient Weight: ________kg<br />
If patient is currently receiving scheduled antibiotics, indicate reason____________________________<br />
NOTE: A pre-operative prophylactic antibiotic must be given regardless of the patient being on therapeutic antibiotics.<br />
All Antibiotics are to be administered 0-60 minutes prior to the first incision<br />
(exception: within 120 minutes if using a fluoroquinolone or vancomycin)<br />
First Choice<br />
CeFAZolin (KEFZOL)<br />
• For patients less than 120 kg, CeFAZolin (KEFZOL) 2 grams IV push once<br />
• For patients greater than or equal to 120 kg, CeFAZolin (KEFZOL) 3 grams IV push once<br />
For documented High Risk MRSA:<br />
Vancomycin AND CeFAZolin (KEFZOL)<br />
• For patients less than 80 kg, Vancomycin 1 gram IVPB once<br />
• For patients greater than or equal to 80 kg, Vancomycin 1.5 grams IVPB once<br />
AND<br />
• For patients less than 120 kg, CeFAZolin (KEFZOL) 2 grams IV push once<br />
• For patients greater than or equal to 120 kg, CeFAZolin (KEFZOL) 3 grams IV push once<br />
Alternative if Beta Lactam Allergy:<br />
Clindamycin (CLEOCIN) 900 mg IVPB once<br />
Vancomycin<br />
• For patients less than 80 kg, Vancomycin 1 gram IVPB once<br />
• For patients greater than or equal to 80 kg, Vancomycin 1.5 grams IVPB once<br />
Vancomycin reasons: Must have physician/APN/PA documentation<br />
Beta-lactam (penicillin or cephalosporin ) allergy<br />
MRSA colonization or infection<br />
High risk due to acute inpatient hospitalization within last year prior to admission<br />
High risk due nursing home or extended care facility within last year prior to admission<br />
Facility wide or operation-specific increased MRSA rate<br />
Chronic wound care or dialysis<br />
Continuous inpatient stay of more than 24 hours prior to principal procedure<br />
Transfer of patient following a 3-day inpatient hospitalization at another facility<br />
Other Reason_____________________________________________<br />
4. For Pruritus:<br />
DiphenhydrAMINE (BENADRYL) 25 mg IV every 6 hours PRN pruritus<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 10/24/13 CSM – 10/24/13<br />
<strong>CHN4104</strong> Expires – 10/2016<br />
Page 1 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED
P<br />
H<br />
Y<br />
S<br />
I<br />
C<br />
I<br />
A<br />
N<br />
‘<br />
S<br />
O<br />
R<br />
D<br />
E<br />
R<br />
USE BALL POINT PEN – PRESS FIRMLY<br />
CARONDELET HEALTH NETWORK<br />
HOSPITAL PROVIDED PRE-PRINTED PHYSICIAN’S ORDERS<br />
HIP FRACTURE ADMISSION ORDERS<br />
(TO BE USED WITH MEDICINE ADMISSION ORDERS)<br />
STAT/NOW<br />
(Check Box to Left)<br />
5. For Pain:<br />
Ketorolac (TORADOL) 30 mg IV now, then 15 mg IV every 6 hours x 24 hours<br />
Choose one<br />
Severe Pain (Prescribe One):<br />
Morphine 2 mg IV every hour PRN severe pain. May repeat once within same one hour time frame. If patient<br />
does not achieve acceptable pain relief after repeat dose, notify physician for further orders.<br />
Morphine _________ mg IV every __________ hour(s) PRN severe pain.<br />
HydroMORPHone (DILAUDID) 0.5 mg IV every 4 hours PRN severe pain. May repeat once within same four<br />
hour time frame. If patient does not achieve acceptable pain relief after repeat dose notify physician for further<br />
orders. Max Dose: 1 mg in four hours.<br />
Moderate Pain (PRIORITIZE and Check one box within each category):<br />
____ Acetaminophen 325 mg/OXYcodone 5 mg (PERCOCET)<br />
1 tablet PO every 4 hours PRN moderate pain. May repeat once within same four hour time frame. If<br />
patient does not achieve acceptable pain relief after repeat dose, notify physician for further orders.<br />
(Total Acetaminophen not to exceed 4 grams/day).<br />
2 tablets PO every 4 hours PRN moderate pain. (Total Acetaminophen not to exceed 4<br />
grams/day)<br />
____ Acetaminophen 325 mg/HydroCODONE 5 mg<br />
1 tablet PO every 4 hours PRN moderate pain. May repeat once within same four hour time frame. If<br />
patient does not achieve acceptable pain relief after repeat dose, notify physician for further orders.<br />
(Total Acetaminophen not to exceed 4 grams/day)<br />
2 tablets PO every 4 hours PRN moderate pain. (Total Acetaminophen not to exceed 4<br />
grams/day)<br />
____ Morphine ________ mg IV every ______ hours PRN moderate pain. May repeat once within same time<br />
frame.<br />
Other (No range order accepted) Drug ______________________ Dose _____ Route_____<br />
every ______ hours ____ PRN (indication) ____________________________<br />
6. INITIATE PREOP ANESTHESIA PROTOCOL (SEE CHN8215)<br />
7. Do not start anticoagulants until after surgery<br />
VTE Mechanical Prophylaxis<br />
TED hose on unaffected limb (caution in peripheral arterial insufficiency) Calf high Thigh high<br />
SCDs on unaffected limb (caution in peripheral arterial insufficiency)<br />
8. Labs: SAIL tests on blood already drawn in the EC, if possible<br />
Blood Bank Hold Clot<br />
Vitamin D (25 hydroxy) Level<br />
Other _____________________________________________________________<br />
9. Consultant: ________________________________ Indication: ___________________________________<br />
Notified: (Date) _________________ (Time) ____________________<br />
10. Other <strong>Orders</strong>:<br />
Physician Signature: Date Signed: Time Signed:<br />
Physician Printed Name / License # / Telephone #:<br />
PATIENT IDENTIFICATION<br />
MEC Approval CSJ – 10/24/13 CSM – 10/24/13<br />
<strong>CHN4104</strong> Expires – 10/2016<br />
Page 2 of 2<br />
UNLESS NOTED AS PBO (PRESCRIBED BRAND ONLY), A FORMULARY EQUIVALENT MEDICATION MAY BE DISPENSED