Diapositiva 1 - Università degli Studi di Perugia
Diapositiva 1 - Università degli Studi di Perugia
Diapositiva 1 - Università degli Studi di Perugia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Università <strong>degli</strong> <strong>Stu<strong>di</strong></strong> <strong>di</strong> <strong>Perugia</strong><br />
Encefaliti<br />
Prof. Paolo Calabresi<br />
Corso Integrato <strong>di</strong> Neurologia
ENCEPHALITIS<br />
1. Encephalitis, an inflammation of the brain parenchyma,<br />
presents as <strong>di</strong>ffuse and/or focal neuropsychological<br />
dysfunction.<br />
2. From an epidemiologic and pathophysiologic perspective,<br />
encephalitis is <strong>di</strong>stinct from meningitis, though on clinical<br />
evaluation the 2 often coexist with signs and symptoms of<br />
meningeal inflammation, such as photophobia, headache,<br />
or a stiff neck.<br />
3. Cerebritis describes the stage prece<strong>di</strong>ng abscess<br />
formation and implies a highly destructive bacterial<br />
infection of brain tissue, whereas acute encephalitis is<br />
most commonly a viral infection with parenchymal damage<br />
varying from mild to profound.
1. Of the subacute and chronic encephalopathies, the ED<br />
physician is most likely to encounter toxoplasmosis in<br />
immunocompromised patients.<br />
2. No satisfactory treatment exists for the relatively common<br />
acute arboviral encephalitides, which vary in epidemiology,<br />
mortality, and morbi<strong>di</strong>ty, if not clinical presentation.<br />
3. Clinically <strong>di</strong>stinguishing these acute arboviral encephalitides<br />
from the 2 potentially treatable acute viral encephalitides is<br />
important. The latter encephalitides include herpes simplex<br />
encephalitis (HSE), which is a spora<strong>di</strong>c and lethal <strong>di</strong>sease of<br />
neonates and the general population, and the less common<br />
varicella-zoster encephalitis, which is deadly in<br />
immunocompromised patients.
1. Swift identification and imme<strong>di</strong>ate treatment can be<br />
lifesaving.<br />
2. Most authorities advocate initiating ED treatment<br />
with the relatively safe acyclovir in any patient<br />
whose CNS presentations (particularly<br />
encephalopathy and focal fin<strong>di</strong>ngs) have no<br />
apparent explanation and in all neonates who<br />
appear ill and are without a final <strong>di</strong>agnosis.
1. In 1999, a late summer outbreak of West Nile encephalitis<br />
(WNE), an arbovirus not found previously in the United States,<br />
was implicated in several deaths in New York.<br />
2. By late summer 2002, West Nile virus has been identified<br />
throughout the eastern and southeastern United States.<br />
3. Following bird migration, the virus is presently exten<strong>di</strong>ng<br />
westward, and by April 2003, virus activity had been detected<br />
in 46 states and the District of Columbia.<br />
4. An updated Centers for Disease Control and Prevention (CDC)<br />
report for 2007 (West Nile Virus Update) includes<br />
information regar<strong>di</strong>ng viremic blood donors.<br />
5. Throughout the world, outbreaks of WNE have been<br />
associated with severe neurologic <strong>di</strong>sease; though, in general,<br />
only 1 in 150 affected patients develop symptomatic WNE.
1. Determining the true incidence is impossible because reporting policies<br />
are neither standar<strong>di</strong>zed nor rigorously enforced.<br />
2. In the United States, several thousand cases of viral encephalitis are<br />
reported yearly. This is probably a fraction of the actual number of<br />
cases.<br />
3. HSE, the most common cause of spora<strong>di</strong>c encephalitis in Western<br />
countries, is relatively rare; the overall incidence is 0.2 per 100,000<br />
(neonatal HSV infection occurs in 2-3 per 10,000 live births).<br />
4. Arboviruses are the most common causes of episo<strong>di</strong>c encephalitis with<br />
reported incidence similar to that of HSV.<br />
5. These statistics may be even more mislea<strong>di</strong>ng because most people<br />
bitten by arbovirus-infected insects do not develop clinical <strong>di</strong>sease, and<br />
only 10% develop overt encephalitis.
1. Clinical presentation and course can be markedly variable. Acuity and severity<br />
of presentation correlates with prognosis.<br />
2. The patient may have history of animal bite for which antirabies treatment<br />
may not have been obtained.<br />
3. The general viral prodrome is several days long and consists of fever,<br />
headache, nausea and vomiting, lethargy, and myalgias.<br />
4. The specific prodrome in VZV, EBV, CMV, measles, and mumps includes<br />
rash, lymphadenopathy, hepatosplenomegaly, and parotid enlargement.<br />
5. Dysuria and pyuria are reported with St Louis encephalitis.<br />
6. Extreme lethargy has been noted with WNE
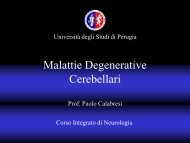
Pathophysiology<br />
1. Portals of entry are virus specific.<br />
2. Many viruses are transmitted by humans, although<br />
most cases of HSE are thought to be reactivation of<br />
the herpes simplex virus (HSV) lying dormant in the<br />
trigeminal ganglia.<br />
3. Mosquitoes or ticks inoculate arbovirus, and rabies<br />
virus is transferred via animal bite.<br />
4. With some viruses, such as varicella-zoster virus (VZV)<br />
and cytomegalovirus (CMV), an immunocompromised<br />
host is a key risk factor.
1. In general, the virus replicates outside the CNS and gains entry either<br />
by hematogenous spread or by traveling along neural (rabies, HSV,<br />
VZV) and olfactory (HSV) pathways.<br />
2. The etiology of slow virus infections, such as those implicated in the<br />
measles-related subacute sclerosing panencephalitis (SSPE) and<br />
progressive multifocal leukoencephalopathy (PML), is poorly<br />
understood.<br />
3. Once across the blood-brain barrier, the virus enters neural cells, with<br />
resultant <strong>di</strong>sruption in cell functioning, perivascular congestion,<br />
hemorrhage, and inflammatory response <strong>di</strong>ffusely affecting gray<br />
matter <strong>di</strong>sproportionately to white matter.<br />
4. Focal pathology is the result of neuron cell membrane receptors found<br />
only in specific portions of the brain and accounts for regional tropism<br />
found with some viruses. For example, HSV has a pre<strong>di</strong>lection for the<br />
inferior and me<strong>di</strong>al temporal lobes.
1. Although most histologic features are nonspecific,<br />
brain biopsies are the <strong>di</strong>agnostic criterion standard for<br />
rabies.<br />
2. Presence of Negri bo<strong>di</strong>es in the hippocampus and<br />
cerebellum are pathognomonic of rabies, as are HSV<br />
Cowdry type A inclusions with hemorrhagic necrosis in<br />
the temporal and orbitofrontal lobes.<br />
3. In contrast to viruses that invade gray matter <strong>di</strong>rectly,<br />
acute <strong>di</strong>sseminated encephalitis and postinfectious<br />
encephalomyelitis (PIE), secondary to measles (most<br />
common), Epstein-Barr virus (EBV), and CMV, are<br />
immune-me<strong>di</strong>ated processes, which result in multifocal<br />
demyelination of perivenous white matter.
The classic presentation is encephalopathy with <strong>di</strong>ffuse or focal<br />
neurologic symptoms, inclu<strong>di</strong>ng the following:<br />
1. Behavioral and personality changes, decreased level of<br />
consciousness<br />
2. Stiff neck, photophobia, and lethargy<br />
3. Generalized or localized seizures (60% of children with California<br />
encephalitis [CE])<br />
4. Acute confusion or amnestic states<br />
5. Flaccid paralysis (10% with WNE)<br />
6. Less common symptoms include headache and other complaints of<br />
meningismus.
Neonatal HSV infection symptoms (1-45 d) may occur in any combination.<br />
1. Skin, eye, and mouth lesions (early presentation)<br />
2. Encephalitis - Change in level of alertness, irritability, seizures, poor<br />
fee<strong>di</strong>ng<br />
3. Evidence of widespread, <strong>di</strong>sseminated <strong>di</strong>sease, such as rash or shock<br />
HSE in older children and adults<br />
1. Unrelated to history of oral lesions in infants<br />
2. Acute onset of severe symptoms of encephalitis<br />
Toxoplasma encephalopathy accounts for as many as 40% of patients who are<br />
HIV positive with neurologic <strong>di</strong>sease who present with a subacute headache,<br />
encephalopathy, and, often, a focal neurological complaint. This may be the<br />
presenting symptom of immunosuppression/HIV infection.
The signs of encephalitis may be <strong>di</strong>ffuse or focal (80% of patients with HSE<br />
present with focal fin<strong>di</strong>ngs) as follows:<br />
•Altered mental status and/or personality changes (most common)<br />
•Focal fin<strong>di</strong>ngs, such as hemiparesis, focal seizures, and autonomic dysfunction<br />
•Movement <strong>di</strong>sorders (St Louis encephalitis, EEE, WEE)<br />
•Ataxia<br />
•Cranial nerve defects<br />
•Dysphagia (Rabies may account for foaming at the mouth and hydrophobia.)<br />
•Meningismus (less common and less pronounced than in meningitis)<br />
•Unilateral sensorimotor dysfunction (PIE)<br />
HSV infection in the neonate (aged 1-45 d)<br />
Herpetic skin lesions over the presenting surface from birth or with breaks in the<br />
skin, such as those resulting from fetal scalp monitors<br />
Keratoconjunctivitis<br />
Oropharyngeal involvement, particularly buccal mucosa and tongue<br />
Encephalitis symptoms, such as seizures, irritability, change in level of<br />
attentiveness, bulging fontanels<br />
Ad<strong>di</strong>tional signs of <strong>di</strong>sseminated HSV, such as shock, jaun<strong>di</strong>ce, and<br />
hepatomegaly<br />
Toxoplasma encephalopathy: In immunosuppressed patients, 75% present with a focal<br />
neuropathology, about one half with encephalopathic changes.
Lab <strong>Stu<strong>di</strong></strong>es<br />
Complete blood count (CBC) with <strong>di</strong>fferential: Fin<strong>di</strong>ngs are usually within the<br />
reference range.<br />
Serum electrolytes: These are usually within the reference range. Syndrome of<br />
inappropriate secretion of anti<strong>di</strong>uretic hormone (SIADH) occurs in 25% of patients<br />
with St Louis encephalitis.)<br />
Serum glucose level: Use this level as a baseline for determining normal CSF<br />
glucose values. The result may be low if glycogen stores are depleted or high in<br />
infected patients with <strong>di</strong>abetes mellitus.<br />
BUN/creatinine and liver function tests (LFTs): Assess organ function and the need<br />
to adjust the antibiotic dose.<br />
Platelet test and a coagulation profile: These are in<strong>di</strong>cated in patients with<br />
chronic alcohol use, liver <strong>di</strong>sease, or if <strong>di</strong>sseminated intravascular coagulation<br />
(DIC) is suspected. The patient may require platelets or fresh-frozen plasma (FFP)<br />
before lumbar puncture (LP).<br />
Urinary electrolyte test: Perform this assessment if SIADH is suspected.<br />
Urine and/or serum toxicology screening: Perform 1 or both of these tests, if<br />
in<strong>di</strong>cated.
Other laboratory tests:<br />
CSF polymerase chain reaction (PCR): A PCR for DNA HSV is 100% specific<br />
and 75-98% sensitive within the first 25-45 hours. Types 1 and 2 cross-react,<br />
but no cross-reactivity with other herpes viruses occurs. Arguably, a series of<br />
quantitative PCRs documenting the decline of viral load with acyclovir<br />
treatment may clinch <strong>di</strong>agnosis without brain biopsy.<br />
HSV cultures: These are used to test lesions (also Tzanck smear), CSF (rarely<br />
positive), and blood.<br />
Viral serology: Complement fixation antibo<strong>di</strong>es are useful in identifying<br />
arbovirus. Cross-reactivity exists among one subgroup of arboviruses, the<br />
flaviviruses (eg, St Louis encephalitis, JE, WNE), and with antibo<strong>di</strong>es raised in<br />
persons inoculated with the yellow fever vaccine.<br />
Viral serology: Complement fixation antibo<strong>di</strong>es are useful in identifying<br />
arbovirus.<br />
Heterophile antibody and cold agglutinins for EBV: These tests may be helpful.<br />
Serologic tests for toxoplasmosis: These can be helpful in light of an abnormal<br />
CT scan, particularly in the case of single lesions. However, the overlap in titer<br />
between previously exposed but presently uninfected and reactivated groups<br />
may complicate interpretation.
Imaging <strong>Stu<strong>di</strong></strong>es<br />
Perform head CT, with and without contrast agent, in virtually all patients with<br />
encephalitis before LP to search for evidence of elevated intracerebral pressure<br />
(ICP), obstructive hydrocephalus, or mass effect. It is helpful also in <strong>di</strong>fferential<br />
<strong>di</strong>agnosis. MRI is more likely to show abnormalities earlier in <strong>di</strong>sease course<br />
than head CT.<br />
In HSE, an MRI may show several foci of increased T2 signal intensity in me<strong>di</strong>al<br />
temporal lobes and inferior frontal gray matter. Head CT may show petechial<br />
hemorrhage in the same areas.<br />
EEE and tick-borne encephalitis may show similar increased signal intensity in<br />
the basal ganglia and thalami.<br />
In toxoplasmosis, contrast-enhanced head CT typically reveals several nodular<br />
or ring-enhancing lesions. Because lesions may be missed without contrast, MRI<br />
should be performed in patients for whom use of contrast material is<br />
contrain<strong>di</strong>cated.
Electroencephalography<br />
Other Tests<br />
In HSE, characteristic paroxysmal lateral epileptiform <strong>di</strong>scharges (PLEDs)<br />
often are observed, even before neurora<strong>di</strong>ographic changes.<br />
Eventually, PLEDs are positive in 80% of cases. The presence of PLEDs is<br />
not pathognomonic for HSE.<br />
CSF analysis is essential.<br />
General patterns in bacterial and fungal (cryptococcal) meningitis found<br />
during the measurement of CSF pressure and CSF analysis may support a<br />
<strong>di</strong>agnosis (see the Table below).<br />
The most important <strong>di</strong>agnostic test in the ED to rule out bacterial meningitis<br />
is well-performed Gram staining and, if available, polymerase chain<br />
reaction of the CSF in patients with suspected HSV encephalitis.
Prehospital Care<br />
1. Evaluate and treat for shock or hypotension. Administer a crystalloid<br />
infusion until the patient is euvolemic.<br />
2. Consider airway protection in patients with an altered mental status.<br />
3. Consider seizure precautions. Treat seizures accor<strong>di</strong>ng to usual<br />
protocol (ie, lorazepam 0.1 mg/kg given intravenously [IV]).<br />
4. Stabilize alert patients with normal vital signs by administering oxygen,<br />
securing IV access, and provi<strong>di</strong>ng rapid transport to the ED.
Emergency Department Care<br />
With the important exceptions of HSE and varicella-zoster encephalitis, the viral<br />
encephalitides are not treatable beyond supportive care.<br />
The goal of treatment for acutely ill patients is administration of the first dose or<br />
doses acyclovir with or without antibiotics or steroids as quickly as possible.<br />
The standard for acute bacterial meningitis is the initiation of treatment<br />
within 30 minutes of arrival.<br />
Consider instituting an ED triage protocol to identify patients at risk for HSE.<br />
Collect laboratory samples and blood cultures before the start of IV therapy.<br />
Even in uncomplicated cases of encephalitis, most authorities recommend a<br />
neuroimaging study (eg, contrast-enhanced head CT scan) before LP.<br />
Signs of hydrocephalus and increased ICP
Emergency Department Care<br />
General measures: Manage fever and pain, control straining and coughing,<br />
and avoid seizures and systemic hypotension.<br />
In otherwise stable patients, elevating the head and monitoring neurologic<br />
status usually are sufficient.<br />
When more aggressive maneuvers are in<strong>di</strong>cated, some authorities favor the<br />
early use of <strong>di</strong>uresis (eg, furosemide 20 mg IV, mannitol 1 g/kg IV) provided<br />
circulatory volume is protected. Dexamethasone 10 mg IV q6h helps in<br />
managing edema surroun<strong>di</strong>ng space-occupying lesions. Hyperventilation<br />
(PaCO2 30 mm Hg) may cause a <strong>di</strong>sproportional decrease in cerebral blood<br />
flow (CBF), but it is used to control increasing ICP on an emergency basis.<br />
Look for and treat systemic complications, particularly in HSE, EEE, JE, such as<br />
hypotension or shock, hypoxemia, hyponatremia (SIADH), and exacerbation of<br />
chronic <strong>di</strong>seases.
Other Problems to be Considered<br />
•Acute CNS events, such as hemorrhagic stroke<br />
•Acute confusional states secondary to drugs, toxins, psychosis<br />
•Amoeba (Naegleria, Acanthamoeba)<br />
•Head trauma<br />
•CNS syphilis<br />
•Ehrlichiosis<br />
•Intracranial hemorrhage<br />
•Intracranial tumor<br />
•Trauma
Background:<br />
Herpes encephalitis is the most common cause of spora<strong>di</strong>c viral encephalitis,<br />
with a pre<strong>di</strong>lection for the temporal lobes and a range of clinical presentations,<br />
from aseptic meningitis and fever to a severe rapidly progressive form<br />
involving altered consciousness.<br />
In adults, herpes simplex virus type 1 (HSV-1) accounts for 95% of all fatal<br />
cases of spora<strong>di</strong>c encephalitis and usually results from reactivation of the<br />
latent virus.<br />
The clinical fin<strong>di</strong>ngs and neuroimaging appearance are both consistent with<br />
spread of the virus from a previously infected ganglion.<br />
In children and neonates, herpes simplex virus type 2 (HSV-2) accounts for<br />
80-90% of neonatal and almost all congenital infections.<br />
An isolated case report of an immunocompromised adult patient developing<br />
HSV-2 infection has been described.<br />
MRI can play an important role in determining the <strong>di</strong>agnosis and extent of<br />
<strong>di</strong>sease.
On pathology, herpes viruses cause a fulminant<br />
hemorrhagic and necrotizing meningoencephalitis.<br />
Typical gross fin<strong>di</strong>ngs include severe edema and massive<br />
tissue necrosis, with petechial hemorrhages and<br />
hemorrhagic necrosis.<br />
Often, the petechial hemorrhage is not observed on CT or<br />
MRI.<br />
On microscopy, a focal necrotizing vasculitis is observed<br />
with perivascular and meningeal lymphocytic infiltration and<br />
eosinophilic intranuclear inclusions in glial cells and<br />
neurons.
Mortality/Morbi<strong>di</strong>ty:<br />
Untreated patients with HSV-1 have a 70% mortality rate.<br />
With early treatment, 40% of patients recover without significant neurologic<br />
deficits; however, despite appropriate <strong>di</strong>agnosis and therapy, the mortality rate<br />
remains at 30%.<br />
Interestingly, HSV does not appear to be more common in<br />
immunocompromised patients than in normal hosts. HSV-1 is rarely associated<br />
with pregnancy.<br />
HSV mortality in neonates with isolated CNS <strong>di</strong>sease is 15%, and in those with<br />
<strong>di</strong>sseminated CNS <strong>di</strong>sease, the rate is 57%.<br />
Morbi<strong>di</strong>ty for these groups is also high.
Clinical Details:<br />
In adults, the most common early symptoms are headache and fever. Ad<strong>di</strong>tional<br />
symptoms include intellectual impairment, aphasia, meningeal signs, seizures, and<br />
paresthesias. Early treatment is crucial to a good outcome, and empiric acyclovir<br />
therapy can be initiated before a definitive <strong>di</strong>agnosis is established. The virus<br />
cannot be cultured routinely from CSF, though lymphocytic pleocytosis and<br />
elevations in protein concentrations are observed. CSF viral cultures are positive<br />
for HSV in fewer than 5% of patients. Anti-HSV antibo<strong>di</strong>es often do not appear until<br />
1-3 weeks after symptom onset; therefore, antibody culture is helpful only in<br />
retrospective <strong>di</strong>agnosis. In some patients, a brain biopsy may be required for a<br />
definitive <strong>di</strong>agnosis.<br />
EEG also can reveal focal temporal abnormalities, which are seen in 80% of<br />
patients; a normal EEG is believed to exclude the <strong>di</strong>agnosis. Perio<strong>di</strong>c lateralized<br />
epileptiform <strong>di</strong>scharges also support the <strong>di</strong>agnosis, but this fin<strong>di</strong>ng is nonspecific.<br />
Historically, a brain biopsy provided a definitive <strong>di</strong>agnosis, but this procedure is not<br />
highly sensitive and can result in complications, inclu<strong>di</strong>ng hemorrhage and edema<br />
at the biopsy site. An RNA polymerase test of CSF permits a more definitive<br />
<strong>di</strong>agnosis because it is both sensitive and specific. In this test, 2 sets of<br />
oligonucleotide primers amplify gene products from HSV-1 and HSV-2.
Picture 1. Axial proton density–<br />
weighted image in a 62-year-old<br />
woman with confusion and herpes<br />
encephalitis shows T2<br />
hyperintensity involving the right<br />
temporal lobe.
Picture 2. Axial nonenhanced T1-<br />
weighted image shows cortical<br />
hyperintensity (arrows) consistent<br />
with petechial hemorrhage. In<br />
general, this is a common pathologic<br />
fin<strong>di</strong>ng but less commonly depicted<br />
in herpes encephalitis.
Picture 3. Axial<br />
gadolinium-enhanced T1-<br />
weighted image reveals<br />
enhancement of the right<br />
anterior temporal lobe<br />
and parahippocampal<br />
gyrus. At the right anterior<br />
temporal tip is a<br />
hypointense, crescentic<br />
region surrounded by<br />
enhancement consistent<br />
with a small epidural<br />
abscess.
Picture 4. Axial <strong>di</strong>ffusionweighted<br />
image reveals<br />
restricted <strong>di</strong>ffusion in the<br />
left me<strong>di</strong>al temporal lobe<br />
consistent with herpes<br />
encephalitis. This patient<br />
also had a positive result on<br />
polymerase chain reaction<br />
assay for herpes simplex<br />
virus, which is both<br />
sensitive and specific. In<br />
ad<strong>di</strong>tion, the patient had<br />
perio<strong>di</strong>c lateralized<br />
epileptiform <strong>di</strong>scharges on<br />
EEG, which supports the<br />
<strong>di</strong>agnosis of herpes<br />
encephalitis.
Picture 5. Coronal T2-<br />
weighted image reveals<br />
hyperintensity in the left<br />
temporal lobe (arrows) in<br />
a <strong>di</strong>stribution similar to<br />
the restricted <strong>di</strong>ffusion<br />
abnormality seen in<br />
Image 4. This fin<strong>di</strong>ng is<br />
typical for herpes<br />
encephalitis.
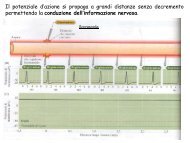
La <strong>di</strong>agnosi viene fatta sulla base dei sintomi<br />
clinici e per le caratteristiche<br />
dell'elettroencefalogramma che presenta<br />
particolari alterazioni (pseudoperio<strong>di</strong>smi) in<br />
un numero rilevante <strong>di</strong> casi. L'aumentata<br />
concentrazione della proteina 14-3-3 e della<br />
proteina TAU nel fluido cerebrospinale. La<br />
conferma <strong>di</strong>agnostica può essere fatta solo<br />
me<strong>di</strong>ante la <strong>di</strong>mostrazione delle<br />
caratteristiche lesioni spongiformi<br />
accompagnate dalla presenza <strong>di</strong> proteina<br />
prionica (PrPres o PrPsc) in un prelievo <strong>di</strong><br />
tessuto nervoso.<br />
La malattia <strong>di</strong> Creutzfeldt-Jacob, originariamente descritta negli anni '20 del XX<br />
secolo da Hans Gerhard Creutzfeldt ed Alfons Maria Jakob, è una malattia<br />
neurodegenerativa rara, che conduce ad una forma <strong>di</strong> demenza progressiva fatale. La<br />
sindrome clinica è caratterizzata da per<strong>di</strong>ta <strong>di</strong> memoria, cambiamenti <strong>di</strong> personalità,<br />
allucinazioni, <strong>di</strong>sartria, mioclonie, rigi<strong>di</strong>tà posturale e convulsioni. I sintomi ed i segni<br />
sono dovuti alla progressiva per<strong>di</strong>ta <strong>di</strong> neuroni causata da alterazione <strong>di</strong> una proteina<br />
<strong>di</strong> membrana, espressa prevalentemente in cellule del sistema nervoso e del sistema<br />
reticolo-endoteliale, il prione. La sua incidenza si è mantenuta relativamente costante<br />
negli ultimi 80 anni, nell'or<strong>di</strong>ne <strong>di</strong> 1-2/1000000. Ottiene gli onori della cronaca dopo la<br />
descrizione dei primi casi <strong>di</strong> una forma variante, ancor più rara, legata all'epidemia <strong>di</strong><br />
Encefalopatia spongiforme bovina, la cosiddetta malattia della "mucca pazza".
Head CT (left) and MRI (right) both given with contrast of the same patient<br />
with new seizures, focal weakness, and HIV infection. Multiple ring-enhancing<br />
lesions are seen in the periventricular white matter. The lesions are consistent<br />
with Toxoplasma encephalitis. The images point out the enhanced sensitivity<br />
of MRI scanning over CT scanning in this instance.
MR Imaging of<br />
Autopsy-<br />
Proved<br />
Paraneoplasti<br />
c Limbic<br />
Encephalitis in<br />
Non-Hodgkin<br />
Lymphoma<br />
Initial MR images obtained 1 day after the first generalized seizure occurred.<br />
A, Axial fluid-attenuated inversion recovery image (9000/110 [TR/TE]; inversion<br />
time, 2261 ms) shows a slightly elevated signal intensity of both hippocampal<br />
formations (black arrows) and amygdala (white arrows).<br />
B, Coronal conventional T2-weighted turbo spin-echo image
Typical cranial magnetic resonance imaging (MRI) fin<strong>di</strong>ngs in patients with<br />
paraneoplastic limbic encephalitis. Coronal fluid-attenuated inversion<br />
recovery (FLAIR) MRI showing bilateral (left) and unilateral (middle) mesial<br />
temporal signal abnormalities. Axial FLAIR MRI showing extralimbic signal<br />
abnormalities involving the left operculum and insular cortex (right).
Brain magnetic resonance imaging (MRI) stu<strong>di</strong>es. A and B, Axial MRI fluidattenuated<br />
inversion recovery images at presentation show increased signal in the cerebellar<br />
vermis and periventricular white matter. C and D, Follow-up images (same sequences<br />
and levels) 16 days later show progression of signal abnormality in the cerebellar<br />
vermis and periventricular white matter with extension across the corpus callosum.
La Panencefalite sclerosante subacuta è una rara malattia degenerativa<br />
del sistema nervoso centrale, causata dalla persistenza <strong>di</strong> un virus del<br />
morbillo <strong>di</strong>fettivo.<br />
Si verifica in me<strong>di</strong>a a <strong>di</strong>stanza <strong>di</strong> 9 anni dal morbillo.<br />
La malattia cerebrale è evolutiva, subdola ed inesorabile ed è caratterizzata<br />
da gravi lesioni cerebrali, con una progressiva per<strong>di</strong>ta <strong>di</strong> tutte le funzioni<br />
cognitive, con spasmi mioclonici e convulsioni.<br />
È un’encefalite a lenta evoluzione, la cui frequenza è <strong>di</strong> circa 1 caso ogni<br />
100.000 casi <strong>di</strong> morbillo, più frequente nei soggetti che lo avevano contratto<br />
nei primi due anni <strong>di</strong> vita.<br />
Sono stati segnalati anche 20 casi <strong>di</strong> panancefalite progressiva dopo rosolia.<br />
I dati epidemiologici <strong>di</strong>sponibili non documentano però un rischio legato al<br />
vaccino.<br />
Il vaccino contro il morbillo riduce in maniera significativa la possibilità <strong>di</strong><br />
sviluppare la PESS, così come <strong>di</strong>mostrato dalla sostanziale eliminazione dei<br />
casi <strong>di</strong> PESS dopo l’introduzione del vaccino contro il morbillo, sebbene la<br />
malattia è stata raramente riscontrata in bambini senza una storia d’infezione<br />
morbillosa, ma che avevano ricevuto il vaccino contro il morbillo.<br />
È da segnalare che i bambini <strong>di</strong> età inferiore ad 1 anno, o malnutriti,<br />
immunocompromessi o affetti da patologie croniche, sono particolarmente<br />
suscettibili all'infezione.
PESS: QUADRO CLINICO<br />
• Deterioramento intellettivo. I primi segni sono spesso un ridotto ren<strong>di</strong>mento<br />
scolastico, per<strong>di</strong>ta della memoria, cambiamenti repentini dell'umore, <strong>di</strong>strazione,<br />
insonnia ed allucinazioni. Possono anche verificarsi crisi convulsive. I pazienti<br />
mostrano quin<strong>di</strong> un ulteriore declino intellettuale, manifestando alterazioni della<br />
parola.<br />
• Convulsioni. Le convulsioni fanno seguito alle alterazioni mentali ed<br />
inizialmente sono costituite da spasmi mioclonici.<br />
• Anomalie motorie e movimenti involontari anomali. Possono comparire<br />
movimenti <strong>di</strong>stonici e perio<strong>di</strong> transitori <strong>di</strong> opistotono. Più tar<strong>di</strong>vamente, si verifica<br />
una rigi<strong>di</strong>tà della muscolatura corporea, <strong>di</strong>fficoltà alla deglutizione, cecità<br />
corticale e atrofia ottica. In molti pazienti si verificano corioretinite focale e<br />
altre anomalie del fundus. Nelle fasi finali, il paziente <strong>di</strong>viene progressivamente<br />
rigido, con segni intermittenti d'interessamento ipotalamico (per esempio,<br />
ipertermia, sudorazione, <strong>di</strong>sturbi della PA e del ritmo car<strong>di</strong>aco).
PESS: MRI scans of the brain at<br />
the time of presentation in the<br />
neurology clinic (A and B) and 3<br />
months later (C and D). Panels A<br />
and C are T1-weighted images; B<br />
and D are T2-weighted images.<br />
The initial MRI scan (A and B)<br />
reveals a focal abnormality in the<br />
subcortical white matter of the left<br />
frontal lobe, consisting of a<br />
hypointense signal on the T1-<br />
weighted image (arrow in A) and a<br />
hyperintense signal on the T2-<br />
weighted image (arrow in B). In the<br />
followup scan, the focal<br />
abnormality in the left frontal lobe<br />
is less obvious than previously<br />
(arrow in D), but advanced and<br />
<strong>di</strong>ffuse cortical atrophy is present,<br />
signified by the ventriculomegaly<br />
and markedly enlarged sulci<br />
(arrowheads in C).
Acute <strong>di</strong>sseminated encephalomyelitis (ADEM)<br />
ADEM is an inflammatory demyelinating <strong>di</strong>sease of the central nervous<br />
system (CNS) that is known to occur spontaneously in association with<br />
specific and nonspecific viral illnesses and after vaccination against<br />
various pathogens.<br />
Although it is often a self-limited monophasic illness, the fatality rate is<br />
estimated to be as high as 30%, and many patients suffer residual<br />
neurologic impairment.<br />
Clinical improvement has been reported after initiation of corticosteroid<br />
therapy, and relapse has occurred after <strong>di</strong>scontinuation of therapy.
ADEM A and B, Axial<br />
magnetic resonance<br />
images, demonstrating<br />
multifocal subcortical and<br />
periventricular areas of<br />
increased T2 signal, without<br />
mass effect or surroun<strong>di</strong>ng<br />
edema. C and D,<br />
Correspon<strong>di</strong>ng axial T1-<br />
weighted images after<br />
administration of gadolinium.
Progressive multifocal leukoencephalopathy (PML)<br />
PML was a fairly rare demyelinating <strong>di</strong>sease of the white matter of the brain until<br />
the AIDS epidemic started. As PML requires a weakened immune system to<br />
develop, it is no wonder that AIDS has significantly increased its frequency.<br />
PML is caused by the human<br />
papovavirus, an RNA virus<br />
called JC virus (=JCV). We<br />
know from serological stu<strong>di</strong>es<br />
on children where by age 10<br />
about 50% of them have<br />
antibody titers to JCV that this<br />
virus is widely <strong>di</strong>stributed.<br />
Normally JCV infection stays<br />
suppressed by the immune<br />
system's cell me<strong>di</strong>ated<br />
immune response. In the case<br />
of immune weakening<br />
<strong>di</strong>seases such as leukemias,<br />
lymphomas, AIDS and in<br />
transplant patients JCV can<br />
then be reactivated and cause<br />
PML. About 5% of AIDS<br />
patients are suffering from<br />
PML.