Cancer Referral form - Upper GI
Cancer Referral form - Upper GI
Cancer Referral form - Upper GI
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
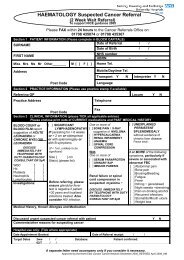
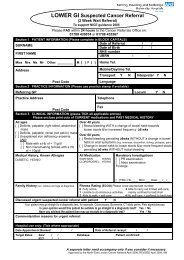
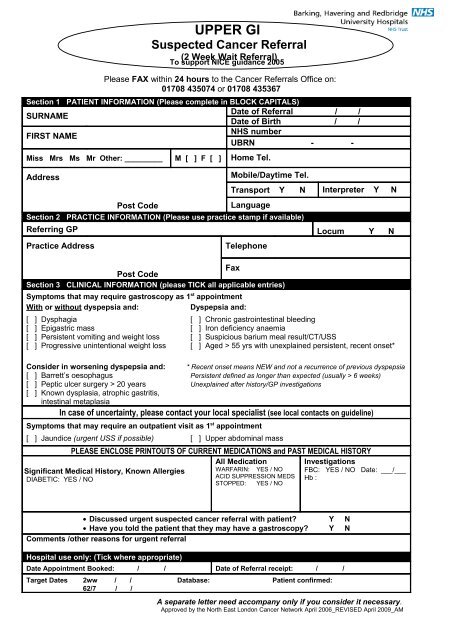
UPPER <strong>GI</strong><br />
Suspected <strong>Cancer</strong> <strong>Referral</strong><br />
(2 Week Wait <strong>Referral</strong>)<br />
To support NICE guidance 2005<br />
Please FAX within 24 hours to the <strong>Cancer</strong> <strong>Referral</strong>s Office on:<br />
01708 435074 or 01708 435367<br />
Section 1 PATIENT INFORMATION (Please complete in BLOCK CAPITALS)<br />
SURNAME<br />
Date of <strong>Referral</strong> / /<br />
Date of Birth / /<br />
FIRST NAME<br />
NHS number<br />
UBRN - -<br />
Miss Mrs Ms Mr Other: _________ M [ ] F [ ] Home Tel.<br />
Address<br />
Post Code<br />
Mobile/Daytime Tel.<br />
Transport Y N Interpreter Y N<br />
Language<br />
Section 2 PRACTICE INFORMATION (Please use practice stamp if available)<br />
Referring GP Locum Y N<br />
Practice Address<br />
Telephone<br />
Fax<br />
Post Code<br />
Section 3 CLINICAL INFORMATION (please TICK all applicable entries)<br />
Symptoms that may require gastroscopy as 1 st appointment<br />
With or without dyspepsia and:<br />
Dyspepsia and:<br />
[ ] Dysphagia [ ] Chronic gastrointestinal bleeding<br />
[ ] Epigastric mass [ ] Iron deficiency anaemia<br />
[ ] Persistent vomiting and weight loss [ ] Suspicious barium meal result/CT/USS<br />
[ ] Progressive unintentional weight loss [ ] Aged > 55 yrs with unexplained persistent, recent onset*<br />
Consider in worsening dyspepsia and: * Recent onset means NEW and not a recurrence of previous dyspepsia<br />
[ ] Barrett’s oesophagus Persistent defined as longer than expected (usually > 6 weeks)<br />
[ ] Peptic ulcer surgery > 20 years Unexplained after history/GP investigations<br />
[ ] Known dysplasia, atrophic gastritis,<br />
intestinal metaplasia<br />
In case of uncertainty, please contact your local specialist (see local contacts on guideline)<br />
Symptoms that may require an outpatient visit as 1 st appointment<br />
[ ] Jaundice (urgent USS if possible) [ ] <strong>Upper</strong> abdominal mass<br />
PLEASE ENCLOSE PRINTOUTS OF CURRENT MEDICATIONS and PAST MEDICAL HISTORY<br />
All Medication<br />
Significant Medical History, Known Allergies<br />
DIABETIC: YES / NO<br />
WARFARIN: YES / NO<br />
ACID SUPPRESSION MEDS<br />
STOPPED: YES / NO<br />
Investigations<br />
FBC: YES / NO Date: ___/___<br />
Hb :<br />
• Discussed urgent suspected cancer referral with patient Y N<br />
• Have you told the patient that they may have a gastroscopy Y N<br />
Comments /other reasons for urgent referral<br />
Hospital use only: (Tick where appropriate)<br />
Date Appointment Booked: / / Date of <strong>Referral</strong> receipt: / /<br />
Target Dates 2ww / / Database: Patient confirmed:<br />
62/7 / /<br />
A separate letter need accompany only if you consider it necessary.<br />
Approved by the North East London <strong>Cancer</strong> Network April 2006_REVISED April 2009_AM
LOCAL CONTACT DETAILS<br />
<strong>Cancer</strong> Waiting Times Co-ordinator Tel. 01708 435169 Queen’s Hospital<br />
CRITERIA 1 FOR URGENT SUSPECTED CANCER REFERRAL<br />
Please FAX the referral <strong>form</strong> within 24 hours<br />
Refer a patient who presents with symptoms suggestive of upper <strong>GI</strong> cancer to a team<br />
specialising in the management of upper <strong>GI</strong> cancer, depending on local arrangements.<br />
Helicobacter pylori status should not affect the decision to refer for suspected cancer.<br />
Note that for patients
![[4] Biopsy Leaflet.pub - Barking, Havering and Redbridge University ...](https://img.yumpu.com/51285530/1/190x134/4-biopsy-leafletpub-barking-havering-and-redbridge-university-.jpg?quality=85)