Annual report and accounts 2011/12 - Homerton University Hospital
Annual report and accounts 2011/12 - Homerton University Hospital
Annual report and accounts 2011/12 - Homerton University Hospital
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Annual</strong> <strong>report</strong> <strong>and</strong> <strong>accounts</strong><br />
<strong>2011</strong>/<strong>12</strong><br />
www.homerton.nhs.uk
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
<strong>Annual</strong> Report <strong>and</strong><br />
Accounts <strong>2011</strong>/<strong>12</strong><br />
Presented to Parliament pursuant to Schedule 7,<br />
paragraph 25(4) of the National Service Act 2006
4 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
<strong>Annual</strong> Report <strong>and</strong> Accounts <strong>2011</strong>/<strong>12</strong><br />
This <strong>Annual</strong> Report follows best practice in corporate <strong>report</strong>ing by articulating our<br />
strategy; <strong>report</strong>ing back on our performance against strategic objectives <strong>and</strong> national<br />
targets; <strong>and</strong> presenting information about our service <strong>and</strong> financial performance.<br />
The structure of the <strong>report</strong> is as follows:<br />
Contents<br />
Introduction 7<br />
consisting of a statement by the Chairman.<br />
Chief Executive’s <strong>report</strong> 9<br />
including our strategic vision, performance against corporate objectives<br />
<strong>2011</strong>/<strong>12</strong> <strong>and</strong> details of our corporate objectives 20<strong>12</strong>/13.<br />
Performance <strong>report</strong> 11<br />
including our financial performance <strong>and</strong> non financial performance<br />
against national targets.<br />
Governance <strong>report</strong> 22<br />
including details of the Board of Directors, Council of Governors <strong>and</strong><br />
Foundation Trust membership.<br />
Quality Account 33<br />
demonstrating our commitment to providing quality care for all patients<br />
<strong>and</strong> <strong>report</strong>ing back on our performance against priorities for quality<br />
improvement agreed by the Board of Directors <strong>and</strong> identifying our<br />
priorities for 20<strong>12</strong>/13.<br />
Finance 81<br />
including the full <strong>Annual</strong> Accounts for the financial year <strong>2011</strong>/<strong>12</strong>.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 5
Trust Infection Control Nurse Vickie Longstaff with one of<br />
the new Kwick screens used in wards to form a mobile<br />
infection control barrier<br />
The arrival of the new MRI scanner at the hospital during<br />
the summer of <strong>2011</strong><br />
A patient tries out the new gym sports training equipment<br />
in the Physiotherapy Department<br />
Radiologists Nan Mutsau <strong>and</strong> Beverley Bvute with the new<br />
mammography machine donated to the hospital as part<br />
of the GE Healthcare Olympic legacy<br />
WAWASHSH – artist Kevin Harrison’s work forms the<br />
centre piece of the newly refurbished back entrance to<br />
the hospital – part of a major facelift given to signs, wards<br />
<strong>and</strong> corridors during the year<br />
A mother <strong>and</strong> child are seen by Health Visitor Nana<br />
Larbi-Amoah at one of the Trust’s community locations<br />
6 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Chairman’s statement<br />
Despite the recent passing of the new Health <strong>and</strong> Social<br />
Care Bill, parts of the NHS continue to be buffeted by the<br />
ongoing transition of power within the system <strong>and</strong> the<br />
need for the NHS to meet the efficiency challenge at this<br />
time of unprecedented change has in no way diminished.<br />
North East London <strong>and</strong> the populations we serve are not<br />
immune from these factors. Indeed, we have experienced<br />
their impact at close quarters.<br />
We also face important changes to our own leadership in<br />
the year ahead in light of the planned retirement of our<br />
strong <strong>and</strong> dedicated Chief Executive.<br />
I am pleased to <strong>report</strong> that the belt-tightening exercise<br />
I referred to last year has proved successful. Despite the<br />
significant challenges on our doorstep, we have maintained<br />
<strong>and</strong> improved the safety <strong>and</strong> quality of the services<br />
we offer, with positive <strong>report</strong>s from the various quality<br />
inspections, while delivering strong financial performance.<br />
Over time this will be reflected in patient surveys when we<br />
can get the response rate up to better levels.<br />
Closer to home, we have forged ahead in developing<br />
stronger relationships with our local <strong>and</strong> neighbouring<br />
GPs. We welcome the introduction of the Commissioning<br />
Groups <strong>and</strong> are greatly encouraged by our shared aims of<br />
securing the best health care available for the residents of<br />
Hackney, the City, <strong>and</strong> beyond.<br />
Our first year providing both acute <strong>and</strong> community care has<br />
filled us with immense pride. We have made great progress<br />
in bringing the services together <strong>and</strong> improving the<br />
environment <strong>and</strong> infrastructure supporting their delivery.<br />
We, in conjunction with our commissioning partners,<br />
are committed to building on this success to continue to<br />
transform these services to the significant benefit of our<br />
patients.<br />
We have good st<strong>and</strong>ing with our local GPs, we have<br />
short waiting times, <strong>and</strong> we can offer patients brilliant<br />
consultants <strong>and</strong> nurses. The hospital has never been<br />
looking better <strong>and</strong> we are committed to ensuring the<br />
community service environments achieve a similar st<strong>and</strong>ard.<br />
We are well prepared for the Olympics <strong>and</strong> will play our<br />
part if called upon to do so.<br />
So I am very confident of the important role <strong>Homerton</strong> will<br />
play as the new world continues to take shape. The Board<br />
is committed to growing our hospital <strong>and</strong> community<br />
services to compete with the best in our sector <strong>and</strong><br />
compare favourably with the best in class.<br />
I thank all of my colleagues <strong>and</strong> all our staff for their<br />
continued support through a period of major change.<br />
Michael Cassidy CBE<br />
Chairman<br />
30 May 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 7
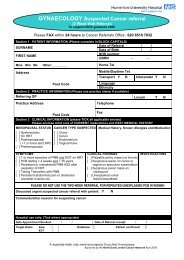
How our health services pan out across Hackney <strong>and</strong> The City –<br />
health services are run in over 30 health centres, GP surgeries <strong>and</strong><br />
people’s homes as well as <strong>Homerton</strong> <strong>Hospital</strong><br />
7<br />
A105<br />
6<br />
Islington<br />
A503<br />
9<br />
8<br />
26<br />
1<br />
STOKE<br />
NEWINGTON<br />
10<br />
32<br />
27<br />
28<br />
29<br />
A10<br />
A10<br />
2<br />
3 4<br />
13<br />
11<br />
14<br />
30<br />
19<br />
5<br />
<strong>12</strong><br />
Hackney<br />
Downs<br />
UPPER<br />
CLAPTON<br />
Hackney<br />
15<br />
20<br />
23 21<br />
HACKNEY<br />
33<br />
25<br />
24<br />
A<strong>12</strong>07<br />
DALSTON<br />
HAGGERSTON<br />
A107<br />
A104<br />
LOWER<br />
CLAPTON<br />
16<br />
Waltham Forest<br />
LEA BRIDGE<br />
17<br />
18<br />
34<br />
22<br />
H o m e r t o n H<br />
i g h S t r e e t<br />
HOMERTON<br />
A<strong>12</strong><br />
Tower Hamlets<br />
London<br />
20<strong>12</strong><br />
Olympics<br />
Newham<br />
R I V<br />
31<br />
City<br />
E R T H A M<br />
E S<br />
Sites <strong>and</strong> locations<br />
1. Cranwich Road Health Centre<br />
2. Stamford Hill Group Practice<br />
3. Stamford Hill Community Centre<br />
4. Tyssen Children’s Centre<br />
5. Fountayne Road Health Centre<br />
6. Woodberry Downs Children’s Centre<br />
<strong>and</strong> Lillyput Nursery<br />
7. John Scott Health Centre<br />
8. Norwood Bearstead Health <strong>and</strong><br />
Wellbeing Centre<br />
9. Statham Grove Surgery<br />
10. Barton House Health Centre<br />
11. Linden Children’s Centre<br />
<strong>12</strong>. Nightingale Practice<br />
13. Somerford Grove Health Centre<br />
14. Hackney Ark<br />
15. Lower Clapton Health Centre<br />
<strong>and</strong> CHYPS Plus<br />
16. <strong>Homerton</strong> <strong>Hospital</strong><br />
17. Sorsby Health Centre<br />
18. Daubeney Children’s Centre<br />
19. Dalston Practice; S<strong>and</strong>ringham<br />
Practice (Madinah Road)<br />
20. Learning Trust<br />
21. Elsdale Street Surgery<br />
22. Wick Health Centre<br />
23. Sickle Cell <strong>and</strong> Thalassaemia Centre<br />
24. Ann Taylor Children’s Centre<br />
25. Well Street Surgery (Shore Road)<br />
26. Shoreditch Park Surgery;<br />
Hoxton Surgery (Rushton Street)<br />
27. St Leonard’s <strong>Hospital</strong><br />
28. Lawson Practice<br />
29. Defoe Block, Hackney College<br />
Hackney Community College,<br />
B Block<br />
30. Sebright Children’s Centre<br />
31. Neaman Surgery<br />
32. Mary Seacole Nursing Home<br />
33. Greenhouse Walk-in, Tudor Road<br />
(Managed by the London Borough<br />
of Hackney)<br />
34. South East Resource Centre<br />
8 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Chief Executive’s Report<br />
In this section we profile the principal activities of the Trust<br />
throughout the course of the past year <strong>and</strong> highlight the<br />
progress we have made in developing the range <strong>and</strong> scope<br />
of services we provide. We also consider the year ahead.<br />
Our business review is covered in detail in the Performance<br />
Report followed by our Governance Report <strong>and</strong> Quality<br />
Account. The final section of the <strong>report</strong> is the <strong>Annual</strong><br />
Accounts.<br />
This is <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust’s<br />
(<strong>Homerton</strong>) first <strong>Annual</strong> Report as an integrated acute <strong>and</strong><br />
community foundation trust.<br />
Our principal activities<br />
<strong>Homerton</strong> provides hospital <strong>and</strong> community services for<br />
Hackney, the City <strong>and</strong> the surrounding communities, <strong>and</strong> a<br />
bespoke range of specialist services for a wider population.<br />
The Trust comprises <strong>Homerton</strong> <strong>Hospital</strong>; Mary Seacole<br />
Continuing Care Nursing Home; <strong>and</strong> community <strong>and</strong> home<br />
care services across Hackney <strong>and</strong> the City.<br />
We have unconditional registration from the Care Quality<br />
Commission.<br />
The main hospital, which opened in 1986 is based on one<br />
site. <strong>Homerton</strong> became an NHS Foundation Trust in 2004,<br />
under the Health <strong>and</strong> Social Care (Community Health <strong>and</strong><br />
St<strong>and</strong>ards) Act 2003.<br />
Progress in <strong>2011</strong>/<strong>12</strong> in developing the range <strong>and</strong><br />
scope of services<br />
Community based services<br />
This is our first year as an integrated acute <strong>and</strong> community<br />
trust, <strong>and</strong> it has been a real privilege to work alongside the<br />
community teams, many of whom work with individuals<br />
<strong>and</strong> families experiencing enormous challenges. It is<br />
humbling to witness their work. Our focus this year has<br />
been on home support for mothers <strong>and</strong> new babies <strong>and</strong><br />
community services for the frail elderly but there is so much<br />
more we aspire to do.<br />
We have worked hard on the modernisation of community<br />
Information Technology (IT) systems, facilities <strong>and</strong> buildings.<br />
On IT the progress is good. Buildings <strong>and</strong> facilities continue<br />
to need our attention.<br />
Services in the hospital<br />
More women have delivered their babies with us this year<br />
than ever <strong>and</strong> more people have chosen to be referred<br />
here for treatment. We have been asked to provide more<br />
specialist services, particularly in the areas of stroke <strong>and</strong><br />
neuro-rehabilitation, retinal screening, obesity surgery <strong>and</strong><br />
intensive care for the newborn.<br />
Buildings <strong>and</strong> equipment<br />
Our new Elderly Care Unit has opened offering support<br />
<strong>and</strong> rehabilitation for the elderly <strong>and</strong> those with dementia.<br />
Our Main Entrance, corridors <strong>and</strong> signage have all been<br />
upgraded <strong>and</strong> complemented with new art work. Work<br />
will soon complete on a new <strong>and</strong> enlarged Endoscopy<br />
Unit. Investment in IT has been significant, with a state of<br />
the art maternity management system installed <strong>and</strong> a new<br />
contract agreed for our core patient systems agreed.<br />
I must take this opportunity to once again thank the<br />
Olympic sponsor General Electric (GE) for supporting us<br />
with their Olympic legacy donation which has allowed<br />
us to equip our specialist neonatal services with the most<br />
sophisticated equipment available.<br />
London 20<strong>12</strong> Olympic <strong>and</strong> Paralympic Games<br />
We are fully prepared for <strong>and</strong> proud to support the Games<br />
in our role as an Olympic hospital. The Olympic Torch passes<br />
in front of hospital on 21 July <strong>and</strong> the roar of the crowd at<br />
the Opening Ceremony on 27 July will be easily heard from<br />
here. It will of course be business as usual for all of our<br />
services during the Games.<br />
Service performance <strong>and</strong> quality<br />
There are not many organisations that can say that the<br />
year has passed without a single patient acquiring an<br />
MRSA blood infection but <strong>Homerton</strong> can. In a challenging<br />
climate, we met or surpassed our financial, activity <strong>and</strong><br />
key performance targets, <strong>and</strong> demonstrate in our Quality<br />
Account that this was without compromise to service<br />
quality.<br />
There are of course areas where we could <strong>and</strong> should have<br />
done better. Not every patient – whether in our hospital<br />
or looked after by us at home – received the thoughtful,<br />
effective care they deserve. We exist to provide health care<br />
<strong>and</strong> must never let up in our endeavours to make this of<br />
the highest st<strong>and</strong>ard.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 9
Key objectives<br />
Our direction of travel is not changing but we are going<br />
at a faster pace. Our focus remains on getting the<br />
fundamentals right - ensuring that the people we serve<br />
get safe, effective, thoughtful health care, within the rules<br />
that apply to NHS. But we have aspirations beyond this. In<br />
previous times we have set these out in broad terms, this<br />
year we are being much more specific about our plans for<br />
the next three years. These are set out on page <strong>12</strong>.<br />
Principal risks<br />
<strong>Homerton</strong> is in good shape <strong>and</strong> we face the year ahead<br />
with enthusiasm. We are a high performing organisation<br />
with a clear sense of purpose. There are of course risks <strong>and</strong><br />
uncertainties ahead. We have new health care legislation,<br />
in London hospital mergers <strong>and</strong> service changes are taking<br />
place, <strong>and</strong> the economic situation remains challenging. In<br />
setting our corporate goals we have done so with these<br />
risks in mind.<br />
Final word<br />
This will be my last <strong>Annual</strong> Report. After nearly 20 years at<br />
<strong>Homerton</strong> I am to retire at Christmas. In this Olympic year, it<br />
is with pride that I h<strong>and</strong> the baton on.<br />
Nancy Hallett<br />
Chief Executive<br />
30 May 20<strong>12</strong><br />
10 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Performance Report<br />
The Trust’s strategic vision in <strong>2011</strong>/<strong>12</strong><br />
The core components of our strategic vision have remained<br />
consistent throughout our foundation trust existence: to<br />
serve the people of Hackney; to provide a defined range of<br />
specialist services; to be thriving <strong>and</strong> sustainable; to improve<br />
performance continuously; to be characterised by modern<br />
high quality systems <strong>and</strong> processes enabled by innovation<br />
<strong>and</strong> technology with a comprehensive supporting<br />
infrastructure <strong>and</strong> buildings.<br />
With the transfer of the contract for Hackney <strong>and</strong> the City’s<br />
community health services, <strong>Homerton</strong> this year achieved an<br />
important strategic advance.<br />
In <strong>2011</strong>/<strong>12</strong> we defined three medium-term overarching<br />
strategic goals.<br />
Strategic goal 1: ‘Our Services, Our Business, Our<br />
Purpose’<br />
To maintain, grow or develop health <strong>and</strong> education<br />
‘services’ which contribute to core business <strong>and</strong> meet<br />
health need <strong>and</strong> quality requirements.<br />
Strategic goal 2: ‘Quality: Everyone – patient, visitor,<br />
staff member – treated safely, effectively <strong>and</strong><br />
decently’<br />
To, at all times, ensure that whatever we do we continually<br />
strive to improve the quality <strong>and</strong> relevance of the services<br />
we provide to our patients, their friends <strong>and</strong> loved ones <strong>and</strong><br />
our staff. A specific objective was to demonstrate real year<br />
on year progress against Quality Account measures.<br />
Strategic goal 3: ‘strengthening our reputation’<br />
To define <strong>and</strong> focus on a realistic range of areas where<br />
<strong>Homerton</strong> can build or develop its national profile,<br />
including:<br />
• community <strong>and</strong> hospital service integration <strong>and</strong>, where<br />
appropriate, the delivery of integrated care<br />
• further develop our already strong clinical informatics<br />
capability, <strong>and</strong><br />
• strengthen <strong>and</strong> build on our reputation for quality<br />
academic output.<br />
Immediate aims for <strong>2011</strong>/<strong>12</strong><br />
We identified a small number of more immediate aims for<br />
<strong>2011</strong>/<strong>12</strong>:<br />
i. Community health service integration: to integrate<br />
fully hospital <strong>and</strong> community services for the benefit of<br />
the patients we serve, our community <strong>and</strong> the Trust.<br />
ii. Quality <strong>and</strong> innovation (QIPP): to demonstrate with<br />
confidence that patient safety <strong>and</strong> quality of care are at<br />
the forefront of our work.<br />
iii. Performance <strong>and</strong> prevention (QIPP): to meet the<br />
challenging efficiency requirements we face through<br />
improving performance <strong>and</strong> productivity.<br />
Performance against corporate objectives <strong>2011</strong>/<strong>12</strong><br />
During the course of <strong>2011</strong>/<strong>12</strong> we have recorded a number<br />
of achievements:<br />
1. Successfully transferred <strong>and</strong> integrated Hackney <strong>and</strong><br />
the City’s Community Health Services.<br />
2. Through our Quality Account demonstrated that<br />
patient safety <strong>and</strong> quality of care were at the forefront<br />
of our work.<br />
3. Through our CQC inspections demonstrated safe <strong>and</strong><br />
effective care for our patients<br />
4. Achieved our financial targets without compromise<br />
to quality st<strong>and</strong>ards, allowing us to invest further in our<br />
buildings, equipment <strong>and</strong> services.<br />
5. Sustained performance against all measures, with<br />
community immunisation <strong>and</strong> screening rates seeing<br />
major improvements since transfer to us.<br />
6. Grew <strong>and</strong> developed services in response to<br />
commissioner <strong>and</strong> patient choice <strong>and</strong> using the<br />
opportunities provided by integration with community<br />
services.<br />
7. Placed ourselves back at the vanguard of health<br />
informatics, with an upgraded Electronic Patient<br />
Record system commissioned <strong>and</strong> bespoke systems<br />
such as Maternity Management in place <strong>and</strong> changing<br />
the way we work.<br />
8. The refurbishment of the hospital Main Entrance <strong>and</strong><br />
corridors, l<strong>and</strong>scaping of open spaces, <strong>and</strong> new art<br />
works <strong>and</strong> signage have revitalised the environment.<br />
9. New buildings <strong>and</strong> departments for our endoscopy,<br />
elderly care, operating theatres, HIV <strong>and</strong> sickle cell<br />
services are complete or in development.<br />
10. We were in the top 20% in the country for overall<br />
staff engagement.<br />
11. Continued to benefit from Olympic legacy donations,<br />
with the commissioning of the GE state of the art MRI<br />
scanner.<br />
<strong>12</strong>. We looked forward to <strong>and</strong> finalised preparations for<br />
the London 20<strong>12</strong> Olympic <strong>and</strong> Paralympic Games<br />
which take place on our doorstep.<br />
We may not have achieved everything we set out to do<br />
but our year has been a successful one. We did not get<br />
everything right, every time, for every patient <strong>and</strong> client,<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 11
PERFORMANCE REPORT<br />
<strong>and</strong> this we must continue to strive to do, but we do know<br />
that overall our hospital <strong>and</strong> community serves worked<br />
well, providing safe, effective, thoughtful care for those in<br />
need.<br />
Corporate Objectives 20<strong>12</strong>/13<br />
Our Corporate Objectives for 20<strong>12</strong>/13 <strong>and</strong> beyond are<br />
designed to guide staff, services <strong>and</strong> departments in setting<br />
their work programme for the year. The objectives are<br />
divided into those things we must do <strong>and</strong> those which we<br />
aspire to do.<br />
Must-do: our core work<br />
We exist to provide safe, effective, thoughtful NHS<br />
health care. In order to be allowed to continue to do this<br />
we must meet legislative <strong>and</strong> regulatory requirements.<br />
Departments need to underst<strong>and</strong> what specifically this<br />
means for them, but to some extent it can be encapsulated<br />
as follows: maintain compliance with CQC essential<br />
st<strong>and</strong>ards <strong>and</strong> those of related agencies; maintain<br />
compliance with Monitor’s financial <strong>and</strong> governance<br />
requirements; comply with legislation including fire, carbon<br />
reduction, equalities; <strong>and</strong> achieve national requirements for<br />
service delivery, teaching <strong>and</strong> research.<br />
In addition, a must-do for us is to fulfil the requirements of<br />
our 20<strong>12</strong> Olympic <strong>and</strong> Paralympic Games contract.<br />
Aspire to do<br />
We aspire to do the following because we believe<br />
they are important to our future <strong>and</strong> we will focus<br />
time <strong>and</strong> energy on them.<br />
1. Quality <strong>and</strong> safety for patients<br />
To provide the public with confidence that <strong>Homerton</strong><br />
is a very safe hospital by maintaining hospital mortality<br />
markers at a level which demonstrate this to be the case<br />
<strong>and</strong> to provide evidence that all of our services have the<br />
hallmarks of quality <strong>and</strong> safety.<br />
2. Exp<strong>and</strong>ing the organisation<br />
To grow the organisation, through a planned <strong>and</strong><br />
strategic approach to increasing referrals <strong>and</strong> establishing<br />
new services, so that we are confident we are the right<br />
size for the future.<br />
3. Community/hospital integration<br />
To be an exemplar organisation for community health<br />
<strong>and</strong> hospital services integration by fulfilling our<br />
integration programme <strong>and</strong> associated informatics <strong>and</strong><br />
premises plans. This will support us to retain the contract<br />
for the provision of community services for Hackney <strong>and</strong><br />
the City beyond 2014.<br />
4. Short waits<br />
To be a ‘short-wait’ organisation, with all patients<br />
being offered an appointment for a consultation or<br />
investigation within four weeks of referral. Patients for<br />
urgent consultations will continue to wait no more than<br />
two weeks <strong>and</strong> those presenting to the emergency<br />
department attended to within four hours.<br />
5. Communications with patients, GPs <strong>and</strong><br />
professionals<br />
To be exemplary in our engagement with the patient,<br />
GP <strong>and</strong> key professionals in relation to every interaction<br />
with our services; ensuring consultation <strong>and</strong> investigation<br />
<strong>report</strong>s are conveyed to patient, GP <strong>and</strong> professionals<br />
within five working days; <strong>and</strong> summaries from inpatient<br />
stays <strong>and</strong> emergency attendances shared within 24<br />
hours.<br />
6. Preparing <strong>and</strong> supporting our staff<br />
To prepare staff for the <strong>Homerton</strong> of the future by<br />
ensuring everyone is clear on their contribution to<br />
making this organisation <strong>and</strong> their service better,<br />
through programmes which develop service line<br />
management, clinical leaders <strong>and</strong> the ability of staff to<br />
achieve the Trust’s objectives.<br />
Principal risks & uncertainties facing the Trust<br />
All of the principal risks identified by the Trust are<br />
monitored regularly through st<strong>and</strong>ing performance <strong>report</strong>s<br />
to the Trust Board.<br />
Key risks identified include the following:<br />
• Risks associated with the condition of community health<br />
service buildings posing a risk to the ability to deliver<br />
clinical services <strong>and</strong> meeting regulatory compliance in<br />
these locations. (both in-year <strong>and</strong> future risk),<br />
• Risks to Trust business associated with the health<br />
economy reconfiguration in North East London (in-year<br />
<strong>and</strong> future risk),<br />
• Risks to Trust business associated with commissioner-led<br />
actions (both in-year <strong>and</strong> future risk),<br />
• Risks associated with the Olympic travel change<br />
impacting on access to the Trust (future risk), <strong>and</strong><br />
• Risk to organisational continuity due to change of Chief<br />
Executive Officer (future risk).<br />
The Trust has comprehensive action plans in place to<br />
mitigate the above risks which are monitored by the Risk<br />
Committee <strong>and</strong> Trust Board.<br />
The Trust’s Corporate Risk Registers <strong>and</strong> governance<br />
processes are designed to assess the impact of identified<br />
risks on the Trust’s plans, <strong>and</strong> ensure that they are<br />
appropriately mitigated or managed.<br />
<strong>12</strong> <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
The Board of Directors has reviewed the risks that may<br />
prevent the Trust from achieving its objectives, complying<br />
with its Terms of Authorisation <strong>and</strong> achieving the operating<br />
<strong>and</strong> financial plan over the review period.<br />
The objectives with the highest potential negative impact<br />
if not achieved, are identified within the Board Assurance<br />
Framework. This document is reviewed regularly by the<br />
Board with independent assurance being provided by<br />
KPMG, the Trust’s internal auditors.<br />
Review of financial performance<br />
The Trust achieved an Income & Expenditure (I&E) surplus<br />
of £6.2m for financial year <strong>2011</strong>/<strong>12</strong> (before an impairment<br />
loss of £0.9m), which exceeds the planned for surplus<br />
of 1% of our turnover. The main source of income for<br />
the Trust is contracts with commissioners in respect of<br />
healthcare services; the Trust’s main Commissioner being<br />
NHS North East London <strong>and</strong> the City.<br />
The impairment to our tangible fixed asset value was due<br />
to a reduction in market value of the Trust estate. It should<br />
be noted that the impairment does not have any impact<br />
on our financial risk rating, <strong>and</strong> is excluded from the I&E<br />
figures shown below.<br />
A comparison of planned <strong>and</strong> actual performance is shown<br />
in the table below.<br />
<strong>2011</strong>/<strong>12</strong> <strong>2011</strong>/<strong>12</strong> <strong>2011</strong>/<strong>12</strong><br />
Plan Actual Variance<br />
Income £m £m £m<br />
Clinical contracts 209.2 213.3 4.1<br />
Other income 22.7 30.4 7.7<br />
Total Income 231.9 243.7 11.8<br />
Expenses<br />
Pay (150.9) (158.8) (7.9)<br />
Non pay (68.8) (69.3) (0.5)<br />
Total Expenses (219.7) (228.1) (8.4)<br />
EBITDA* <strong>12</strong>.2 15.6 3.4<br />
Depreciation <strong>and</strong><br />
amortisation<br />
(6.3) (6.0) 0.3<br />
PDC Dividends (3.5) (3.3) 0.2<br />
Interest receivable 0.1 0.1 -<br />
Interest payable on loans (0.2) (0.2) -<br />
Net Surplus before<br />
Impairment<br />
2.3 6.2 3.9<br />
*Earnings Before Interest, Tax, Depreciation <strong>and</strong> Amortisation.<br />
The I&E surplus was achieved with additional income<br />
generated from higher than expected levels of day case,<br />
elective <strong>and</strong> outpatient activity. Activity <strong>and</strong> income for our<br />
neonatal <strong>and</strong> special care baby unit also exceeded plans.<br />
Income from non-patient activity was also above plan, for<br />
education <strong>and</strong> training <strong>and</strong> for services provided to other<br />
organisations. Expenditure was above planned levels mainly<br />
due to the costs of delivering increased activity, particularly<br />
in surgical, intensive care, <strong>and</strong> diagnostic departments.<br />
The Trust achieved £9.6m of savings during the year as part<br />
its Quality, Innovation, Productivity <strong>and</strong> Prevention (QIPP)<br />
agenda. Projects included staffing <strong>and</strong> skill mix reviews,<br />
more efficient use of our capacity <strong>and</strong> procurement<br />
initiatives to secure better prices <strong>and</strong> contractual terms from<br />
suppliers.<br />
The Trust’s liquidity position remained strong, due partly<br />
to ongoing slippage in the capital programme. Capital<br />
expenditure totalled just over £4.9m, including £1.5m<br />
related to the expansion of the endoscopy suite, a new<br />
fluoroscopy room <strong>and</strong> new <strong>and</strong> replacement medical<br />
equipment. The cash balance held by the Trust at the end<br />
of the financial year was £30.6m.<br />
The Trust complied with the cap on private patient income<br />
<strong>and</strong> achieved a financial risk rating score of 4 from Monitor,<br />
which was better than planned.<br />
The Trust strives to pay all suppliers in line with the agreed<br />
terms for each supplier but in any event no later than 30<br />
days from receipt of goods or services or the invoice date if<br />
later. During the financial year to 31 March 20<strong>12</strong> the Trust<br />
paid 87% of all non-NHS suppliers, by volume, within 30<br />
days <strong>and</strong> we will endeavour to improve this performance in<br />
future years.<br />
The Trust is in a relatively strong financial position having<br />
achieved or exceeded its planned level of surplus in recent<br />
years. We are also projecting surpluses in each of the next<br />
three years.<br />
As a result of these surpluses, careful planning, <strong>and</strong> a<br />
degree of slippage in the capital programme, the Trust has<br />
accumulated significant cash resources. We also have a<br />
working capital facility of £8.5m.<br />
Our forecast financial position can be projected with a<br />
reasonable degree of certainty in the short term as in<br />
excess of 70% of our clinical income is derived from one<br />
commissioner with which we have a good relationship.<br />
The Trust’s treasury management strategy is routinely<br />
reviewed by the Finance <strong>and</strong> Performance Committee,<br />
a subcommittee of the Board. The most recent review<br />
occurred in March 20<strong>12</strong>. The Committee did not identify<br />
any immediate liquidity concerns. We are confident that we<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 13
PERFORMANCE REPORT<br />
have sufficient funds to remain as a going concern - that is<br />
for at least the next <strong>12</strong> months.<br />
The Trust has complied with the cost allocation <strong>and</strong><br />
charging requirements set out in HM Treasury <strong>and</strong> Office of<br />
Public Sector Information guidance. Accounting policies for<br />
pensions are set out in note 1.4 to the <strong>accounts</strong> <strong>and</strong> details<br />
of senior employees’ remuneration can be found on page<br />
105 of the <strong>Annual</strong> Accounts.<br />
Counter fraud policies <strong>and</strong> procedures<br />
The Trust has a counter fraud policy for dealing with<br />
suspected fraud <strong>and</strong> corruption, <strong>and</strong> other illegal acts<br />
involving dishonesty or damage to property. Staff can<br />
contact Nominated Officers in confidence if they suspect a<br />
fraudulent act. The Nominated Officers are the Director of<br />
Finance <strong>and</strong> our local counter fraud specialist, RSM Tenon.<br />
Regulatory ratings<br />
In line with Monitor’s Compliance Framework each<br />
foundation trust must submit an <strong>Annual</strong> Plan including<br />
detailed financial forecasts for the three years ahead by the<br />
end of May each year.<br />
Monitor use the information in the plan submitted by<br />
foundation trusts to evaluate the risk of failure to comply<br />
with the Trust’s Terms of Authorisation <strong>and</strong> to assign risk<br />
ratings covering financial <strong>and</strong> governance.<br />
Explanation of ratings<br />
Financial risk rating - when assessing financial risk,<br />
Monitor assigns a financial risk rating using a scorecard<br />
comparing key financial metrics on a consistent basis across<br />
all NHS foundation trusts.<br />
The risk rating is intended to reflect the likelihood of a<br />
significant breach of the Terms of Authorisation.<br />
The financial indicators used to derive the financial<br />
risk rating incorporate individual metrics comprising<br />
achievement of plan; underlying performance; financial<br />
activity <strong>and</strong> liquidity which are each rated 1 (high risk) to 5<br />
(low risk).<br />
Governance risk rating - Monitor’s assessment of<br />
governance risk is based predominantly on NHS foundation<br />
trusts’ plans for ensuring compliance with their Terms of<br />
Authorisation but will also reflect historic performance<br />
where this may be indicative of future risk.<br />
Monitor considers the following elements when assessing<br />
the governance risk rating: legality of constitution; growing<br />
a representative membership; appropriate Board roles <strong>and</strong><br />
structures; service performance; clinical quality <strong>and</strong> patient<br />
safety; effective risk <strong>and</strong> performance management; cooperation<br />
with NHS bodies <strong>and</strong> local authorities; <strong>and</strong> the<br />
provision of m<strong>and</strong>atory services.<br />
Monitor rates governance risk using a graduated system<br />
of green, amber/green, amber/red <strong>and</strong> red, where green<br />
indicates low risk <strong>and</strong> red indicates high risk.<br />
Performance is reviewed in-year by Monitor. The nature <strong>and</strong><br />
frequency of their review is based on each trust’s risk scores,<br />
with those foundation trusts rated at a higher level of risk<br />
required to <strong>report</strong> more often <strong>and</strong> in greater detail.<br />
Summary of performance<br />
The tables below show <strong>Homerton</strong>’s risk rating scores for<br />
2010/11 <strong>and</strong> <strong>2011</strong>/<strong>12</strong>.<br />
2010/11<br />
Financial<br />
risk rating<br />
Governance<br />
risk rating<br />
<strong>2011</strong>/<strong>12</strong><br />
Financial<br />
risk rating<br />
Governance<br />
risk rating<br />
<strong>Annual</strong><br />
Plan<br />
Q1 Q2 Q3 Q4<br />
3 4 3 3 3<br />
Green Green Green Amber/<br />
Green<br />
<strong>Annual</strong><br />
Plan<br />
Amber/<br />
Red<br />
Q1 Q2 Q3 Q4<br />
3 4 4 4 4<br />
Green Green Green Green<br />
Financial risk rating<br />
For <strong>2011</strong>/<strong>12</strong> the planned financial risk rating of 3 was<br />
exceeded with all key financial targets met.<br />
Amber/<br />
Green<br />
Governance risk rating<br />
In the first three quarters <strong>2011</strong>/<strong>12</strong> the Trust was rated<br />
“green” for governance risk. The “amber/green” rating<br />
for <strong>Homerton</strong> in Q4 <strong>2011</strong>/<strong>12</strong> was due to the Trust’s minor<br />
under achievement against the 62 day cancer target.<br />
14 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Review of non-financial performance<br />
Patient activity<br />
With the transfer of City & Hackney’s community health<br />
services, there has been a significant increase in patient<br />
activity in the Trust. In addition, there has been a marked<br />
increase in activity within a number of our hospital services.<br />
The table below shows the <strong>report</strong>ed activity levels against<br />
the contractual plan for <strong>2011</strong>/<strong>12</strong>.<br />
The Trust has decreased clinically unnecessary outpatient<br />
follow up appointments <strong>and</strong> outpatient DNA (did not<br />
attend) rates. These improvements have been possible<br />
through effective joint working with City & Hackney GPs<br />
<strong>and</strong> through the implementation of initiatives such as the<br />
expansion of telephone <strong>and</strong> email advice services for GPs.<br />
These measures have allowed the Trust to accommodate<br />
the increase in new GP referrals identified above.<br />
Category <strong>2011</strong>/<strong>12</strong><br />
plan<br />
<strong>2011</strong>/<strong>12</strong><br />
activity<br />
% above/below<br />
plan<br />
<strong>Hospital</strong> (acute) elective spells 16,620 18,047 8.6%<br />
<strong>Hospital</strong> (acute) non-elective spells (including deliveries) 28,989 30,9<strong>12</strong> 6.6%<br />
<strong>Hospital</strong> outpatient attendances 258,494 258,498 0 %<br />
A&E attendances (including pucc) 116,173 111,533 -4.0%<br />
Adult community services – attendances <strong>and</strong> contacts* 332,101 315,496 -5.0%<br />
Children’s community services – attendances <strong>and</strong> contacts* 275,831 287,416 4.2%<br />
Adult critical care <strong>and</strong> rehabilitation – occupied bed days 30,377 26,189 -13.8%<br />
Neonatal critical care – occupied bed days 11,049 13,960 26.4%<br />
Direct access diagnostics (radiology, pathology, cardiac) – tests 836,731 902,833 7.9%<br />
Outreach neurological rehabilitation – sessions 1,<strong>12</strong>5 1,317 17.1%<br />
Other (inc. fertility, regular attenders, therapies <strong>and</strong> podiatry) - attendances 13,547 14,522 7.2%<br />
* The Trust is continuing to review the way in which community<br />
activity is defined <strong>and</strong> recorded<br />
The services with the most marked increase in activity<br />
are: Neonatal Critical Care; Oral & Maxillofacial surgery;<br />
Gastroenterology; Children’s Specialist Nursing; Wheelchair<br />
services; Community Paediatrics; Community Sexual Health<br />
services<br />
In <strong>2011</strong>/<strong>12</strong>, there was a small reduction in Emergency<br />
Department attendances (4%) but an increase in the<br />
number of emergency admissions (excluding deliveries) by<br />
5.2%. This may suggest that patients who are less acutely<br />
ill are accessing services outside of hospital locations.<br />
Despite this, the average length of stay for emergency<br />
admissions has been reduced from 5.1 days to 4.9 days.<br />
Although Outpatient activity overall was on plan, the<br />
Trust has seen a growth in dem<strong>and</strong> for first Outpatient<br />
attendances (3.7% above plan). This reflects increased<br />
referrals for both City & Hackney patients (1.6%) <strong>and</strong><br />
out of borough patients (8.9% above plan). A new<br />
Nephrology service was introduced this year, offering City &<br />
Hackney patients suffering from chronic kidney disease the<br />
opportunity to be seen at their local hospital.<br />
<strong>2011</strong>/<strong>12</strong> saw the Trust deliver over 5,000 babies, with an<br />
increase in women from out of area booking with us for<br />
maternity care. The implementation of a new electronic<br />
maternity management system is expected to contribute to<br />
improved service outcomes.<br />
With the national focus on the care of older people,<br />
significant changes were made to the <strong>Homerton</strong> Elderly<br />
Care service in <strong>2011</strong>/<strong>12</strong>. A daily care of the elder consultant<br />
ward round has been implemented on the Acute Care<br />
Unit (emergency receiving ward). This ensures that patients<br />
are identified early <strong>and</strong> are transferred quickly to the new<br />
integrated Elderly Care Unit. This unit combines both<br />
the acute medical <strong>and</strong> rehabilitation elements of older<br />
people’s care, with improved outcomes for elderly patients<br />
anticipated.<br />
The Regional Neurological Rehabilitation Unit (RNRU)<br />
increased its capacity in <strong>2011</strong>/<strong>12</strong> by three beds (<strong>12</strong>.5%)<br />
enabling the Trust to admit <strong>and</strong> rehabilitate more<br />
neurological patients than it has in previous years.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 15
PERFORMANCE REPORT<br />
Sickle Cell related emergency admissions continued<br />
to rise in <strong>2011</strong>/<strong>12</strong>. To help avoid clinically unnecessary<br />
admissions for Sickle Cell patients, the Trust has invested in<br />
the provision of a dedicated psychological service <strong>and</strong> has<br />
implemented an automated exchange transfusion system.<br />
It is anticipated that this will lead to a reduction in both the<br />
frequency of admissions <strong>and</strong> length of stay.<br />
A number of acute <strong>and</strong> community services were<br />
integrated for the first time in <strong>2011</strong>/<strong>12</strong>. This includes the<br />
sexual health services who now share patient information<br />
systems <strong>and</strong> clinical governance structures, resulting in<br />
anticipated better clinical outcomes.<br />
With the transfer of community services to the Trust, it<br />
has been possible to integrate the hospital’s Emergency<br />
Department <strong>and</strong> Primary <strong>and</strong> Urgent Care Centre (PUCC),<br />
enabling clinical teams to work more effectively in providing<br />
emergency <strong>and</strong> urgent care to the local population. This<br />
has also led to an increase in the proportion of patients<br />
seen in PUCC rather than the Emergency Department.<br />
Other anticipated benefits of acute <strong>and</strong> community<br />
integration have, we believe, been realised including the<br />
reduction in attendances to the Emergency Department, a<br />
reduction in emergency length of stay <strong>and</strong> a reduction in<br />
the number of hospital follow up appointments patients<br />
receive.<br />
The Hackney referrals processing service <strong>and</strong> the<br />
<strong>Homerton</strong> outpatient booking team now have an<br />
integrated management structure. This has supported an<br />
improvement in the h<strong>and</strong>ling of patient calls to book or<br />
change appointments.<br />
Community paediatric services have improved the links<br />
with the acute paediatric team; this has led to improved<br />
psychology support for the hospital paediatric service <strong>and</strong><br />
improvement in the case management of children with<br />
complex needs.<br />
Our operational performance<br />
The Trust performed strongly in <strong>2011</strong>/<strong>12</strong>. Our average<br />
waiting time for an outpatient appointment was five weeks<br />
<strong>and</strong> for elective or day surgery was 11 weeks.<br />
The Trust was set challenging targets with regard to MRSA<br />
<strong>and</strong> Clostridium difficile infections but achieved these,<br />
making <strong>Homerton</strong> one of the highest achieving Trusts with<br />
regard to infection control in the country with no cases<br />
of MRSA in <strong>2011</strong>/<strong>12</strong>. The Trust has also seen a reduction<br />
in the number of mixed sex accommodation breaches it<br />
has <strong>report</strong>ed in <strong>2011</strong>/<strong>12</strong> <strong>and</strong> this remains a focus area for<br />
20<strong>12</strong>/13.<br />
The following table sets out performance against certain<br />
key targets on a cumulative basis for the year as a whole<br />
although we, as with all foundation trusts, are required<br />
to <strong>report</strong> to Monitor on a range of measures in-year on a<br />
quarterly basis. Further information on performance against<br />
quality st<strong>and</strong>ards is included in the Quality Account.<br />
Key Performance<br />
Indicators<br />
A&E patients<br />
discharged < 4hrs<br />
<strong>2011</strong>/<strong>12</strong><br />
Target<br />
<strong>2011</strong>/<strong>12</strong><br />
Performance<br />
95% 96.8%<br />
Cancer Waiting List<br />
2 Week Wait 93% 96.0%<br />
31 Day Target 96% 100%<br />
62 Day Target 85% 89.4%<br />
Infection Control<br />
MRSA ≤ 3 0<br />
Clostridium difficile (C diff) ≤<strong>12</strong> 9<br />
18 Week RTT Indicator<br />
Admitted<br />
(95th percentile)<br />
Non Admitted<br />
(95th percentile)<br />
23 weeks 18 weeks<br />
18.3 weeks 15 weeks<br />
Whilst we performed strongly, we recognise that there are<br />
always areas for improvement.<br />
Despite seeing a continued improvement in our cancer 62<br />
day waits, our Q4 performance dropped below the national<br />
threshold.<br />
With regard to community health services, the Trust is<br />
performing well against the National KPIs for sexual health<br />
services, referral to treatment time targets <strong>and</strong> breast<br />
feeding targets. However, immunisation targets remain the<br />
area presenting the greatest challenge.<br />
Patient care<br />
The Trust’s new Patient Experience Strategy, launched in<br />
September <strong>2011</strong>, ensures patients, users, the membership<br />
<strong>and</strong> staff are involved in planning improvements <strong>and</strong> giving<br />
their views regarding the quality of services provided by the<br />
Trust.<br />
The strategy was developed following a large listening<br />
exercise whereby the views of patients, users, members,<br />
staff <strong>and</strong> Governors were sought. It combines the<br />
previous Patient <strong>and</strong> Public Engagement Strategy <strong>and</strong> the<br />
Membership Strategy into one simple framework.<br />
16 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Comprehensive detail regarding the quality of patient care<br />
<strong>and</strong> patient satisfaction is included in the Trust Quality<br />
Account.<br />
Complaints<br />
The Trust received a total of 253 complaints for the year<br />
ending 31 March 20<strong>12</strong>. The graph below shows the<br />
comparison of the complaints received in <strong>2011</strong>/<strong>12</strong> with<br />
previous years.<br />
Total formal complaints April 2009 – March 20<strong>12</strong> by month<br />
35<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Apr<br />
May<br />
Jun<br />
Jul<br />
Aug<br />
Sep<br />
Oct<br />
Nov<br />
Dec<br />
2009/10 2010/11 <strong>2011</strong>/<strong>12</strong><br />
Jan<br />
Feb<br />
Mar<br />
Six complainants have asked the Parliamentary Health<br />
Service Ombudsman (PHSO) to review their cases. Of these<br />
complaints, the Trust is awaiting the ombudsman’s decision<br />
on two cases. No further action has been taken on the<br />
remaining four.<br />
The Trust recorded the theme for all complaints received<br />
during <strong>2011</strong>/<strong>12</strong>. The table below shows that the main area<br />
of concerns for patients <strong>and</strong> service users were:<br />
Area of concern<br />
All aspects of clinical treatment 110<br />
Attitude of staff 44<br />
Communication/information to patients<br />
(written <strong>and</strong> oral) 25<br />
Appointments, delay/cancellation<br />
(outpatient) 19<br />
Admissions, discharge <strong>and</strong> transfer<br />
arrangements 13<br />
Failure to follow agreed procedures 11<br />
Others 31<br />
Total: 253<br />
Response times<br />
A total of 253 formal complaints were received between<br />
April <strong>2011</strong> to March 20<strong>12</strong>, of these the Trust responded<br />
to 195 (77%) within 25 working days excluding those<br />
complaints where the case was ‘clock stopped’ due to<br />
meetings being arranged with the complainant, or the<br />
complaint was declared a Serious Incident. The Trust aims<br />
to respond to 75% of complaints within 25 days however,<br />
we recognise that in more complex cases a longer period is<br />
required to fully investigate the issues raised.<br />
Learning from complaints<br />
Whilst it is disappointing to receive any complaints about<br />
the services we provide, we want to know when patients<br />
or their carers are dissatisfied with any aspect of their<br />
involvement with the Trust, so that we can take actions<br />
to improve services. Some specific actions that have been<br />
taken as a result of complaints included:<br />
• changes to the processes for managing GP patient<br />
referrals through the Accident <strong>and</strong> Emergency<br />
Department<br />
• increased security <strong>and</strong> changes to entrance/exit doors to<br />
the Trust’s Nursing Care Home<br />
• reviewed arrangements for patient property in the Trust<br />
surgical centre, <strong>and</strong><br />
• introduction of a new twins information leaflet in<br />
Maternity.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 17
PERFORMANCE REPORT<br />
Working with staff<br />
With the integration of community health services, the<br />
number of people directly employed by <strong>Homerton</strong> grew<br />
from 2,573 in 2010/11 to 3,354 in 20<strong>12</strong>/13 (3044 wte).<br />
Excluded from these numbers are pre <strong>and</strong> postgraduate<br />
health care practitioners who were placed with us for<br />
training, <strong>and</strong> catering <strong>and</strong> domestic personnel provided<br />
under contract.<br />
The integration of the hospital <strong>and</strong> community teams<br />
is considered to have gone well, with staff appearing<br />
comfortable with the change <strong>and</strong> no drops in service<br />
performance or quality noted.<br />
In the national staff survey for 2010/11 <strong>and</strong> <strong>2011</strong>/<strong>12</strong> we<br />
remained in the top 20% for ‘recommending the Trust as a<br />
place to work <strong>and</strong> receive treatment’.<br />
Staff performance <strong>and</strong> support<br />
Performance against workforce indicators overall remains<br />
steady, with the Board <strong>and</strong> managers receiving monthly<br />
performance information.<br />
We have seen a small <strong>report</strong>ed increase in average sickness<br />
absence rates in the last year from 3.2% to 3.5%. The Trust<br />
has well established policies <strong>and</strong> procedures for managing<br />
sickness absence, <strong>and</strong> also has onsite occupational health<br />
services.<br />
The Trust’s staff influenza vaccination campaign resulted<br />
in 1,744 staff vaccinated, including just over 53.2% of<br />
frontline staff, putting the Trust in the top four performing<br />
acute Trusts in London.<br />
The <strong>Homerton</strong> Health Works initiative continues, offering<br />
exercise <strong>and</strong> lifestyle improvement activities for staff<br />
with the support of a personal trainer providing lifestyle<br />
coaching. Other staff benefits include child care support,<br />
social events <strong>and</strong> staff discounts.<br />
Staff survey response rate<br />
Top four ranking scores<br />
Percentage of staff able to contribute towards<br />
improvements at work<br />
Staff involvement <strong>and</strong> engagement<br />
We have established mechanisms to ensure the<br />
involvement of staff <strong>and</strong> staff representatives in the<br />
planning <strong>and</strong> development of services. A ‘Team Brief’<br />
system operates which cascades key messages across the<br />
Trust on a monthly basis. This is complemented with a Staff<br />
Newsletter <strong>and</strong> item specific briefings. Payslip attachments<br />
(or personal letters) are also used where assurance is<br />
required that 100% of staff have received information on a<br />
specific matter.<br />
The Joint Staff Consultative Committee <strong>and</strong> the Local<br />
Negotiating Committee (for doctors) are well established.<br />
All elected Staff Governor positions are filled <strong>and</strong> their<br />
participation in Council of Governors meetings supported.<br />
Staff survey<br />
The Trust experienced a reduction in response rate from<br />
52% to 42%; we did not campaign as hard as we normally<br />
do to secure respondents <strong>and</strong> we will need to refocus for<br />
next year.<br />
In the ‘staff engagement’ category we continued to be in<br />
the highest 20% for the country; strong performance was<br />
shown in the facets; ‘staff feel they are able to contribute<br />
towards improvements at work’; ‘staff motivation’;<br />
‘recommend <strong>Homerton</strong> as place to work <strong>and</strong> as a place to<br />
be treated’. These continue to be encouraging results.<br />
There are areas where improvements need to be made.<br />
Our action plan will include a focus on: further increasing<br />
appraisal <strong>and</strong> m<strong>and</strong>atory training including equalities<br />
training rates; reducing the sources of pressure <strong>and</strong> stress in<br />
the workplace <strong>and</strong> ‘long hours’ culture. We are concerned<br />
that staff are <strong>report</strong>ing abuse from patients <strong>and</strong> focused<br />
work will be required to ensure our staff feel safe.<br />
2010/11 <strong>2011</strong>/<strong>12</strong><br />
Change<br />
Trust Nat. Ave Trust Nat. Ave<br />
52% 52% 42% 53% 10%<br />
2010/11 <strong>2011</strong>/<strong>12</strong><br />
Change<br />
Trust Nat. Ave Trust Nat. Ave<br />
71% 62% 77% 61% + 6%<br />
Quality of job design (clear job content, feedback 3.60* 3.41* 3.59* 3.41* - 0.01<br />
<strong>and</strong> staff involvement)<br />
Percentage of staff satisfied with the quality of work 89% 74% 85% 74% - 4%<br />
<strong>and</strong> patient care they are able to deliver<br />
Support from immediate managers 3.84* 3.61* 3.79* 3.61* - 0.05<br />
*5 point scale summary score<br />
18 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Bottom four ranking scores<br />
2010/11 <strong>2011</strong>/<strong>12</strong><br />
Trust Nat. Ave Trust Nat. Ave<br />
Change<br />
Percentage of staff experiencing harassment, bullying or<br />
abuse from patients, relatives or public in last <strong>12</strong> months<br />
Percentage of staff suffering work-related stress in last<br />
<strong>12</strong> months<br />
Percentage of staff having equality <strong>and</strong> diversity training<br />
in last <strong>12</strong> months<br />
Percentage of staff experiencing discrimination at work<br />
in last <strong>12</strong> months<br />
18% 15% 20% 15% + 2%<br />
26% 28% 34% 29% + 8%<br />
35% 41% 29% 48% - 6%<br />
16% 13% 19% 13% + 3%<br />
Education <strong>and</strong> related activities<br />
Statutory <strong>and</strong> m<strong>and</strong>atory training, functional skills for<br />
work, <strong>and</strong> personal <strong>and</strong> professional staff development<br />
skills are delivered through the Learning & Development<br />
Department. The national Staff Survey <strong>2011</strong> results<br />
<strong>report</strong>ed the Trust was in the highest 20% in the<br />
country for staff having opportunities to develop their<br />
potential at work over the last <strong>12</strong> months receiving wellstructured<br />
appraisals <strong>and</strong> job-relevant training, learning or<br />
development.<br />
The Trust is committed to providing a safe <strong>and</strong> healthy<br />
environment for its patients, members of the public <strong>and</strong><br />
staff. The Trust is required by law <strong>and</strong> national guidance to<br />
provide a range of training in order to maintain a healthy<br />
working environment <strong>and</strong> ensure the workforce has the<br />
correct level of knowledge <strong>and</strong> skills to operate safely.<br />
This is known as statutory <strong>and</strong> m<strong>and</strong>atory training (SMT).<br />
In recent years the Trust has had inadequate compliance<br />
rates for SMT. In the last 18 months, the delivery of SMT<br />
has been restructured, <strong>and</strong> the appraisal process has been<br />
updated to include a review of SMT compliance. These<br />
measures have resulted in an increase in compliance.<br />
Further work is continuing to ensure that satisfactory levels<br />
are achieved.<br />
Professional nursing & midwifery education<br />
<strong>Homerton</strong> continues to provide educational placements for<br />
pre <strong>and</strong> post registration students in nursing, midwifery <strong>and</strong><br />
health visiting as well as a range of opportunities for our<br />
own nursing, midwifery <strong>and</strong> health visiting staff.<br />
The placement of the year is an award given to clinical<br />
areas where City <strong>University</strong> pre-registration students in<br />
nursing <strong>and</strong> midwifery have had an exemplary learning<br />
experience. In <strong>2011</strong>/<strong>12</strong> the Acute Care, Respiratory<br />
Community team, the Emergency Department, Starlight<br />
Ward, Somerford Grove Health Visiting <strong>and</strong> Barton House<br />
District Nursing were all commended by students in the<br />
awards.<br />
We received funding from NHS London to establish a<br />
nursing <strong>and</strong> midwifery academic research unit here at the<br />
<strong>Homerton</strong>.<br />
Medical education<br />
In the <strong>2011</strong>/<strong>12</strong> the Trust continued to demonstrate<br />
its commitment to the delivery of undergraduate<br />
<strong>and</strong> postgraduate education. The annual inspections<br />
undertaken by Barts <strong>and</strong> the London School of Medicine<br />
<strong>and</strong> Dentistry, North East Thames Foundation School <strong>and</strong><br />
the London Deanery were all positive. Although the results<br />
of the <strong>2011</strong> National Trainee Survey identified some areas<br />
requiring improvement, the results were generally strong.<br />
The Simulation Centre was officially opened in October<br />
<strong>2011</strong> <strong>and</strong> both the Simulation Centre <strong>and</strong> the Library won<br />
awards for their work in <strong>2011</strong>. The Trust hosted its first<br />
annual Simulation Conference in <strong>2011</strong>. Other innovations<br />
included a project exploring new ways of improving the<br />
teaching skills of foundation programme trainees.<br />
The Trust continues to see a good number of medical<br />
students who have undertaken placements at the Trust<br />
choosing to return to <strong>Homerton</strong> for foundation programme<br />
or specialty training. A number of our recent consultant<br />
appointments have been doctors who undertook training<br />
posts at <strong>Homerton</strong>.<br />
Research & development.<br />
Research <strong>and</strong> development (R&D) in the Trust continues<br />
to develop <strong>and</strong> support research studies in areas of local<br />
relevance for example HIV, respiratory disease/TB, allergy,<br />
neuro-rehabilitation, stroke, diabetes, fertility, community<br />
services <strong>and</strong> neonatal care. We have 157 active research<br />
projects within the Trust in 23 different specialties. In<br />
addition the Trust is an active member of the Central<br />
London Comprehensive Local Research Network <strong>and</strong><br />
currently hosts 70 NIHR Portfolio Studies.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 19
PERFORMANCE REPORT<br />
Equality & diversity<br />
The Board Executive lead for equality <strong>and</strong> diversity is the<br />
Chief Nurse & Director of Governance. The Equalities<br />
Report <strong>2011</strong> <strong>and</strong> our Equality Objectives 20<strong>12</strong> are available<br />
from our website at www.homerton.nhs.uk. All publication<br />
duties have been met.<br />
We chose our equality objectives by considering evidence<br />
from patient <strong>and</strong> public feedback, complaints <strong>and</strong> Patient<br />
Advocacy <strong>and</strong> Liaison Service (PALS) enquiries, as well as the<br />
results of the national staff <strong>and</strong> patient surveys.<br />
Our objectives are:<br />
1. To establish a Governor-led equality <strong>and</strong> diversity group<br />
in order to lead <strong>and</strong> champion our programme of work<br />
related to equality <strong>and</strong> diversity.<br />
2. To foster an organisation which underst<strong>and</strong>s the cultural<br />
needs of our patients <strong>and</strong> staff through a series of<br />
activities including a cultural awareness campaign.<br />
3. To build on our work to ensure the needs of patients<br />
with learning disabilities are met when receiving<br />
healthcare by promoting the MENCAP ‘Getting it Right<br />
Charter’ for learning disabilities.<br />
4. To participate in the MIND / Rethink mental illness ‘time<br />
to change’ campaign to tackle stigma <strong>and</strong> discrimination<br />
by changing attitudes <strong>and</strong> behaviour towards mental<br />
health problems.<br />
Policies in relation to disabled employees<br />
<strong>and</strong> equal opportunities<br />
Our services <strong>and</strong> employment practices must be accessible<br />
<strong>and</strong> fair to all; employees <strong>and</strong> service users must be<br />
treated with respect <strong>and</strong> not subject to any form of<br />
discrimination, harassment or victimisation on the basis<br />
Summary of Trust workforce <strong>and</strong> Foundation Trust membership diversity data<br />
Staff<br />
Membership<br />
2010/11 % <strong>2011</strong>/<strong>12</strong> % 2010/11 % <strong>2011</strong>/<strong>12</strong> %<br />
Age<br />
Age<br />
16-25 193 8 230 7 17-21 89 1 72 1<br />
26-35 758 31 1041 31 22-29 458 7 420 6<br />
36-45 7<strong>12</strong> 29 904 27 30-39 713 11 735 11<br />
46-55 5<strong>12</strong> 21 774 23 40-49 655 10 717 11<br />
56-65 237 10 337 10 50-59 441 7 511 7<br />
66+ 20 1 31 1 60-74 426 7 481 7<br />
75+ 156 2 185 3<br />
Not Stated Not stated 3571 55 3698 54<br />
Total 2432 3317 Total 6509 6819<br />
Ethnicity<br />
Ethnicity<br />
White 1044 43 1488 45 White 2175 33 2256 33<br />
Mixed 68 3 74 2 Mixed 185 3 198 3<br />
Asian or Asian British 423 17 495 15 Asian or Asian British 545 8 560 8<br />
Black or Black British 749 30 1055 32 Black or Black British 1078 17 1198 17<br />
Undefined 22 1 5 0.1 Other - Specified 230 4 233 4<br />
Other Specified 76 2 107 3 Undisclosed 2296 35 2374 34<br />
Not Stated 50 2 93 3<br />
Total 2432 3317 Total 6509 6819<br />
Gender<br />
Gender<br />
Male 630 26 776 23 Male 2293 35 2326 34<br />
Female 1802 74 2541 77 Female 3949 61 4134 60<br />
Total 2432 3317 Undisclosed 267 4 359 5<br />
Total 6509 6819<br />
Recorded Disability 26 1 34 1 Recorded Disability 6 0.1 30 0.4<br />
Total 2432 3317 Total 6509 6819<br />
20 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
of age, disability, gender reassignment, marriage <strong>and</strong> civil<br />
partnership, pregnancy or maternity, race (this includes<br />
ethnic or national origins, colour or nationality), religion or<br />
belief (including lack of belief), sex <strong>and</strong> sexual orientation.<br />
These are known as the nine protected characteristics of<br />
the Equalities Act 2010. We are committed to promoting<br />
equality of opportunity <strong>and</strong> eliminating discriminatory<br />
practice.<br />
Stakeholder relations<br />
The Trust continues to have strong relationships with<br />
stakeholders within the NHS, Local Authority <strong>and</strong> education<br />
partners as well as community <strong>and</strong> patient representative<br />
groups. The City <strong>and</strong> Hackney Clinical Commissioning<br />
Group is now established as the lead health commissioner<br />
for the Hackney <strong>and</strong> City populations. We are engaged in<br />
the development of the Health <strong>and</strong> Social Care Partnership<br />
Board for Hackney. The Trust is now an executive partner of<br />
<strong>University</strong> College London Partners.<br />
Key stakeholders have nominated representatives on<br />
the Council of Governors which also includes elected<br />
representatives of members of the public living in our local<br />
boroughs <strong>and</strong> Trust staff.<br />
The Trust has a statutory duty to collaborate with partners<br />
in health <strong>and</strong> social care. We have representation at the<br />
monthly Hackney Health Scrutiny Commission meetings,<br />
which are held in public, providing them with regular<br />
service <strong>and</strong> performance updates.<br />
Sustainability/Climate change <strong>report</strong><br />
The NHS Sustainable Development Unit’s “Saving Carbon,<br />
Improving Health” sets a target for NHS trusts to reduce<br />
their carbon emissions by at least 10% between 2007<br />
<strong>and</strong> 2015 <strong>and</strong> to develop a Board approved carbon<br />
management strategy. The Board approved the Carbon<br />
Management Strategy in June 2010 <strong>and</strong> this is available<br />
on the Trust website. Our plan indentifies opportunities<br />
for carbon reduction, target setting <strong>and</strong> outcome<br />
measurement, to reduce our carbon footprint by the<br />
m<strong>and</strong>ated 10% by 2015. The Trust successfully completed<br />
the Carbon Trust’s NHS Carbon Management Programme<br />
in March <strong>2011</strong>.<br />
Water consumption <strong>and</strong> expenditure has reduced<br />
significantly following the implementation of water<br />
efficiency measures.<br />
Electricity consumption appears to be stabilising, reversing<br />
the previous trend of a 3% increase per year. This is most<br />
likely due to awareness raising activities, staff training <strong>and</strong><br />
the higher profile of environmental sustainability at the<br />
Trust. However electricity costs were higher <strong>and</strong> this is<br />
reflected in expenditure. Gas <strong>and</strong> Oil consumption have<br />
reduced in line with dem<strong>and</strong> reduction measures <strong>and</strong> a<br />
mild winter. On average the price of utilities has increased<br />
in <strong>2011</strong>/<strong>12</strong>.<br />
Summary environmental performance is shown in the<br />
table below<br />
Non-financial data<br />
Financial data(£k)<br />
Type 2010/11 <strong>2011</strong>/<strong>12</strong> 2010/11 <strong>2011</strong>/<strong>12</strong><br />
Utilities<br />
Water (m3) 94,070 86,445 192 148<br />
Electricity<br />
(MWh)<br />
Gas<br />
(MWh)<br />
Oil<br />
(MWh)<br />
9,793 9,892 950 1,054<br />
3,880 3,145 154 185<br />
20,643 18,426 765 889<br />
Total 2061 2276<br />
Waste<br />
Residual<br />
(tonnes)<br />
Recycling<br />
(tonnes)<br />
Clinical<br />
(tonnes)<br />
Offensive<br />
(tonnes)<br />
High Temp<br />
Incineration<br />
(tonnes)<br />
508 488<br />
86 88<br />
309 252<br />
7 96<br />
32 36<br />
Total 942* 960 241 193<br />
*2010/11 amount of waste produced has been restated to correct<br />
an understatement in last year’s <strong>Annual</strong> Report.<br />
The total amount of waste generated by the Trust has<br />
increased <strong>and</strong> this may be due to increased activity. The<br />
Trust has now rolled out an “offensive” waste stream to<br />
most general wards <strong>and</strong> outpatient departments which<br />
is reducing costs <strong>and</strong> benefiting the environment as this<br />
waste stream does not need to be sterilised before final<br />
disposal. The financial savings reflect this <strong>and</strong> the new<br />
contract for clinical waste management that started in<br />
October.<br />
The Trust’s Carbon Footprint, associated with emissions<br />
from energy, waste, water <strong>and</strong> business travel, have fallen<br />
from 11,150 tonnes in 2010/11 to 10,920 tonnes in<br />
<strong>2011</strong>/<strong>12</strong> representing a 2% reduction CO2.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 21
GOVERNANCE REPORT<br />
Governance Report<br />
The following disclosures relate to the Trust’s governance<br />
arrangements <strong>and</strong> illustrate the application of the main <strong>and</strong><br />
supporting principles of Monitor’s Code of Governance (the<br />
Code).<br />
It is the responsibility of the Board of Directors to ensure<br />
that the Trust complies with the provisions of the Code or,<br />
where it does not, to provide an explanation which justifies<br />
departure from the Code in the particular circumstances.<br />
For the year ending 31 March 20<strong>12</strong> the Trust complied with<br />
all the provisions of the Code.<br />
Board of Directors<br />
Composition of the Board<br />
In accordance with our Constitution, the Board of Directors<br />
had seven executive <strong>and</strong> seven non-executive directors<br />
including the Chairman at the start of <strong>2011</strong>/<strong>12</strong>. The<br />
Board of Directors is accountable to the membership<br />
via the Council of Governors. The Board provides<br />
leadership to the hospital <strong>and</strong> sets the strategic direction<br />
of the organisation. The Board decides upon matters of<br />
operational performance, risk, assurance <strong>and</strong> governance.<br />
Board members are invited to attend Council of Governors<br />
meetings <strong>and</strong> joint Board meetings are held twice a year to<br />
discuss strategic plans.<br />
In <strong>2011</strong>/<strong>12</strong> the Board had the following members:<br />
Non-Executive Directors<br />
Chairman, Michael Cassidy; Deputy Chairman <strong>and</strong> Senior<br />
Independent Director, Stephen Hay, Prof Michael Keith,<br />
Imelda Redmond, Prof Christopher Griffiths, David Stewart,<br />
Sir John Gieve (from November <strong>2011</strong>) <strong>and</strong> Eric Sorensen<br />
(until October <strong>2011</strong>).<br />
Executive Directors<br />
Nancy Hallett, Chief Executive; Dr John Coakley, Medical<br />
Director <strong>and</strong> Joint Deputy CEO; Tracey Fletcher, Chief<br />
Operating Officer <strong>and</strong> Joint Deputy CEO; Charlie Sheldon,<br />
Chief Nurse & Director of Governance; Jo Farrar, Director<br />
of Finance; Cheryl Clements, Director of Workforce <strong>and</strong><br />
Education; <strong>and</strong> Andrew Panniker, Director of Environment<br />
(until October <strong>2011</strong>).<br />
The term of office for non-executive directors is three years.<br />
Following this term, <strong>and</strong> subject to satisfactory appraisal,<br />
a non-executive director is eligible for consideration by<br />
the Council of Governors for a further uncontested term<br />
of three years. The appointment process, undertaken<br />
on behalf of the Council of Governors by a Nominations<br />
Committee, is outlined in Section 13 of the Trust’s<br />
constitution.<br />
The Chairman <strong>and</strong> Non-Executive Directors can also be<br />
removed by the Council of Governors. The removal of<br />
a Non-Executive Director requires the approval of threequarters<br />
of members of the Council of Governors. Details<br />
of disqualification from holding office of a director can be<br />
found in the Constitution.<br />
The executive directors hold permanent NHS contracts<br />
subject to NHS terms <strong>and</strong> conditions <strong>and</strong> are appointed by<br />
a Nominations Committee.<br />
Balance of Board membership & independence<br />
The Board of Directors is satisfied that its balance of<br />
knowledge, skills, <strong>and</strong> experience is appropriate to the<br />
Board <strong>and</strong> its sub-committees. The Board collectively<br />
considers that it is appropriately composed in order to fulfill<br />
its function <strong>and</strong> remain within its Terms of Authorisation.<br />
Non-executive directors meet the independence criteria laid<br />
down within the Code.<br />
Performance evaluation<br />
The annual appraisal of the Chairman involves collaboration<br />
between the Senior Independent Director <strong>and</strong> the Vice<br />
Chairman of the Council of Governors to seek the views<br />
of both Executive Directors <strong>and</strong> Governors. Executive<br />
Directors have an annual appraisal with the Chief Executive.<br />
The performance of Non-Executive Directors is evaluated<br />
annually by the Chairman. Overall Board performance is<br />
also evaluated.<br />
During the year the Board conducted a review of its<br />
committees <strong>and</strong> confirmed that each committee is fit for<br />
purpose <strong>and</strong> functions effectively.<br />
Board meetings<br />
The Board meets regularly, on average once a month.<br />
Special meetings are convened as <strong>and</strong> when required.<br />
There were 11 ordinary meetings during <strong>2011</strong>/<strong>12</strong>.<br />
Attendance at Board of Directors’ meetings<br />
Brief details of each Board members’ record of attendance<br />
at Board meetings are shown below.<br />
Non-Executive Directors<br />
Meetings<br />
Michael Cassidy 11/11<br />
Stephen Hay 10/11<br />
Prof. Michael Keith 9/11<br />
Prof. Chris Griffiths 9/11<br />
Imelda Redmond 10/11<br />
David Stewart 10/11<br />
Sir John Gieve* 4/5<br />
Eric Sorensen** 6/6<br />
*appointed from November <strong>2011</strong><br />
**retired from the Trust in October <strong>2011</strong><br />
22 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Executive Directors<br />
Meetings<br />
Nancy Hallett, Chief Executive 11/11<br />
John Coakley, Medical Director 10/11<br />
Tracey Fletcher, Chief Operating Officer 10/11<br />
Charlie Sheldon, Chief Nurse & Director<br />
of Governance<br />
11/11<br />
Jo Farrar, Director of Finance 10/11<br />
Cheryl Clements, Director of Workforce<br />
<strong>and</strong> Education<br />
5/11*<br />
Andrew Panniker, Director of Environment** 6/6<br />
*period of sickness absence<br />
**finished working for the Trust in October <strong>2011</strong><br />
Members of the Board of Directors<br />
Non-Executive Directors<br />
Michael Cassidy CBE, Chairman<br />
Mr Cassidy has held the post of Chairman since December<br />
2006. He was appointed by the Council of Governors<br />
to serve for a further three year term in 2009, which<br />
completes in 20<strong>12</strong>. Mr Cassidy has been a City lawyer<br />
for 35 years. In addition, he has served on the Board of<br />
quoted property companies <strong>and</strong> UBS limited. Mr Cassidy<br />
is the chair of the Museum of London. Mr Cassidy chairs<br />
the Remuneration Committee. He is a member of the Risk<br />
Committee <strong>and</strong> also sits on the Trust’s Charitable Funds<br />
Committee.<br />
Stephen Hay, Senior Independent Director <strong>and</strong><br />
Deputy Chair<br />
Mr Hay was re-appointed by the Council of Governors<br />
to serve for a second three year term in 2009, which<br />
completes in 20<strong>12</strong>. He is a self-employed management<br />
consultant <strong>and</strong> prior to this he was a managing director at<br />
Goldman Sachs. Mr Hay chairs the Audit Committee.<br />
Professor Michael Keith<br />
Professor Keith was re-appointed by the Council of<br />
Governors to serve for a second three year term in 2010,<br />
which completes in 2013. He is Professor of Anthropology<br />
at Merton College Oxford having previously been Professor<br />
<strong>and</strong> Director for the Centre for Urban <strong>and</strong> Community<br />
Research at Goldsmith’s, <strong>University</strong> of London. He was<br />
previously leader of the London Borough of Tower<br />
Hamlets. Professor Keith is a member of the Audit <strong>and</strong> Risk<br />
Committees.<br />
Imelda Redmond CBE<br />
Ms Redmond was re-appointed by the Council of<br />
Governors to serve for a second three year term in <strong>2011</strong>,<br />
which completes in 2014. She was the Chief Executive of<br />
Carers UK from 2003 to <strong>2011</strong>. She is now the Director<br />
of Policy <strong>and</strong> Public Affairs at Marie Curie Care. She was<br />
awarded a CBE in 2010 for services to disadvantaged<br />
people. Ms Redmond is a member of the Audit Committee.<br />
Professor Chris Griffiths<br />
Professor Griffiths was re-appointed by the Council of<br />
Governors to serve for a second three year term in <strong>2011</strong>,<br />
which completes in 2014. He is a Professor of General<br />
Practice at Queen Mary College, <strong>University</strong> of London.<br />
Professor Griffiths is also a General Practitioner. Professor<br />
Griffiths is a member of the Infection Prevention <strong>and</strong><br />
Control Committee.<br />
David Stewart<br />
Mr Stewart was re-appointed by the Council of<br />
Governors to serve for a second three year term in<br />
<strong>2011</strong>, which completes in 2014. He is a fellow of the<br />
Institute of Chartered Accounts <strong>and</strong> a fellow of the<br />
Institute of Directors <strong>and</strong> was the Partner in charge of<br />
the Central London office of Coopers <strong>and</strong> Lybr<strong>and</strong> (now<br />
PricewaterhouseCoopers). Mr Stewart is a member of the<br />
Finance Committee <strong>and</strong> chairs the Risk Committee.<br />
Sir John Gieve<br />
Sir John Gieve was appointed by the Council of Governors<br />
in <strong>2011</strong>. He currently holds a number of chairman <strong>and</strong><br />
directorships for a range of private <strong>and</strong> third sector<br />
organisations including Chair of the Clore Social Leadership<br />
Programme. Sir John chairs the Finance <strong>and</strong> Performance<br />
Committee.<br />
Eric Sorensen<br />
Mr Sorensen was re-appointed by the Council of Governors<br />
to serve for a second <strong>and</strong> final three year term in 2008,<br />
which completed in October <strong>2011</strong>.<br />
Executive Directors<br />
Nancy Hallett, Chief Executive<br />
Ms Hallett has been Chief Executive since 1999. She joined<br />
the Trust in 1993 as director of nursing <strong>and</strong> patient services,<br />
<strong>and</strong> later became the director of service development.<br />
She was awarded an OBE in 2004 for services to health<br />
in Hackney. Ms Hallett sits on the Charitable Funds<br />
Committee, Risk Committee <strong>and</strong> Finance <strong>and</strong> Performance<br />
Committee.<br />
Dr John Coakley, Medical Director, Joint Deputy Chief<br />
Executive<br />
Dr Coakley has been an Intensive Care consultant at<br />
<strong>Homerton</strong> since 1992. He became Medical Director of<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 23
GOVERNANCE REPORT<br />
<strong>Homerton</strong> in 1998, having previously been Director of<br />
Postgraduate Medical Education. Dr Coakley sits on the<br />
Charitable Funds <strong>and</strong> Risk Committees.<br />
Tracey Fletcher, Chief Operating Officer, Joint Deputy<br />
Chief Executive<br />
Ms Fletcher re-joined the trust in 2010 as Chief Operating<br />
Officer, having previously been with <strong>Homerton</strong> <strong>Hospital</strong> for<br />
many years. She has extensive experience in health care<br />
management. Ms Fletcher holds the post of joint deputy<br />
Chief Executive Officer. Ms Fletcher sits on the Finance <strong>and</strong><br />
Performance Committee.<br />
Charlie Sheldon, Chief Nurse & Director Governance<br />
Mr Sheldon joined the Trust in June 2010. A Registered<br />
General Nurse, he was previously Chief Nurse at the Royal<br />
National Orthopaedic <strong>Hospital</strong> NHS Trust. He is an Honorary<br />
Visiting Professor, City <strong>University</strong>. Mr Sheldon sits on the<br />
Infection Control <strong>and</strong> the Risk Committees.<br />
Jo Farrar, Director of Finance<br />
Mr Farrar joined the Trust in March 2010. He previously<br />
worked as acting Chief Executive of NHS London’s Provider<br />
Agency, <strong>and</strong> Head of Compliance at Monitor. Mr Farrar<br />
trained as a chartered accountant at KPMG. Mr Farrar<br />
chairs the Charitable Funds Committee <strong>and</strong> is a member of<br />
the Finance & Performance <strong>and</strong> Risk Committees.<br />
Cheryl Clements, Director of Workforce<br />
Mrs Clements joined the Trust in June 2009. Mrs Clements<br />
left the Trust in April 20<strong>12</strong>.<br />
Andrew Panniker, Director of Environment<br />
Mr Panniker joined the Trust in 2002. Mr Panniker left the<br />
Trust in October <strong>2011</strong>.<br />
Register of Directors’ interests<br />
Some of our Directors hold interests that may be relevant or<br />
material to NHS business matters. All directors declare those<br />
interests in the Register of Directors’ Interests. The register is<br />
available for inspection by members of the public. Anyone<br />
who wishes to see the register of directors’ interest should<br />
make enquiries to the Foundation Trust Secretary on<br />
020 8510 7321. There have not been any material<br />
relationships that have influenced individual director’s roles.<br />
Audit Committee<br />
Membership <strong>and</strong> attendance<br />
The Audit Committee is chaired by Stephen Hay, a Non-<br />
Executive Director, <strong>and</strong> includes three other Non-Executive<br />
Directors – Imelda Redmond, Eric Sorensen (until October<br />
<strong>2011</strong>) <strong>and</strong> Prof Michael Keith. It met four times in <strong>2011</strong>/<strong>12</strong><br />
Title<br />
Attendance at meetings<br />
Stephen Hay NED (Chair) 4/4<br />
Imelda Redmond 3/4<br />
Eric Sorensen* 2/2<br />
Michael Keith 2/4<br />
*retired from the Trust in October <strong>2011</strong><br />
How the Audit Committee discharges its<br />
responsibilities<br />
The Audit Committee’s primary purpose is to conclude<br />
upon the adequacy <strong>and</strong> effective operation of the Trust’s<br />
overall system of control. It is directly accountable to the<br />
Board. The Committee assures the Board of Directors that<br />
probity <strong>and</strong> professional judgement are exercised in all<br />
financial matters. It advises the Board on the adequacy of<br />
the Trust’s system of internal control <strong>and</strong> its processes for<br />
securing economy, efficiency <strong>and</strong> effectiveness.<br />
Auditors<br />
The external auditors for <strong>Homerton</strong> are Deloitte LLP,<br />
appointed by the Council of Governors in July <strong>2011</strong>.<br />
Their fees for audit services undertaken in <strong>2011</strong>/<strong>12</strong> were<br />
£79,000. Deloitte’s accompanying <strong>report</strong> on our financial<br />
statements is based on their audit conducted in accordance<br />
with International Financial Reporting St<strong>and</strong>ards <strong>and</strong> the<br />
Financial Reporting Manual issued by Monitor. Their work<br />
includes a review of our system of internal control which<br />
is used to inform the nature <strong>and</strong> scope of their audit<br />
procedures.<br />
The Trust’s external auditors may perform non-audit<br />
work where the work is clearly audit related <strong>and</strong> the<br />
external auditors are best placed to do that work. For such<br />
assignments the Audit Committee approved protocol<br />
is followed which ensures all such work is properly<br />
considered. The processes in place ensure auditor objectivity<br />
<strong>and</strong> independence is safeguarded.<br />
As far as the Directors are aware, there is no information<br />
relevant to the audit which has not been disclosed to<br />
the auditors. The Directors have taken all the steps that<br />
they ought to have taken as a director in order to make<br />
themselves aware of any relevant audit information <strong>and</strong> to<br />
establish that the NHS Foundation Trust’s auditor is aware<br />
of that information.<br />
Risk Committee<br />
The Risk Committee is constituted as a st<strong>and</strong>ing committee<br />
of the Board of Directors <strong>and</strong> monitors all aspects of clinical<br />
<strong>and</strong> non-clinical risk. The purpose of the committee is to<br />
ensure that all risks are identified, assessed <strong>and</strong> evaluated<br />
according to the risk management framework. The<br />
24 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
committee seeks assurance that all risks are being managed<br />
effectively <strong>and</strong>, where necessary, directs what action is<br />
required to mitigate risk or to gain further assurance. The<br />
Committee is chaired by David Stewart, a Non-Executive<br />
Director, <strong>and</strong> its membership also includes Michael Cassidy,<br />
Chairman <strong>and</strong> Prof Michael Keith, Non-Executive Directors.<br />
It met four times in <strong>2011</strong>/<strong>12</strong>.<br />
Nominations Committee of the Council of Governors<br />
The Nominations Committee of the Council of Governors<br />
comprises public <strong>and</strong> staff Governors <strong>and</strong> is chaired by the<br />
Trust Chairman. Its purpose is to select the non-executive<br />
directors. In the case of recruiting a new chairman, the<br />
senior independent director replaces the current chairman<br />
for interview purposes. The committee selects a c<strong>and</strong>idate<br />
who is appointed by the Council of Governors.<br />
There were three meetings of the Nominations Committee<br />
of the Council of Governors in <strong>2011</strong>/<strong>12</strong> which met to<br />
reappoint three Non-Executive Directors for second three<br />
year terms <strong>and</strong> to appoint two new Non-Executive Directors<br />
to replace outgoing Non-Executive Directors.<br />
Nominations Committee of the Board of Directors<br />
The Nominations Committee of the Board of Directors<br />
comprises members of the Board of Directors <strong>and</strong> is<br />
chaired by the Trust Chairman. This committee appoints<br />
the chief executive <strong>and</strong> executive directors of the Trust. The<br />
committee meets annually to review the board structure,<br />
size <strong>and</strong> composition, <strong>and</strong> to give consideration to<br />
succession planning <strong>and</strong> identify the skills <strong>and</strong> knowledge<br />
of the Board. The committee must also meet as part of the<br />
process of appointment for executive directors.<br />
The Nominations Committee of the Board of Directors met<br />
once in <strong>2011</strong>/<strong>12</strong> to review the Board structure <strong>and</strong> consider<br />
the reappointment process for the Chief Executive Officer.<br />
Both Nominations Committees work to common principles<br />
<strong>and</strong> share similar procedures.<br />
Remuneration <strong>report</strong><br />
For the purposes of this <strong>report</strong> the disclosure of<br />
remuneration to senior managers is limited to executive <strong>and</strong><br />
non-executive directors of the Trust.<br />
In accordance with the constitution the remuneration<br />
of the executive directors is determined by the Executive<br />
Director Remuneration Committee comprising the<br />
Chairman <strong>and</strong> Non-Executive Directors. The remuneration<br />
of the Chairman <strong>and</strong> Non-Executive directors is determined<br />
by the Non Executive Remuneration Committee of the<br />
Council of Governors.<br />
Both committees work to common principles <strong>and</strong><br />
procedures. Remuneration levels are set taking into account<br />
the requirements of the role, market rates, the performance<br />
of the Trust, internal comparability <strong>and</strong> affordability. No<br />
individual is involved in any decision that affects his or her<br />
own remuneration. Both committees adopt the principles<br />
of good governance in setting remuneration, <strong>and</strong> take into<br />
account a wide range of pay guidance across other public<br />
sector <strong>and</strong> relevant independent organisations to inform<br />
the process.<br />
The Executive Director Remuneration Committee advises<br />
on any major changes in employee benefit structure in the<br />
Trust <strong>and</strong> ensures that contractual terms on termination<br />
<strong>and</strong> any payments made are fair to the individual <strong>and</strong> the<br />
organisation. Both committees are authorised to obtain<br />
external or other professional advice on any matters within<br />
their terms of reference, with due regard to probity <strong>and</strong><br />
cost. Both committees consider board performance <strong>and</strong><br />
individual performance as part of the remuneration review.<br />
The Trust does not award performance bonuses.<br />
Executive Directors are required to give six month’s notice<br />
to terminate their employment contracts. Non-Executive<br />
Directors are required to provide one month’s notice.<br />
All directors have permanent contracts. Non-Executive<br />
Directors are appointed for a period of three years in<br />
accordance with the Constitution.<br />
The Trust currently carries a provision of £687k for early<br />
retirements relating to ex-members of staff.<br />
The Remuneration Committee of the Council of Governors<br />
met once in <strong>2011</strong>/<strong>12</strong> to consider Non- Executive<br />
remuneration. No pay inflation award was given to Non-<br />
Executive Directors.<br />
The Remuneration Committee of the Board of Directors<br />
met twice in <strong>2011</strong>/<strong>12</strong>. The Chairman <strong>and</strong> all six Non-<br />
Executive Directors were in attendance. The meetings were<br />
also part attended by the Chief Executive <strong>and</strong> Director of<br />
Workforce <strong>and</strong> Education for the purpose of providing<br />
advice or services to the committee that materially assisted<br />
the committee with the matters before them. No pay<br />
inflation award was given to Executive Directors.<br />
Salary <strong>and</strong> pension entitlements of senior managers are<br />
available in the Accounts. Page 105<br />
Nancy Hallett<br />
Chief Executive<br />
30 May 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 25
GOVERNANCE REPORT<br />
The Council of Governors<br />
How the Board of Directors <strong>and</strong> the Council of<br />
Governors operate<br />
The Council of Governors represents the interests of the<br />
local community defined as public <strong>and</strong> staff who are<br />
Foundation Trust members, <strong>and</strong> shares information about<br />
key decisions with membership.<br />
There are 26 Governors under the leadership of the Trust<br />
Chairman including:<br />
• 14 Public (elected) -10 representing Hackney, 2<br />
representing the City of London <strong>and</strong> 2 representing<br />
adjoining boroughs<br />
• 6 Staff (elected) - 4 representing clinical staff <strong>and</strong> 2<br />
representing non-clinical staff<br />
• 6 Partnership Governors (appointed) - nominated from 5<br />
partnership organisations.<br />
The Governors act as a link between the Board of Directors<br />
<strong>and</strong> the membership. The opinion of the Council of<br />
Governors is sought by the Board of Directors on key<br />
strategic issues. The Council of Governors is invited to<br />
review issues of importance at its meetings <strong>and</strong> advise the<br />
Chairman of their views. The Chairman ensures that these<br />
views are considered at the Board of Directors meeting as<br />
part of the decision-making process.<br />
During the year, a Guidebook for new Governors was<br />
published providing information about the Trust <strong>and</strong><br />
Governor responsibilities.<br />
The Council of Governors <strong>and</strong> the Board of Directors<br />
meet jointly twice a year. The agendas developed for<br />
those meetings reflect the issues both parties need to<br />
discuss. In particular the joint meeting enables board<br />
members to underst<strong>and</strong> the views of the Governors <strong>and</strong><br />
members. Executive directors regularly attend Council of<br />
Governors meetings to gain an underst<strong>and</strong>ing of the views<br />
of Governors <strong>and</strong> the membership constituencies they<br />
represent. The Governors held six meetings in <strong>2011</strong>/<strong>12</strong><br />
including two joint meetings of the Council of Governors<br />
<strong>and</strong> the Board of Directors, <strong>and</strong> the <strong>Annual</strong> Members’<br />
meeting. The Trust constitution requires the Council of<br />
Governors to meet at least three times a year.<br />
The following table summarises the record of Governor<br />
attendance at Council of Governors’ meetings.<br />
Name Constituency Date elected or appointed Attendance*<br />
Michael Cassidy Chairman N/A 5/6<br />
Clyde Baker Public (Hackney) Sept 2010 (1st term) 5/6<br />
Eli Kernkraut Public (Hackney) Sept <strong>2011</strong> (1st term) 3/3<br />
Patricia Bennett Public (Hackney) Sept 2010 (1st term) 3/6<br />
Suri Friedman Public (Hackney) Sept 2010 (2nd term) 6/6<br />
Talaat Qureshi (1 year) Public (Hackney) Sept <strong>2011</strong> (1st term) 3/3<br />
Jude Williams Public (Hackney) Sept <strong>2011</strong> (1st term) 3/3<br />
Jamie Bishop Public (Hackney) Sept 2009 (1st term) 6/6<br />
Florence Osaigbovo Public (Hackney) Sept 2009 (2nd term) 4/6<br />
Christopher Sills (1 year) Public (Hackney) Sept <strong>2011</strong> (1st term) 5/5<br />
Sarah Weiss (2 year) Public (Hackney) Sept <strong>2011</strong> (3rd term) 6/6<br />
Doug Hiza Public (Hackney) Sept 2008 (1st term) 3/3<br />
Sarah Horsfield Public (Hackney) Sept 2010 (1st term) 2/2<br />
John Bootes Public (City) Mar 2010 (1st term) 5/6<br />
Geoffrey Rivett** Public (City) Sept 2010 (3rd term) 6/6<br />
Fatmata Sesay Public (Outer) Sept <strong>2011</strong> (1st term) 2/3<br />
Eric Sorensen Public (Outer) Sept <strong>2011</strong> (1st term) 1/2<br />
Dr Katherine Coyne Staff (Clinical) Sept <strong>2011</strong> (1st term) 2/3<br />
Val Dimmock Staff (Clinical) Sept 2010 (1st term) 2/6<br />
Mr Andrew Ezsias Staff (Clinical) Sept <strong>2011</strong> (1st term) 2/3<br />
Ros Constable Staff (Clinical) Sept <strong>2011</strong> (1st term) 2/3<br />
26 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Name Constituency Date elected or appointed Attendance*<br />
Dr Helen Cugnoni Staff (Clinical) Aug 2008 (1st term) 1/3<br />
Dr Paul Cannon Staff (Clinical) Mar 2010 (2nd term) 1/1<br />
Henry Muss Staff (Non Clinical) Sept <strong>2011</strong> (1st term) 1/3<br />
Robert Duke Staff (Non Clinical) Mar 2010 (1st term) 6/6<br />
Jonathon McShane Hackney Council Appointed Oct <strong>2011</strong> 0/3<br />
Deborah James Queen Mary Westfield Appointed Feb 2010 2/6<br />
Gareth Moore City of London Appointed Jul 2009 1/6<br />
Dr Lesley Mountford East London <strong>and</strong> City Appointed 2004 4/6<br />
Prof. Stan Newman City <strong>University</strong> Appointed Jan <strong>2011</strong> 1/6<br />
*If individuals joined or left the Council of Governors during the<br />
financial year, the number of meetings they could attend has been<br />
adjusted accordingly. A total of six meetings including two joint<br />
meetings of the Council of Governors <strong>and</strong> Board of Directors were<br />
held in <strong>2011</strong>/<strong>12</strong><br />
**Nominated lead Governor<br />
A register of interests is maintained in relation to the<br />
Governors. This is available for viewing from the Trust<br />
Offices.<br />
If there is a dispute between the Council of Governors <strong>and</strong><br />
Board of Directors, the Chairman, in the first instance, will<br />
endeavour to resolve it. If the Chairman cannot resolve it,<br />
the Senior Independent Director <strong>and</strong> the Vice Chairman<br />
of the Council of Governors will together attempt to<br />
resolve the issue. Should the Senior Independent Director<br />
<strong>and</strong> the Vice Chairman of the Council of Governors fail<br />
to resolve the conflict, the Board of Directors, pursuant<br />
to section15(2) of Schedule 7 of the Act, will decide the<br />
disputed matter.<br />
Public <strong>and</strong> staff Governors are elected by the membership.<br />
Elections are held in accordance with the election rules,<br />
as stated in the Constitution, using a single transferable<br />
vote system. Elections for vacancies in four constituencies<br />
(Hackney, outer, Staff (non-clinical) <strong>and</strong> Staff (clinical)) were<br />
held this year to replace those Governors who had resigned<br />
or completed their term of office in accordance with the<br />
transition schedule. The elections were administered on<br />
behalf of the Trust by Electoral Reform Services Limited.<br />
Foundation Trust membership<br />
The Trust embraces the concept of a wide membership<br />
base. There is no set limit on the number of people who<br />
can register as members within the eligibility criteria.<br />
Patient Experience <strong>and</strong> Engagement Committee will be<br />
overseeing the recruitment <strong>and</strong> involvement of members<br />
through the Membership Development Strategy. Previously<br />
membership development activities were <strong>report</strong>ed to <strong>and</strong><br />
monitored by the Patient <strong>and</strong> Public Involvement <strong>and</strong><br />
Membership Development Group.<br />
The overall public <strong>and</strong> staff membership has increased over<br />
the past year with 640 new members recruited <strong>and</strong> 254<br />
members leaving.<br />
At year start<br />
(April 1 <strong>2011</strong>)<br />
New<br />
members<br />
Members<br />
leaving<br />
Public 4467 277 88 4656<br />
Staff 2024 363 166 2221<br />
Total 6491 640 254 6877<br />
At year end<br />
(March<br />
31 20<strong>12</strong>)<br />
The public constituencies – Hackney, City <strong>and</strong> Outer – are<br />
broadly representative of the areas from which the majority<br />
of patients come to <strong>Homerton</strong>.<br />
Membership is open to any member of the public over the<br />
age of 16 who lives in the London Borough of Hackney, the<br />
City of London or the outer area. The outer constituency<br />
includes Tower Hamlets, Waltham Forest, Newham,<br />
Redbridge, Barking, Havering, Camden, Islington, Haringey,<br />
Enfield, Lambeth, Southwark, Westminster <strong>and</strong> Epping<br />
Forest District. There is no separate patient constituency.<br />
Active membership is highest within the London Borough<br />
of Hackney. The staff constituency is divided into clinical<br />
<strong>and</strong> non-clinical staff categories. Any staff on permanent<br />
employment contracts or those who have worked at the<br />
Trust for at least <strong>12</strong> months, including contractual staff or<br />
those holding honorary contracts, are eligible to join.<br />
A representative membership<br />
Our membership strategy for 20<strong>12</strong>-2014 outlines our<br />
vision for a representative <strong>and</strong> engaged membership. The<br />
following four key objectives are set out:<br />
• to increase the overall number of members who are<br />
representative of our patients <strong>and</strong> local community<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 27
GOVERNANCE REPORT<br />
• to strive for the composition of membership to reflect<br />
the diversity of the local community with a focus on<br />
recruiting young people <strong>and</strong> people with disabilities<br />
• to engage the local community through health <strong>and</strong><br />
social care events, <strong>and</strong><br />
• to ensure members receive appropriate communications<br />
to improve their underst<strong>and</strong>ing of the services<br />
delivered by the Trust <strong>and</strong> its relationship with the local<br />
community.<br />
The public membership continues to be largely<br />
representative of the local population in terms of ethnicity<br />
<strong>and</strong> gender. The Hackney 2001 Census data has been used<br />
for comparison of the local population, as the majority of<br />
Trust’s patients live in the borough with the majority of<br />
public members in the Hackney constituency. The <strong>2011</strong><br />
Census data will be used when it becomes available later<br />
this year.<br />
The Trust is able to closely monitor its membership through<br />
the membership database using the information supplied<br />
by the members on their application forms. The application<br />
form is available online via the Trust website <strong>and</strong> at public<br />
areas across the Trust. Ongoing analysis <strong>and</strong> review of<br />
membership enables the Trust to undertake detailed<br />
demographic analysis of the membership, <strong>and</strong> identify<br />
where gaps exist in recruitment.<br />
In <strong>2011</strong>/<strong>12</strong> three Memberlink newsletters were sent to all<br />
public members providing information <strong>and</strong> news about the<br />
Trust’s services.<br />
Get in touch<br />
If a member of the public wishes to contact a governor<br />
they can do so via members@homerton.nhs.uk or by<br />
phoning the Trust Offices on 020 8510 5221. A member of<br />
the team will then put the query through to a Governor.<br />
28 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 29
30 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Quality Account<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 31
32 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Quality Account<br />
Contents<br />
Section 1:<br />
Chief Executive’s statement 34<br />
Section 2:<br />
Priorities for improvement 35<br />
Section 3:<br />
<strong>Homerton</strong> acute <strong>and</strong> community services <strong>2011</strong>/<strong>12</strong> 38<br />
Section 4:<br />
Quality improvements <strong>2011</strong>/<strong>12</strong> 50<br />
Section 5:<br />
Quality improvement plans 20<strong>12</strong>/13 70<br />
Section 6:<br />
Consultation <strong>and</strong> feedback 73<br />
Section 7:<br />
Statement of Directors’ responsibilities 77<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 33
QUALITY ACCOUNT<br />
Quality Account <strong>2011</strong>/<strong>12</strong><br />
SECTION 1 – Chief Executive’s Statement<br />
Introduction <strong>and</strong> welcome<br />
I am pleased to present our Quality Account for <strong>2011</strong>/<br />
<strong>12</strong>, our first as a combined acute <strong>and</strong> community NHS<br />
Foundation Trust. The safety <strong>and</strong> quality of the care we<br />
provide to patients has to be the number one priority for<br />
our Board, staff <strong>and</strong> Governors.<br />
In this document we <strong>report</strong> on the work undertaken to<br />
maintain <strong>and</strong> improve the quality of care we provide <strong>and</strong><br />
set out related plans for the year ahead. It is prepared in<br />
line with the requirements set out in the Quality Accounts<br />
legislation (part of the Health Act 2009) <strong>and</strong> Monitors<br />
annual <strong>report</strong>ing guidance.<br />
The information presented in the Quality Account is<br />
accurate <strong>and</strong> true to the best of my knowledge.<br />
That said, there is of course plenty of room for<br />
improvement. We have made the decision to join the<br />
NHS QUEST programme. This is a quality benchmarking<br />
programme open to foundation trusts with a strong track<br />
record in quality improvement <strong>and</strong> an ambition to be in the<br />
best.<br />
20<strong>12</strong>/13<br />
In terms of our quality programme for 20<strong>12</strong>/13 much is<br />
determined by national requirements or those set by the<br />
commissioners of health services. These are the must-dos<br />
for any NHS trust. Our Quality Account objectives challenge<br />
us to go beyond our must-dos. These are now set before<br />
you. In compiling these we have taken into account many<br />
factors but importantly we have linked them more closely<br />
than we have done in other years to the Trust’s corporate<br />
objectives <strong>and</strong> to the opportunities that we believe the<br />
QUEST programme will bring.<br />
<strong>2011</strong>/<strong>12</strong><br />
Measuring <strong>and</strong> assessing for quality <strong>and</strong> safety in health<br />
care is not straightforward. There is no one measure that<br />
can tell us precisely where we are. We have to use a range<br />
of measures, interpret the findings with care <strong>and</strong> challenge<br />
ourselves to keep testing the evidence.<br />
When I say now that in <strong>2011</strong>/<strong>12</strong> we saw some very positive<br />
indicators of safety <strong>and</strong> quality at <strong>Homerton</strong> I do so in the<br />
light of the statement above. I have however highlighted<br />
below two measures from our basket where we did<br />
particularly well because I believe they are important.<br />
In the entire year we had not one case of MRSA<br />
bacteraemia (blood infection). The importance of this is<br />
that, taken in conjunction with other findings, it shows that<br />
st<strong>and</strong>ards of infection control in the hospital are high.<br />
The other area is external inspection. These are increasing<br />
in their intensity, with the Care Quality Commission (CQC)<br />
undertaking unannounced inspections to all hospitals,<br />
care homes <strong>and</strong> health centres. Since May <strong>2011</strong>, both<br />
the main <strong>Homerton</strong> <strong>Hospital</strong> <strong>and</strong> our care home, Mary<br />
Seacole received visits, with no prior warning. For our<br />
community services we participated in a combined Ofsted/<br />
CQC inspection of children’s safeguarding services. These<br />
were not ‘spot checks’; there were many assessors over a<br />
number of days. We were found to be meeting the CQC<br />
st<strong>and</strong>ards.<br />
Nancy Hallett<br />
Chief Executive<br />
34 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
SECTION 2 – Priorities for improvement<br />
In this section we look at our quality improvement priorities<br />
for hospital <strong>and</strong> community health services <strong>and</strong> for our<br />
teaching <strong>and</strong> research activities.<br />
It is important to us that we set priorities for the coming<br />
year in consultation with our partners in care. We consulted<br />
between December <strong>2011</strong> <strong>and</strong> February 20<strong>12</strong> with;<br />
patients, staff, Members, Governors, commissioners, NHS<br />
London, LINks <strong>and</strong> overview <strong>and</strong> scrutiny committees of<br />
Hackney <strong>and</strong> the City of London to determine quality<br />
priorities.<br />
Information from the consultation was fed back to the<br />
Trust Board with the recommendation of retaining two<br />
of our existing quality improvement priorities, retire two<br />
<strong>and</strong> add four new. These priorities are all linked to the<br />
Trust’s strategic objectives <strong>and</strong> the work of the QUEST<br />
programme.<br />
Trust strategic objectives<br />
The Trust strategic objectives for the coming year are;<br />
Our core objective:<br />
We exist to provide safe, effective, thoughtful NHS health<br />
care. In order to be allowed to continue to do this we must<br />
meet legislative <strong>and</strong> regulatory requirements.<br />
Departments need to underst<strong>and</strong> what specifically<br />
this means for them, but to some extent it can be<br />
encapsulated as follows: maintain compliance with<br />
CQC essential st<strong>and</strong>ards <strong>and</strong> those of related agencies;<br />
maintain compliance with Monitor’s financial <strong>and</strong><br />
governance requirements; comply with legislation relating<br />
to fire, carbon reduction, equalities etc; achieve national<br />
requirements for service, teaching <strong>and</strong> research.<br />
In addition, a must-do for us is to fulfil the requirements of<br />
our 20<strong>12</strong> Olympic Games contract.<br />
Aspire to do<br />
We aspire to do the following because we believe they are<br />
important to our future <strong>and</strong> we will focus time <strong>and</strong> energy<br />
on them.<br />
i. Quality <strong>and</strong> safety for patients<br />
To provide the public with confidence that <strong>Homerton</strong><br />
is a very safe hospital by maintaining hospital mortality<br />
markers at a level which demonstrates this to be the<br />
case, <strong>and</strong> to provide evidence that all of our services<br />
have the hallmarks of quality <strong>and</strong> safety.<br />
ii. Exp<strong>and</strong>ing the organisation<br />
To grow the organisation, through a planned<br />
<strong>and</strong> strategic approach to increasing referrals <strong>and</strong><br />
establishing new services, so that we are confident we<br />
are the right size for the future.<br />
iii. Community/hospital integration<br />
To be an exemplar organisation for community health<br />
<strong>and</strong> hospital services integration, by fulfilling our<br />
integration programme <strong>and</strong> associated informatics<br />
<strong>and</strong> premises plans. This will support us to retain the<br />
contract for the provision of community services for<br />
Hackney <strong>and</strong> the City beyond 2014.<br />
iv. Short waits<br />
To be a ‘short-wait’ organisation, with all patients<br />
being offered an appointment for a consultation or<br />
investigation within four weeks of referral. Patients for<br />
urgent consultations will continue to wait no more than<br />
two weeks <strong>and</strong> those presenting to the emergency<br />
department attended to within four hours.<br />
v. Communications with patients, GPs <strong>and</strong><br />
professionals<br />
To be exemplary in our engagement with patients,<br />
GPs <strong>and</strong> key professionals in relation to every<br />
interaction with our services; ensuring consultation <strong>and</strong><br />
investigation <strong>report</strong>s are conveyed to patient, GP <strong>and</strong><br />
professionals within five working days; summaries from<br />
inpatient stays <strong>and</strong> emergency attendances within 24<br />
hours.<br />
vi. Preparing <strong>and</strong> supporting staff<br />
To prepare staff for <strong>Homerton</strong> of the future by ensuring<br />
everyone is clear on their contribution to making<br />
this organisation <strong>and</strong> their service better, through<br />
programmes which develop service line management,<br />
clinical leaders <strong>and</strong> the ability of staff to achieve the<br />
Trust’s objectives.<br />
NHS QUEST<br />
NHS QUEST is an organisation of 14 foundation trusts in<br />
Engl<strong>and</strong> who work together to innovate <strong>and</strong> share learning<br />
to improve quality.<br />
QUEST members work as partners on improvement<br />
projects, e.g. Harm-Free Care, Reducing Readmissions, <strong>and</strong><br />
Reducing Mortality. Members learn together <strong>and</strong> from one<br />
another, consistently measure <strong>and</strong> <strong>report</strong> improvement <strong>and</strong><br />
together, galvanise collective leadership <strong>and</strong> staff capability.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 35
QUALITY ACCOUNT<br />
Foundation trusts who are members of NHS QUEST focus<br />
on the following:<br />
• improving quality <strong>and</strong> safety<br />
• aspire to a level of excellence beyond all current<br />
expectations<br />
• build the capability of our workforce to improve<br />
• support our leaders to create the right culture for<br />
reliability<br />
• measure <strong>and</strong> <strong>report</strong> our outcomes<br />
• learn from one another <strong>and</strong> share through actionorientated<br />
projects<br />
• believe we can always do better for our patients.<br />
In the context of the Trust strategic objectives <strong>and</strong><br />
becoming a member of NHS QUEST, <strong>Homerton</strong> sets out its<br />
quality priorities for the year ahead below.<br />
Priorities for quality improvement for the<br />
coming year April 20<strong>12</strong> to end March 2013:<br />
SAFE<br />
Priority 1<br />
Reduce harm to patients caused by pressure ulcers,<br />
falls, urinary catheter infections, <strong>and</strong> venous<br />
thrombo-embolism (VTE) identified within the Safety<br />
Thermometer / Harm Free Care Programme.<br />
(Linked to Trust objective I, the NHS QUEST programme <strong>and</strong><br />
the Patient Experience Strategy Campaign One: Delivering<br />
thoughtful care).<br />
Description of the issue <strong>and</strong> reason for making it a<br />
priority: The use of a tool called the Safety Thermometer<br />
is a National Commissioning for Quality <strong>and</strong> Innovation<br />
(CQUIN) scheme <strong>and</strong> an operating framework requirement.<br />
The four harms to be monitored are:<br />
• pressure ulcers<br />
• slips, trips <strong>and</strong> falls<br />
• patients with a urinary catheter who develop a urinary<br />
tract infection<br />
• venous thrombo-embolism.<br />
Aim<br />
To be fully involved with the safety thermometer<br />
measurement programme <strong>and</strong> to reduce harm, over the<br />
coming year, to acute <strong>and</strong> community patients, from the<br />
four harms listed above.<br />
Priority 2<br />
Demonstrate improvements in safety by continuing<br />
to deliver a programme of work relating to: urgent<br />
care, end of life care <strong>and</strong> clinically led coding, using<br />
the St<strong>and</strong>ardised <strong>Hospital</strong> Mortality Indicator (SHMI)<br />
as a measure.<br />
(Linked to Trust objective I, the NHS QUEST programme <strong>and</strong><br />
the Patient Experience Strategy Campaign One: Delivering<br />
thoughtful care).<br />
Description of the issue <strong>and</strong> reason for making it a<br />
priority: The St<strong>and</strong>ardised <strong>Hospital</strong> Mortality Indicator<br />
(SHMI) compares the expected rate of death in a hospital<br />
with the actual rate of death. The SHMI model removes<br />
palliative care coding <strong>and</strong> focuses on 30 day mortality. The<br />
SHMI is an indicator of the quality of care in a hospital.<br />
Aim<br />
NHS QUEST organisations aim to score a St<strong>and</strong>ardised<br />
<strong>Hospital</strong> Mortality Indicator (SHMI) of 75 or below by<br />
January 2013 by focusing on the following four work<br />
streams:<br />
• moving to a 24 hours a day, seven days a week, 365<br />
days a year service<br />
• reviewing systems for measurement<br />
• reducing harm <strong>and</strong> deterioration<br />
• excellence in end of life care.<br />
This will indicate that we are a safer organisation.<br />
EFFECTIVE<br />
Priority 3<br />
Ensure that, where national clinical guidelines have<br />
been produced by the National Institute for Health<br />
<strong>and</strong> Clinical Excellence (NICE) which are relevant to<br />
the care we provide, we can demonstrate we are<br />
using them in everyday practice.<br />
(Linked to Trust objective I <strong>and</strong> the Patient Experience<br />
Strategy Campaign One: Delivering thoughtful care).<br />
Description of the issue <strong>and</strong> reason for making it a<br />
priority: NICE provides national guidance on promoting<br />
good health <strong>and</strong> preventing <strong>and</strong> treating ill health in<br />
acute <strong>and</strong> community settings. This guidance provides an<br />
important benchmark for any Trust in ensuring effectiveness<br />
of care. We have a responsibility to review their guidance,<br />
see if it applies to what we do at the Trust <strong>and</strong> check<br />
whether our practice meets a similar st<strong>and</strong>ard of care. It is<br />
also vital that we audit our practice against the guidance<br />
to clearly show that over time we are maintaining the high<br />
st<strong>and</strong>ards of care we expect to provide.<br />
36 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Aim<br />
Ensure that the Trust has evidence of the implementation of<br />
NICE clinical guidelines that are relevant to the Trust (acute<br />
<strong>and</strong> community). This will include regular audit of the<br />
guidelines to demonstrate that clinical practice continues to<br />
be of the highest st<strong>and</strong>ard.<br />
Priority 4<br />
Reduce hospital readmissions.<br />
(Linked to Trust objective I, III, IV, V, the NHS QUEST<br />
programme <strong>and</strong> the Patient Experience Strategy<br />
Campaign Two: Leaving or transferring from our care with<br />
confidence).<br />
Description of the issue <strong>and</strong> reason for making it a<br />
priority: The readmission of patients to hospital within<br />
30 days for the same condition, if avoidable, is something<br />
we want to prevent. It is disruptive for the patient <strong>and</strong><br />
requires that we review our discharge planning process <strong>and</strong><br />
our collaborative working with community <strong>and</strong> social care<br />
services.<br />
Aim<br />
Reduce readmission rates within 30 days of discharge by<br />
20% by implementing the QUEST Reducing Readmission<br />
improvement programme.<br />
Review the care of all patients who are readmitted within<br />
30 days to see if this could have been avoided <strong>and</strong> what<br />
actions we can take to improve our processes for the<br />
efficient discharge of all patients.<br />
Priority 6<br />
We will improve the effectiveness of discharge from<br />
our care.<br />
(Linked to the Patient Experience Strategy Campaign two;<br />
Leaving or transferring from our care with confidence).<br />
Description of the issue <strong>and</strong> reason for making it a<br />
priority: We have had feedback from patients <strong>and</strong> their<br />
carers concerning delays they have experienced whilst<br />
being discharged from our care. Leaving hospital to go<br />
home should be a smooth <strong>and</strong> efficient process that<br />
enables patients to depart as soon as they are medically fit<br />
to do so. Being discharged from community care should<br />
also be smooth <strong>and</strong> efficient with patients feeling confident<br />
to manage their ongoing care.<br />
Aim<br />
We will improve the effectiveness <strong>and</strong> timeliness of hospital<br />
discharge. We will review <strong>and</strong> improve the discharge of<br />
patients from community care/support. We will measure<br />
patient satisfaction in relation to; communication, waiting<br />
for medicines/transport, the level of support patients have<br />
<strong>and</strong> whether they feel confident to manage their on going<br />
health.<br />
These six priorities will be <strong>report</strong>ed on in forthcoming<br />
<strong>Annual</strong> Reports.<br />
THOUGHTFUL<br />
Priority 5<br />
Sharing care <strong>and</strong> treatment information with<br />
patients.<br />
(Linked to the Patient Experience Strategy Campaign Three:<br />
Getting the information right).<br />
Description of the issue <strong>and</strong> reason for making it a<br />
priority: We will ensure that every patient receives a copy<br />
of every letter sent to their GP or referring practitioner.<br />
Following feedback from patients <strong>and</strong> carers <strong>and</strong> the aims<br />
of the Health <strong>and</strong> Social care bill, we are keen to ensure<br />
that patients are fully involved with their care. Copies of all<br />
letters sent to other professionals about patients ongoing<br />
treatment <strong>and</strong> care will be shared with the patient.<br />
Aim<br />
For 100% of letters sent to the patient’s GP or referring<br />
practitioner to be copied to the patient concerned.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 37
QUALITY ACCOUNT<br />
SECTION 3 – <strong>Homerton</strong> acute <strong>and</strong><br />
community services <strong>2011</strong>/<strong>12</strong> <strong>and</strong><br />
registration with the Care Quality<br />
Commission<br />
In this section we have provided information about the<br />
services that are currently provided at <strong>Homerton</strong>.<br />
During <strong>2011</strong>/<strong>12</strong> we provided 61 NHS services which are<br />
grouped into three clinical divisions as illustrated in Table 1.<br />
Table 1: <strong>Homerton</strong> Clinical Divisions<br />
Children’s Services, Diagnostics <strong>and</strong> Outpatients<br />
Integrated Medical <strong>and</strong> Rehabilitation Services<br />
Surgery, Women’s <strong>and</strong> Sexual Health Services<br />
Each Clinical Division comprises both acute <strong>and</strong> community<br />
services. Services were reorganised following integration<br />
with Community Health Services in April <strong>2011</strong> <strong>and</strong> these<br />
three Divisions were established in September <strong>2011</strong>.<br />
The Trust has reviewed the data available for the quality<br />
of care in the 61 NHS services. This information has come<br />
from a range of sources including: local <strong>and</strong> national<br />
audits, patient surveys, national targets, locally agreed<br />
performance measures <strong>and</strong> last year’s Commissioning for<br />
Quality <strong>and</strong> Innovation (CQUIN) targets.<br />
The income generated by the NHS services reviewed in<br />
<strong>2011</strong>/<strong>12</strong> represents 100% of the total income generated<br />
from the provision of NHS services by <strong>Homerton</strong> for<br />
<strong>2011</strong>/<strong>12</strong> – this income is divided into two contracts; an<br />
acute <strong>and</strong> a community contract.<br />
Management of quality at service level<br />
Service level quality groups review specific information<br />
including; infection control, <strong>report</strong>s on incidents,<br />
complaints, litigation, implementation of new guidance<br />
relevant to the specialty, progress on audits, positive<br />
feedback from patients.<br />
Specialty groups <strong>report</strong> to the Division which in turn <strong>report</strong><br />
to the Trust’s Quality Improvement Committee. This process<br />
ensures that the three elements of quality are reviewed as<br />
an integral part of everyday working in the Trust.<br />
Information received by the Trust Board<br />
The Trust Board receives monthly information on:<br />
• patient experience <strong>and</strong> quality (the quarterly quality<br />
<strong>report</strong>)<br />
• performance against national targets with plans for<br />
improvement if there are concerns in relation to any<br />
particular targets<br />
• key performance indicators which are a measure of<br />
how well we are providing services to patients including<br />
waiting times for outpatients <strong>and</strong> inpatients <strong>and</strong> the<br />
average length of stay in particular patient groups<br />
• targets for the timely care of patients with known <strong>and</strong><br />
suspected cancer.<br />
Quarterly Quality Report<br />
This <strong>report</strong> produced by the Medical Director <strong>and</strong> Chief<br />
Nurse is a detailed quarterly <strong>report</strong> that provides the Board<br />
with information on:<br />
• patient experience (detail from surveys <strong>and</strong> audits)<br />
• complaints, litigation, incidents <strong>and</strong> PALS (CLIP)<br />
• staff experience<br />
• updates on specific projects (for example work being<br />
done by the falls steering group, safeguarding adults<br />
group)<br />
• serious incidents<br />
• hospital acquired infection rates<br />
• local <strong>and</strong> national audit<br />
• mortality rates<br />
• patient related outcome measures (PROMS).<br />
The <strong>report</strong> includes details of actions that are being taken<br />
to address any areas of concern.<br />
Quality initiatives driven from outside the<br />
Trust<br />
National Audits: <strong>Homerton</strong> involvement in national<br />
audits<br />
During <strong>2011</strong>/<strong>12</strong>, 55 national clinical audits <strong>and</strong> four<br />
confidential enquiries covered NHS services.<br />
Of these, 41 national clinical audits <strong>and</strong> three confidential<br />
enquiries covered services that <strong>Homerton</strong> provides. 14<br />
national clinical audits <strong>and</strong> one confidential enquiry were<br />
not applicable to the Trust (services we did not provide).<br />
During <strong>2011</strong>/<strong>12</strong> <strong>Homerton</strong> participated in 35 (85%) national<br />
clinical audits <strong>and</strong> three (100%) national confidential<br />
enquiries of those it was eligible to participate in.<br />
Six national clinical audits were applicable but no data was<br />
submitted – in five cases, the audits related to; Paediatric<br />
Asthma, Seizure Management, Risk Factors (occupational<br />
health related), Diabetes <strong>and</strong> Childhood Epilepsy Clinical<br />
Audit, the data collection deadline was not met. In one<br />
case the audit is carried out two yearly <strong>and</strong> data will be<br />
collected next year.<br />
38 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
The national clinical audits <strong>and</strong> national confidential<br />
enquiries that <strong>Homerton</strong> participated in <strong>and</strong> for which<br />
data collection was completed during <strong>2011</strong>/<strong>12</strong> are listed in<br />
table 2. This also includes the number of cases submitted<br />
to each audit or enquiry as a percentage of the number<br />
of registered cases required by the terms of that audit or<br />
enquiry:<br />
Table 2 – Audits we took part in <strong>and</strong> the amount of<br />
information we sent in for each audit<br />
Audit title<br />
Percentage of data submitted<br />
Peri- <strong>and</strong> Neonatal<br />
Perinatal mortality 100<br />
Neonatal intensive <strong>and</strong> special care (NNAP) 100<br />
Paediatrics<br />
Paediatric pneumonia 100<br />
Pain management 100<br />
Childhood epilepsy (RCPH National Childhood Epilepsy) -<br />
100<br />
Organisational Audit<br />
Acute care<br />
Emergency use of oxygen 100<br />
Adult community acquired pneumonia Data collection in progress until 31/5/20<strong>12</strong><br />
Non invasive ventilation (NIV) - adults Data collection in progress until 31/5/20<strong>12</strong><br />
Pleural procedures 100<br />
Cardiac arrest 100<br />
Severe sepsis & septic shock 100<br />
Adult critical care 100<br />
Potential donor audit 100<br />
Long term conditions<br />
Baseline data completed on 31 January – further<br />
Heavy menstrual bleeding<br />
questionnaires being sent until February 2013<br />
Chronic pain 100<br />
Ulcerative colitis <strong>and</strong> Crohn’s disease 100<br />
Parkinson’s disease 100<br />
Chronic obstructive pulmonary disease (COPD) 100<br />
Adult asthma 100<br />
Bronchiectasis 100<br />
Elective procedures<br />
Hip, knee <strong>and</strong> ankle replacements 100<br />
Elective Surgery PROMs 100<br />
Cardiovascular disease<br />
MINAP (inc ambulance care): acute myocardial infarction<br />
(AMI) & other acute coronary syndromes (ACS) 100<br />
Heart failure 100<br />
Acute stroke 100<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 39
QUALITY ACCOUNT<br />
Audit title<br />
Percentage of data submitted<br />
Cancer<br />
Lung cancer 100<br />
Bowel cancer 100<br />
Head & neck cancer 100<br />
Oesophago-gastric cancer 100<br />
Trauma<br />
Hip fracture 100<br />
Severe trauma 100<br />
Falls <strong>and</strong> non-hip fractures 100<br />
Blood transfusion<br />
Bedside transfusion 100<br />
Medical use of blood 100<br />
End of life<br />
Care of dying in hospital 100<br />
NCEPOD<br />
Cardiac arrest procedures 100<br />
Peri-operative Care 100<br />
Bariatric surgery 100<br />
National audit <strong>report</strong>s – our response<br />
The Trust reviewed the 13 <strong>report</strong>s that were published in relation to national clinical audits during <strong>2011</strong>/<strong>12</strong>. Table 3 shows the<br />
action being taken or planned as a result of a review of the <strong>report</strong> to improve the quality of health care provided:<br />
Table 3: Trust response to national clinical audit <strong>report</strong>s <strong>2011</strong>/<strong>12</strong><br />
National audit <strong>report</strong>s<br />
issued in <strong>2011</strong><br />
College of Emergency<br />
Medicine: Paediatric<br />
Fever<br />
Date issued<br />
Apr-11<br />
Action taken as a result of recommendations<br />
Local policy reflects the recommendations - ambulant patients are<br />
assessed within 20 minutes, patients via ambulances within 15 minutes<br />
of arrival<br />
All vital signs <strong>and</strong> requests are documented on the Electronic Patient<br />
Record (EPR)<br />
College of Emergency<br />
Medicine: Vital Signs<br />
Apr-11<br />
The Trust Wide Policy on Vital Signs covers the recommendations from<br />
the <strong>report</strong><br />
College of Emergency<br />
Medicine: Renal Colic<br />
Apr-11<br />
A pathway for the management of renal colic was written <strong>and</strong> is<br />
available on the Trust intranet<br />
40 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
National audit <strong>report</strong>s<br />
issued in <strong>2011</strong><br />
National Falls <strong>and</strong> Bone<br />
Health Audit: Falls <strong>and</strong><br />
Non Hip Fractures<br />
Date issued<br />
May-11<br />
Action taken as a result of recommendations<br />
The recommendations from the <strong>report</strong> have been incorporated into local<br />
guidance <strong>and</strong> provide evidence of compliance with NICE guidance<br />
National Confidential<br />
Inquiry into Suicide <strong>and</strong><br />
Homicide by People<br />
with Mental Illness<br />
Jul-11<br />
There are processes in place that address the recommendations of this<br />
<strong>report</strong><br />
<strong>Homerton</strong> <strong>and</strong> East London Foundation Trust have meetings at an<br />
operational <strong>and</strong> a strategic level to enhance joint working to improve the<br />
care of patients mental <strong>and</strong> physical health<br />
National Confidential<br />
Enquiry into post<br />
operative death:<br />
Surgery in Children<br />
Oct-11<br />
This <strong>report</strong> will be evaluated by the paediatric team by the end of July<br />
20<strong>12</strong><br />
British Thoracic Society -<br />
Non Invasive Ventilation<br />
Nov-11<br />
This <strong>report</strong> will be evaluated by the chest physicians by the end of June<br />
20<strong>12</strong><br />
Depression <strong>and</strong> Anxiety Nov-11 This <strong>report</strong> will be evaluated by the psychology service by the end of July<br />
20<strong>12</strong><br />
NCEPOD Peri-Operative<br />
care<br />
Dec-11<br />
Two of the recommendations are already routine practice in anaesthesia<br />
– high risk patients are assessed pre –operatively <strong>and</strong> an assessment of<br />
mortality risk is calculated<br />
Urgent surgical patients also have a robust pre operative review <strong>and</strong><br />
preparation for surgery<br />
Further review of the <strong>report</strong> is underway with regard to how the<br />
recommendations are implemented within the surgical specialties<br />
Paediatric Inflammatory<br />
Bowel Disease<br />
Feb-<strong>12</strong><br />
This <strong>report</strong> will be evaluated by the multidisciplinary team by the end of<br />
July 20<strong>12</strong><br />
National Inflammatory<br />
Bowel Disease<br />
Feb-<strong>12</strong><br />
This <strong>report</strong> will be evaluated by the multidisciplinary team by the end of<br />
June 20<strong>12</strong><br />
Lung Cancer Mar-<strong>12</strong> The <strong>report</strong> has been reviewed, <strong>Homerton</strong> compares favourably to similar<br />
service providers. This <strong>report</strong> will be reviewed at the Network Tumour<br />
Advisory Board<br />
National Pain Audit -<br />
Chronic Pain<br />
Nov-<strong>12</strong><br />
This was a phase one organisational <strong>report</strong> only - no implementation<br />
plans will be required until Phase 2 has been completed in 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 41
QUALITY ACCOUNT<br />
Local audit<br />
<strong>Homerton</strong> reviewed 89 local clinical audits <strong>and</strong> is taking<br />
action as a result to improve the quality of healthcare<br />
provided. Table 4 provides a selection of actions taken from<br />
audits carried out in the Trust.<br />
Table 4: Selection of actions taken to improve care as a<br />
result of audits carried out in the Trust<br />
Local audit title Actions Done<br />
Evaluating use of occupational<br />
therapy equipment within<br />
Therapy at Home<br />
Produce a bid to re-establish ordering rights for rehabilitation<br />
equipment for the Therapy at Home team<br />
4<br />
Evaluating changes in Therapy<br />
at Home discharge <strong>report</strong>s<br />
Continue to use the new Therapy at Home discharge <strong>report</strong>s <strong>and</strong><br />
re-audit in six months time to see if they are used correctly<br />
4<br />
The use of TILEE (task,<br />
individual, load, environment,<br />
equipment- A manual h<strong>and</strong>ling<br />
assessment for patients during<br />
therapy) in the Therapy at<br />
Home team<br />
Carry out teaching sessions on TILEE (task, individual, load,<br />
environment, equipment) <strong>and</strong> the paperwork to ensure that TILEE<br />
paperwork is completed properly<br />
4<br />
An audit of the quality of spinal<br />
plain films (x-rays)<br />
Breast imaging requests<br />
• Encourage <strong>report</strong>ers to utilise the inadequate images files on the<br />
Picture Archiving Communication Systems (PACS)<br />
• Organise tutorial to recap spinal techniques <strong>and</strong> protocols<br />
• Re-audit of film quality <strong>and</strong> audit other body parts to improve film<br />
quality.<br />
• General Practitioner (GP) direct access clinic to open<br />
• Audit the (GP) direct access breast imaging requests <strong>and</strong> numbers<br />
• Gather data for an audit next year<br />
4<br />
4<br />
4<br />
4<br />
4<br />
4<br />
Audit of 100 abdomen X rays<br />
• Provide staff training on criteria for abdomen x-ray<br />
• Organise lunchtime continuous professional development sessions<br />
on abdominal x-rays<br />
4<br />
4<br />
City <strong>and</strong> Hackney Young<br />
Peoples Services (CHYPS) Plus<br />
consent <strong>and</strong> HIV Screening<br />
Audit<br />
• Remind staff to always complete the sexual health section on RIO<br />
when undertaking any Sexually Transmitted Infection checks<br />
• Remind staff to ensure that patients receive a pre-test discussion<br />
prior to testing<br />
• Remind staff to ensure that consent to tests is obtained prior to<br />
testing<br />
• Staff to record pertinent information on patients’ manual files<br />
• Deliver training to staff on consent <strong>and</strong> patient risk awareness<br />
• Increase offer of HIV testing to young people attending the service<br />
for matters relating to their sexual health by offering HIV testing<br />
as part of sexual health screening to patients<br />
• Identify training needed by staff to ensure they are competent in<br />
the use of point of care testing for HIV<br />
4<br />
4<br />
4<br />
4<br />
4<br />
4<br />
4<br />
42 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Local audit title Actions Done<br />
Clinical Manual H<strong>and</strong>ling Risk<br />
Assessment Audit<br />
Redesign new patient h<strong>and</strong>ling form; include new form in training<br />
<strong>and</strong> in the policy<br />
4<br />
Quality of information given<br />
to patients before fertility<br />
procedure<br />
• Provide training update for all staff concerned on a regular basis<br />
• Make the latest statistical information easily available on the<br />
fertility database<br />
• To ensure that emergency/out of hours contacts numbers are<br />
present on all treatment information leaflets<br />
4<br />
4<br />
4<br />
Audit to assess consent taking<br />
in Fertility<br />
• Provide training update on using consent forms<br />
• Provide training update for time schedules required for; giving,<br />
signing <strong>and</strong> returning consent forms to ensure that treatment<br />
consent is properly signed<br />
4<br />
4<br />
Priorities of Care<br />
Documentation Audit<br />
• Ward managers to disseminate information to staff.<br />
• Ward managers to monitor nursing documentation on a regular<br />
basis.<br />
4<br />
4<br />
Research<br />
The total number of patients receiving NHS services<br />
provided or sub-contracted by the Trust between 1 April<br />
<strong>2011</strong> <strong>and</strong> 28 February 20<strong>12</strong> who were recruited to<br />
participate in research approved by the research ethics<br />
committee was 1,<strong>12</strong>5.<br />
Participation in clinical research demonstrates the Trust’s<br />
commitment to improving the quality of care we offer <strong>and</strong><br />
to making our contribution to wider health improvement.<br />
<strong>Homerton</strong> was involved in conducting 146 clinical research<br />
studies in 23 specialties from April <strong>2011</strong> to the end of<br />
March 20<strong>12</strong>.<br />
A total of 53 clinical staff led on research approved by a<br />
research ethics committee at <strong>Homerton</strong> during April <strong>2011</strong><br />
to the end of March 20<strong>12</strong>.<br />
In the last three years, 164 publications have resulted from<br />
our involvement in Nation Institute for Health Research<br />
(NIHR), which shows our commitment to transparency <strong>and</strong><br />
desire to improve patient outcomes <strong>and</strong> experience across<br />
the NHS.<br />
Commissioning for quality <strong>and</strong> innovation (CQUIN)<br />
schemes<br />
This year CQUIN schemes will drive quality with some of<br />
the Trust’s income linked directly to the achievement of<br />
quality improvement goals. These goals are agreed with<br />
our commissioners to ensure that our planned quality<br />
improvements reflect the quality issues important to<br />
patients, carers <strong>and</strong> staff. For example being seen in a timely<br />
way once admitted to hospital <strong>and</strong> improving the way we<br />
interact with patients.<br />
We recognise that these issues continue to be important to<br />
our patients following the <strong>2011</strong> patient surveys.<br />
In <strong>2011</strong>/<strong>12</strong> 1.5% of the Trust’s clinical income was<br />
conditional on achieving the quality improvement <strong>and</strong><br />
innovation goals agreed between the <strong>Homerton</strong>, our<br />
commissioners NHS North East London <strong>and</strong> the City <strong>and</strong><br />
our specialist commissioners, through the Commission<br />
for Quality <strong>and</strong> Innovation payment frame work. Over the<br />
past year we have been running three CQUIN schemes;<br />
one for the acute care in the hospital, one for care in the<br />
community <strong>and</strong> specialist schemes.<br />
Further details of the agreed goals for <strong>2011</strong>/<strong>12</strong> <strong>and</strong> for the<br />
following <strong>12</strong> month period are available online at: http://<br />
www.institute.nhs.uk/commissioning/pct_portal/cquin.html<br />
As a result of the schemes we received a total of<br />
£2.2 million.<br />
See section four for further details.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 43
QUALITY ACCOUNT<br />
Care Quality Commission (CQC) registration<br />
<strong>Homerton</strong> is required to register with the Care Quality<br />
Commission <strong>and</strong> its current registration status is;<br />
registered with no conditions.<br />
The Care Quality Commission has not taken any<br />
enforcement action against <strong>Homerton</strong> during <strong>2011</strong>/<strong>12</strong>.<br />
<strong>Homerton</strong> has participated in special reviews or<br />
investigations by the CQC in relation to the following areas<br />
in <strong>2011</strong>/<strong>12</strong>:<br />
• Dignity <strong>and</strong> Nutrition Inspection (DANI) (older people)<br />
May <strong>2011</strong><br />
• Mary Seacole Nursing Home on 13 October <strong>2011</strong><br />
• <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
headquarters (comprising <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong><br />
<strong>and</strong> all the services provided by the Trust in community<br />
locations including those delivered in patients’ homes)<br />
on 15 <strong>and</strong> 22 November <strong>2011</strong><br />
• Review of termination of pregnancy services in March<br />
20<strong>12</strong> – the <strong>report</strong> from this inspection is being finalised<br />
by CQC<br />
• Safeguarding <strong>and</strong> Looked After Children Inspection in<br />
March 20<strong>12</strong> – the <strong>report</strong> from this inspection is being<br />
finalised by CQC<br />
All of these inspections were positive <strong>and</strong> constructive<br />
feedback was given by the regulator. The Trust was found<br />
to be compliant with all assessed outcomes.<br />
<strong>Homerton</strong> intends to take the following actions<br />
(see tables 5, 6 <strong>and</strong> 7) to address the conclusions or<br />
requirements <strong>report</strong>ed by the CQC. The action plan also<br />
shows the progress <strong>Homerton</strong> has made with these plans<br />
by 31 March 20<strong>12</strong>.<br />
Table 5: Action Plan following the DANI May <strong>2011</strong><br />
Regulation/ Outcome<br />
17/1<br />
Respecting <strong>and</strong> involving<br />
people who use services<br />
CQC Judgement on compliance<br />
Outcome met<br />
14/5<br />
Meeting nutritional needs<br />
Outcome met<br />
Minor concern<br />
Improvement action to maintain compliance<br />
The observations of care during the spot check will be:<br />
• disseminated widely <strong>and</strong><br />
• key lessons will be embedded in clinical staff training<br />
• access to adapted cutlery <strong>and</strong> assistance for eating <strong>and</strong> drinking to be included in the ward nutrition audits <strong>and</strong><br />
monitored.<br />
Activity<br />
The CQC Dignity <strong>and</strong> Nutrition Inspection <strong>report</strong> was emailed to all Trust staff with a covering email from<br />
the Trust Chief Executive, Nancy Hallett, on 26 May <strong>2011</strong>. The covering email noted that areas of good<br />
practice were found by the inspection team. The email also set out the improvements needed, including<br />
increasing access to specialist eating equipment <strong>and</strong> improving communication with patients.<br />
Status<br />
Completed<br />
The Council of Governors discussed the inspection <strong>report</strong> findings at their June meeting together with the<br />
action plan which was presented to them by the Chief Nurse/Director of Governance. The Trust Board of<br />
Directors also discussed the inspection <strong>report</strong> findings at their June <strong>2011</strong> meeting.<br />
The findings from the <strong>report</strong> were included in m<strong>and</strong>atory clinical update training which takes place every<br />
fortnight. Key points included in the training session are:<br />
Completed<br />
• the importance of ensuring that patients are assessed by an Occupational Therapist (OT) where<br />
relevant so that people who use services are enabled to maintain their independence supported by the<br />
provision <strong>and</strong> use of specialist eating equipment such as adapted cutlery<br />
44 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Activity<br />
Status<br />
• the importance of patients being positioned properly when eating<br />
• the importance of engaging with patients when assisting them with eating.<br />
Seventy members of staff have completed this training since the end of May <strong>2011</strong>.<br />
Awareness of the need to refer patients for assessment by an OT has been raised through m<strong>and</strong>atory<br />
clinical update training <strong>and</strong> this message has been reinforced with all of the ward managers.<br />
Completed<br />
The stock of adapted cutlery has been increased <strong>and</strong> access to this cutlery has been improved by ensuring<br />
that patients are referred for assessment by an OT. The proportion of inpatients assessed as needing<br />
assistance with eating <strong>and</strong> drinking <strong>and</strong> who received assistance improved between June <strong>and</strong> August.<br />
Direct feedback from patients using the Patient Experience Tracker shows that over 80% of patients<br />
<strong>report</strong>ed they were given help with their meals when needed. The Commissioning for Quality <strong>and</strong><br />
Innovation (CQUIN) target last year was for 75% of patients to <strong>report</strong> that they were given help with<br />
meals.<br />
2. Inspectors found that patients on Aske ward were waiting a long time for their lunch since it took<br />
approximately an hour between the arrival of first <strong>and</strong> last meal.<br />
The reasons for delays in the delivery of meals to the wards <strong>and</strong> service to patients were reviewed.<br />
The review by catering services <strong>and</strong> the dietetics staff found that the key factors behind any delays in<br />
the service of hot food to patients was not related to the capacity of the microwaves on the wards.<br />
Communication between ward staff <strong>and</strong> the ward hostess was the most important factor in ensuring that<br />
hot meals are served on the ward without delay.<br />
Key performance indicators (KPI) for the time of service of the first <strong>and</strong> last meal on the ward have been<br />
developed <strong>and</strong> are monitored in the monthly nutrition audits of all 10 wards. The total time between<br />
service of the first meal <strong>and</strong> the last meal must be no more than 30 minutes. Meals are served by <strong>12</strong>:10,<br />
<strong>12</strong>:40 or 13:10 depending on the arrangements for the individual ward due to the nature of the patients<br />
on the ward. These KPIs are also included in the monitoring of the contract with the catering supplier.<br />
Completed<br />
3. Patients with communication difficulties or who have difficulties reading the menu should be<br />
assisted by the provision of large print menus with large images<br />
A pictorial menu has been developed by the Trust Speech <strong>and</strong> Language therapists for use on Graham<br />
ward stroke unit.<br />
The monthly nutrition audits capture whether patients have seen the pictorial menu(s).<br />
The Nutrition Steering Group is working with the catering supplier (Medirest) to ensure that menus with<br />
appropriate pictures of foods are developed for all the wards.<br />
Improve the access to Kosher meals.<br />
In addition, discussion is ongoing with the Charedi Forum to ensure that all Orthodox Jewish <strong>and</strong> other<br />
patients requiring Kosher food have access to the Kosher meal menus. The Kosher meal menus have<br />
been laminated <strong>and</strong> are distributed to patients on the breakfast trays each morning.<br />
Completed<br />
Completed<br />
Ongoing<br />
Ongoing<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 45
QUALITY ACCOUNT<br />
Table 6: Action Plan from visit to Mary Seacole Nursing Home<br />
Regulation/ Outcome<br />
9/4<br />
Care <strong>and</strong> welfare of people<br />
who use services<br />
CQC Judgement on compliance<br />
Minor concerns<br />
The home was providing safe <strong>and</strong> effective care. However, the home did not always fully<br />
document people’s social background, preferences <strong>and</strong> interests <strong>and</strong> how these were<br />
being addressed, for example, through the activities on offer.<br />
1. Improving the documentation of the social background, preferences <strong>and</strong> interests of residents through the<br />
reintroduction of the existing ‘Getting to know you’ booklet<br />
Activity<br />
Implementation of the ‘Getting to know you’ booklet<br />
It is planned that the ‘Getting to know you’ booklet will be implemented in a phased manner.<br />
Engaging with Mary Seacole staff <strong>and</strong> monitoring the use of the ‘Getting to know you’<br />
booklet<br />
The ‘Getting to know you’ booklet was reintroduced to staff at the staff meeting in December <strong>2011</strong><br />
<strong>and</strong> was followed up through a reminder memo after six weeks. In addition the completion of<br />
the ‘Getting to know you’ booklet with each resident will be a st<strong>and</strong>ing item for discussion at the<br />
monthly staff meetings <strong>and</strong> in one to one meetings with the activity coordinator.<br />
Status<br />
Ongoing<br />
2. Using the information in the ‘Getting to know you’ booklet to shape activities offered<br />
<strong>and</strong> participated in by residents<br />
The nursing home has a daily living activity profile template which is used to record participation<br />
of residents in a wide range of activities. The template will be amended to make an explicit link<br />
between the activities that each resident is offered <strong>and</strong> chooses to participate in <strong>and</strong> their ‘Getting to<br />
know you’ booklet profile.<br />
Ongoing<br />
3. Improving the recording of the views of residents on their participation in activities<br />
The views of the resident (positive <strong>and</strong> negative) on different types of activities will be recorded in<br />
their personal record. At present this record is used to document when a resident has not been able<br />
to participate in an activity through tiredness or other reasons, but tends not to include when they<br />
have enjoyed an activity.<br />
Ongoing<br />
Regulation/ Outcome<br />
13/9<br />
Management of<br />
medicines<br />
CQC Judgement on compliance<br />
Minor concerns<br />
Staff generally administered <strong>and</strong> stored medicines safely. However the provider<br />
did not record its h<strong>and</strong>ling <strong>and</strong> disposal of medicines appropriately.<br />
1. Recording the h<strong>and</strong>ling <strong>and</strong> disposal of medicines in the medication administration record chart.<br />
Activity<br />
Obtaining duplicate stickers for each medication from the dispensing pharmacist<br />
The consultant nurse for medicines management <strong>and</strong> acute pain is in discussion with the pharmacy<br />
that dispenses medication for Mary Seacole Nursing Home so that a duplicate medication label will<br />
Status<br />
Completed<br />
46 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Activity<br />
Status<br />
be generated whenever medication is dispensed. This sticker will contain details of each medicine,<br />
including the quantity of medicine dispensed. It will be put on the medical administration record chart<br />
to facilitate the logging of medication.<br />
Developing a new medication administration record chart<br />
The consultant nurse for medicines management <strong>and</strong> acute pain is discussing the development<br />
of a new medication administration record chart with the company that produces these charts<br />
for the Trust.<br />
The medication administration record chart will be amended so that the sticker containing<br />
information about the medicines prescribed (as noted above) will be placed on the chart. When<br />
medication is administered to the resident, the quantity of medication given will be recorded on<br />
the chart <strong>and</strong> a running balance of medication remaining will be calculated <strong>and</strong> recorded on the<br />
chart. When medication is disposed of this will also be recorded on the chart, <strong>and</strong> the balance of<br />
medication remaining at the nursing home will also be noted.<br />
In addition, the new medication administration record chart will contain a box where allergies<br />
will be recorded.<br />
The new chart will be piloted in the nursing home before full implementation.<br />
Audit of the use of the new medication administration record chart.<br />
Completed<br />
Table 7: Action Plan from visit to <strong>Homerton</strong> <strong>Hospital</strong><br />
Regulation/ Outcome<br />
17/1<br />
Respecting <strong>and</strong> involving<br />
people who use services<br />
Regulated activity<br />
Treatment of disease,<br />
disorder or injury<br />
CQC Judgement on compliance<br />
Minor concern<br />
Patients <strong>report</strong>ed having to wait for care (for example, help with getting dressed) on<br />
the Regional Neurological Rehabilitation Unit. The Trust provided some information<br />
about improvements planned for this unit, but this did not explain in any detail how<br />
this concern would be addressed.<br />
Improve the way in which the Trust monitors <strong>and</strong> records how the multi-disciplinary team on the Regional<br />
Neurological Rehabilitation Unit (RNRU) operates so that the care provided continues to respect <strong>and</strong> involve<br />
people who use services.<br />
Activity<br />
When/Status<br />
1. Strengthening the means by which feedback from people who use services is gathered <strong>and</strong> used to<br />
improve patient care<br />
The Trust has recently developed a Patient Experience Strategy a key part of which is to use<br />
patient involvement to improve the services delivered by the Trust. The strategy recognises<br />
that ‘one size does not fit all’ <strong>and</strong> encourages each of the Trust’s services <strong>and</strong> divisions to<br />
set their own patient experience campaign objectives <strong>and</strong> <strong>report</strong> on these to the Patient<br />
Experience <strong>and</strong> Engagement Committee (PEEC).<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 47
QUALITY ACCOUNT<br />
Activity<br />
Head of Nursing (acute) Integrated Medical <strong>and</strong> Rehabilitation Services (IMRS) <strong>and</strong> the senior<br />
sister in charge of RNRU will meet with the RNRU patient family carers group <strong>and</strong> patients to<br />
discuss the contents of the CQC inspection <strong>report</strong> <strong>and</strong> to gain their views <strong>and</strong> suggestions<br />
on the actions planned.<br />
This meeting will also be an opportunity to set up regular meetings at a time (including<br />
evenings or on a Saturday) <strong>and</strong> frequency to suit the family carers. These meetings will<br />
complement the regular individual meetings between the key worker <strong>and</strong> each family.<br />
The Head of Occupational Therapy will develop a patient feedback questionnaire which will<br />
be implemented <strong>and</strong> <strong>report</strong>ed on to the PEEC.<br />
When/Status<br />
March 20<strong>12</strong><br />
completed<br />
September 20<strong>12</strong><br />
2. Monitoring the way in which nursing staff <strong>and</strong> therapists work together to provide<br />
personal care to patients<br />
Joint sessions between nursing staff <strong>and</strong> therapists are recorded <strong>and</strong> <strong>report</strong>ed to UK specialist<br />
Rehabilitation Outcomes Collaborative (UK-ROC) as well as recorded in the individual patient<br />
record.<br />
A summary of these sessions will be discussed at the quarterly Head of Department meeting. July 20<strong>12</strong><br />
3. ‘Priorities of Care’ audits to assess, plan, implement <strong>and</strong> evaluate nursing care<br />
The unit will continue to carry out monthly ‘Priorities of Care’ audits. Particular attention will<br />
be paid to the results for the ‘hygiene <strong>and</strong> continence’ element of this framework.<br />
A summary of these audits <strong>and</strong> the follow up action needed will be discussed at the<br />
quarterly Head of Department meeting.<br />
November 20<strong>12</strong><br />
4. Improving the recording of feedback from nursing staff<br />
There is a weekly meeting for nursing staff on the unit. These meetings are an opportunity to<br />
discuss a variety of issues such as workload including any occasion where breaks are missed.<br />
The agenda <strong>and</strong> notes of these meetings will be formalised to include issues such as<br />
workload <strong>and</strong> staffing resources <strong>and</strong> any effect on patient care.<br />
A summary of issues raised at the weekly nursing staff meeting will be discussed between<br />
the senior sister in charge of the unit <strong>and</strong> the IMRS divisional Head of Nursing (acute).<br />
May 20<strong>12</strong><br />
Statement on data quality<br />
The Trust’s Data Quality Policy has been implemented,<br />
defining the st<strong>and</strong>ards that must be applied to all databases<br />
within the Trust (in line with the st<strong>and</strong>ards set by the<br />
Connecting for Health Quality <strong>and</strong> Assurance Programme<br />
for Data Quality).<br />
The data we produce to verify our position must be of the<br />
highest quality. Data is regarded as being of high quality if<br />
it is:<br />
• accurate<br />
• up to date<br />
• free from duplication<br />
• free from confusion<br />
• comprehensive<br />
• valid<br />
• available when needed<br />
• stored securely <strong>and</strong> confidentially.<br />
The Data Quality Committee has been reviewed; the Trust<br />
now has an Electronic Patient Record (EPR) Management<br />
Group which is chaired by the Associate Director for IT. This<br />
48 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
group <strong>report</strong>s to the Informatics Committee chaired by the<br />
Chief Operating Officer.<br />
Over the last year <strong>Homerton</strong> has taken the following<br />
actions to improve data quality:<br />
• Intensive work has been undertaken specifically to<br />
review the quality of data surrounding outpatient activity.<br />
• M<strong>and</strong>atory data was reviewed on a regular <strong>and</strong> on going<br />
basis, for errors.<br />
• A suite of <strong>report</strong>s was been developed which detect<br />
errors in order that they can be identified <strong>and</strong> corrected.<br />
• Staff were consulted <strong>and</strong> involved with reviewing<br />
working practices <strong>and</strong> st<strong>and</strong>ard operating procedures, to<br />
identify why the errors were occurring.<br />
• Training for staff using the IT systems is under review to<br />
ensure that staff have the most robust training available<br />
to help minimise errors.<br />
• There has been significant improvement over the year,<br />
regular monitoring <strong>and</strong> support for staff have resulted in<br />
improved quality data.<br />
Trust data that was submitted for national use<br />
The Trust submitted records during <strong>2011</strong>/<strong>12</strong> to the<br />
Secondary Uses Service (SUS) for inclusion in the <strong>Hospital</strong><br />
Episode Statistics (HES) which are included in the latest<br />
published data. The percentage of records in the published<br />
data that included the patients’ valid NHS numbers was:<br />
- 95.6% for admitted patient care<br />
- 97.4% for outpatient care, <strong>and</strong><br />
- 86.5% for accident <strong>and</strong> emergency care.<br />
Data which included the patients valid General Medical<br />
Practice Code was:<br />
- 100% for admitted patient care<br />
- 100% for outpatient care<br />
- 100% for accident <strong>and</strong> emergency care.<br />
Information governance (IG)<br />
The Trust’s Information Governance Assessment Report<br />
overall score for <strong>2011</strong>/<strong>12</strong> was 71%. This is graded as not<br />
satisfactory.<br />
This figure is an improvement on last year (67%) but trusts<br />
are expected to achieve level two in all areas in order to be<br />
graded as satisfactory. <strong>Homerton</strong> is at level one for three<br />
areas.<br />
The key actions to address the three areas are managed by<br />
the Information Governance Committee, these are:<br />
• improvements in training - trusts are required to<br />
demonstrate that 95% of staff have had IG training<br />
every year.<br />
• carry out a clinical records keeping audit – this is<br />
currently underway (April 20<strong>12</strong>).<br />
• pseudonomisation – this is about ensuring we do not<br />
use personal identifiable information for secondary use.<br />
The information team have the software in place to<br />
assist with this, but we are not permitted to score this<br />
element of the toolkit at level 2 until we have level 2 in<br />
all other areas.<br />
Alternative ways of delivering IG training to staff are being<br />
discussed with Connecting for Health in order to improve<br />
<strong>and</strong> maintain training rates over the coming years.<br />
Payment by Results<br />
The Trust was subject to the Payment by Results clinical<br />
coding audit during the <strong>report</strong>ing period by the Audit<br />
Commission <strong>and</strong> the error rate* in the latest published<br />
audit for that period for spells with an error affecting price<br />
(clinical coding) was: 3.7%<br />
Primary diagnoses incorrect 7.5%<br />
Secondary diagnoses incorrect 13.8%<br />
Primary procedure incorrect 4.0%<br />
Secondary procedures incorrect 8.7%<br />
These results should not be extrapolated further than the<br />
actual sample audited; the following services were audited:<br />
Total sample size was 200 finished<br />
consultant episodes (FCEs)**<br />
Obstetrics: sample size 100 FCEs<br />
R<strong>and</strong>omly chosen: sample size 100 FCEs<br />
*This audit was of 200 patient records in <strong>2011</strong>/<strong>12</strong> selected<br />
at r<strong>and</strong>om by the Audit Commission from SUS data. The<br />
audit showed that of this sample 3.7% had the inaccurate<br />
code for the patients episode of care recorded.<br />
**A Finished Consultant Episode is the period of time<br />
during which the patient was cared for by one consultant.<br />
A patient could have more than one consultant episode<br />
during their hospital stay if care was transferred to another<br />
consultant.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 49
QUALITY ACCOUNT<br />
SECTION 4 – Quality improvements<br />
<strong>2011</strong>-20<strong>12</strong><br />
This section of the <strong>report</strong> summarises our performance<br />
from April <strong>2011</strong> to the end of March 20<strong>12</strong> in relation to:<br />
national targets; the priorities we set in last year’s Quality<br />
Account, CQUINS, <strong>and</strong> other work streams directly relating<br />
to the quality of care.<br />
The information is divided into four sections: specific<br />
National Targets; Safety; Clinical Effectiveness; <strong>and</strong> Patient<br />
Experience.<br />
National targets<br />
The Trust is required to monitor regularly its position against<br />
a number of performance targets set buy the Department<br />
of Health. Table 8 shows the Trust’s position against these<br />
targets for the years <strong>2011</strong>/<strong>12</strong> against the required target.<br />
Table 8: Trust position against national performance targets<br />
for <strong>2011</strong>/<strong>12</strong>.<br />
<strong>2011</strong>/<strong>12</strong><br />
Actual<br />
<strong>2011</strong>/<strong>12</strong><br />
Target<br />
Emergency Care patients seen in
Meticillin Resistant Staphylococcus aureus (MRSA)<br />
This year our target, not to be exceeded for MRSA<br />
bacteraemias, (a blood stream infection with MRSA whilst<br />
in hospital) was three cases.<br />
We have not had a single patient develop MRSA<br />
bacteraemia this year. This is due to the hard work of<br />
our Infection Control Team working together with staff,<br />
patients <strong>and</strong> visitors.<br />
The Infection Control Team provide ongoing training for<br />
staff, raise awareness of the need for clean h<strong>and</strong>s in staff,<br />
patients <strong>and</strong> visitors <strong>and</strong> monitor compliance with h<strong>and</strong><br />
hygiene requirements.<br />
All patients are now screened on admission to hospital for<br />
MRSA <strong>and</strong> some prior to coming in for planned procedure.<br />
Work continues in relation to invasive devices such as drips<br />
<strong>and</strong> drains to reduce the risk of patients developing an<br />
infection.<br />
Our rate of MRSA bacteraemia not to be exceeded for next<br />
year is no more than one case.<br />
Clostridium difficile (C.diff)<br />
Our C.diff rates this year have been low - a total of nine<br />
patients developed C.diff in hospital – this is one patient<br />
less than the year before. We are maintaining very low<br />
rates of C.diff in the hospital (see page 54 for further<br />
information).<br />
Priorities <strong>2011</strong>/<strong>12</strong><br />
In <strong>2011</strong>/<strong>12</strong> following consultation with our Council of<br />
Governors <strong>and</strong> our Foundation Trust members we identified<br />
four priorities that the Board of Directors agreed we should<br />
strive to achieve. These were put together with the local,<br />
regional <strong>and</strong> local CQUINS to formally provide our quality<br />
priorities for <strong>2011</strong>/<strong>12</strong>.<br />
Safety St<strong>and</strong>ards: safety of patient, staff<br />
<strong>and</strong> visitors<br />
Maintaining the safety of patients, staff <strong>and</strong> visitors is a vital<br />
part of running the Trust; anyone who visits us for clinical<br />
care or to work needs to be confident that they will be safe<br />
whilst they are here.<br />
Priority 1 – Maximise safety for patients – ensure that<br />
clinical incidents are regularly <strong>report</strong>ed in the Trust <strong>and</strong><br />
demonstrate improvements to safety gained from this<br />
information.<br />
This year we aimed to increase our clinical incident<br />
<strong>report</strong>ing to demonstrate that our safety culture is<br />
improving. Figure 1 shows the total clinical incidents<br />
<strong>report</strong>ed from April 2009 to the end of March 20<strong>12</strong> (data<br />
from the Trust’s risk management database).<br />
Figure 1: Total <strong>report</strong>ed clinical incidents April 2009 to<br />
March 20<strong>12</strong><br />
4100<br />
4000<br />
3900<br />
3800<br />
3700<br />
3600<br />
3500<br />
3400<br />
3300<br />
3200<br />
3100<br />
3000<br />
09/10 10/11 11/<strong>12</strong><br />
2009/10 2010/11 <strong>2011</strong>/<strong>12</strong><br />
We <strong>report</strong>ed 4033 clinical incidents last year, 641 more<br />
than the year before. The fact that we have become a<br />
larger organisation, with the integration of community<br />
health services, does not in itself account for this increase.<br />
There has been a general rise in clinical incident <strong>report</strong>ing.<br />
This is a positive sign <strong>and</strong> indicates that staff are confident<br />
to <strong>report</strong> all clinical incidents no matter how small.<br />
Information collated from data we sent to the National<br />
Patient Safety Agency (NPSA) for 1 April <strong>2011</strong> <strong>and</strong> 30<br />
September <strong>2011</strong> shows that we were <strong>report</strong>ing 7.9 clinical<br />
incidents for every 100 patient admissions to the hospital.<br />
When we compare ourselves to other NHS trusts of a<br />
similar size in Engl<strong>and</strong>, eight out of 30 trusts are <strong>report</strong>ing<br />
a greater number of incidents per 100 admissions than<br />
us. We are just below the top 25% of trusts with high<br />
<strong>report</strong>ing rates. The top trust in the group <strong>report</strong>s 14.5<br />
incidents for every 100 patient admissions.<br />
Because we have seen an improvement over the year with<br />
no increased harm this priority will be retired from the<br />
Quality Account for the coming year. Despite not being<br />
a Quality Account priority our work will continue to train<br />
more staff to use the risk management database <strong>and</strong> carry<br />
on encouraging <strong>report</strong>ing as part of routine practice within<br />
the Trust. We aspire to be in the top 25% of trusts for<br />
<strong>report</strong>ing by the end of March 2013.<br />
Figure 2 shows the total incidents <strong>report</strong>ed by the degree<br />
of harm to the patient. The majority (77%) of <strong>report</strong>ed<br />
incidents resulted in no harm to the patient. The number<br />
of patients who sustained minor harm has increased<br />
compared to last year from 14% to 18%. Moderate <strong>and</strong><br />
severe harm incidents have made marginal increases.<br />
We will be closely monitoring all clinical incidents that result<br />
in any type of harm <strong>and</strong> reviewing the data to ensure that<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 51
QUALITY ACCOUNT<br />
the correct information is recorded. For incidents where<br />
there is no harm, risk reducing actions are put into place to<br />
guard against harm.<br />
Figure 2: Degree of harm to patients from clinical incidents<br />
April 2009 to March 20<strong>12</strong><br />
3500<br />
3000<br />
2500<br />
2000<br />
1500<br />
1000<br />
500<br />
0<br />
None Minor Moderate Severe Catas<br />
2009/10 2010/11 <strong>2011</strong>/<strong>12</strong><br />
The trend in increased <strong>report</strong>ing indicates that we are<br />
becoming more safety aware <strong>and</strong> <strong>report</strong>ing incidents even<br />
though no one was injured. This is a trend we want to<br />
encourage as it gives us an early opportunity to address any<br />
issues <strong>and</strong> take steps to reduce risks to the patients in our<br />
care.<br />
The top three <strong>report</strong>ed types of clinical incidents were<br />
related to: falls, medication, <strong>and</strong> treatment. The top three<br />
have remained the same for the last three years.<br />
Serious incidents (SI)<br />
A serious incident or SI covers incidents with serious<br />
consequences including those that compromise the Trust<br />
from providing care e.g. fire, power failure, adverse serious<br />
media coverage or a patient sustaining a major injury or<br />
avoidable death as a result of a clinical incident whilst in<br />
the care of the Trust. These incidents are <strong>report</strong>ed to the<br />
Strategic Health Authority, NHS London <strong>and</strong> the Trust<br />
commissioners NHS North East London <strong>and</strong> the City.<br />
As our incident <strong>report</strong>ing rate has risen so has our SI<br />
<strong>report</strong>ing rate. During the past year <strong>2011</strong>/<strong>12</strong> we have<br />
<strong>report</strong>ed 62 serious incidents. These SIs represent 1.5% of<br />
all <strong>report</strong>ed clinical incidents; an increase of 0.5% on last<br />
year.<br />
All SIs are investigated using root cause analysis methods<br />
to establish precisely why the incident occurred so<br />
recommendations can be made for changes to practice.<br />
This process reduces the risk of a similar incident occurring<br />
again.<br />
The highest number of SIs last year related to pressure<br />
ulcers (see page 52 for further information on pressure<br />
ulcers). Pressure ulcers occur in both hospital <strong>and</strong><br />
community settings. The investigations into these pressure<br />
ulcers have led to the following changes:<br />
• The implementation of a Trust wide policy on the<br />
prevention <strong>and</strong> treatment of pressure ulcers.<br />
• The development of an information leaflet for patients<br />
<strong>and</strong> their families.<br />
• Increased education <strong>and</strong> awareness amongst staff of<br />
how to prevent ulcers occurring.<br />
• Increased education amongst staff on the grading <strong>and</strong><br />
management of pressure ulcers that do develop.<br />
Never Events<br />
The National Patient Safety Agency <strong>and</strong> the Department of<br />
Health have identified certain incidents that should never<br />
happen; these are known as Never Events.<br />
This list of never events was extended from eight to 25 last<br />
year. Please see the following web site for more information<br />
http://www.dh.gov.uk/en/Publications<strong>and</strong>statistics/<br />
Publications/PublicationsPolicyAndGuidance/DH_<strong>12</strong>4552<br />
Last year at <strong>Homerton</strong> we had three Never Events: two<br />
involving a retained swab following a procedure <strong>and</strong> one<br />
wrong site surgery. We have reviewed current clinical<br />
practice to establish how these events occurred <strong>and</strong> audited<br />
the areas where similar activities are carried out. The fact<br />
that these incidents have happened has been shared with<br />
staff so that they can learn from them.<br />
The procedure for checking the details of a patient <strong>and</strong><br />
the planned procedure prior to surgery was audited in<br />
November <strong>2011</strong>, the results demonstrated good practice.<br />
Some areas for improvement were identified <strong>and</strong> the<br />
clinical teams have discussed the audit <strong>and</strong> changed<br />
practice. The audit will be repeated again in the summer.<br />
The policy <strong>and</strong> practice related to the counting of swabs<br />
following any clinical procedure, has been reviewed<br />
<strong>and</strong> made more stringent. An audit of this policy will be<br />
repeated in the summer.<br />
Pressure ulcers<br />
Pressure ulcer prevention remains of the utmost importance<br />
at <strong>Homerton</strong>, whether for patients in hospital or patients<br />
we are caring for at home.<br />
Figures 3 <strong>and</strong> 4 show the total number of pressure ulcers<br />
of all grades that were detected in the Trust in <strong>2011</strong>/<strong>12</strong>.<br />
The ulcer grading runs from: 1 being the mildest blanching<br />
effect on the skin <strong>and</strong> surrounding tissues to 4 being the<br />
most severe.<br />
Prevention of pressure ulcers is imperative, however if a<br />
patient does develop a pressure ulcer it is essential that this<br />
52 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
is <strong>report</strong>ed as a clinical incident so that the extent of this<br />
problem is clear <strong>and</strong> can be addressed.<br />
The <strong>report</strong>ing of pressure ulcers is a vital tool in reducing<br />
their occurrence. These figures are higher than last year<br />
partly due to increased awareness amongst staff. Staff are<br />
acutely conscious of the importance of; monitoring patients<br />
skin <strong>and</strong> <strong>report</strong>ing even the most minor blemish, calling for<br />
assistance <strong>and</strong> initiating treatment as soon as possible.<br />
We are working toward zero tolerance of pressure<br />
ulcers, this is one of the elements of the harm free care<br />
programme that the Trust will be part of next year.<br />
Figure 3: Total <strong>Hospital</strong> acquired pressure ulcers by month<br />
20<br />
18<br />
16<br />
14<br />
<strong>12</strong><br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar<br />
Figure 5: Total <strong>Homerton</strong> community acquired pressure<br />
ulcers by month<br />
5<br />
4<br />
4<br />
3<br />
3<br />
2<br />
2<br />
1<br />
1<br />
0<br />
The total number of pressure ulcers acquired in the<br />
community by grade 2 to 4 is shown in figure 6<br />
Figure 6: Total community pressure ulcers by grade April<br />
<strong>2011</strong> to March 20<strong>12</strong><br />
<strong>12</strong><br />
10<br />
8<br />
6<br />
4<br />
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar<br />
2<br />
Figure 4: Total hospital acquired pressure ulcers grade 2 to 4<br />
April <strong>2011</strong> to March 20<strong>12</strong><br />
90<br />
80<br />
0<br />
Hommerton<br />
Community Care<br />
acquired pressure<br />
ulcer grade 2<br />
Hommerton<br />
Community Care<br />
acquired pressure<br />
ulcer grade 3<br />
Hommerton<br />
Community Care<br />
acquired pressure<br />
ulcer grade 4<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
Falls<br />
Over the course of the year the number of <strong>report</strong>ed falls<br />
has increased, this is thought to be due to increased<br />
awareness of staff to the requirement to <strong>report</strong> all<br />
incidents. Figure 7 provides information on the number of<br />
falls <strong>report</strong>ed.<br />
0<br />
<strong>Hospital</strong> acquired<br />
(>72 hours)<br />
pressure ulcer<br />
grade 2<br />
<strong>Hospital</strong> acquired<br />
(>72 hours)<br />
pressure ulcer<br />
grade 3<br />
<strong>Hospital</strong> acquired<br />
(>72 hours)<br />
pressure ulcer<br />
grade 4<br />
Figure 7: Total <strong>report</strong>ed patient falls April 2010 to<br />
March 20<strong>12</strong><br />
790<br />
780<br />
770<br />
760<br />
750<br />
740<br />
730<br />
720<br />
2010/11 <strong>2011</strong>/<strong>12</strong><br />
The main increase appears to be the type of fall where the<br />
patient has sustained minor harm; this could be anything<br />
from a bruise to a laceration.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 53
QUALITY ACCOUNT<br />
Figure 8 shows actual harm to patients in 2010/11<br />
compared with <strong>2011</strong>/<strong>12</strong><br />
Figure 8: Degree of actual harm to patients as a result of a<br />
fall April 2010 – March 20<strong>12</strong><br />
600<br />
500<br />
400<br />
300<br />
200<br />
100<br />
0<br />
None Minor Moderate Severe Catas<br />
2010/11 <strong>2011</strong>/<strong>12</strong><br />
All patients who fall in the hospital are reviewed by the Falls<br />
Prevention Nurse Specialist. Staff training is on going to<br />
ensure all patients are assessed on admission for their risk<br />
of falling <strong>and</strong> that appropriate measures are put in place to<br />
reduce the risks to the patient.<br />
There is also a Falls Prevention Clinic which works together<br />
with patients to help them to take actions that can reduce<br />
their risk of falling, particularly at home.<br />
Summary <strong>Hospital</strong>‐Level Mortality Indicator (SHMI)<br />
The way mortality rates are calculated nationally has been<br />
altered to a new measure called the Summary <strong>Hospital</strong>‐<br />
Level Mortality Indicator (SHMI). This measure gives an<br />
indication of whether the mortality rate of our patients<br />
is above or below what is expected when compared to<br />
a national baseline. In the data produced by the NHS<br />
Information Centre in January 20<strong>12</strong> (coving the period July<br />
2010 to June <strong>2011</strong>) our mortality rate for the past year was<br />
within the expected range.<br />
The SHMI is b<strong>and</strong>ed for each trust as follows:<br />
1 – where the Trust’s mortality rate is ‘higher than expected’<br />
2 – where the Trust’s mortality rate is ‘as expected’<br />
3 – where the Trust’s mortality rate is ‘lower than expected’<br />
Our SHMI is b<strong>and</strong>ed at 2 on the data from the NHS<br />
information centre.<br />
The percentage of our admitted patients during this time<br />
period with a palliative care coding was 0.1%.<br />
The percentage of patients that died with a palliative care<br />
coding was 2.7%.<br />
We will be focusing on improving safety <strong>and</strong> reducing our<br />
mortality rate next year as a Quality Account priority <strong>and</strong><br />
part of the QUEST programme.<br />
Clostridium difficile (C.diff)<br />
Our C.diff rates have been very low - a total of nine patients<br />
developed C.diff infection in hospital last year – this is one<br />
patient less than the year before. We are maintaining very<br />
low rates of C.diff in the hospital.<br />
This is due to a combination of:<br />
• h<strong>and</strong> hygiene which continues to be a vital part of<br />
combating infection at the Trust. All clinical areas audit<br />
their h<strong>and</strong> hygiene every two weeks <strong>and</strong> the results are<br />
shared on the Trust intranet. These audits show that<br />
staff are washing/using alcohol gel on their h<strong>and</strong>s on<br />
average 90% of the time. There are some areas that are<br />
achieving 100% on each audit, <strong>and</strong> these audits show a<br />
steady improvement on last year when we were cleaning<br />
our h<strong>and</strong>s 85% of the time.<br />
• good antibiotic prescribing with regular audits to<br />
monitor compliance.<br />
• the work of the infection control team <strong>and</strong> other staff.<br />
• if any patient does develop C.diff whilst in hospital<br />
they continue to be looked after by their own team of<br />
doctors <strong>and</strong> nurses but they are also seen at least once<br />
a week on a multidisciplinary ward round – the team is<br />
made up of; infection control nurses, a microbiologist<br />
(doctor), dietitians <strong>and</strong> the antibiotic pharmacist. These<br />
patients are monitored <strong>and</strong> followed up by this team for<br />
the rest of their stay in hospital.<br />
Our C.diff rate per 100,000 bed days is not yet available<br />
for last year, but the figures for the preceding three years<br />
indicate the improvements we have made in reducing the<br />
number of patients developing C.diff in hospital. Figure<br />
9 shows C.diff rates in patients over two years of age (all<br />
patients) <strong>and</strong> also in patients over 65 years of age.<br />
Figure 9: Rates of C.diff per 100,000 bed days at <strong>Homerton</strong><br />
from 2008 to <strong>2011</strong><br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
2008-09 2009-10 2010-11<br />
C.diff rate per 1000,000<br />
bed days in patients >2<br />
C.diff rate per 1000,000<br />
bed days in patients >65<br />
When we compare our rates of C.diff to other trusts, we<br />
are one of only nine trusts in Engl<strong>and</strong> that currently has a<br />
C.diff rate of fewer than 10 cases per 100,000 bed days for<br />
all patients. We are also in the top five of trusts with a rate<br />
of fewer than 20 cases per 100,000 bed days for patients<br />
over 65.<br />
54 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
This data was taken from:<br />
http://www.hpa.org.uk/Topics/InfectiousDiseases/<br />
InfectionsAZ/ClostridiumDifficile/EpidemiologicalData/<br />
M<strong>and</strong>atorySurveillance/cdiffM<strong>and</strong>atoryReportingScheme/<br />
High impact interventions (HIIs)<br />
We are continuing with the activities that have a high<br />
impact on reducing the risk of infection related to care.<br />
These are the bundles of care for specific interventions that<br />
involve; how to carry out that care <strong>and</strong> how to measure<br />
that it has been done correctly. Using the care bundle<br />
approach keeps the risk of infection to patients low. The<br />
high impact interventions that we use include:<br />
• Central venous catheter care (insertion <strong>and</strong> ongoing)<br />
• Peripheral venous catheter care (insertion <strong>and</strong> ongoing)<br />
• Renal dialysis catheter care (insertion <strong>and</strong> ongoing)<br />
• Prevention of surgical site Infection (pre operative <strong>and</strong><br />
peri operative)<br />
• Care of ventilated patients (ongoing)<br />
• Urinary catheter care (insertion <strong>and</strong> ongoing)<br />
• Reducing the risk of C.diff.<br />
• Clinical equipment decontamination (Not contaminated<br />
<strong>and</strong> HCAI)<br />
• Stoma care (planning <strong>and</strong> ongoing)<br />
All clinical teams collect data on how they are carrying out<br />
the high impact interventions, this data is then sent to the<br />
Infection Control Team who monitor activity, collate the<br />
information <strong>and</strong> work with any areas that require support.<br />
Patient safety CQUINS<br />
Table 9 shows the Trust position against the patient safety<br />
CQUINS<br />
Table 9: Patient safety CQUINS<br />
CQUIN<br />
What were we<br />
aiming to do<br />
Did we<br />
achieve it<br />
What is the evidence<br />
National<br />
Introduce the Department<br />
of Health’s patients risk<br />
assessment for venous<br />
thrombosis (blood clots) for<br />
all adult patients<br />
Demonstrate that 90%<br />
of all eligible adult<br />
patients have been<br />
assessed for VTE risk in<br />
quarter 4 (January to<br />
end March)<br />
No<br />
See below.<br />
London wide<br />
Continue with <strong>and</strong> extend<br />
the Enhanced Recovery<br />
Programme to reduce<br />
length of stay <strong>and</strong> improve<br />
the patient’s experience of<br />
surgery.<br />
Report on the national<br />
ERP database<br />
Partial<br />
This CQUIN is also about Clinical<br />
effectiveness <strong>and</strong> the patient experience<br />
Gynaecology did not come in to the<br />
programme until October <strong>2011</strong> which<br />
meant <strong>report</strong>ing on the national database<br />
did not included gynaecology for the full<br />
year.<br />
Reduce length of stay<br />
to agreed targets in<br />
orthopaedics, colorectal,<br />
gynaecology <strong>and</strong><br />
urology (for specific<br />
procedures)<br />
Use of fluid directed<br />
therapy in colorectal<br />
patients.<br />
Carry out surgery on the<br />
day of admission<br />
50% Length of stay targets have not been met<br />
in colorectal <strong>and</strong> orthopaedics.<br />
100%<br />
(see below for more detail)<br />
85% This figure is due to gynaecology data not<br />
being included on the national data base<br />
for the full year.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 55
QUALITY ACCOUNT<br />
CQUIN<br />
What were we<br />
aiming to do<br />
Did we<br />
achieve it<br />
What is the evidence<br />
<strong>Homerton</strong><br />
Discharge communications<br />
Reduce the amount of<br />
discharge summaries<br />
not received by GPs<br />
(ELC/GP audit<br />
showed the<br />
following)<br />
Quality: 70%<br />
Timeliness:47%<br />
Reduce the time for<br />
outpatients letters to<br />
reach GPs<br />
Yes<br />
Data collected by the commissioners<br />
<strong>Homerton</strong><br />
Surgical Theatres<br />
Programme<br />
For 95% of patients<br />
requiring emergency<br />
surgery to have the<br />
surgery done in
In orthopaedics, an audit by junior doctors showed that<br />
it would be advantageous in helping patients get home<br />
quickly to; enhance preparation of patients preoperatively<br />
<strong>and</strong> ensure early action to address any patient not<br />
recovering as rapidly as expected post operatively. To<br />
address these elements of the ERP a multidisciplinary,<br />
orthopaedic specific, Enhanced Recovery Group has been<br />
set up to work on every element of the patients pathway to<br />
ensure that optimum conditions are in place for patients to<br />
go home on the expected day following surgery.<br />
Although ERP will not be a CQUIN for 20<strong>12</strong>/13 we will<br />
be continuing our work to become an ERP hospital. All<br />
patients having surgery when they need to stay overnight<br />
in hospital will benefit from ERP.<br />
Clinical effectiveness: Effective treatment<br />
with good outcomes<br />
Priority 2 – Promote effective care – ensure that, where<br />
national clinical guidelines have been produced by the<br />
National Institute for Health <strong>and</strong> Clinical Excellence<br />
(NICE) which are relevant to the care we provide, we<br />
can demonstrate we are using or planning to use them<br />
in everyday practice. This year we aimed to develop a<br />
formal audit programme to ensure that established clinical<br />
guidelines from NICE that are relevant to the Trust are<br />
audited regularly to demonstrate that clinical practice<br />
continues to be of the highest st<strong>and</strong>ard.<br />
NICE guidance is broad ranging <strong>and</strong> affects a significant<br />
proportion of our services. Some cover the entire<br />
patient pathway, others specific treatments with specific<br />
medications.<br />
Over the last year we have reviewed all NICE guidance<br />
that has been released since 2003 to see which ones<br />
are relevant to the Trust – as of April 20<strong>12</strong> a total of 184<br />
guidelines apply to our services. These are broken down as<br />
follows:<br />
Clinical Guidelines 96<br />
Interventional Procedures 40<br />
Technology appraisals (not medicines) 15<br />
Public Health Guidelines 31<br />
Medical Technologies 2<br />
We have been liaising with the relevant clinical staff in order<br />
to establish whether the NICE guidelines are being used in<br />
practice. The current position is as shown in table 10.<br />
We are currently assessing 45 guidelines to see if they are<br />
relevant to our practice (public health <strong>and</strong> interventional<br />
procedures) <strong>and</strong> waiting for information on compliance<br />
from clinicians on 18 guidelines (clinical guidelines).<br />
There are challenges involved in collecting this information<br />
<strong>and</strong> we currently do not have a complete picture. For this<br />
reason this remains a priority for next year.<br />
Fourteen audits have been carried out by departments in<br />
the past year against their use of NICE guidelines; these<br />
ranged from smoking cessation to the use of analgesia in<br />
patients with dementia to use of the falls pathway by the<br />
Therapy at Home Team. In any audit where a shortfall in<br />
practice was identified an action plan was put in place to<br />
address any issues the audit had highlighted.<br />
Table 10: Implementation of NICE guidance from<br />
March 11 to March <strong>12</strong><br />
Type of Guideline<br />
Number Fully Implemented<br />
March 20<strong>12</strong><br />
Percentage of relevant<br />
guidelines fully<br />
implemented<br />
March 20<strong>12</strong><br />
Percentage of relevant<br />
guidelines fully<br />
implemented<br />
March <strong>2011</strong><br />
Clinical Guidelines 69 72% 27%<br />
Interventional Procedures 16 35% 19%<br />
Technology Appraisals 15 (non medication) 100% 8%<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 57
QUALITY ACCOUNT<br />
Table 11 shows the Trust’s position against clinical<br />
effectiveness indicators.<br />
Table 11: 2010/11 position against clinical effectiveness<br />
indicators CQUINS<br />
CQUIN<br />
What did we have to do<br />
Did we<br />
achieve it<br />
What is the evidence<br />
In the community<br />
The Virtual Ward<br />
(community)<br />
N/A<br />
This CQUIN has been<br />
discontinued. There is another<br />
project beginning relating to<br />
regular, case conferences with all<br />
professionals to discuss patients<br />
being looked after at home or in<br />
the community<br />
London Wide<br />
Adult patients should be<br />
reviewed by a consultant<br />
within <strong>12</strong> hours of<br />
admission to hospital<br />
75% of adult emergency patients<br />
should be reviewed by a consultant<br />
within <strong>12</strong> hours of admission<br />
Yes<br />
This CQUIN is also about patient<br />
safety <strong>and</strong> the patient experience<br />
Locally collected data<br />
In the community:<br />
End of Life Care (EoLC)<br />
Ensure 80% of patients who die at<br />
home are to be on the Liverpool Care<br />
Pathway<br />
100% This CQUIN is also about patient<br />
safety <strong>and</strong> the patient experience<br />
Local data<br />
Repeat the patient equipment audit<br />
<strong>and</strong> <strong>report</strong> on outcomes.<br />
Achieved<br />
Local audit<br />
Increase referrals to Palliative Care<br />
For 95% of patients who die at home<br />
to have a documented advance care<br />
planning discussion<br />
100%<br />
Achieved<br />
Local data<br />
Local data<br />
Report the progress on actions set<br />
out in 11/<strong>12</strong> LCP improvement Plan,<br />
including:<br />
Evidence of engagement of staff<br />
through ongoing training sessions <strong>and</strong>/<br />
or meetings with District Nurses, team<br />
leaders, community matrons<br />
End of Life Facilitator <strong>and</strong>/or Link<br />
Nurses to be informed of all new EoLC<br />
patients within 24 hours of referral to<br />
the service<br />
Process to ensure proactive case<br />
finding of EoLC patients on ACN<br />
caseload<br />
The <strong>report</strong><br />
has been<br />
produced<br />
which<br />
demonstrates<br />
all the<br />
requirements<br />
listed.<br />
Local data<br />
Improving the 0-5 year<br />
pathway for children<br />
Development of a systematic approach<br />
to recording the 0-5 year old pathway<br />
developed in 2010/11.<br />
A systematic<br />
approach<br />
has been<br />
developed<br />
This CQUIN is also about patient<br />
safety<br />
58 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
CQUIN<br />
What did we have to do<br />
Did we<br />
achieve it<br />
What is the evidence<br />
New Birth Visits at 14 days to be 100%<br />
New Birth Visits at 21 days to be 100%<br />
8-10 month Development Checks<br />
to be 75%<br />
Over all areas<br />
90% was<br />
achieved<br />
Local data<br />
27 month Development Checks to be<br />
75%<br />
Specialist CQUINS<br />
Neonatal Intensive Care<br />
(NICU) CQUIN<br />
Reduction in length of stay in NICU<br />
Increase the number of outcome<br />
assessments at 2 years of age<br />
Yes<br />
Yes<br />
Local data<br />
Local data – measure was on<br />
appointments issued<br />
HIV<br />
Improve involvement of HIV patients in<br />
decisions about their care<br />
Yes<br />
Local data demonstrated an<br />
increase in all areas<br />
Increase the numbers of HIV positive<br />
patients consenting to GP notification<br />
Yes<br />
Increase the numbers of HIV positive<br />
patients consenting, letter sent to GP<br />
Yes<br />
Reports from clinical services demonstrating<br />
effectiveness<br />
First response duty team (FRDT)<br />
Members of the FRDT work both in hospital <strong>and</strong> the<br />
community, their aims are:<br />
• Rapid assessment of patients in the Emergency<br />
Department <strong>and</strong> the Acute Care Unit (ACU) to facilitate<br />
rapid, safe discharge from hospital <strong>and</strong> prevent<br />
unnecessary admissions to hospital.<br />
• Rapid assessment of patients in the community (these<br />
patients are usually referred to FRDT by their GP) to<br />
assist in keeping them at home <strong>and</strong> prevent unnecessary<br />
admissions to hospital.<br />
An audit carried out by the team this year looked at their<br />
activity between June <strong>and</strong> November <strong>2011</strong> <strong>and</strong> compared<br />
this with previous data from June to November 2009:<br />
• There has been a 19% increase in patients being seen<br />
by FRDT in the Emergency Department (ED) to prevent<br />
unnecessary admission to hospital.<br />
• There has been an increase of 4% in the patients<br />
discharged home from the ED when seen by FRDT, this is<br />
from 82% to 86%.<br />
• There has been a 67% increase in community referrals<br />
(patients seen urgently by FRDT at home) in the last two<br />
years. GPs know of the service <strong>and</strong> are using it to help<br />
their patients.<br />
• There has been a 10% increase in the number of<br />
patients kept at home when seen urgently in the<br />
community by FRDT, this is from 87% to 97%.<br />
• The team has seen a 13.7% increase in total referrals for<br />
their expertise, from 2009/10 to <strong>2011</strong>/<strong>12</strong>.<br />
FRDT are instrumental in a multiagency group reviewing<br />
patients that frequently attend the ED, initial figures have<br />
shown that patients discussed at this group <strong>and</strong> actions<br />
taken to support them has resulted in a 42% reduction in<br />
the frequency of attendance to the ED in this patient group<br />
from 2010 to <strong>2011</strong>.<br />
This indicates that the work of FRDT <strong>and</strong> the frequent<br />
attenders group is assisting people to be cared for in the<br />
most effective way <strong>and</strong> helping patients to stay at home<br />
unless there is an overriding clinical need for them to be<br />
admitted to hospital.<br />
HIV team<br />
There is a project that has been running for two years, run<br />
by one of the HIV liaison nurses <strong>and</strong> a TB outreach worker,<br />
to de-stigmatise perceptions of HIV <strong>and</strong> TB in Hackney’s<br />
faith communities.<br />
The aim of the project team is to normalise discussion<br />
around HIV <strong>and</strong> TB within traditionally hard-to-reach faith<br />
groups, with the expectation that this will make routine<br />
screening for both conditions more acceptable <strong>and</strong> improve<br />
rates of early disease detection.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 59
QUALITY ACCOUNT<br />
To support this, they aim to develop culturally appropriate<br />
information about HIV <strong>and</strong> TB, in terms of signs <strong>and</strong><br />
symptoms, diagnosis <strong>and</strong> treatment, <strong>and</strong> to train peer<br />
educators.<br />
This year’s <strong>report</strong> from the team carrying out the work<br />
indicates a number of points.<br />
• They have used all networking opportunities to access<br />
groups of people <strong>and</strong> talk about TB <strong>and</strong> HIV. In some<br />
cases the team has been asked back to develop a<br />
relationship with specific groups.<br />
• Achieving their aims <strong>and</strong> objectives, this year has<br />
been harder <strong>and</strong> slower than they anticipated. The<br />
most successful work has been done with the Turkish<br />
<strong>and</strong> Polish communities, which looks as if it will be<br />
sustainable beyond the life of the project.<br />
• In certain ways, the team have strayed from their original<br />
objective of working exclusively with faith communities,<br />
but they have gone into areas where the need is<br />
greatest.<br />
• The demographic recording includes asking everyone<br />
what their religion is, <strong>and</strong> no-one has objected to being<br />
screened for HIV or TB on the grounds of faith or stigma,<br />
so far.<br />
• Because for many populations in Hackney, faith <strong>and</strong><br />
culture are synonymous, the team had anticipated<br />
that pathways into communities would be via clerics,<br />
churches <strong>and</strong> mosques. This past year has shown other<br />
access points, such as the women’s coffee mornings, the<br />
team will be exploring these during the next year.<br />
The team have also managed to gain some further grant<br />
money for equipment to help them run their Wednesday<br />
evening clinic at a homelessness drop-in centre run by<br />
North London Action for the Homeless.<br />
Detecting TB <strong>and</strong> HIV early enables staff to manage<br />
the patient as effectively as possible, reduce the costs<br />
of treatment <strong>and</strong> help to reduce the risk of onward<br />
transmission.<br />
Critical care outreach team (CCOT)<br />
This team is made up of experienced critical care nurses,<br />
whose purpose is to:<br />
• avert admission of patients to the Intensive Care Unit<br />
(ICU)<br />
• facilitate transfers of patients from the ICU<br />
• transfer critical care skills to ward teams.<br />
The team ran a survey in April <strong>2011</strong> to identify the views<br />
of staff that used their services, to assist with the care of<br />
acutely ill patients. The team had a 75% response rate to<br />
their questionnaire.<br />
100% of staff knew how to contact CCOT <strong>and</strong> 95% of<br />
them had done so. 96% of staff thought that the CCOT<br />
were supportive <strong>and</strong> helpful to them.<br />
Of concern was that 43% of staff felt that staff in their<br />
clinical area lacked the skills to care for an acutely sick<br />
patient, but that the members of CCOT had made a<br />
difference to this knowledge deficit in 85% of cases.<br />
Staff also thought that through the team’s efforts,<br />
particularly teaching, they had enabled the ward staff<br />
to reduce risks for deteriorating patients <strong>and</strong> improved<br />
the care of patients being transferred to a ward from the<br />
Intensive Care Unit.<br />
Staff commented as part of the survey that they would like<br />
more teaching <strong>and</strong> training about the deteriorating <strong>and</strong> the<br />
unwell patient. CCOT are currently reviewing what further<br />
help <strong>and</strong> support they can offer staff within their current<br />
resources.<br />
Training on the deteriorating <strong>and</strong> unwell patient is provided<br />
to all newly qualified nurses <strong>and</strong> junior doctors in the Trust’s<br />
Simulation Centre. This training is evaluated well particularly<br />
the aspect of nurses <strong>and</strong> doctors learning together.<br />
Readmission rates<br />
We monitor readmissions to hospital within 30 days of<br />
the last discharge it is essential for patients that when they<br />
are ready to go home everything is in place so that they<br />
can look after themselves, with appropriate community<br />
support <strong>and</strong> not have to return to hospital. Our current<br />
readmission rate is 6.9% (this was calculated over the year).<br />
Readmission to hospital is an issue across the county <strong>and</strong><br />
reducing the rate will be one of our priorities for the year<br />
ahead, in line with the QUEST programme.<br />
Patient Experience: a good experience for<br />
patients <strong>and</strong> staff<br />
Improving the experience patients have when they are<br />
treated remains a high priority.<br />
Patients’ experience can be positive or negative <strong>and</strong> we<br />
want <strong>and</strong> need feedback on all types of experience from<br />
our patients. We use this information to support services,<br />
change them where necessary, <strong>and</strong> in the case of new<br />
services, set them up with patients’ input.<br />
Priority 3 – Further improve the experience of our<br />
patients – increase the number of patients who answer<br />
“Yes always” to the question posed in the national patient<br />
survey: Overall, did you feel you were treated with respect<br />
<strong>and</strong> dignity while you were in the hospital<br />
Our score remained the same in both 2009 <strong>and</strong> 2010 at<br />
68%.<br />
60 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
There is still work to be done in terms of a greater<br />
percentage of “yes always“ answers in the patient survey<br />
which is a publicly scrutinised document <strong>and</strong> used to<br />
compare our Trust to others in the country.<br />
Our target for the year was to improve this response rate by<br />
at least 3%.<br />
We did not achieve this target – our percentage from the<br />
patients responses in the national inpatients survey was<br />
66% for “yes always” which is a decrease compared to<br />
previous years. There is insufficient information in the PET<br />
data to add information from another source to this data.<br />
However the information from the maternity survey is<br />
positive (see page 65 for details)<br />
Even though we did not achieve this specific priority we<br />
are retiring it from the Quality Account because the need<br />
to ensure patients are treated with dignity <strong>and</strong> respect<br />
underpins the patients’ experience strategy <strong>and</strong> the three<br />
campaigns within the strategy. Improvements in patients’<br />
experience in the Trust <strong>and</strong> their responses to this question<br />
in the national survey will be managed <strong>and</strong> improved<br />
through the patients experience strategy. We think that this<br />
approach will work more effectively than having this as a<br />
single Quality Account priority.<br />
Local, more frequent surveys will be undertaken to ensure<br />
that the patients’ experience of dignity <strong>and</strong> respect in all<br />
clinical areas is feedback to staff regularly, so actions can be<br />
taken quickly to address any concerns that are raised. These<br />
surveys will be monitored by the Patient Experience <strong>and</strong><br />
Engagement Committee.<br />
Priority 4 - Increase involvement <strong>and</strong> engagement of the<br />
local community in planning our services <strong>and</strong> developing<br />
the Trust.<br />
Develop the new strategy with key stakeholders for patient<br />
<strong>and</strong> public involvement. Improve communication <strong>and</strong><br />
feedback from members of the community that are not<br />
members of the Foundation Trust.<br />
Strategy<br />
The <strong>Homerton</strong> Patient Experience Strategy has been<br />
developed following a large listening exercise where the<br />
views of patients, users, members, staff <strong>and</strong> Governors<br />
were sought. Often, informing users of developments is<br />
mistaken for involving users in developments. This strategy<br />
aims to ensure users are involved in designing solutions to<br />
issues which arise, within the constraints of commissioning<br />
<strong>and</strong> financial frameworks. The strategy was launched in<br />
September <strong>2011</strong>.<br />
The aims of the strategy are:<br />
• to ensure patients <strong>and</strong> their families receive an<br />
experience that not only meets but exceeds their<br />
expectations of services at the Trust<br />
• to enable to maintain <strong>and</strong> increase public confidence<br />
<strong>and</strong> to sustain its reputation as a health care provider of<br />
choice <strong>and</strong> for that to be reflected in an improvement in<br />
the national patient survey scores<br />
• to demonstrate that we are able to listen <strong>and</strong> respond<br />
to the views of patients, their families <strong>and</strong> the local<br />
community to drive service improvements<br />
• for the Trust to meet its regulatory <strong>and</strong> statutory<br />
requirements in relation to patient <strong>and</strong> public<br />
involvement.<br />
There are three campaigns as part of the strategy:<br />
Campaign One: Delivering Thoughtful Care<br />
Campaign Two: Leaving our care with confidence<br />
Campaign Three: Getting the Right Information<br />
Each Division is working to demonstrate real improvements<br />
for patients in these key areas. Over the coming year<br />
the Patient Experience Strategy will provide a successful<br />
framework to enable patients, not only to feel more<br />
involved in the Trust, but to receive the best possible<br />
experience whilst in our care.<br />
Engagement<br />
Engaging our patients, the public, members, staff <strong>and</strong><br />
stakeholders in the planning <strong>and</strong> delivery of high quality<br />
services is key to our model of improving the patient<br />
experience. Within the strategy, engagement is divided into<br />
two separate activities<br />
• Gathering feedback<br />
• Building involvement to improve services<br />
The information that we can use to transform services<br />
comes from the experiences of people using those services.<br />
A ‘User Engagement Group’ is to be set up which will work<br />
closely with the Council of Governors to develop new <strong>and</strong><br />
innovative ways to involve <strong>and</strong> elicit views from a broad<br />
spectrum of users <strong>and</strong> staff.<br />
One example is organising large community events<br />
where people will have the opportunity to hear about<br />
developments planned within the Trust <strong>and</strong> give their views<br />
or active support.<br />
The user engagement group will <strong>report</strong> into the Patient<br />
Experience <strong>and</strong> Engagement Committee.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 61
QUALITY ACCOUNT<br />
Feedback<br />
The Patient Feedback Committee works proactively <strong>and</strong> in<br />
partnership with our Governors, members, patients <strong>and</strong><br />
the wider community to learn from the patient experience;<br />
identifying themes from feedback <strong>and</strong> <strong>report</strong>ing them to<br />
Patient Experience <strong>and</strong> Engagement Committee for further<br />
action.<br />
Our patient feedback strategy includes a programme of<br />
planned audits within our three clinical divisions using the<br />
Picker Institute portable h<strong>and</strong>-held electronic devices. The<br />
survey period will be for one month followed by action<br />
planning <strong>and</strong> then a repeat survey.<br />
Currently we are gathering feedback from people using<br />
the following: patient questionnaires, staff questionnaires<br />
<strong>and</strong> mealtime surveys. These are carried out by <strong>Homerton</strong><br />
Helper volunteers. Patients are also telephoned after<br />
discharge from hospital so we can to gather their views<br />
about their experience of care.<br />
These surveys began at the end of February 20<strong>12</strong>. So far<br />
we have gathered views from:<br />
• 206 patients in outpatient clinics<br />
• 20 responses from children’s community services<br />
• 113 from patients talking about eating <strong>and</strong> drinking<br />
• 55 inpatients, <strong>and</strong><br />
• 21 staff surveys.<br />
Monthly <strong>report</strong>s are sent to each Division for discussion <strong>and</strong><br />
the implementation of any actions.<br />
Because we have achieved this priority (the implementation<br />
of the strategy) we are retiring it as a Quality Account<br />
priority. The strategy is a three year plan, progress will be<br />
monitored by the Patient Experience <strong>and</strong> Engagement<br />
Committee chaired by the Associate Director: Patient<br />
Experience.<br />
The Quality Account priorities for the coming year have<br />
been mapped to the relevant; patient experience strategy<br />
campaign, Trust objective <strong>and</strong> element of Quest. This<br />
mapping demonstrates our commitment to working<br />
collaboratively towards an essential goal – safe, effective<br />
<strong>and</strong> thoughtful care.<br />
Face-to-face patient feedback day in Outpatients<br />
A survey was carried on 7 July <strong>2011</strong> in the main entrance<br />
of the hospital <strong>and</strong> in Starlight Ward (our children’s ward).<br />
Patients were invited to sit with staff <strong>and</strong> discuss set<br />
questions on their experience in Outpatients that day.<br />
Outpatient managers, reception staff <strong>and</strong> nursing assistants<br />
helped to collect the feedback.<br />
Staff actively asked patients to participate rather than just<br />
wait for patients to come to them. 83 out of a possible 904<br />
patients gave feedback on their Outpatient visit; this was<br />
9% of all patients attending an outpatient appointment<br />
that day.<br />
The results were positive, some areas for improvement were<br />
identified <strong>and</strong> a follow up survey is planned for July 20<strong>12</strong> to<br />
ensure that recommendations have been actioned.<br />
Introduction of the Purple Book for patients with<br />
learning difficulties<br />
Seven hundred copies of the Purple Book - which is<br />
designed for patients to be able to communicate clearly<br />
with staff - have been distributed across Hackney. Positive<br />
feedback has been given by people with learning disabilities<br />
to the work done by <strong>Homerton</strong> over the past year.<br />
The Trust web site has an enabled map showing the<br />
route to the hospital from the train station in photos<br />
<strong>and</strong> plain text. The route was photographed <strong>and</strong> the<br />
map was developed by Hackney mappers, who all have<br />
learning disabilities. This map was tested by the Camden<br />
easy information group. Please follow this link for further<br />
information:<br />
http://enabledmaps.com/tool/index.php/view/map/a-stepfree-route-from-homerton-overl<strong>and</strong>-station-to-homertonhospital<br />
62 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Patient experience CQUINS<br />
Table <strong>12</strong> shows the Trust position against the patient experience CQUINS<br />
Table <strong>12</strong>: Patient experience CQUINS<br />
CQUIN<br />
Goal<br />
Did we<br />
achieve<br />
it<br />
What is the evidence<br />
National<br />
Improve the experience<br />
of patients being<br />
cared for at <strong>Homerton</strong><br />
(measured by answers<br />
to five specific questions<br />
in the National Patient<br />
Survey) that are about<br />
the over arching theme<br />
of “responsiveness to<br />
personal needs”<br />
We were asked to improve the<br />
answers to these questions in the<br />
national survey by 5%<br />
1. Were you involved as much as<br />
you wanted to be in decisions about<br />
your care <strong>and</strong> treatment<br />
2. Did you find someone on the<br />
hospital staff to talk to about your<br />
worries <strong>and</strong> fears<br />
3. Were you given enough privacy<br />
when discussing your condition <strong>and</strong><br />
treatment<br />
No<br />
Results in the in patient survey<br />
The “yes definitely” response had<br />
gone down by 1% i<br />
The “yes definitely” response had<br />
gone down by 5% i<br />
The “yes definitely” response had<br />
gone down by 1% i<br />
4. Did a member of staff tell you<br />
about medication side effects to<br />
watch for when you went home<br />
The “yes completely” response had<br />
gone down by 6% i<br />
5. Did hospital staff tell you who to<br />
contact if you were worried about<br />
your condition or treatment after<br />
you left hospital<br />
The “yes” response to t his<br />
question had gone up by 6% h<br />
<strong>Homerton</strong> specific<br />
Maternity patient<br />
experience (in the<br />
maternity patient survey)<br />
We focused on out patients<br />
responses to five questions in the<br />
maternity survey<br />
1. Percentage of women who have<br />
a named midwife documented on<br />
notes – currently approx 30% would<br />
like to see this rise to 50% over this<br />
year<br />
Yes<br />
We commissioned the national<br />
maternity survey to be carried out<br />
again just with <strong>Homerton</strong> patients.<br />
83% this is considerable<br />
improvement<br />
h<br />
2. Increase numbers of women who<br />
confirm having the opportunity for<br />
skin to skin contact following birth<br />
currently 72% would like to see that<br />
increase by 8%<br />
79% of women had skin to skin<br />
contact - this is an increase of 5%.<br />
3. Increase the numbers of women<br />
sutured within 1hr currently 55%<br />
increase to 65%<br />
Results show only 6% of women<br />
waited for more than an hour for<br />
sutures – this is below the national<br />
result of 11%<br />
84% were sutured within an hour<br />
h<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 63
QUALITY ACCOUNT<br />
CQUIN<br />
Goal<br />
Did we<br />
achieve<br />
it<br />
What is the evidence<br />
<strong>Homerton</strong> specific<br />
Maternity patient<br />
experience (in the<br />
maternity patient survey)<br />
4. Inconsistency in feeding advice<br />
given in postnatal period – only 56%<br />
women said advice consistent – see<br />
this increase to 66%<br />
5. Only 68% of women said they<br />
were treated with dignity & respect<br />
–this has improved since 2007 survey,<br />
however would like to see this<br />
increase to 75% over the year<br />
Yes<br />
71% of women felt they had<br />
consistent advice on feeding.<br />
h<br />
This has increased to 86% which<br />
is over the expected increase <strong>and</strong><br />
a really positive reflection on the<br />
service.<br />
h<br />
Local patient<br />
experience (hospital)<br />
Aim to achieve a 85% “Yes”<br />
for each of the following questions:<br />
No<br />
This information was collected using<br />
our new h<strong>and</strong> held devices managed<br />
by the Picker institute<br />
1. Were you greeted in a friendly<br />
manner by a member of staff when<br />
you arrived<br />
81%<br />
2.When you first arrived were you<br />
made to feel welcome by hospital<br />
staff<br />
80%<br />
3.Have hospital staff asked you how<br />
you would like to be addressed (For<br />
example by your first name or title)<br />
35%<br />
4.Do the nurses caring for you keep<br />
you informed about what is going to<br />
happen each day<br />
44%<br />
5.As far as you know, do hospital<br />
staff wash or clean their h<strong>and</strong>s<br />
between touching patients<br />
79%<br />
In the community<br />
patient experience<br />
Implement a structure to enable the<br />
patient experience in the community<br />
to be captured.<br />
Yes<br />
The survey was undertaken – the<br />
results are in the process of being<br />
analysed.<br />
Carry out an assessment of patients<br />
experience in the community aiming<br />
for an 80% positive response rate<br />
The only element not achieving 80%<br />
was:<br />
“Did staff ask you what you want to<br />
be called”<br />
The positive response rate to this<br />
question was 23%.<br />
This is the same question that<br />
received the lowest score when<br />
asked of patients in hospital.<br />
64 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Specialist CQUIN<br />
Regional Neurological<br />
Rehabilitation Unit<br />
(RNRU)<br />
May<br />
baseline<br />
Data collected on PET from May<br />
to September demonstrated the<br />
following improvements<br />
up to September.<br />
A patient feedback<br />
survey was required to be<br />
carried out covering the<br />
following five questions<br />
Were staff friendly, approachable <strong>and</strong><br />
sensitive to your needs<br />
How long did you usually wait after<br />
using the call bell<br />
71%<br />
47%<br />
h 84%<br />
h 62%<br />
Were your family <strong>and</strong> visitors made to<br />
feel welcome<br />
88%<br />
h 95%<br />
Were you satisfied with the overall<br />
cleanliness of the ward<br />
82%<br />
h 91%<br />
Did you receive adequate assistance<br />
with choosing <strong>and</strong> eating your meal<br />
79%<br />
h 89%<br />
National inpatient survey<br />
The Quality Health National Inpatient Survey was sent to<br />
850 patients who were discharged from our acute hospital<br />
in June, July or August <strong>2011</strong>. The expected response<br />
rate for the National Patient Survey is 60% (approx 500<br />
responses)<br />
<strong>Homerton</strong> had responses from 330 patients - a response<br />
rate of 41%. Our results have to be read bearing this in<br />
mind.<br />
From the results, the overarching areas where the survey<br />
indicates a review <strong>and</strong> possible actions may be required are:<br />
• communication between staff <strong>and</strong> patients<br />
• the involvement of patients in their care<br />
• the type <strong>and</strong> quality of information that is given to<br />
patients particularly pre operative <strong>and</strong> post operative.<br />
• delays to discharge.<br />
All of these elements, that patients indicated they<br />
are concerned about will be addressed by the Patient<br />
Experience Strategy campaigns<br />
Campaign One: Delivering Thoughtful Care<br />
Campaign Two: Leaving our care with confidence<br />
Campaign Three: Getting the Right Information<br />
Maternity<br />
In August/September <strong>2011</strong> a survey of women’s experience<br />
in maternity services was carried out.<br />
The survey was completed by 154 women <strong>and</strong> covered<br />
all aspects of their care during pregnancy, delivery <strong>and</strong> the<br />
post natal period.<br />
The five questions being monitored for the CQUIN are<br />
detailed in table <strong>12</strong> above. The survey results demonstrated<br />
significant improvements in certain areas of care; there was<br />
considerable reduction in the time women were waiting for<br />
suturing following delivery, women felt they were getting<br />
consistent feeding advice <strong>and</strong> an increased number of<br />
women had a named midwife.<br />
Though the number of women stating they had an<br />
opportunity for skin to skin contact immediately after<br />
delivery was higher than the previous survey, this did not<br />
improve as much as we were anticipating.<br />
The areas that we aim to address over the coming year are:<br />
• increasing the consistency of information given to<br />
women prior to consenting for tests, this has already<br />
been discussed at the Hackney Maternity Board<br />
meeting which is chaired by a local GP. GPs have equal<br />
responsibility, with midwives, for this aspect of ante natal<br />
care.<br />
• improving consistency in the advice given by midwives<br />
<strong>and</strong> carers regarding women breast or bottle feeding<br />
their babies<br />
• looking at ways we can increase the percentage of<br />
women who feel that in the postnatal period they were<br />
treated with respect <strong>and</strong> kindness.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 65
QUALITY ACCOUNT<br />
The final survey <strong>report</strong> will be shared with staff <strong>and</strong> action<br />
plan developed to address areas of concern. The action<br />
plan will by monitored at the Maternity Risk Management<br />
<strong>and</strong> Clinical Governance Committee.<br />
Outpatients<br />
The National Outpatient Survey was carried out between<br />
June <strong>and</strong> October <strong>2011</strong>, a questionnaire was sent to<br />
patients who had recently attended an outpatient<br />
appointment for each NHS trust in Engl<strong>and</strong>. Responses<br />
were received from 355 patients at <strong>Homerton</strong>.<br />
Our results showed improvements over the last year in:<br />
• choice of appointment time <strong>and</strong> waiting time (for an<br />
appointment)<br />
• answers that could be understood from the doctor by<br />
the patient<br />
• involvement in decisions about their care <strong>and</strong> treatment.<br />
Patients’ trust <strong>and</strong> confidence in the doctors /other health<br />
professionals also improved since last year but other Trusts<br />
had improved more. We are monitoring this aspect of<br />
patient experience using the surveys in our h<strong>and</strong> held Picker<br />
devices.<br />
One of our lowest scores were about patients not being<br />
seen on time for their appointment <strong>and</strong> the lack of<br />
information about whether a clinic was running late.<br />
Waiting times are monitored <strong>and</strong> this information is feed<br />
back to the relevant division <strong>and</strong> the consultants so that<br />
actions can be taken to reduce waiting times. We now have<br />
boards which display information in order that patients<br />
know if there is a delay <strong>and</strong> an update announcement is<br />
given every 15 minutes.<br />
Our scores for the outpatient environment were:<br />
8.5 /10 for describing the Outpatients Department as clean.<br />
7.4 /10 for describing the toilets in the Outpatients<br />
Department as clean.<br />
We have refitted the toilets <strong>and</strong> ensure they are checked<br />
regularly by the domestic staff to ensure they are kept as<br />
clean as possible. We have also installed new chairs in the<br />
waiting area.<br />
In both our community <strong>and</strong> hospital based sexual health<br />
clinical patients responded as follows:<br />
• 95% of them said they were made to feel welcome by<br />
reception staff<br />
• 95% they had trust <strong>and</strong> confidence in the staff treating<br />
them<br />
• 95% said they were treated with dignity <strong>and</strong> respect<br />
• <strong>and</strong> >95% would recommend the service to family or<br />
friends<br />
• the only question where we scored in the 80% range<br />
was patients view of whether staff had explained their<br />
medications <strong>and</strong> any possible side effects to them.<br />
This positive feedback has been maintained from the year<br />
before <strong>and</strong> demonstrates the consistently high quality care<br />
that is provided for all patients in our sexual health clinics.<br />
Patient Experience Tracker (PET)<br />
During the year our contract with Dr Foster Intelligence<br />
(who provided the services for our PET trackers) came to<br />
an end. We have data from the first six months of the year<br />
April to September <strong>2011</strong>. Almost 5500 patients answered<br />
questions via the PET. These responses are amalgamated<br />
information from across the Trust <strong>and</strong> do not relate to any<br />
particular department.<br />
A selection of the questions they responded to with their<br />
views is below:<br />
Figure 10: PET question “Were staff friendly, approachable<br />
<strong>and</strong> sensitive to your needs”<br />
82% stated “yes”<br />
Yes - 1041<br />
Most of time - 70<br />
Some staff were - 57<br />
No - 48<br />
Survey in sexual health<br />
A survey of patients’ experiences of using sexual health<br />
services in North East London was carried out in June <strong>2011</strong>.<br />
This was the third year the audit had been carried out.<br />
Between the sexual health clinic at the acute site <strong>and</strong> those<br />
in the community we see the highest proportion of patients<br />
in the sector.<br />
66 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Figure 11: PET Question – “Were you satisfied with the<br />
overall cleanliness of the ward/ department”<br />
98% of people said yes<br />
Figure <strong>12</strong>: PET question – “Did you have confidence <strong>and</strong><br />
trust in the nurses treating you”<br />
75% said yes always<br />
Yes - 2169<br />
No - 47<br />
Yes - 2169<br />
Some staff - 47<br />
No - 67<br />
Figure 13: PET question – “Overall how would you rate the<br />
care you received”<br />
69% of patients said excellent or very good<br />
Excellent - 451<br />
Very good - 317<br />
Good - 197<br />
Fair - 88<br />
Poor - 49<br />
Figure 13 shows that the majority of patients responding to<br />
this question thought their care was; excellent, very good<br />
or good. But <strong>12</strong>% of patients thought that their care was<br />
fair or poor. This is the same percentage as last year. In<br />
the PET responses this equates to 137 patients who were<br />
disappointed with the care they received between April<br />
<strong>and</strong> September <strong>2011</strong>. It is imperative that we receive this<br />
feedback in order to be able to take action to reduce that<br />
number of patients who have had a fair or poor experience<br />
in hospital.<br />
Our new contract for patient feedback using h<strong>and</strong> held<br />
devices is with Picker – these devices are currently being<br />
introduced into the Trust.<br />
Patient related outcome measures (PROMS)<br />
Patient related outcome measures (PROMs) measure quality<br />
from the patient perspective. Initially they covered four<br />
clinical procedures <strong>and</strong> calculate the improvements to a<br />
patients health, as they perceive it, after surgical treatment<br />
using pre <strong>and</strong> post operative surveys.<br />
The four procedures are:<br />
• hip replacements<br />
• knee replacements<br />
• hernia<br />
• varicose veins (we do not carry out this surgery at<br />
<strong>Homerton</strong>).<br />
From April 2010 to March <strong>2011</strong> there were 332 patient<br />
episodes for which a patient could complete a pre operative<br />
questionnaire – 188 did so, this a 56.6% participation rate.<br />
Patients undergoing orthopaedic surgery showed the best<br />
response rates. The participation rate across Engl<strong>and</strong> was<br />
69.8%.<br />
Following their operation we sent 93% of patients a follow<br />
up questionnaire – 70.9% of patients returned these<br />
(national average response rate 89%).<br />
However PROMS can only calculate the patient’s perceived<br />
improvement in their health following surgery when both<br />
questionnaires have been fully completed. Our numbers<br />
of questionnaires that could be used for these calculations<br />
were under the threshold to provide meaningful data for<br />
hernias <strong>and</strong> hip replacements.<br />
Patients that had knee replacements demonstrated<br />
that they viewed their health had improved following<br />
their operation in line with the national average level of<br />
improvement.<br />
For April to December <strong>2011</strong> we had 280 patients eligible<br />
to be part of PROMS (provisional data), our response rate<br />
to the first questionnaire was 46% - this is in contrast to<br />
the national response rate of 72.5%. Again the patients<br />
who returned the most questionnaires were those<br />
having orthopaedic surgery, 80% for those having knee<br />
replacements. It is likely that this response rate is high as<br />
the Clinical Nurse Practitioner for orthopaedics is involved<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 67
QUALITY ACCOUNT<br />
in each patient’s pre-operative preparation <strong>and</strong> explaining<br />
PROMs is part of this process.<br />
Our overall response rate for patients completing the<br />
second questionnaire was 55% compared to the national<br />
average of 64%. Our response rate is stable at this level.<br />
However in this time period there were not enough fully<br />
completed questionnaires to extract data.<br />
Source for information:<br />
http://www.hesonline.nhs.uk/Ease/servlet/ContentServersit<br />
eID=1937&categoryID=1632<br />
Complaints<br />
There have been more formal complaints from patients in<br />
<strong>2011</strong>/<strong>12</strong> than in the previous two years; the Trust received<br />
253 complaints in <strong>2011</strong>/<strong>12</strong>. Figure 14 shows comparisons<br />
with previous years Trust wide.<br />
Five cases were reviewed by the Ombudsman, in four<br />
cases no action was taken, the fifth case is currently being<br />
assessed.<br />
Figure 14: Total formal complaints April 2009 – March 20<strong>12</strong><br />
by month<br />
35<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar<br />
Figure 15: shows the complaint figures cumulatively over<br />
the year<br />
300<br />
250<br />
200<br />
150<br />
100<br />
2009/10 2010/11 <strong>2011</strong>/<strong>12</strong><br />
The complaints were about the following concerns:<br />
Complaints by type<br />
Area of concern<br />
Number<br />
All aspects of clinical treatment 110<br />
Attitude of staff 44<br />
Communication/information to patients<br />
(written <strong>and</strong> oral) 25<br />
Appointments, delay/cancellation (out-patient) 19<br />
Admissions, discharge <strong>and</strong> transfer arrangements 13<br />
Failure to follow agreed procedure 11<br />
Others 31<br />
Total: 253<br />
They were distributed over the following service areas<br />
Complaints by area<br />
Service Area<br />
Number<br />
Inpatient 105<br />
Outpatient 92<br />
Maternity 23<br />
A&E 16<br />
Community Health 15<br />
Elderly 4<br />
Totals: 253<br />
Further information on complaints can be found in the<br />
<strong>Annual</strong> Report<br />
Patient Advice <strong>and</strong> Liaison Service (PALs)<br />
The PALs service received 1187 enquiries during the year –<br />
this is 87 more than last year.<br />
These enquiries came from patients, carers, family members<br />
<strong>and</strong> members of the public.<br />
The top five enquiries are shown in figure 16:<br />
50<br />
0<br />
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar<br />
2009/10 2010/11 <strong>2011</strong>/<strong>12</strong><br />
68 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Figure 16: top 5 enquiries to PALs<br />
200<br />
180<br />
160<br />
140<br />
<strong>12</strong>0<br />
100<br />
80<br />
60<br />
40<br />
20<br />
0<br />
Communication<br />
Information<br />
requested<br />
Positive<br />
feedback<br />
Administration<br />
Attitude<br />
of staff<br />
The top five are the same topics as last year, it is gratifying<br />
to know that positive feedback about the Trust <strong>and</strong> staff<br />
remains in the top five. When combined, requests for<br />
information <strong>and</strong> positive feedback made up 20% of all<br />
PALs enquiries; this is marginally less than last year.<br />
Information from the PALs queries is reviewed at the weekly<br />
Complaints, Litigation, Incidents <strong>and</strong> PALs (CLIP) meeting to<br />
identify emerging themes (positive or negative).<br />
Actions are then taken forward to address any negative<br />
themes. For example in the last year there has been a focus<br />
on departments where problems with communication have<br />
been flagged up by the PALs enquiries.<br />
Single sex accommodation<br />
<strong>Homerton</strong> is committed to providing every patient with<br />
same sex accommodation, because it helps to safeguard<br />
their privacy <strong>and</strong> dignity at a time when they are often at<br />
their most vulnerable.<br />
Patients who are admitted to our hospital, will only share<br />
the room where they sleep with members of the same sex.<br />
Same sex toilets <strong>and</strong> bathrooms will be close to their bed<br />
area.<br />
Sharing with members of the opposite sex will only happen<br />
by exception based on clinical need; for example where<br />
patients need urgent specialist equipment such as in our<br />
cardiology ward or acute stroke unit. Any breaches of<br />
same sex accommodation have to be authorised by the<br />
senior manager on call to ensure all alternatives have been<br />
considered first. In the past year we have had only one<br />
breach – this affected six patients for a short amount of<br />
time.<br />
<strong>Homerton</strong> will not turn patients away just because a “rightsex”<br />
bed is not immediately available.<br />
We have 13 inpatient wards at <strong>Homerton</strong> (including<br />
Intensive Care <strong>and</strong> Paediatrics), two of these wards are<br />
entirely single sex; the remaining wards have male <strong>and</strong><br />
female patients cared for in single sex bays or rooms.<br />
In the last year the Trust has:<br />
• built privacy screens across the bays in; Edith Cavell Ward<br />
<strong>and</strong> part of the new Elderly Care Unit<br />
• reconfigured the Day Stay Unit so it now has separate<br />
male <strong>and</strong> female areas.<br />
Any breaches are <strong>report</strong>ed monthly to the Board of<br />
Directors <strong>and</strong> quarterly to the Council of Governors. We<br />
monitor complaints <strong>and</strong> PALS enquiries for issues related<br />
to mixed sex accommodation. This year’s responses from<br />
patients completing the National Inpatient Survey resulted<br />
in the following recommendation in the <strong>report</strong>:<br />
• Review progress on eliminating mixed gender rooms,<br />
bays <strong>and</strong> bathroom facilities in the light of information<br />
contained in the survey.<br />
This recommendation came from patients being unhappy<br />
that only the bay they slept in was single sex.<br />
An ‘Enter <strong>and</strong> View’ visit was carried out by representatives<br />
from the Hackney LINk in May <strong>2011</strong>, they visited two<br />
surgical wards: Thomas Audley, male surgical ward,<br />
Priestley, female surgical ward.<br />
In their <strong>report</strong> LINks identified as an area of concern on the<br />
visit to Thomas Audley Ward that there were two female<br />
patients. Due to bed pressures the end bay had been<br />
changed into an area for female surgical patients. The use<br />
of the end bay ensured that females did not have to cross<br />
the male bay to go to the bathroom <strong>and</strong> vice versa, the<br />
toilet near the bay was dedicated to female patients <strong>and</strong><br />
the signs on the doors were changed to indicate this.<br />
Since this visit the ward configurations have changed.<br />
All areas have been reviewed to see what actions can<br />
be taken. There are limits to the actions we can take<br />
considering the architecture of our hospital, but we are<br />
putting into place all we can.<br />
Feedback from staff<br />
This year staff gave us positive feedback in the staff survey,<br />
331 staff responded – our scores were in some cases<br />
within the top 20% of all trusts across the country. Our top<br />
four scores that ranked more positively than the national<br />
average were:<br />
• percentage of staff able to contribute towards<br />
improvements at work<br />
• quality of job design (clear job content, feedback <strong>and</strong><br />
staff involvement)<br />
• percentage of staff feeling satisfied with the quality of<br />
work <strong>and</strong> patient care they are able to deliver<br />
• support from immediate managers.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 69
QUALITY ACCOUNT<br />
Staff also <strong>report</strong>ed that 72% of them would be happy with<br />
the st<strong>and</strong>ard of care provided by this Trust if a friend or<br />
relative needed treatment. This is higher than the national<br />
average response of 62% to this question.<br />
Staff responses show that we were below the national<br />
average for acute trusts in the following areas:<br />
• percentage of staff experiencing harassment, bullying or<br />
abuse from patients<br />
• relatives or the public in last <strong>12</strong> months<br />
• percentage of staff suffering work-related stress in last<br />
<strong>12</strong> months<br />
• percentage of staff having equality <strong>and</strong> diversity training<br />
in last <strong>12</strong> months<br />
• percentage of staff experiencing discrimination at work<br />
in last <strong>12</strong> months.<br />
• there were four areas where staff experience had<br />
diminished since the 2010 survey, these were:<br />
• percentage of staff feeling pressure in last three months<br />
to attend work when feeling unwell<br />
• percentage of staff receiving job-relevant training,<br />
learning or development in last <strong>12</strong> months<br />
• percentage of staff suffering work-related stress in last<br />
<strong>12</strong> months<br />
• percentage of staff feeling there are good opportunities<br />
to develop their potential at work.<br />
An action plan has been developed to address these <strong>and</strong><br />
some other concerns raised by the staff survey. This action<br />
plan is part of the Trust’s overall Workforce Strategy.<br />
SECTION 5 – Quality improvement plans<br />
20<strong>12</strong> - 2013<br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust:<br />
Incorporating hospital <strong>and</strong> community health services,<br />
teaching <strong>and</strong> research.<br />
In this section of the <strong>report</strong> <strong>Homerton</strong> is setting out the<br />
plan for the coming year <strong>and</strong> how we intend to progress in<br />
order to improve the quality of care our patients receive.<br />
As we identified at the very beginning of the quality<br />
account we have six specific priorities for the coming year:<br />
SAFE<br />
Priority 1<br />
Reduce harm to patients caused by pressure ulcers, falls,<br />
catheter infections, falls <strong>and</strong> venous thrombo-embolism<br />
identified within the Safety Thermometer / Harm Free Care<br />
Programme.<br />
(Linked to Trust objective I, the NHS QUEST programme <strong>and</strong><br />
the Patient Experience Strategy Campaign One: Delivering<br />
thoughtful care)<br />
Priority 2<br />
Demonstrate improvements in safety by continuing to<br />
deliver a programme of work relating to: urgent care, end<br />
of life care <strong>and</strong> clinically led coding, using the St<strong>and</strong>ardised<br />
<strong>Hospital</strong> Mortality Indicator (SHMI) as a measure.<br />
(Linked to Trust objective I, the NHS QUEST programme <strong>and</strong><br />
the Patient Experience Strategy Campaign One: Delivering<br />
thoughtful care)<br />
EFFECTIVE<br />
Priority 3<br />
Ensure that, where national clinical guidelines have been<br />
produced by the National Institute for Health <strong>and</strong> Clinical<br />
Excellence (NICE) which are relevant to the care we provide,<br />
we can demonstrate we are using them in everyday<br />
practice.<br />
(Linked to Trust objective I <strong>and</strong> the Patient Experience<br />
Strategy Campaign One: Delivering thoughtful care)<br />
Priority 4<br />
Reduce hospital readmissions.<br />
(Linked to Trust objective I, III, IV, V, the NHS QUEST<br />
programme <strong>and</strong> the Patient Experience Strategy Campaign<br />
Two: Leaving or transferring from our care with confidence)<br />
70 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
THOUGHTFUL<br />
Priority 5<br />
Sharing care <strong>and</strong> treatment information with patients.<br />
(Linked to the Patient Experience Strategy Campaign Three:<br />
Getting the information right)<br />
Priority 6<br />
We will improve the effectiveness of discharge from our<br />
care.<br />
(Linked to the Patient Experience Strategy Campaign two;<br />
Leaving or transferring from our care with confidence)<br />
Priorities for quality improvement have also been identified<br />
by the commissioners that purchase services from us for the<br />
year ahead. The Commissioning for Quality <strong>and</strong> Innovation<br />
scheme (CQUIN) has identified elements of care where we<br />
must demonstrate improvement to be paid accordingly. The<br />
proportion of funding that CQUINS are worth has increased<br />
for 20<strong>12</strong>/13 to 2.5% of the Trust’s income (about £3.17<br />
million). This funding is dependent on the Trust achieving<br />
the improvements listed below.<br />
There are three levels of CQUIN; national, regional <strong>and</strong><br />
local that we will be working on in the next <strong>12</strong> months.<br />
Table 16 provides a summary of the CQUINs the Trust will<br />
be working on next year for acute care. Table 17 is the<br />
summary of community care CQUINS.<br />
Table 16: Commissioning for Quality <strong>and</strong> Innovation scheme<br />
(CQUIN) Targets 20<strong>12</strong>/13 acute care<br />
What are we going to do<br />
The details of these CQUINS are being established<br />
Which element of Quality does<br />
this relate to<br />
National 1. Venous Thrombo-embolism risk assessment Safety <strong>and</strong> effectiveness<br />
2. Dementia: identifying <strong>and</strong> assessing patients with dementia Safety <strong>and</strong> effectiveness<br />
Regional<br />
Local<br />
3. Safety thermometer –<br />
Reduce harm from : falls, pressure ulcers, urinary tract<br />
infections (patients with catheters) <strong>and</strong> VTE<br />
Baseline to be set in Q1<br />
4. Patient Experience –<br />
This is the same national patients experience CQUIN as the past<br />
two years improvement on five questions in the national survey<br />
5. Cancer Staging<br />
Details being negotiated<br />
6. Older People’s Care<br />
Details being negotiated<br />
7. Patient Experience in Maternity<br />
Details being negotiated<br />
8. Smoking Cessation<br />
Details being negotiated<br />
9. Discharge Communication<br />
Details being negotiated<br />
Safety<br />
Patient experience<br />
Safety <strong>and</strong> effectiveness<br />
Safety, effectiveness <strong>and</strong> experience<br />
experience<br />
effectiveness <strong>and</strong> experience<br />
Safety, effectiveness <strong>and</strong> experience<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 71
QUALITY ACCOUNT<br />
Table 17: Commissioning for Quality <strong>and</strong> Innovation scheme (CQUIN) Targets 20<strong>12</strong>/13 Community Care<br />
What are we going to do<br />
Local 1. Patient Experience –<br />
A local survey will be commissioned from the<br />
Picker Institute across all services.<br />
2. Discharge Communication<br />
Details being negotiated<br />
3. Smoking Cessation<br />
Details being negotiated<br />
4. Older People’s Care<br />
Details being negotiated<br />
Which element of Quality does this relate to<br />
Experience<br />
Effectiveness<br />
Experience<br />
Effectiveness<br />
Experience<br />
Safety, effectiveness <strong>and</strong> experience<br />
All of these elements will be measured throughout the<br />
year so that the Trust can show that it is improving the<br />
experience of the patients, their safety <strong>and</strong> the effectiveness<br />
of the services.<br />
We will <strong>report</strong> to the commissioners every month to<br />
demonstrate this improvement. Without reaching the<br />
agreed targets the Trust will not be paid the money the<br />
commissioners have attached to these elements of care.<br />
In the coming year we will also comply with all national<br />
requirements for improvements in quality. We will continue<br />
with our involvement in relevant national audit projects<br />
<strong>and</strong> maintain our local audit programme. We will carry<br />
on monitoring complaints <strong>and</strong> ensure that we learn from<br />
any adverse events. The Quality <strong>and</strong> Risk Department will<br />
support Trust staff in all aspects of quality improvement<br />
providing; help, support, training <strong>and</strong> guidance.<br />
How will we monitor progress on all these<br />
aspects of quality improvement<br />
All quality improvements; the Trust priorities <strong>and</strong> the<br />
CQUINS will have actions plans developed to address the<br />
requirements needed to implement them. The progress on<br />
these action plans will be monitored every two months by<br />
the Trust Quality Improvement Committee. This committee<br />
will <strong>report</strong> to the Trust Board of Directors.<br />
A half year update will be presented to the Board <strong>and</strong> the<br />
Council of Governors.<br />
72 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
SECTION 6 – Consultation <strong>and</strong> comment<br />
on the Quality Account<br />
Chief Executive Statement for <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong><br />
Foundation Trust Quality Account <strong>2011</strong>/<strong>12</strong><br />
NHS North East London <strong>and</strong> the City welcomes the opportunity to provide this statement on<br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> Foundation Trust’s Quality Account. We confirm that we have<br />
reviewed the information contained within the Account <strong>and</strong> checked this against data sources<br />
where this is available to us as part of existing contract/performance monitoring discussions <strong>and</strong><br />
is accurate in relation to the services provided.<br />
We have reviewed the content of the Account <strong>and</strong> confirm that this complies with the<br />
prescribed information, form <strong>and</strong> content as set out by the Department of Health. We believe<br />
that the Account represents a fair, representative <strong>and</strong> balanced overview of the quality of care<br />
at <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> Foundation Trust. We have discussed the development of this<br />
Quality Account with <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> Foundation Trust over the year <strong>and</strong> have<br />
been able to contribute our views on consultation <strong>and</strong> content.<br />
This Account has been reviewed within NHS North East London <strong>and</strong> the City by colleagues in<br />
commissioning, quality <strong>and</strong> clinical governance, Clinical Commissioning Groups (CCGs), as well<br />
as specialists in infection control <strong>and</strong> safeguarding.<br />
Overall we welcome the vision described within the Quality Account, agree on the priority areas<br />
<strong>and</strong> will continue to work with <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> Foundation Trust to continually<br />
improve the quality of services provided to patients.<br />
Alwen Williams<br />
Chief Executive<br />
NHS North East London <strong>and</strong> the City<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 73
QUALITY ACCOUNT<br />
Chairman, City of London Health <strong>and</strong> Social Care Scrutiny Sub<br />
(Community & Children’s Services) Committee<br />
The Rev’d Dr. Martin Dudley<br />
Melanie Mavers<br />
Head of Clinical Quality<br />
Quality <strong>and</strong> Risk Department<br />
1st Floor Brooksby House<br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
<strong>Homerton</strong> Row<br />
Hackney<br />
E9 6SR<br />
Dear Ms Mavers,<br />
Due to the level of other scrutiny issues that Members have been dealing with over the last<br />
two months, including the GP Choice Pilot, new Public Health responsibilities <strong>and</strong> LINk <strong>report</strong>s<br />
on Mental Health <strong>and</strong> <strong>Hospital</strong> Discharge from Bart’s <strong>and</strong> the London, the <strong>Homerton</strong> Quality<br />
Accounts have not been formally considered by the Health <strong>and</strong> Social Care Committee.<br />
However my officers have reviewed the <strong>accounts</strong> <strong>and</strong> have informed me that apart from<br />
improving the information on the usage of <strong>Homerton</strong> <strong>Hospital</strong>, <strong>and</strong> in particular Community<br />
Services provided by <strong>Homerton</strong>, by City residents we have no major concerns <strong>and</strong> are happy to<br />
endorse them.<br />
Yours sincerely,<br />
The Rev’d Dr. Martin Dudley,<br />
Chairman,<br />
City of London Health & Social Care Scrutiny Sub<br />
(Community & Children’s Services) Committee<br />
74 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Hackney LINk<br />
1. CQC inspection<br />
Hackney LINk congratulates <strong>Homerton</strong> on the generally favourable CQC Inspection which LINk members<br />
heard about at a Steering Group meeting. We also note that in one area where the CQC Inspection<br />
was less favourable, the RNRU, <strong>Homerton</strong> had already run a patient feedback survey between May <strong>and</strong><br />
September showing an improvement in patient responses on some of the issues identified.<br />
2. Patient safety<br />
Hackney LINk welcomes the work <strong>Homerton</strong> has done to improve Clinical Incident Reporting, which was the<br />
focus of work against this the first priority set for <strong>2011</strong>/<strong>12</strong>. However we also note<br />
• NEVER incidents increased from zero in 2010/11 to three in <strong>2011</strong>/<strong>12</strong> (<strong>and</strong> that only the <strong>2011</strong>/<strong>12</strong> figure is<br />
given in the <strong>report</strong>). We also note that the number of events covered by this category has increased this<br />
year.<br />
• An increase in the number of <strong>report</strong>ed falls, largely in the minor falls category, <strong>and</strong> that this is partly<br />
attributed to increased awareness of the requirement to <strong>report</strong> all incidents. We welcome the work<br />
on <strong>report</strong>ing, <strong>and</strong> would be keen to work with <strong>Homerton</strong> to look into any other possible causes of this<br />
increase.<br />
3. Dignity <strong>and</strong> respect<br />
We have some concerns that the Dignity <strong>and</strong> Respect priority has not been achieved but is being<br />
removed. There are several indicators in this <strong>report</strong> showing that this priority continues to be an issue,<br />
particularly the Patient Experience CQUINS data.<br />
Hackney LINk welcomes the response in the Quality Account to the issue of mixed wards picked up in the<br />
LINk’s May Enter <strong>and</strong> View, <strong>and</strong> the action to address this. A later visit to the Intensive Care Unit which<br />
<strong>Homerton</strong> has not had the chance to respond to, also found a mixed ward, <strong>and</strong> although this makes it more<br />
flexible from the hospital’s point of view we question if this is appropriate from the point of view of patient<br />
dignity <strong>and</strong> privacy, but recognise the work <strong>Homerton</strong> has done to reconfigure wards given the dem<strong>and</strong> for<br />
beds <strong>and</strong> the limits of the architecture.<br />
4. Patient Experience Strategy<br />
We welcome the other two str<strong>and</strong>s of the Patient Experience Strategy (Sharing Care <strong>and</strong> Treatment<br />
Information with patients, <strong>and</strong> Improving the effectiveness of discharge) being identified as priorities for<br />
20<strong>12</strong>/13.<br />
5. Sample comments from patients<br />
More than half the comments received by the LINk from patients using <strong>Homerton</strong> were favourable.<br />
Examples are:<br />
• “Great experience with <strong>Homerton</strong> <strong>Hospital</strong>. Good aftercare. I was an inpatient for five weeks”<br />
• “The nurse was amazing when I was first admitted to <strong>Homerton</strong> as I was very upset <strong>and</strong> crying.<br />
She comforted me <strong>and</strong> sat with me at night when I could not sleep”.<br />
The less favourable comments varied widely, with waiting times, noise at night from staff <strong>and</strong> the need for<br />
more advocacy being the only ones that came up more than once.<br />
Hackney LINk, May 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 75
QUALITY ACCOUNT<br />
Health in Hackney Scrutiny Commission for the <strong>Homerton</strong> Quality Account<br />
Comments<br />
The Commission would like it noted in reference to the Patient Experience CQUIN (table<br />
<strong>12</strong> on page 39) the results noted from the questions asked, match with the comments the<br />
Commission has repeatedly heard from members of the public that attend its regular meetings.<br />
The Commission expresses concern about the emphasis placed on the PET in what appears to<br />
be the main source of intelligence gathering of patient views <strong>and</strong> experience by the Trust. The<br />
Commission is of the opinion that this is largely getting the views of patients that are in contact<br />
with the service <strong>and</strong> very little from the wider population (people using the service are less likely<br />
to be critical). This being the case the Commission is keen to see the Trust continues to improve<br />
in this area <strong>and</strong> find ways to hear the voice of the wider population too. The Commission<br />
would like to recommend developing proposals to engage with the wider population about<br />
services <strong>and</strong> service development. To obtain the views not only from service users in contact<br />
with the Trust <strong>and</strong> using services; but also members of the population who may not necessarily<br />
be in contact with services, who may have preconceived views about the trust or prejudices<br />
against using the Trust services. This could give the Trust valuable insight into its public<br />
reputation <strong>and</strong> general views from people in the population not using the service that could<br />
start if they were convinced their preconceptions were unfounded.<br />
76 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
SECTION 7 – Statement of Directors’<br />
responsibilities in respect of the Quality<br />
Account<br />
The Directors are required under the Health Act 2009 <strong>and</strong><br />
the National Health Service (Quality Accounts) Regulations<br />
2010 to prepare Quality Accounts for each financial year.<br />
Monitor has issued guidance to NHS foundation trust<br />
boards on the form <strong>and</strong> content of annual quality <strong>report</strong>s<br />
(which incorporate the above legal requirements) <strong>and</strong> on<br />
the arrangements that foundation trust boards should put<br />
in place to support the data quality for the preparation of<br />
the quality <strong>report</strong>.<br />
In preparing the Quality Report, directors are required to<br />
take steps to satisfy themselves that:<br />
• the content of the quality <strong>report</strong> meets the requirements<br />
set out in the NHS Foundation Trust <strong>Annual</strong> Reporting<br />
Manual <strong>2011</strong>/<strong>12</strong>;<br />
• the content of the Quality Report is not inconsistent with<br />
internal <strong>and</strong> external sources of information including:<br />
––<br />
Board minutes <strong>and</strong> papers for the period April <strong>2011</strong><br />
to June 20<strong>12</strong><br />
––<br />
Papers relating to Quality <strong>report</strong>ed to the Board over<br />
the period April <strong>2011</strong> to June 20<strong>12</strong><br />
––<br />
Feedback from the commissioners dated 17/05/20<strong>12</strong><br />
––<br />
Feedback from Governors dated 10/05/20<strong>12</strong><br />
––<br />
Feedback from LINks dated 21/05/20<strong>12</strong><br />
––<br />
The Trust’s complaints <strong>report</strong> published under<br />
regulation 18 of the Local Authority Social Services<br />
<strong>and</strong> NHS Complaints Regulations 2009, dated<br />
30/05/20<strong>12</strong>;<br />
––<br />
The national patient survey February 20<strong>12</strong><br />
––<br />
The national staff survey January 20<strong>12</strong><br />
––<br />
The Head of Internal Audit’s annual opinion over the<br />
Trust’s control environment dated 18 May 20<strong>12</strong><br />
––<br />
CQC quality <strong>and</strong> risk profiles dated April <strong>2011</strong> to June<br />
20<strong>12</strong><br />
• the Quality Report presents a balanced picture of the<br />
NHS Foundation Trust’s performance over the period<br />
covered;<br />
• the performance information <strong>report</strong>ed in the Quality<br />
Report is reliable <strong>and</strong> accurate;<br />
• there are proper internal controls over the collection<br />
<strong>and</strong> <strong>report</strong>ing of the measures of performance included<br />
in the Quality Report, <strong>and</strong> these controls are subject to<br />
review to confirm that they are working effectively in<br />
practice;<br />
• the data underpinning the measures of performance<br />
<strong>report</strong>ed in the Quality Report is robust <strong>and</strong> reliable,<br />
conforms to specified data quality st<strong>and</strong>ards <strong>and</strong><br />
prescribed 107 definitions, is subject to appropriate<br />
scrutiny <strong>and</strong> review; <strong>and</strong> the Quality Report has been<br />
prepared in accordance with Monitor’s annual <strong>report</strong>ing<br />
guidance (which incorporates the Quality Account’s<br />
regulations) (published at www.monitornhsft.gov.<br />
uk/annual<strong>report</strong>ingmanual) as well as the st<strong>and</strong>ards<br />
to support data quality for the preparation of the<br />
Quality Report (available at www.monitornhsft.gov.uk/<br />
annual<strong>report</strong>ingmanual)).<br />
The Directors confirm to the best of their knowledge <strong>and</strong><br />
belief they have complied with the above requirements in<br />
preparing the Quality Report. By order of the Board.<br />
Michael Cassidy CBE<br />
Chairman<br />
30 May 20<strong>12</strong><br />
Nancy Hallett<br />
Chief Executive<br />
30 May 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 77
78 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
<strong>Annual</strong> Accounts<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 79
80 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
<strong>Annual</strong> Accounts<br />
Contents<br />
Foreword to the Accounts 82<br />
<strong>Annual</strong> Governance Statement 83<br />
Statement of Accounting Officer’s Responsibilities 88<br />
Independent Auditor’s Report 89<br />
Statement of Comprehensive Income<br />
for the year ended 31 March 20<strong>12</strong> 90<br />
Statement of Financial Position as at 31 March 20<strong>12</strong> 91<br />
Statement of Changes in Taxpayers’ Equity <strong>2011</strong>/<strong>12</strong> 92<br />
Statement of Changes in Taxpayers’ Equity 2010/11 92<br />
Statement of Cash Flows for the year<br />
ended 31 March 20<strong>12</strong> 93<br />
Notes to the Accounts 94<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 81
ANNUAL ACCOUNTS<br />
Foreword to the Accounts<br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
These <strong>accounts</strong> for the year ended 31 March 20<strong>12</strong> have<br />
been prepared by the <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS<br />
Foundation Trust in accordance with paragraphs 24 & 25 of<br />
Schedule 7 to the NHS Act 2006.<br />
Nancy Hallett<br />
Chief Executive<br />
28 May 20<strong>12</strong><br />
82 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
<strong>Annual</strong> Governance Statement <strong>2011</strong>/<strong>12</strong><br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
1 Scope of responsibility<br />
As Accounting Officer, I have responsibility for maintaining<br />
a sound system of internal control that supports the<br />
achievement of the NHS foundation trust’s policies, aims<br />
<strong>and</strong> objectives, whilst safeguarding the public funds <strong>and</strong><br />
departmental assets for which I am personally responsible,<br />
in accordance with the responsibilities assigned to me.<br />
I am also responsible for ensuring that the NHS foundation<br />
trust is administered prudently <strong>and</strong> economically <strong>and</strong><br />
that resources are applied efficiently <strong>and</strong> effectively. I also<br />
acknowledge my responsibilities as set out in the NHS<br />
Foundation Trust Accounting Officer Memor<strong>and</strong>um.<br />
2 The purpose of the system of internal control<br />
The system of internal control is designed to manage risk to<br />
a reasonable level rather than to eliminate all risk of failure<br />
to achieve policies, aims <strong>and</strong> objectives; it can therefore<br />
only provide reasonable <strong>and</strong> not absolute assurance of<br />
effectiveness. The system of internal control is based on<br />
an ongoing process designed to identify <strong>and</strong> prioritise the<br />
risks to the achievement of the policies, aims <strong>and</strong> objectives<br />
of <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust, to<br />
evaluate the likelihood of those risks being realised <strong>and</strong><br />
the impact should they be realised, <strong>and</strong> to manage them<br />
efficiently, effectively <strong>and</strong> economically. The system of<br />
internal control has been in place in <strong>Homerton</strong> <strong>University</strong><br />
<strong>Hospital</strong> NHS Foundation Trust for the year ended 31 March<br />
20<strong>12</strong> <strong>and</strong> up to the date of approval of the annual <strong>report</strong><br />
<strong>and</strong> <strong>accounts</strong>.<br />
3 Capacity to h<strong>and</strong>le risk<br />
The Trust has ensured that its risk management system<br />
receives the appropriate leadership <strong>and</strong> management.<br />
The Chief Nurse & Director of Governance is the executive<br />
lead for risk management at Board level. The Director of<br />
Finance has delegated responsibility for managing the<br />
strategic development <strong>and</strong> implementation of Financial Risk<br />
Management. All Executive Directors take responsibility for<br />
risk identification, management <strong>and</strong> mitigation within their<br />
areas of work <strong>and</strong> practice.<br />
The Risk Committee, as a Board Sub-Committee, takes<br />
overall responsibility for coordinating <strong>and</strong> monitoring all<br />
risk issues within the Trust including scrutiny of <strong>report</strong>s<br />
from both internal <strong>and</strong> external sources. A number of<br />
sub-committees <strong>and</strong> working groups <strong>report</strong> to the Risk<br />
Committee on both clinical <strong>and</strong> organisational risk. Key<br />
risks are reviewed by the Board either as part of its regular<br />
monitoring of performance (e.g. Board receives minutes of<br />
both the Risk <strong>and</strong> Audit Committees) or in the context of<br />
specific issues that arise.<br />
In particular:<br />
• The Risk Committee, which has been established for a<br />
number of years, is chaired by a Non-Executive Director<br />
(NED) <strong>and</strong> its membership includes the Chairman <strong>and</strong><br />
Trust Executive Directors. The Risk Committee meets on<br />
a quarterly basis <strong>and</strong> <strong>report</strong>s to the Board of Directors.<br />
• The Risk Committee is kept informed about all aspects<br />
of risk management by way of <strong>report</strong>s <strong>and</strong> minutes<br />
from the Quality Improvement Committee, Information<br />
Governance Committee <strong>and</strong> the Health & Safety<br />
Committee.<br />
• The Clinical Risk Manager <strong>report</strong>s regularly via the<br />
Head of Clinical Quality <strong>and</strong> the Head of Governance<br />
to the Chief Nurse <strong>and</strong> Director of Governance. The<br />
Non-Clinical Risk Manager <strong>report</strong>s to the Director of<br />
Environment who has Board level responsibility for<br />
Health <strong>and</strong> Safety.<br />
• As required by the Trust’s Risk Management Strategy,<br />
clinical directors, divisional operations directors,<br />
senior nurses, <strong>and</strong> other relevant senior managers are<br />
responsible for the management of risk within the<br />
workplace. They foster a culture of risk awareness<br />
throughout their divisions <strong>and</strong> ensure assessments for all<br />
work-based activity are conducted.<br />
• The Trust is continuing to develop a comprehensive risk<br />
register, identifying risks at both Trust <strong>and</strong> divisional<br />
level. The Head of Clinical Quality is responsible for the<br />
maintenance of this register.<br />
Risk management training is delivered to all staff as part of<br />
induction <strong>and</strong> regular training opportunities are provided<br />
within the Trust to staff at all levels. The programme of risk<br />
training is subject to continuous internal review.<br />
4 The risk <strong>and</strong> control framework<br />
The Trust has a comprehensive Risk Management Strategy<br />
which is reviewed by the Risk Committee, approved by the<br />
Board of Directors <strong>and</strong> is available to all staff through the<br />
Trust’s intranet.<br />
The Strategy describes the Trust’s overall risk management<br />
approach, corporate <strong>and</strong> divisional responsibilities for<br />
risk, the risk management process <strong>and</strong> the Trust’s risk<br />
identification, assessment <strong>and</strong> control system. It includes<br />
guidance on the risk assessment matrix used to evaluate<br />
risks to facilitate inclusion on the Trust’s risk registers.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 83
ANNUAL ACCOUNTS<br />
Risk management is embedded in the activities of the<br />
organisation in a number of ways:<br />
• corporate <strong>and</strong> divisional objectives are risk assessed as<br />
part of the annual business planning <strong>and</strong> performance<br />
management process<br />
• structured processes are used for the completion of local<br />
risk assessments to populate the Trust’s Risk Register<br />
• the Trust is compliant with the NHS Litigation Authority<br />
Risk Management St<strong>and</strong>ards for both its Acute <strong>and</strong><br />
Maternity Services at Level 2<br />
• there are structured processes in place for incident<br />
<strong>report</strong>ing, the investigation of Serious Incidents (SIs),<br />
complaints <strong>and</strong> litigation cases, <strong>and</strong><br />
• all Executive Directors regularly review the Board<br />
Assurance Framework <strong>and</strong> risk register to ensure that<br />
appropriate action is being taken against key risks.<br />
The Trust continues to carry out an annual exercise<br />
to capture both clinical <strong>and</strong> non-clinical risk data at<br />
divisional <strong>and</strong> departmental levels through local risk<br />
assessments. In addition, ongoing risk assessments form<br />
part of the departmental arrangements with regard to risk<br />
management. Best practice is highlighted <strong>and</strong> shared across<br />
divisions through; divisional leads, the Quality Improvement<br />
Committee <strong>and</strong> the Health <strong>and</strong> Safety Committee <strong>and</strong> their<br />
respective sub-groups. Divisions <strong>report</strong> quarterly on clinical<br />
quality, including the processes to manage clinical risk, to<br />
the Quality Improvement Committee.<br />
The key elements of the quality governance arrangements<br />
are as described in Monitor’s Quality Governance<br />
Framework; strategy, capabilities <strong>and</strong> culture, processes<br />
<strong>and</strong> structure <strong>and</strong> measurement. The Trust is committed<br />
to continuous improvement <strong>and</strong> learning; from incidents<br />
<strong>and</strong> complaints, outcomes from audits <strong>and</strong> the experiences<br />
of patients, clients <strong>and</strong> staff. The quality of performance<br />
information is assessed through data quality <strong>report</strong>s to<br />
divisions <strong>and</strong> regular audit.<br />
The Trust is registered with the Care Quality Commission<br />
(CQC) <strong>and</strong> has a process of self assessment in place<br />
undertaken against the CQC Essential St<strong>and</strong>ards of Quality<br />
<strong>and</strong> Safety. The outcomes of assessments are presented<br />
to <strong>and</strong> monitored by the Risk Committee. In addition,<br />
further assurance is provided by the Audit Committee who<br />
commission specific reviews by the Trust’s internal auditors.<br />
Any areas of concern are risk assessed <strong>and</strong> managed on<br />
the Trust risk register. All of the 16 CQC Essential St<strong>and</strong>ards<br />
of Quality <strong>and</strong> Safety have an identified lead within<br />
the organisation <strong>and</strong> it is their responsibility to provide<br />
compliance evidence.<br />
Additional assurance has also been gained through<br />
participation in CQC special reviews or investigations,<br />
specifically in the last <strong>12</strong> months:<br />
• Dignity <strong>and</strong> Nutrition Inspection (DANI) - May <strong>2011</strong><br />
• Mary Seacole Nursing Home Inspection - October <strong>2011</strong><br />
• <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> Inspection - November<br />
<strong>2011</strong><br />
• Review of Termination of Pregnancy Services - March<br />
20<strong>12</strong>, <strong>and</strong><br />
• Safeguarding <strong>and</strong> Looked After Children Inspection -<br />
March 20<strong>12</strong>.<br />
All of these inspections were positive <strong>and</strong> constructive<br />
feedback was given by the Regulator.<br />
The foundation trust is fully compliant with the registration<br />
requirements of the Care Quality Commission.<br />
The Trust has established a process of information<br />
governance led by the Medical Director. Systems <strong>and</strong><br />
processes have been reviewed, including using the<br />
Information Governance Toolkit. The Trust declared that it<br />
has complied with information governance guidelines <strong>and</strong><br />
the Data Protection Act 1998. The Information Governance<br />
Committee is responsible for monitoring <strong>and</strong> controlling<br />
risks to data security. There were no Serious Incidents<br />
involving data loss or confidentiality issues during the year.<br />
A Board Assurance Framework detailing the principal<br />
risks to the achievement of the Trust’s objectives was in<br />
place for the whole of the financial year. This was based<br />
on the objectives set out in the Trust’s <strong>2011</strong>/<strong>12</strong> <strong>Annual</strong><br />
Plan <strong>and</strong> identified the risks to the achievement of those<br />
objectives, the key controls in place to manage those risks<br />
<strong>and</strong> the sources of assurance available to demonstrate<br />
the effectiveness of those controls. The Board Assurance<br />
Framework has been reviewed regularly <strong>and</strong> updated<br />
through the year by the Board with the latest version<br />
reflecting the position at 31 March 20<strong>12</strong>. The risks in the<br />
Board Assurance Framework are monitored <strong>and</strong> reviewed<br />
by the Risk Committee at each of its meetings <strong>and</strong> <strong>report</strong>s<br />
provided to the Board on key issues arising. All of the<br />
principal risks identified are monitored regularly through<br />
st<strong>and</strong>ing performance <strong>report</strong>s to the Trust Board.<br />
Key risks identified include the following:<br />
• risks associated with the condition of community health<br />
service buildings posing a risk to the ability to deliver<br />
clinical services <strong>and</strong> meeting regulatory compliance in<br />
these locations. (both in-year <strong>and</strong> future risk)<br />
• risks to Trust business associated with the health<br />
economy reconfiguration in North East London (in-year<br />
<strong>and</strong> future risk)<br />
• risks to Trust business associated with commissioner led<br />
actions (both in-year <strong>and</strong> future risk)<br />
84 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
• risks associated with the Olympic travel change<br />
impacting on access to the Trust (future risk), <strong>and</strong><br />
• risk to organisational continuity due to change of Chief<br />
Executive (future risk).<br />
The Trust has comprehensive action plans in place to<br />
mitigate the above risks which are monitored by the<br />
Risk Committee <strong>and</strong> Trust Board. Outcomes are assessed<br />
through performance <strong>report</strong>s to the Trust Board.<br />
The Trust recognises its risk management approach will not<br />
eliminate risks totally, but it will provide the organisation<br />
with a means to identify, prioritise <strong>and</strong> manage the risks.<br />
This will provide a balance between the cost of managing<br />
<strong>and</strong> treating risk, <strong>and</strong> the anticipated benefits that will be<br />
derived.<br />
Equality Impact Assessments are undertaken for major<br />
service changes as well as for policies <strong>and</strong> procedures.<br />
There are arrangements in place for working with<br />
stakeholders <strong>and</strong> partner organisations, including<br />
close working with the Commissioners, local General<br />
Practitioners, the Council of Governors, LINks, NHS London,<br />
the Corporation of London, <strong>and</strong> the London Borough of<br />
Hackney.<br />
Stakeholders are involved in managing risks which impact<br />
on them through their involvement in <strong>and</strong> contributions to<br />
many aspects of the work of the Trust, including:<br />
• public <strong>and</strong> stakeholder representation on the Council of<br />
Governors<br />
• consultation with <strong>and</strong> involvement from the members of<br />
the Foundation Trust<br />
• The National Patient Survey Programme<br />
• Hackney Health Local Improvement Network (LINk)<br />
• Hackney Overview <strong>and</strong> Scrutiny Committee, <strong>and</strong><br />
• The Health <strong>and</strong> Social Care Partnership Board; <strong>and</strong><br />
membership of the Local Strategic Partnership.<br />
Pensions<br />
As an employer with staff entitled to membership of the<br />
NHS Pension Scheme (the Scheme), control measures<br />
are in place to ensure all employer obligations contained<br />
within the Scheme regulations are complied with. This<br />
includes ensuring that deductions from salary, employer’s<br />
contributions <strong>and</strong> payments into the Scheme are in<br />
accordance with the Scheme rules, <strong>and</strong> that member<br />
Scheme records are accurately updated in accordance with<br />
the timescales detailed in the Regulations.<br />
Equality, diversity <strong>and</strong> human rights<br />
Control measures are in place to ensure that all the<br />
organisation’s obligations under equality, diversity <strong>and</strong><br />
human rights legislation are complied with.<br />
Carbon reduction<br />
The Foundation Trust has undertaken risk assessments <strong>and</strong><br />
Carbon Reduction Delivery Plans are in place in accordance<br />
with emergency preparedness <strong>and</strong> civil contingency<br />
requirements, as based on UKCIP 2009 weather projects,<br />
to ensure that the Trust’s obligations under the Climate<br />
Change Act <strong>and</strong> the Adaptation Reporting requirements<br />
are complied with.<br />
5. Review of Economy, Efficiency <strong>and</strong> Effectiveness<br />
of the Use of Resources<br />
In addition to the financial review of resources within the<br />
quarterly monitoring returns to Monitor all budget holders<br />
are provided with monthly financial information to help<br />
them ensure resources are used economically, efficiently<br />
<strong>and</strong> effectively. Monthly finance <strong>and</strong> performance <strong>report</strong>s<br />
are provided for the Board. Internal Audit has an important<br />
role, as does the Finance <strong>and</strong> Performance Committee, to<br />
challenge how resources are used. The Trust also has an<br />
internal performance management review process which<br />
provides evidence of performance at divisional level <strong>and</strong><br />
the actions being taken to ensure resources are being used<br />
effectively <strong>and</strong> efficiently.<br />
In addition the annual business planning process, including<br />
the requirement to identify cost improvements, provides<br />
another mechanism to achieve this aim. The Trust also<br />
has a comprehensive Quality, Innovation, Productivity<br />
<strong>and</strong> Prevention (QIPP) progamme in place to identify <strong>and</strong><br />
deliver efficiencies against the Trust target for savings. This<br />
programme is led by the Chief Operating Officer, progress<br />
<strong>and</strong> associated risks are <strong>report</strong>ed to the Board of Directors.<br />
6. <strong>Annual</strong> Quality Report<br />
The Directors are required under the Health Act 2009 <strong>and</strong><br />
the National Health Service (Quality Accounts) Regulations<br />
2010 (as amended) to prepare Quality Accounts for<br />
each financial year. Monitor has issued guidance to<br />
NHS foundation trust boards on the form <strong>and</strong> content<br />
of annual Quality Reports which incorporate the above<br />
legal requirements in the NHS Foundation Trust <strong>Annual</strong><br />
Reporting Manual.<br />
The <strong>Annual</strong> Quality Report <strong>2011</strong>/<strong>12</strong> has been developed<br />
in line with relevant national guidance <strong>and</strong> legislative<br />
requirements. Assurance over the content <strong>and</strong> quality<br />
of the information in the <strong>report</strong> is gained through the<br />
following:<br />
• The Chief Nurse & Director of Governance leads on the<br />
production of the Quality Report at Board level. The<br />
Head of Clinical Quality is responsible for compiling<br />
<strong>and</strong> writing the draft Quality Report, managing the<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 85
ANNUAL ACCOUNTS<br />
consultation processes in relation to the draft <strong>report</strong> (for<br />
both planning priorities <strong>and</strong> feedback), <strong>and</strong> managing<br />
the process of regular <strong>report</strong>ing to the Board <strong>and</strong> the<br />
Quality Improvement Committee.<br />
• Plans for the achievement of the main quality priorities<br />
are developed, reviewed <strong>and</strong> assured by the Quality<br />
Improvement Committee <strong>and</strong> the Board.<br />
• Consultation is carried out with internal <strong>and</strong> external<br />
stakeholders <strong>and</strong> fed back to the Board before they set<br />
quality priorities for the coming year. The content of<br />
the draft <strong>report</strong> is reviewed by the Board <strong>and</strong> sent for<br />
internal <strong>and</strong> external consultation including the Council<br />
of Governors. The Board approves the final content of<br />
the <strong>report</strong>.<br />
• The Trust has in place a range of policies <strong>and</strong> procedures<br />
to support the achievement of quality priorities.<br />
• The data used for the Quality Account is a combination<br />
of centrally <strong>and</strong> locally collected data. All information<br />
routinely presented to the Board is compiled by the<br />
Trust’s Information Team. This data is managed using<br />
the Trust’s Data Quality Policy <strong>and</strong> processes are in place<br />
to ensure the data is validated. Other data is collected<br />
locally by clinical teams using separate databases.<br />
Internal <strong>and</strong> External Auditors annually review three<br />
items of data (two national <strong>and</strong> one local) that are in the<br />
Quality Account.<br />
7. Review of Effectiveness<br />
As Accounting Officer, I have responsibility for reviewing<br />
the effectiveness of the system of internal control. My<br />
review of the effectiveness of the system of internal<br />
control is informed by the work of the Internal Auditors,<br />
clinical audit <strong>and</strong> the executive managers <strong>and</strong> clinical leads<br />
within the NHS foundation trust who have responsibility<br />
for the development <strong>and</strong> maintenance of the internal<br />
control framework. I have drawn on the content of the<br />
quality <strong>report</strong> attached to this <strong>Annual</strong> Report <strong>and</strong> other<br />
performance information available to me. My review is also<br />
informed by comments made by the External Auditors in<br />
their management letter <strong>and</strong> other <strong>report</strong>s. I have been<br />
advised on the implications of the result of my review of the<br />
effectiveness of the system of internal control by the Board,<br />
the Audit Committee <strong>and</strong> Risk Committee, <strong>and</strong> a plan to<br />
address weaknesses <strong>and</strong> ensure continuous improvement<br />
of the system is in place.<br />
• Reports from both the External Auditors <strong>and</strong> the Local<br />
Counter Fraud Specialist<br />
• Patient <strong>and</strong> staff surveys<br />
• Outcomes of Care Quality Commission Reviews<br />
• NHSLA assessments, <strong>and</strong><br />
• The Trust’s regular <strong>report</strong>ing to Monitor providing<br />
additional assurance with regard to compliance with our<br />
Terms of Authorisation.<br />
The key considerations of my review of the effectiveness<br />
of the system of internal control can be summarised as<br />
follows:<br />
• The Board has been actively involved in developing<br />
<strong>and</strong> reviewing the Trust’s risk management processes<br />
including receiving <strong>and</strong> reviewing <strong>report</strong>s <strong>and</strong> minutes<br />
from the Risk <strong>and</strong> Audit Committees. The Board has<br />
also reviewed the Board Assurance Framework as well<br />
as monitoring performance objectives via the balanced<br />
scorecard.<br />
• The Risk Committee has overseen the effectiveness of<br />
all the Trust’s risk management arrangements including<br />
review <strong>and</strong> endorsement of the Strategy <strong>and</strong> Policy<br />
for Risk Management <strong>and</strong> the development of the<br />
Board Assurance Framework. The Risk Committee also<br />
monitors all key clinical <strong>and</strong> non-clinical risks highlighted<br />
by other committees.<br />
• The Audit Committee has been a directing force in<br />
relation to reviewing the system of internal control<br />
particularly with regard to corporate risk <strong>and</strong> counter<br />
fraud. Internal Audit has reviewed <strong>and</strong> <strong>report</strong>ed upon<br />
control, governance <strong>and</strong> risk management processes,<br />
based on an audit plan approved by the Committee. The<br />
work included identifying <strong>and</strong> evaluating controls <strong>and</strong><br />
testing their effectiveness. Where scope for improvement<br />
was found, recommendations were made <strong>and</strong><br />
appropriate action plans agreed with management.<br />
• Executive Directors have ensured that key risks have<br />
been highlighted <strong>and</strong> monitored within their area of<br />
responsibility <strong>and</strong> the necessary action taken to address<br />
them. Executive Directors were also directly involved<br />
in producing <strong>and</strong> reviewing the Board Assurance<br />
Framework.<br />
• Internal Audit have provided consistent support <strong>and</strong><br />
advice with regard to the system of internal control<br />
including the ongoing development of the Board<br />
Assurance Framework.<br />
• The Finance & Performance Committee is responsible<br />
for overseeing performance management <strong>and</strong> ongoing<br />
regulatory compliance, <strong>and</strong> of developing the Trust’s<br />
longer term financial strategy.<br />
• The Quality Improvement Committee is responsible for<br />
the governance <strong>and</strong> management of clinical risk.<br />
Internal Audit’s review of the Board Assurance Framework<br />
has concluded that it provides reasonable assurance that<br />
there is an effective system of internal control to manage<br />
the principal risks identified by the Trust.<br />
86 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
As noted above, the Board Assurance Framework identifies<br />
gaps in control <strong>and</strong> gaps in assurance in relation to the<br />
Trust’s principal risks <strong>and</strong> the actions being taken to address<br />
them.<br />
Conclusion<br />
My review confirms that <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong><br />
NHS Foundation Trust has a sound system of internal<br />
control that supports the achievement of its policies, aims<br />
<strong>and</strong> objectives. No significant control issues have been<br />
identified.<br />
Nancy Hallett<br />
Chief Executive<br />
28 May 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 87
ANNUAL ACCOUNTS<br />
Statement of Accounting Officer’s<br />
Responsibilities<br />
Statement of the Chief Executive’s responsibilities as the<br />
Accounting Officer of <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS<br />
Foundation Trust.<br />
The NHS Act 2006 states that the Chief Executive is the<br />
Accounting Officer of the NHS foundation trust. The<br />
relevant responsibilities of Accounting Officer, including<br />
their responsibility for the propriety <strong>and</strong> regularity of<br />
public finances for which they are answerable, <strong>and</strong> for<br />
the keeping of proper <strong>accounts</strong>, are set out in the NHS<br />
Foundation Trust Accounting Officer Memor<strong>and</strong>um issued<br />
by Monitor, the Independent Regulator of NHS Foundation<br />
Trusts.<br />
Under the NHS Act 2006, Monitor has directed <strong>Homerton</strong><br />
<strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust to prepare for<br />
each financial year a statement of <strong>accounts</strong> in the form<br />
<strong>and</strong> on the basis set out in the Accounts Direction. The<br />
<strong>accounts</strong> are prepared on an accruals basis <strong>and</strong> must give<br />
a true <strong>and</strong> fair view of the state of affairs of <strong>Homerton</strong><br />
<strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust <strong>and</strong> of its income<br />
<strong>and</strong> expenditure, total recognised gains <strong>and</strong> losses <strong>and</strong> cash<br />
flows for the financial year.<br />
In preparing the <strong>accounts</strong>, the Accounting Officer is<br />
required to comply with the requirements of the NHS<br />
Foundation Trust <strong>Annual</strong> Reporting Manual <strong>and</strong> in<br />
particular to:<br />
• observe the Accounts Direction issued by Monitor,<br />
including the relevant accounting <strong>and</strong> disclosure<br />
requirements, <strong>and</strong> apply suitable accounting policies on<br />
a consistent basis<br />
• make judgments <strong>and</strong> estimates on a reasonable basis<br />
• state whether applicable Accounting St<strong>and</strong>ards as set<br />
out in the NHS Foundation Trust <strong>Annual</strong> Reporting<br />
Manual have been followed, <strong>and</strong> disclose <strong>and</strong> explain<br />
any material departures in the financial statements, <strong>and</strong><br />
• prepare the financial statements on a going concern<br />
basis.<br />
The Accounting Officer is responsible for keeping proper<br />
accounting records which disclose with reasonable accuracy<br />
at any time the financial position of the NHS Foundation<br />
Trust <strong>and</strong> to enable her to ensure that the <strong>accounts</strong> comply<br />
with requirements outlined in the above mentioned Act.<br />
The Accounting Officer is also responsible for safeguarding<br />
the assets of the NHS Foundation Trust <strong>and</strong> hence for<br />
taking reasonable steps for the prevention <strong>and</strong> detection of<br />
fraud <strong>and</strong> other irregularities.<br />
To the best of my knowledge <strong>and</strong> belief, I have properly<br />
discharged the responsibilities set out in Monitor’s NHS<br />
Foundation Trust Accounting Officer Memor<strong>and</strong>um.<br />
Nancy Hallett<br />
Chief Executive<br />
28 May 20<strong>12</strong><br />
88 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Independent Auditor’s <strong>report</strong> to the Board<br />
of Governors <strong>and</strong> Board of Directors<br />
of <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS<br />
Foundation Trust<br />
We have audited the financial statements of <strong>Homerton</strong><br />
<strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust for the year<br />
ended 31 March 20<strong>12</strong> which comprise the Statement of<br />
Comprehensive Income, the Statement of Financial Position<br />
the Statement of Changes in Taxpayers Equity <strong>and</strong> the<br />
Statement of Cash Flows <strong>and</strong> the related notes 1 to 29.<br />
The financial <strong>report</strong>ing framework that has been applied<br />
in their preparation is applicable law <strong>and</strong> the accounting<br />
policies directed by Monitor – Independent Regulator of NHS<br />
Foundation Trusts.<br />
This <strong>report</strong> is made solely to the Board of Governors <strong>and</strong><br />
Board of Directors (“the Boards”) of <strong>Homerton</strong> <strong>University</strong><br />
<strong>Hospital</strong> NHS Foundation Trust, as a body, in accordance with<br />
paragraph 4 of Schedule 10 of the National Health Service Act<br />
2006. Our audit work has been undertaken so that we might<br />
state to the Boards those matters we are required to state to<br />
them in an auditor’s <strong>report</strong> <strong>and</strong> for no other purpose. To the<br />
fullest extent permitted by law, we do not accept or assume<br />
responsibility to anyone other than the trust <strong>and</strong> the Boards as<br />
a body, for our audit work, for this <strong>report</strong>, or for the opinions<br />
we have formed.<br />
Respective responsibilities of the accounting officer<br />
<strong>and</strong> auditor<br />
As explained more fully in the Accounting Officer’s<br />
Responsibilities Statement, the Accounting Officer is<br />
responsible for the preparation of the financial statements<br />
<strong>and</strong> for being satisfied that they give a true <strong>and</strong> fair view.<br />
Our responsibility is to audit <strong>and</strong> express an opinion on the<br />
financial statements in accordance with applicable law, the<br />
Audit Code of NHS Foundation Trusts <strong>and</strong> International<br />
St<strong>and</strong>ards on Auditing (UK <strong>and</strong> Irel<strong>and</strong>). Those st<strong>and</strong>ards<br />
require us to comply with the Auditing Practices Board’s<br />
Ethical St<strong>and</strong>ards for Auditors.<br />
The directors are responsible for the maintenance <strong>and</strong><br />
integrity of the corporate <strong>and</strong> financial information included<br />
on the company’s website. Legislation in the United Kingdom<br />
governing the preparation <strong>and</strong> dissemination of financial<br />
information differs from legislation in other jurisdictions.<br />
Scope of the audit of the financial statements<br />
An audit involves obtaining evidence about the amounts<br />
<strong>and</strong> disclosures in the financial statements sufficient to give<br />
reasonable assurance that the financial statements are free<br />
from material misstatement, whether caused by fraud or<br />
error. This includes an assessment of: whether the accounting<br />
policies are appropriate to the trust’s circumstances <strong>and</strong> have<br />
been consistently applied <strong>and</strong> adequately disclosed; the<br />
reasonableness of significant accounting estimates made by<br />
the Accounting Officer; <strong>and</strong> the overall presentation of the<br />
financial statements. In addition, we read all the financial<br />
<strong>and</strong> non-financial information in the annual <strong>report</strong> to identify<br />
material inconsistencies with the audited financial statements.<br />
If we become aware of any apparent material misstatements<br />
or inconsistencies we consider the implications for our <strong>report</strong>.<br />
Opinion on financial statements<br />
In our opinion the financial statements:<br />
• give a true <strong>and</strong> fair view of the state of the trust’s affairs as<br />
at 31 March 20<strong>12</strong> <strong>and</strong> of its income <strong>and</strong> expenditure for<br />
the year then ended<br />
• have been properly prepared in accordance with the<br />
accounting policies directed by Monitor – Independent<br />
Regulator of NHS Foundation Trusts, <strong>and</strong><br />
• have been prepared in accordance with the requirements<br />
of the National Health Service Act 2006.<br />
Opinion on other matter prescribed by the National<br />
Health Service Act 2006<br />
In our opinion:<br />
• the information given in the Directors’ Report for the<br />
financial year for which the financial statements are<br />
prepared is consistent with the financial statements.<br />
Matters on which we are required to <strong>report</strong> by<br />
exception<br />
We have nothing to <strong>report</strong> in respect of the following matters<br />
where the Audit Code for NHS Foundation Trusts requires us<br />
to <strong>report</strong> to you if, in our opinion:<br />
• the <strong>Annual</strong> Governance Statement does not meet the<br />
disclosure requirements set out in the NHS Foundation Trust<br />
<strong>Annual</strong> Reporting Manual, is misleading or inconsistent<br />
with information of which we are aware from our audit.<br />
We are not required to consider, nor have we considered,<br />
whether the <strong>Annual</strong> Governance Statement addresses all<br />
risks <strong>and</strong> controls or that risks are satisfactorily addressed<br />
by internal controls<br />
• proper practices have not been observed in the compilation<br />
of the financial statements, or<br />
• the NHS foundation trust has not made proper<br />
arrangements for securing economy, efficiency <strong>and</strong><br />
effectiveness in its use of resources.<br />
Certificate<br />
We certify that we have completed the audit of the <strong>accounts</strong><br />
in accordance with the requirements of Chapter 5 of Part 2 of<br />
the National Health Service Act 2006 <strong>and</strong> the Audit Code for<br />
NHS Foundation Trusts.<br />
Heather Bygrave (Senior Statutory Auditor)<br />
for <strong>and</strong> on behalf of Deloitte LLP<br />
Chartered Accountants <strong>and</strong> Statutory Auditor<br />
St. Albans, United Kingdom<br />
Date: 28 May 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 89
ANNUAL ACCOUNTS<br />
Statement of comprehensive income for the year ended 31 March 20<strong>12</strong><br />
Restated<br />
<strong>2011</strong>/<strong>12</strong> 2010/11<br />
NOTE £000 £000<br />
Revenue<br />
Operating income from continuing operations 3.1 243,677 190,871<br />
Operating expenses (excluding impairments) 4.1 (234,150) (182,621)<br />
Impairments charged to operating expenses (916) (5,172)<br />
Operating surplus 8,611 3,078<br />
Finance costs:<br />
Finance income 8 145 113<br />
Finance expenses-finance liabilities 8.1 (187) (198)<br />
Finance expenses-unwinding of discount on provisions 17 (19) (22)<br />
Public dividend capital dividends payable 19 (3,296) (3,491)<br />
Total finance costs (3,357) (3,598)<br />
Retained surplus/(deficit) for the year 5,254 (520)<br />
Other comprehensive income<br />
Net revaluation (losses)/gains <strong>and</strong> impairment losses on l<strong>and</strong>, property, plant <strong>and</strong> equipment (2,197) 1,378<br />
Gain on asset disposals - 14<br />
Total comprehensive income for the year 3,057 872<br />
The Trust <strong>report</strong>ed an underlying trading surplus of £6,170,000 in <strong>2011</strong>/<strong>12</strong> (£4,652,000 in 2010/11) before taking into<br />
account impairments.<br />
Due to the Trust taking on City <strong>and</strong> Hackney community health services on 1st April <strong>2011</strong> <strong>and</strong> the FReM’s interpretation of<br />
IAS 20 (Accounting for Government Grants <strong>and</strong> Disclosure of Government Assistance), certain prior year balances have been<br />
restated. The details of this restatement can be seen at note 1.25 to the <strong>accounts</strong>.<br />
The notes on pages 94 to 119 form part of these <strong>accounts</strong>.<br />
90 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Statement of financial position as at 31 March 20<strong>12</strong><br />
Restated Restated<br />
31 March 20<strong>12</strong> 31 March <strong>2011</strong> 1 April 2010<br />
NOTE £000 £000 £000<br />
Non-current assets<br />
Intangible assets 9 642 742 1,<strong>12</strong>0<br />
Property, plant <strong>and</strong> equipment 10 115,<strong>12</strong>1 117,617 117,494<br />
Total non-current assets 115,763 118,359 118,614<br />
Current assets<br />
Inventories <strong>12</strong>.1 1,<strong>12</strong>1 1,025 887<br />
Trade <strong>and</strong> other receivables 13.1 13,456 10,465 10,684<br />
Other financial assets 14 - 25 23<br />
Cash <strong>and</strong> cash equivalents 15 30,556 17,088 16,535<br />
Total current assets 45,133 28,603 28,<strong>12</strong>9<br />
Total assets 160,896 146,962 146,743<br />
Current liabilities<br />
Trade <strong>and</strong> other payables 16.1 (18,185) (<strong>12</strong>,527) (10,535)<br />
Borrowings 16.1 (257) (257) (257)<br />
Provisions 16.1 (1,685) (638) (204)<br />
Tax payable 16.1 (5,204) (3,996) (3,570)<br />
Other liabilities 16.1 (5,403) (3,104) (6,300)<br />
Total current liabilities (30,734) (20,522) (20,866)<br />
Net current assets 14,399 8,081 7,263<br />
Total assets less current liabilities 130,162 <strong>12</strong>6,440 <strong>12</strong>5,877<br />
Non-current liabilities<br />
Borrowings 16.1 (3,794) (4,051) (4,307)<br />
Provisions 16.1 (641) (644) (694)<br />
Total non current liabilities (4,435) (4,695) (5,001)<br />
Total assets employed <strong>12</strong>5,727 <strong>12</strong>1,745 <strong>12</strong>0,876<br />
Financed by taxpayers’ equity<br />
Public dividend capital 19 84,100 83,175 83,175<br />
Revaluation reserve 20,859 23,142 21,898<br />
Retained earnings 20,768 15,428 15,803<br />
Total taxpayers’ equity <strong>12</strong>5,727 <strong>12</strong>1,745 <strong>12</strong>0,876<br />
The financial statements on pages 90 to 119 were approved by the Board <strong>and</strong> signed on its behalf by:<br />
Chief Executive<br />
28 May 20<strong>12</strong><br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 91
ANNUAL ACCOUNTS<br />
Statement of changes in taxpayers’ equity <strong>2011</strong>/<strong>12</strong><br />
Public dividend Retained Revaluation Donated asset<br />
capital (PDC) earnings reserve reserve Total<br />
£000 £000 £000 £000 £000<br />
Balance at 31 March <strong>2011</strong> (restated) 83,175 15,428 23,142 - <strong>12</strong>1,745<br />
Changes in taxpayers’ equity for <strong>2011</strong>/<strong>12</strong><br />
Total Comprehensive income for the year:<br />
Retained surplus for the year - 5,254 - - 5,254<br />
Impairments <strong>and</strong> reversals - - (2,254) - (2,254)<br />
Net gain on revaluation of tangible assets - - 57 - 57<br />
Transfer from donated asset reserve - 86 (86) - -<br />
New PDC received 925 - - - 925<br />
Balance at 31 March 20<strong>12</strong> 84,100 20,768 20,859 - <strong>12</strong>5,727<br />
Statement of changes in taxpayers’ equity 2010/11<br />
Public dividend Retained Revaluation Donated asset<br />
capital (PDC) earnings reserve reserve Total<br />
£000 £000 £000 £000 £000<br />
Balance at 31 March 2010 (restated) 83,175 <strong>12</strong>,466 21,898 2,966 <strong>12</strong>0,505<br />
Changes in taxpayers’ equity for 2010/11<br />
Total Comprehensive income for the year:<br />
Prior period adjustment - 3,337 - (2,966) 371<br />
Retained deficit for the year - (520) - - (520)<br />
Impairments <strong>and</strong> reversals - - (519) - (519)<br />
Net gain on revaluation of tangible assets - - 1,894 - 1,894<br />
Receipt of donated assets - - - - -<br />
Transfer due to disposal of assets - 145 (131) - 14<br />
Balance at 31 March <strong>2011</strong> (restated) 83,175 15,428 23,142 - <strong>12</strong>1,745<br />
92 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Statement of cash flows for the year ended 31 March 20<strong>12</strong><br />
Restated<br />
<strong>2011</strong>/<strong>12</strong> 2010/11<br />
NOTE £000 £000<br />
Net cash inflow from operating activities 20 21,507 11,386<br />
Cash flows from investing activities<br />
Interest received 145 113<br />
Payments for intangible assets (323) (34)<br />
Payments for property, plant <strong>and</strong> equipment (5,134) (6,815)<br />
Proceeds from disposal of plant, property <strong>and</strong> equipment - 58<br />
Net cash outflow from investing activities (5,3<strong>12</strong>) (6,678)<br />
Net cash inflow before financing 16,195 4,708<br />
Cash flows from financing activities<br />
Public dividend capital received 925 -<br />
Loans repaid to the DH (226) (226)<br />
Other loans repaid (31) (31)<br />
Interest repaid (187) (198)<br />
PDC Dividend paid (3,208) (3,700)<br />
Net cash outflow from financing (2,727) (4,155)<br />
Net increase in cash <strong>and</strong> cash equivalents 13,468 553<br />
Cash <strong>and</strong> cash equivalents (<strong>and</strong> bank overdrafts) at 1 April 17,088 16,535<br />
Cash <strong>and</strong> cash equivalents (<strong>and</strong> bank overdrafts) at 31 March 30,556 17,088<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 93
ANNUAL ACCOUNTS<br />
Notes to the Accounts<br />
1. Accounting policies<br />
Monitor has directed that the financial statements of NHS<br />
foundation trusts shall meet the accounting requirements<br />
of the NHS Foundation Trust <strong>Annual</strong> Reporting Manual<br />
(ARM) which has been agreed with HM Treasury.<br />
Consequently, these financial statements have been<br />
prepared in accordance with the <strong>2011</strong>/<strong>12</strong> ARM issued<br />
by Monitor. The accounting policies contained in that<br />
manual follow International Financial Reporting St<strong>and</strong>ards<br />
(IFRS) <strong>and</strong> HM Treasury’s Financial Reporting Manual to<br />
the extent that they are meaningful <strong>and</strong> appropriate to<br />
NHS foundation trusts. The accounting policies have been<br />
applied consistently in dealing with items considered<br />
material in relation to the <strong>accounts</strong>.<br />
1.1 New <strong>and</strong> revised st<strong>and</strong>ards <strong>and</strong> interpretations<br />
The following St<strong>and</strong>ards, amendments <strong>and</strong> interpretations<br />
have been issued by the International Accounting<br />
St<strong>and</strong>ards Board (IASB) <strong>and</strong> International Financial<br />
Reporting Interpretations Committee (IFRIC) but are not yet<br />
required to be adopted or are not yet effective:<br />
• IFRS 7 & 9 Financial Instruments<br />
• IFRS 10 Consolidated Financial Statements<br />
• IFRS 11 Joint Arrangements<br />
• IFRIC <strong>12</strong> Disclosure of Interests in Other Entities<br />
• IFRIC 13 Fair Value Measurement<br />
• IAS 1 Presentation of Financial Statements on Other<br />
Comprehensive Income<br />
• IAS <strong>12</strong> Income Taxes Amendment<br />
• IAS 27 Separate Financial Statements<br />
• IAS 28 Associates <strong>and</strong> Joint Ventures<br />
The Directors anticipate that the adoption of these<br />
st<strong>and</strong>ards in future periods will have no material impact on<br />
the financial statements.<br />
All other revised <strong>and</strong> new St<strong>and</strong>ards have not been listed<br />
here as they are not considered to have an impact on<br />
the Trust. Monitor does not permit the early adoption of<br />
Accounting St<strong>and</strong>ards, amendments <strong>and</strong> interpretations<br />
that are in issue at the <strong>report</strong>ing date but effective at a<br />
subsequent <strong>report</strong>ing period.<br />
1.2 Accounting convention<br />
These <strong>accounts</strong> have been prepared under the historical<br />
cost convention, modified by the revaluation of properties,<br />
<strong>and</strong>, where material, current asset investments <strong>and</strong><br />
inventories to fair value as determined by the relevant<br />
Accounting St<strong>and</strong>ard.<br />
1.3 Income measurement<br />
Income is accounted for by applying the accruals<br />
convention. Income in respect of services provided is<br />
recognised when, <strong>and</strong> to the extent that, performance<br />
occurs <strong>and</strong> is measured at the fair value of the<br />
consideration receivable. The main source of income for<br />
the Trust is contracts with commissioners in respect of<br />
healthcare services.<br />
Where income is received for a specific activity which is to<br />
be delivered in the following financial year, that income is<br />
deferred.<br />
Income from the sale of non-current assets is recognised<br />
only when all material conditions of sale have been met<br />
<strong>and</strong> is measured as the sums due under the sale contract.<br />
1.4 Expenditure on employee benefits<br />
1.4.1 Short-term Employee Benefits<br />
Salaries, wages <strong>and</strong> employment-related payments are<br />
recognised in the period in which the service is received<br />
from employees. The cost of annual leave entitlement<br />
earned but not taken by employees at the end of the<br />
period is recognised in the financial statements to the<br />
extent that employees are permitted to carry forward leave<br />
in the following period.<br />
1.4.2 Pension costs<br />
Past <strong>and</strong> present employees are covered by the provisions<br />
of the NHS Pensions Scheme. Details of the benefits<br />
payable under these provisions can be found on the NHS<br />
Pensions website at www.nhsbsa.nhs.uk/pensions. The<br />
scheme is an unfunded, defined benefit scheme that<br />
covers NHS employers, General Practices <strong>and</strong> other bodies,<br />
allowed under the direction of the Secretary of State, in<br />
Engl<strong>and</strong> <strong>and</strong> Wales. The scheme is not designed to be run<br />
in a way that would enable the Trust to identify its share of<br />
the underlying scheme assets <strong>and</strong> liabilities. Therefore, the<br />
scheme is accounted for as if it were a defined contribution<br />
scheme: the cost to the Trust of participating in the scheme<br />
is taken as equal to the contributions payable to the<br />
scheme for the accounting period.<br />
Employer’s pension cost contributions are charged to<br />
operating expenses as <strong>and</strong> when they become due. The<br />
cost of the scheme is equal to the contributions payable<br />
to the scheme for the accounting period. The employer<br />
contribution payable in <strong>2011</strong>/<strong>12</strong> was £13.4m (2010/11<br />
£9.7m), <strong>and</strong> is estimated to be £13.7m in 20<strong>12</strong>/13.<br />
Additional pension liabilities arising from early retirements<br />
are not funded by the scheme except where the retirement<br />
is due to ill-health. The full amount of the liability for the<br />
additional costs is charged to the operating expenses at the<br />
94 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
time the trust commits itself to the retirement, regardless of<br />
the method of payment.<br />
1.5 Expenditure on other goods <strong>and</strong> services<br />
Expenditure is accounted for by applying the accruals<br />
convention. Expenditure on goods <strong>and</strong> services is<br />
recognised when, <strong>and</strong> to the extent that they have been<br />
received, <strong>and</strong> measured at the fair value of those goods<br />
<strong>and</strong> services. Expenditure is recognised in operating<br />
expenses except where it results in the creation of a non<br />
current asset such as property, plant <strong>and</strong> equipment.<br />
1.6 Property, plant <strong>and</strong> equipment<br />
1.6.1 Recognition<br />
Property, Plant <strong>and</strong> Equipment is capitalised where:<br />
• it is held for sale in delivering services or for<br />
administrative purposes<br />
• it is probable that future economic benefits will flow to,<br />
or service potential be provided to, the Trust<br />
• it is expected to be used for more than one financial year<br />
• the cost of the item can be measured reliably<br />
• it individually has a cost of at least £5,000, or<br />
• they form a group of assets which individually have<br />
a cost of more than £250, collectively have a cost<br />
of at least £5,000, where the assets are functionally<br />
interdependent, they have broadly simultaneous disposal<br />
dates <strong>and</strong> are under single managerial control, or<br />
• it forms part of the initial setting-up cost of a new<br />
building or unit.<br />
Where a large asset, for example a building, includes<br />
a number of components with significantly different<br />
asset lives, for example plant <strong>and</strong> equipment, then these<br />
components are treated as separate assets <strong>and</strong> depreciated<br />
over their useful economic lives.<br />
1.6.2 Measurement<br />
(i) Valuation<br />
All property, plant <strong>and</strong> equipment are measured initially at<br />
cost, representing the cost directly attributable to acquiring<br />
or constructing the asset <strong>and</strong> bringing it to the location <strong>and</strong><br />
condition necessary for it to be capable of operating in the<br />
manner intended by management. All assets are measured<br />
subsequently at fair value.<br />
L<strong>and</strong> <strong>and</strong> buildings used for the Trust’s services or for<br />
administrative purposes are stated in the Statement of<br />
Financial Position at their revalued amounts, being the<br />
fair value at the date of revaluation less any subsequent<br />
accumulated depreciation <strong>and</strong> impairment losses.<br />
Revaluations are performed with sufficient regularity to<br />
ensure that carrying amounts are not materially different<br />
from those that would be determined at the end of the<br />
<strong>report</strong>ing period.<br />
Fair values are determined as follows:<br />
• L<strong>and</strong> <strong>and</strong> non-specialised buildings – market value for<br />
existing use; <strong>and</strong><br />
• Specialised buildings - Modern Equivalent Asset (MEA)<br />
value, as adjusted for wear <strong>and</strong> tear.<br />
All l<strong>and</strong> <strong>and</strong> buildings are restated to fair value in<br />
accordance with IAS 16 <strong>and</strong> Monitor guidance, using<br />
professional valuations every five years <strong>and</strong> an interim<br />
valuation on an annual basis to ensure that fair values<br />
are not materially different from the carrying amounts.<br />
Valuations are carried out by professionally qualified<br />
valuers in accordance with the Royal Institute of Chartered<br />
Surveyors (RICS) Appraisal <strong>and</strong> Valuation Manual based on<br />
MEA. An interim valuation of l<strong>and</strong>, buildings <strong>and</strong> dwellings<br />
was carried out by DVS Property (Independent Chartered<br />
Surveyors). Buildings were valued on a MEA basis as at 31<br />
March 20<strong>12</strong>.<br />
In order to derive relevant build costs, DVS Property gave<br />
regard to the RICS Build Cost Indices in consultation<br />
with their own building surveyor. In accordance with the<br />
RICS <strong>and</strong> Treasury’s Financial Reporting Manual Valuation<br />
Guidelines, an instant build approach was assumed in that<br />
the Modern Equivalent Assets would be constructed at<br />
the date of valuation without phasing or lead in periods.<br />
It also assumes the site is cleared <strong>and</strong> ready to take the<br />
new buildings <strong>and</strong> therefore there is no allowance for the<br />
demolition of any existing buildings or site preparation.<br />
Assets in the course of construction for service or<br />
administration purposes are carried at cost, less any<br />
impairment loss. Cost includes professional fees but<br />
not borrowing costs, which are recognised as expenses<br />
immediately, as allowed by IAS 23 (Borrowing Costs)<br />
for assets held at fair value. Assets are revalued <strong>and</strong><br />
depreciation commences when they are brought into use.<br />
(ii) Subsequent expenditure<br />
Where subsequent expenditure enhances an asset beyond<br />
its original specification, the directly attributable cost<br />
is capitalised. Where subsequent expenditure restores<br />
the asset to its original specification, the expenditure is<br />
capitalised <strong>and</strong> any existing carrying value of the item<br />
replaced, is charged to operating expenses.<br />
(iii) Depreciation<br />
Items of Property are depreciated on their current value<br />
over their remaining useful economic lives (UEL) as assessed<br />
by the NHS Foundation Trust’s professional valuers in a<br />
manner consistent with the consumption of economic<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 95
ANNUAL ACCOUNTS<br />
or service delivery benefits. Freehold l<strong>and</strong> is considered<br />
to have infinite life <strong>and</strong> is not depreciated. Leaseholds<br />
are depreciated over the primary lease term. Plant <strong>and</strong><br />
Equipment is depreciated on current cost evenly over the<br />
estimated UEL.<br />
Property, Plant <strong>and</strong> Equipment which has been reclassified<br />
as ‘Held for Sale’ ceases to be depreciated upon the<br />
reclassification. Assets in the course of construction are not<br />
depreciated until the asset is brought into use.<br />
The following UELs apply to each individual asset category<br />
based on st<strong>and</strong>ard asset lives adjusted for local use <strong>and</strong><br />
expected technology changes:<br />
• L<strong>and</strong> - The remaining useful life of the asset. L<strong>and</strong> is<br />
generally not depreciated because considered to have<br />
infinite life.<br />
• Non-residential buildings <strong>and</strong> dwellings - average<br />
remaining useful life of the building block in accordance<br />
with the Independent Qualified Valuer‘s <strong>report</strong><br />
• Plant <strong>and</strong> Machinery - 5 to 15 years<br />
• Transport equipment - 7 years<br />
• Furniture <strong>and</strong> Fittings - 3 to 10 years<br />
• Office <strong>and</strong> IT equipment - 3 to 5 years<br />
• Mainframe IT type installation - 5 to 9 years<br />
• Computer software licenses - the shorter of 5 years or<br />
length of licenses.<br />
(iv) Revaluation<br />
Increases in asset values arising from revaluations are<br />
recognised in the revaluation reserve, except where, <strong>and</strong><br />
to the extent that, they reverse an impairment previously<br />
recognised in operating expenses, in which case they are<br />
recognised in operating income.<br />
Decreases in asset values <strong>and</strong> impairments are charged<br />
to the revaluation reserve to the extent that there is an<br />
available balance for the asset concerned, <strong>and</strong> thereafter<br />
are charged to operating expenses.<br />
Gains <strong>and</strong> losses recognised in the revaluation reserve are<br />
<strong>report</strong>ed in the Statement of Comprehensive Income as an<br />
item of other comprehensive income.<br />
(v) Impairment<br />
Impairments that are due to a loss of economic benefits<br />
or service potential in the asset are charged to operating<br />
expenses. If sufficent revaluation reserve is available a<br />
compensating transfer is made from the revaluation reserve<br />
to the income <strong>and</strong> expenditure reserve of an amount equal<br />
to the lower of:<br />
(i) the impairment charged to operating expenses; <strong>and</strong><br />
(ii) the balance in the revaluation reserve attributable to that<br />
asset before the impairment.<br />
An impairment arising from a loss of economic benefit or<br />
service potential is reversed when, <strong>and</strong> to the extent that,<br />
the circumstances that gave rise to the loss are reversed.<br />
Reversals are recognised in operating income to the extent<br />
that the asset is restored to the carrying amount it would<br />
have had if the impairment had never been recognised.<br />
Any remaining reversal is recognised in the revaluation<br />
reserve. Where, at the time of the original impairment,<br />
a transfer was made from the revaluation reserve to the<br />
income <strong>and</strong> expenditure reserve, an amount is transferred<br />
back to the revaluation reserve when the impairment<br />
reversal is recognised.<br />
1.6.3 De-recognition<br />
Assets intended for disposal are reclassified as ‘Held for<br />
Sale’ once all the following criteria are met:<br />
• The asset is available for immediate sale in its present<br />
condition subject only to terms which are usual <strong>and</strong><br />
customary for such sales;<br />
• The sale must be highly probable i.e.<br />
i) Management are committed to selling the asset;<br />
ii) An active programme has begun to find a buyer <strong>and</strong><br />
complete the sale;<br />
iii) The asset is being marketed at a reasonable price;<br />
iv) The sale is expected to be completed within<br />
<strong>12</strong> months of the date of classification <strong>and</strong> as ‘Held for<br />
Sale’; <strong>and</strong><br />
v) The actions needed to complete the plan indicate<br />
it is unlikely that the plan will be terminated or that<br />
significant changes will be made to it.<br />
Following reclassification, the assets are measured at the<br />
lower of their existing carrying amount <strong>and</strong> their ’fair value<br />
less costs to sell’. Depreciation ceases to be charged <strong>and</strong><br />
assets are not revalued, except where the ’fair value less<br />
costs to sell’ falls below the carrying amount. Assets are derecognised<br />
when all material sale contract conditions have<br />
been met.<br />
Property, Plant <strong>and</strong> Equipment which is to be scrapped or<br />
demolished does not qualify for recognition as ‘Held for<br />
Sale’ <strong>and</strong> instead is retained as an operational asset <strong>and</strong> the<br />
asset’s economic life is adjusted. The asset is de-recognised<br />
when scrapping or demolition occurs.<br />
1.6.4 Donated assets<br />
Donated <strong>and</strong> grant funded property, plant <strong>and</strong> equipment<br />
assets are capitalised at their fair value on receipt. The<br />
donation/grant is credited to income at the same time,<br />
96 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
unless the donor has imposed a condition that the future<br />
economic benefits embodied in the grant are to be<br />
consumed in a manner specified by the donor, in which<br />
case, the donation/grant is deferred within liabilities <strong>and</strong> is<br />
carried forward to future financial years to the extent that<br />
the condition has not yet been met.<br />
The donated <strong>and</strong> grant funded assets are subsequently<br />
accounted for in the same manner as other items of<br />
property, plant <strong>and</strong> equipment.<br />
1.7 Intangible assets<br />
1.7.1 Recognition<br />
Intangible assets are non-monetary assets without physical<br />
substance which are capable of being sold separately<br />
from the rest of the Trust’s business or which arise from<br />
contractual or other legal rights. They are capitalised when<br />
they are capable of being used in the Trust’s activities for<br />
more than one year, <strong>and</strong> can be valued <strong>and</strong> have a cost of<br />
at least £5,000.<br />
(i) Internally generated intangible assets<br />
Internally generated goodwill, br<strong>and</strong>s, mastheads,<br />
publishing titles, customer lists <strong>and</strong> similar items are not<br />
capitalised as intangible assets.<br />
Expenditure on research is not capitalised.<br />
Expenditure on development is capitalised only where all<br />
the following can be demonstrated:<br />
• the project is technically feasible to the point of<br />
completion <strong>and</strong> will result in an intangible asset for sale<br />
or use<br />
• the Trust intends to complete the asset <strong>and</strong> sell or use it<br />
• the Trust has the ability to sell or use the asset<br />
• the way in which intangible assets will generate probable<br />
future economic or service delivery benefits e.g. the<br />
presence of a market for its output or, where it is to be<br />
used for internal use, the usefulness of the asset<br />
• adequate financial, technical or other resources are<br />
available to the Trust to complete the development <strong>and</strong><br />
sell or use the asset, <strong>and</strong><br />
• the Trust can measure reliably the expenses attributable<br />
to the asset during development.<br />
(ii) Software<br />
Software which is integral to the operation of hardware<br />
e.g. an operating system is capitalised as part of the<br />
relevant item of property, plant <strong>and</strong> equipment. Software<br />
which is not integral to the operation of hardware e.g.<br />
application software, is capitalised as an intangible asset.<br />
Costs associated with maintaining software are recognised<br />
as an expense when incurred.<br />
Capitalised computer software is amortised over the<br />
expected useful economic life.<br />
1.7.2 Measurement<br />
Intangible assets are recognised initially at cost, comprising<br />
directly all attributable costs needed to create, produce<br />
<strong>and</strong> prepare the asset to the point that it is capable<br />
of operating in a manner intended by management.<br />
Subsequently intangible assets are measured at fair<br />
value. Increases in asset values arising from valuations are<br />
recognised in the revaluation reserve, except where, <strong>and</strong><br />
to the extent that, they reverse an impairment previously<br />
recognised in operating expenses, in which case they are<br />
recognised in operating income. Decreases in asset values<br />
<strong>and</strong> impairments are charged to the revaluation reserve<br />
to the extent that there is an available balance for the<br />
asset concerned, <strong>and</strong> thereafter are charged to operating<br />
expenses. Gains <strong>and</strong> losses recognised in the revaluation<br />
reserve are <strong>report</strong>ed in the Statement of Comprehensive<br />
Income as an item of other comprehensive income.<br />
Intangible assets ‘Held for Sale’ are measured at the lower<br />
of their carrying amount or ’fair value less cost to sell’.<br />
1.7.3 Amortisation<br />
Intangible assets are amortised over their expected useful<br />
economic lives in a manner consistent with consumption of<br />
economic or service delivery benefits.<br />
1.8 Government grants<br />
Government grants are grants from Government bodies<br />
other than income from Primary Care Trusts or NHS<br />
Foundation Trusts for the provision of services. Grants<br />
from the Department of Health are accounted for as<br />
Government grants. Where the Government grant is used<br />
to fund revenue expenditure, it is taken to the Statement of<br />
Comprehensive Income to match that expenditure.<br />
1.9 Inventories<br />
Inventories are valued at the lower of cost <strong>and</strong> net<br />
realisable value.<br />
1.10 Cash <strong>and</strong> cash equivalents<br />
Cash <strong>and</strong> cash equivalents comprise of cash in h<strong>and</strong> <strong>and</strong><br />
on dem<strong>and</strong> deposits <strong>and</strong> other short term highly liquid<br />
investments that are readily convertible to a known amount<br />
of cash <strong>and</strong> are subject to an insignificant risk of changes<br />
in value. These balances exclude monies held in the Trust’s<br />
bank account belonging to patients (see third party assets<br />
in note 1.19 below).<br />
Account balances are only set off where a formal<br />
agreement has been made with the bank to do so. In<br />
all other cases overdrafts are disclosed within payables.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 97
ANNUAL ACCOUNTS<br />
Interest earned on bank <strong>accounts</strong> <strong>and</strong> interest charged<br />
on overdrafts is recorded respectively as finance income<br />
<strong>and</strong> finance cost in the periods to which they relate. Bank<br />
charges are recorded as operating expenses in the periods<br />
to which they relate.<br />
1.11 Financial instruments <strong>and</strong> financial liabilities<br />
1.11.1 Recognition<br />
Financial assets <strong>and</strong> financial liabilities which arise from<br />
contracts for the purchase or sale of non-financial items<br />
(such as goods or services) which are entered into in<br />
accordance with the Trust’s normal purchase, sale or usage<br />
requirements are recognised when, the goods or services<br />
are delivered.<br />
Financial assets or financial liabilities in respect of<br />
assets acquired or disposed of through finance leases<br />
are recognised <strong>and</strong> measured in accordance with the<br />
accounting policy for leases described below.<br />
Regular purchases or sales are recognised <strong>and</strong> derecognised,<br />
as applicable, using the Trade date.<br />
All other financial assets <strong>and</strong> financial liabilities are<br />
recognised when the Trust becomes a party to the<br />
contractual provisions of the instrument.<br />
1.11.2 De-recognition<br />
All financial assets are de-recognised when the rights to<br />
receive cash flows from the assets have expired or the Trust<br />
has transferred substantially all of the risks <strong>and</strong> rewards of<br />
ownership. Financial liabilities are de-recognised when the<br />
obligation is discharged, cancelled or expires.<br />
1.11.3 Classification <strong>and</strong> measurement<br />
(i) Financial assets <strong>and</strong> financial liabilities at Fair value<br />
through Income <strong>and</strong> Expenditure’<br />
Financial assets <strong>and</strong> financial liabilities at Fair value<br />
through Income <strong>and</strong> Expenditure are financial assets or<br />
financial liabilities held for trading. A financial asset or<br />
liability is classified in this category if acquired principally<br />
for the purpose of selling in the short-term. Derivatives<br />
are also categorised as held for trading unless they are<br />
designated as hedges. Derivatives which are embedded<br />
in other contracts but which are not closely-related to<br />
those contracts are separated out from those contracts<br />
<strong>and</strong> measured in this category. Assets <strong>and</strong> liabilities in this<br />
category are classified as current assts <strong>and</strong> current liabilities.<br />
These financial assets <strong>and</strong> financial liabilities are recognised<br />
initially at fair value, with transaction costs charged to<br />
the the income <strong>and</strong> expenditure account. Subsequent<br />
movements in the fair value are recognised as gains <strong>and</strong><br />
losses in the Statement of Comprehensive Income.<br />
(ii) Loans <strong>and</strong> receivables<br />
Loans <strong>and</strong> receivables are non-derivative financial assets<br />
with fixed or determinable payments which are not quoted<br />
in the active market. They are included in current assets.<br />
The Trust’s loans <strong>and</strong> receivables comprise: current<br />
investments, cash <strong>and</strong> cash equivalents, NHS receivables,<br />
accrued income <strong>and</strong> other receivables.<br />
Loans <strong>and</strong> receivables are recognised initially at fair value,<br />
net of transactions costs, <strong>and</strong> are measured subsequently<br />
at amortised cost, using the effective interest method.<br />
The effective interest rate is the rate that discounts exactly<br />
estimated future cash receipts through the expected life of<br />
the financial asset or, when appropriate, a shorter period,<br />
to the net carrying amount of the financial asset.<br />
Interest on loans <strong>and</strong> receivables is calculated using the<br />
effective interest method <strong>and</strong> credited to the Statement of<br />
Comprehensive Income.<br />
(iii) Available-for-sale financial assets<br />
Available for sale financial assets are non-derivative financial<br />
assets which are either designated in this category or not<br />
classified in any of the other categories. They are included<br />
in long-term assets unless the Trust intends to dispose<br />
of them within <strong>12</strong> months of the Statement of Financial<br />
Position date.<br />
Available-for-sale financial assets are recognised initially<br />
at fair value, including transaction costs, <strong>and</strong> measured<br />
subsequently at fair value, with gains or losses recognised in<br />
reserves <strong>and</strong> <strong>report</strong>ed in the Statement of Comprehensive<br />
Income as an item of other comprehensive income. When<br />
items classified as available for sale are sold or impaired,<br />
the accumulated fair value adjustments recognised are<br />
transferred from reserves <strong>and</strong> recognised in Finance Costs<br />
in the Statement of Comprehensive Income.<br />
(iv) Other Financial liabilities<br />
All other financial liabilities are recognised initially at fair<br />
value, net of transaction costs incurred, <strong>and</strong> measured<br />
subsequently at amortised cost using the effective interest<br />
method. The effective interest rate is the rate that discounts<br />
future cash payments through the expected life of the<br />
financial liability or, when appropriate, a shorter period, to<br />
the net carrying amount of the financial liability.<br />
They are included in current liabilities except for amounts<br />
payable more than <strong>12</strong> months after the Statement of<br />
Financial Position date, which are classified as long-term<br />
liabilities.<br />
Interest on financial liabilities carried at amortised cost is<br />
calculated using the effective interest method <strong>and</strong> charged<br />
to Finance Costs. Interest on financial liabilities taken out to<br />
98 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
finance property, plant <strong>and</strong> equipment or intangible assets<br />
is not capitalised as part of the cost of those assets.<br />
(v) Determination of fair value<br />
For financial assets <strong>and</strong> financial liabilities carried at fair<br />
value, the carrying amounts are determined from quoted<br />
market prices, independent appraisals <strong>and</strong> analysis of<br />
discounted cash flows.<br />
(vi) Impairment of financial assets<br />
At the Statement of Financial Position date, the Trust<br />
assesses whether any financial assets, other than those held<br />
at fair value through income <strong>and</strong> expenditure are impaired.<br />
Financial assets are impaired <strong>and</strong> impairment losses are<br />
recognised, if <strong>and</strong> only if, there is objective evidence<br />
of impairment as a result of one or more events which<br />
occurred after the initial recognition of the assets <strong>and</strong><br />
which has an impact on the estimated future cash flows of<br />
the asset.<br />
For financial assets carried at amortised cost, the amount of<br />
the impairment loss is measured as the difference between<br />
the asset’s carrying amount <strong>and</strong> the present value of the<br />
revised cash flows discounted at the asset’s original effective<br />
interest rate. The loss is recognised in the Statement of<br />
Comprehensive Income <strong>and</strong> the carrying amount of the<br />
asset is reduced directly or through the use of an allowance<br />
account/bad debt provision.<br />
1.<strong>12</strong> Leases<br />
1.<strong>12</strong>.1 Finance leases<br />
(i) Lessee<br />
Where substantially all risks <strong>and</strong> rewards of ownership of a<br />
leased asset are borne by the Trust, the asset is recorded as<br />
Property, Plant <strong>and</strong> Equipment <strong>and</strong> a corresponding liability<br />
is recorded. The value at which both are recognised is the<br />
lower of the fair value of the asset or the present value<br />
of the minimum lease payments, discounted using the<br />
interest rate implicit in the lease. The interest rate is that<br />
which produces a constant periodic rate of interest on the<br />
outst<strong>and</strong>ing liability.<br />
The assets <strong>and</strong> liabilities are recognised at the inception<br />
of the lease, <strong>and</strong> are de-recognised when the liability<br />
is discharged, cancelled or expires. The annual rental is<br />
split between the repayment of the liability <strong>and</strong> a finance<br />
cost. The annual finance cost is calculated by applying<br />
the implicit interest rate to the outst<strong>and</strong>ing liability<br />
<strong>and</strong> is charged to ”Finance Costs” in the Statement of<br />
Comprehensive Income.<br />
(ii) Lessor<br />
Assets leased to others under agreements, which transfer<br />
substantially all the risks <strong>and</strong> rewards of ownership, with<br />
or without ultimate legal title are also classified as finance<br />
leases. When assets are held subject to a finance lease the<br />
present value of the lease payments, discounted at the rate<br />
of interest implicit in the lease, is recognised as a receivable.<br />
The difference between the total payments receivable<br />
under the lease <strong>and</strong> the present value of the receivable is<br />
recognised as unearned finance income, which is allocated<br />
to accounting periods to reflect a constant periodic rate of<br />
return.<br />
1.<strong>12</strong>.2 Operating leases<br />
(i) Lessee<br />
Other leases are regarded as operating leases <strong>and</strong> the<br />
rentals are charged to operating expenses on a straight line<br />
basis over the term of the lease. Operating lease incentives<br />
received are added to the lease rentals <strong>and</strong> charged to<br />
operating expenses over the life of the lease.<br />
(ii) Lessor<br />
Assets leased to third parties under agreements which<br />
do not transfer substantially all the risks <strong>and</strong> rewards of<br />
ownership are classified as operating leases. The leased<br />
assets are included within Property, Plant <strong>and</strong> Equipment in<br />
the Trust’s Statement of Financial Position <strong>and</strong> depreciation<br />
is provided on the depreciable amount of these assets on<br />
a systematic basis in accordance with the Trust’s policy.<br />
Lease income is recognised on a straight-line basis over the<br />
period of the lease unless another systematic basis is more<br />
representative of the accruing benefit.<br />
1.<strong>12</strong>.3 Leases of L<strong>and</strong> <strong>and</strong> Buildings<br />
Where a lease is for l<strong>and</strong> <strong>and</strong> buildings, the l<strong>and</strong><br />
component is separated from the building component <strong>and</strong><br />
the classification for each is assessed separately. Leased l<strong>and</strong><br />
is treated as an operating lease.<br />
1.13 Provisions<br />
The Trust provides for legal <strong>and</strong> compensation obligations<br />
that are of certain timing or amount at the Statement of<br />
Financial Position date on the basis of the best estimate of<br />
the expenditure required to settle the obligation. Where<br />
the effect of the time value of money is significant, the<br />
estimated risk-adjusted cash flows are discounted using<br />
HM Treasury’s discount rate of 2.2% in real terms, except<br />
for early retirement provisions <strong>and</strong> injury benefit provisions<br />
which both use the HM Treasury’s pension discount rate of<br />
2.9% in real terms.<br />
(i) Clinical negligence costs<br />
The NHS Litigation Authority (NHSLA) operates a risk<br />
pooling scheme under which the Trust pays an annual<br />
contribution to the NHSLA, which, in return, manages<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 99
ANNUAL ACCOUNTS<br />
all clinical negligence claims. Although the NHSLA is<br />
administratively responsible for all clinical negligence cases,<br />
the legal liability remains with the Trust. The total value<br />
of clinical negligence provisions carried by the NHSLA on<br />
behalf of the Trust is disclosed at note 18.<br />
(ii) Non-clinical risk pooling<br />
The Trust participates in the Property Expenses Scheme <strong>and</strong><br />
the Liabilities to Third Parties Scheme. Both are risk pooling<br />
arrangements under which the Trust pays an annual<br />
contribution to the NHSLA <strong>and</strong> in return receives assistance<br />
with the cost of claims arising. The annual membership<br />
contributions <strong>and</strong> any excesses payable in respect of<br />
particular claims are charged to operating expenses when<br />
the liability arises.<br />
1.14 Contingencies<br />
Contingent assets (that is assets arising from past events<br />
whose existence will only be confirmed by one or more<br />
future events not wholly within the Trust’s control) are not<br />
recognised as assets, but are disclosed in note where an<br />
inflow of economic benefits is probable.<br />
Contingent liabilities are not recognised, but are disclosed<br />
in a note, unless the probability of a transfer of economic<br />
benefits is remote. Contingent liabilities are defined as:<br />
• Possible obligations arising from past events whose<br />
existence will be confirmed only by the occurrence of<br />
one or more uncertain future events not wholly within<br />
the Trust’s control, or<br />
• Present obligations arising from past events but for<br />
which it is not probable that a transfer of economic<br />
benefits will arise or for which the amount of the<br />
obligation cannot be measured with sufficient reliability.<br />
1.15 Public Dividend Capital<br />
Public Dividend Capital (PDC) is a type of public sector<br />
equity finance based on the excess of assets over liabilities<br />
at the time of establishment of the predecessor NHS Trust.<br />
HM Treasury has determined that PDC is not a financial<br />
instrument within the meaning of IAS 32 (Financial<br />
Instruments).<br />
An amount, reflecting the cost of capital utilised by<br />
the NHS foundation trust, is payable as PDC each year.<br />
The charge is calculated at the rate set by HM Treasury<br />
(currently 3.5%) on the average relevant net assets of the<br />
NHS foundation trust during the financial year. Relevant net<br />
assets are calculated as the value of all assets less the value<br />
of all liabilities, except for:<br />
(i) donated assets (including lottery funded assets)<br />
(ii) net cash balances held with the Government Banking<br />
Services (GBS); excluding cash balances held in GBS<br />
<strong>accounts</strong> that relate to a short-term working capital<br />
facility, <strong>and</strong><br />
(iii) any PDC dividend balance receivable or payable.<br />
In accordance with the requirements laid down by the<br />
Department of Health (as the issuer of PDC), the dividend<br />
for the year is calculated on the actual average relevant<br />
net assets as set out in the pre-audit version of the annual<br />
<strong>accounts</strong>. The estimated dividend is not revised should any<br />
adjustment to net assets occur as a result the audit of the<br />
annual <strong>accounts</strong>.<br />
1.16 Value Added Tax<br />
Most activities of the Trust are outside the scope of VAT<br />
<strong>and</strong>, in general, output tax does not apply <strong>and</strong> input tax on<br />
purchases is not recoverable. Irrecoverable VAT is charged<br />
to the relevant expenditure category or included in the<br />
capitalised purchase cost of fixed assets. Where output tax<br />
is charged or input VAT is recoverable, the amounts are<br />
stated net of VAT.<br />
1.17 Corporation Tax<br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust is<br />
a Health Service Body under the definition of section<br />
519A Income <strong>and</strong> Corporation Taxes Act (ICTA) 1988<br />
<strong>and</strong> accordingly is exempt from taxation in respect of<br />
income <strong>and</strong> capital gains within categories covered by<br />
this Act. There is a power for HM Treasury to disapply the<br />
exemption in relation to specified activities of a Foundation<br />
Trust (section 519A (93) to (8) ICTA 1988). The Trust is not<br />
within the scope of corporation tax in respect of activities<br />
which are not related to, or ancillary to, the provision of<br />
healthcare, as the profits derived from these activities do<br />
not exceed £50,000 per annum.<br />
1.18 Foreign exchange<br />
The functional <strong>and</strong> presentational currency of the Trust is<br />
sterling.<br />
A transaction which is denominated in a foreign currency is<br />
translated into the functional currency at the spot exchange<br />
rate on the date of payment for the transaction.<br />
Where the Trust has assets or liabilities denominated in a<br />
foreign currency at the Statement of Financial Position date:<br />
• monetary items (other than financial instruments<br />
measured at ‘fair value’ through income <strong>and</strong> expenditure)<br />
are translated at the spot exchange rate on 31 March<br />
• non-monetary assets <strong>and</strong> liabilities measured at historical<br />
cost are translated using the spot exchange rate at the<br />
date of the transaction, <strong>and</strong><br />
• non-monetary assets <strong>and</strong> liabilities measured at fair value<br />
are translated using the spot exchange rate at the date<br />
the fair value was determined.<br />
100 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
Exchange gains or losses on monetary items (arising on<br />
settlement of the transaction or on re-translation of the<br />
Statement of Financial Position date) are recognised in<br />
income or expense in the period in which they arise.<br />
Exchange gains or losses on non-monetary assets <strong>and</strong><br />
liabilities are recognised in the same manner as other gains<br />
<strong>and</strong> losses on these items.<br />
1.19 Third party assets<br />
Assets belonging to third parties (such as money held on<br />
behalf of patients) are not recognised in the <strong>accounts</strong><br />
since the Trust has no beneficial interest in them. However,<br />
they are disclosed in a separate note in the <strong>accounts</strong><br />
in accordance with the requirements of HM Treasury’s<br />
Financial Reporting Manual. See note 27 for details.<br />
1.20 Losses <strong>and</strong> special payments<br />
Losses <strong>and</strong> special payments are charged to the relevant<br />
functional headings on a cash basis, including losses which<br />
would have been made good through insurance cover<br />
had Foundation Trusts not been bearing its own risk (with<br />
insurance premiums then being included as normal revenue<br />
expenditure).<br />
The total value <strong>and</strong> number of special payments is shown in<br />
note 29 to the <strong>accounts</strong>.<br />
1.21 Related parties<br />
Government Departments <strong>and</strong> their agencies are<br />
considered by HM Treasury to be related parties. During the<br />
year <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
has had a significant number of material transactions with<br />
Government Departments <strong>and</strong> their agencies. These entities<br />
are listed in note 23.<br />
The Trust also receives revenue <strong>and</strong> capital payments from<br />
the <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
Charitable Fund. The Charity is registered with the Charity<br />
Commissioners (Charity Number 1061659) <strong>and</strong> has its own<br />
Trustees drawn from the NHS Foundation Trust Board. It<br />
produces a set of annual <strong>accounts</strong> <strong>and</strong> an annual <strong>report</strong><br />
(separate to that of the NHS Foundation Trust based on UK<br />
GAAP <strong>and</strong> Charities SORP).<br />
Although the Trust has no ownership interest in the Charity,<br />
the composition of the charity trustees result in it being<br />
deemed a subsidiary under IAS27 (Consolidated <strong>and</strong><br />
Separated Financial Statements). HM Treasury has granted<br />
dispensation to the application of IAS 27 (revised) by NHS<br />
foundation trusts in relation to the consolidation of NHS<br />
charitable funds for <strong>2011</strong>/<strong>12</strong> <strong>and</strong> 20<strong>12</strong>/13.<br />
1.22 Partially completed spells<br />
Partially completed spells recognise the value of unfinished<br />
treatment episodes for which Trusts are entitled to accrue<br />
income but would not actually receive funding until the<br />
episode is complete.<br />
The estimation is based on the average HRG price by<br />
specialty <strong>and</strong> point of delivery of the fully coded spells in<br />
the preceding months.<br />
1.23 Transforming community services (TCS)<br />
The community health services previously provided by NHS<br />
City <strong>and</strong> Hackney transferrred to <strong>Homerton</strong> <strong>University</strong><br />
<strong>Hospital</strong> NHS Foundation Trust on 1 April <strong>2011</strong>. The<br />
transfer involved the TUPE of staff <strong>and</strong> a three year contract<br />
was signed. The transaction did not include any transfer of<br />
non-current assets.<br />
This transaction represents the transfer of services between<br />
public sector bodies which are under common control<br />
<strong>and</strong> therefore is classified as Machinery of Government<br />
Change. This transaction meets the definition of a Group<br />
Reconstruction under IFRS 3 Business Combinations<br />
<strong>and</strong> therefore falls outside the scope of that St<strong>and</strong>ard.<br />
In accordance with the FT ARM principles of merger<br />
accounting should have been applied to this transaction.<br />
However the Department of Health has considered the<br />
feasibility of restating Statement of Comprehensive Income<br />
under merger accounting for all local bodies (including<br />
NHS foundation trusts) <strong>and</strong> considers it is impracticable to<br />
undertake this restatement for all bodies in light of cost <strong>and</strong><br />
availability of information.<br />
To meet these requirements, the Trust has only restated its<br />
Statement of Financial Position <strong>and</strong> associated notes. In<br />
addition the Trust has <strong>report</strong>ed <strong>12</strong> months of combined<br />
activity in its <strong>2011</strong>/<strong>12</strong> balances.<br />
1.24 Key areas of estimation <strong>and</strong> judgement<br />
The key areas of estimation <strong>and</strong> judgement used in the<br />
preparation of the <strong>accounts</strong> have been disclosed within<br />
other sections of the accounting policy notes. These<br />
include:<br />
• Provisions for impairments of receivables, injury benefit<br />
claims, early retirements <strong>and</strong> others (note 17)<br />
• Estimates of partially completed patient episodes (note<br />
1.22), <strong>and</strong><br />
• Depreciation rates applied to property, plant <strong>and</strong><br />
equipment (note 10).<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 101
ANNUAL ACCOUNTS<br />
1.25 Restatement of balances<br />
As per note 1.23 the Trust has restated its balances for the TCS transaction. In addition the FReM’s interpretation of IAS<br />
20, ‘Accounting for Government Grants <strong>and</strong> Disclosure’ has resulted in the need to restate certain balances within these<br />
<strong>accounts</strong>. The restatements are summarised as follows:<br />
Statement of Financial Position<br />
Closing balance<br />
as at<br />
31 March <strong>2011</strong><br />
£000<br />
2009/10<br />
IAS 20<br />
Adjustment<br />
£000<br />
Restated<br />
Opening<br />
Balance as at<br />
1 April 2010<br />
2010/11<br />
In Year<br />
movements<br />
£000<br />
2010/11<br />
IAS 20<br />
Adjustment<br />
£000<br />
2010/11<br />
TCS<br />
Transaction<br />
£000<br />
Restated<br />
closing<br />
balance as<br />
at 31 March<br />
<strong>2011</strong><br />
£000<br />
Non-current assets 118,614 - 118,614 (255) - - 118,359<br />
Current assets<br />
Accrued income 3,522 - 3,522 (799) 243 2,966<br />
Other receivables 2,722 - 2,722 220 - 31 2,973<br />
Other current assets 21,885 - 21,885 779 - - 22,664<br />
Total current assets 28,<strong>12</strong>9 - 28,<strong>12</strong>9 200 - 274 28,603<br />
Current liabilities<br />
Deferred income (6,671) 371 (6,300) 2,380 827 (10) (3,103)<br />
Other payables (4,942) - (4,942) - - (264) (5,206)<br />
Other current liabilities (9,624) - (9,624) (2,589) - - (<strong>12</strong>,213)<br />
Total current liabilities (21,237) 371 (20,866) (209) 827 (274) (20,522)<br />
Non-current liabilities (5,001) - (5,001) 306 - - (4,695)<br />
Total assets employed <strong>12</strong>0,505 371 <strong>12</strong>0,876 42 827 - <strong>12</strong>1,745<br />
Taxpayers’ equity<br />
Public dividend capital 83,175 - 83,175 - - - 83,175<br />
Revaluation reserve 21,898 - 21,898 1,248 (4) - 23,142<br />
Donated asset reserve 2,966 (2,966) - 1,856 (1,856) - -<br />
Retained earnings reserve <strong>12</strong>,466 3,337 15,803 (3,062) 2,687 - 15,428<br />
Total taxpayers’ equity <strong>12</strong>0,505 371 <strong>12</strong>0,876 42 827 - <strong>12</strong>1,745<br />
2010/11<br />
Position as at 31 March <strong>2011</strong><br />
£000<br />
2010/11<br />
IAS 20 Adjustment<br />
£000<br />
2010/11<br />
Restated position as at<br />
31 March <strong>2011</strong> £000<br />
Operating income <strong>and</strong> expenditure<br />
Operating income 183,017 - 183,017<br />
Other income 4,713 3,141 7,854<br />
Transfer from donated asset reserve 387 (387) -<br />
Total operating income 188,117 2,754 190,871<br />
Other operating expenses (182,621) - (182,621)<br />
Impairments charged to operating expenses (5,105) (67) (5,172)<br />
Total operating expenses (187,726) (67) (187,793)<br />
Operating surplus 391 2,687 3,078<br />
The cashflow statement balances have been restated in note 20.1<br />
102 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
2. Segmental analysis<br />
All activities of the Trust are considered to be one segment, Healthcare. There are no individual <strong>report</strong>able segments on<br />
which to make disclosures.<br />
3. Operating income from continuing operations<br />
3.1 Income from activities<br />
<strong>2011</strong>/<strong>12</strong><br />
£000<br />
2010/11<br />
£000<br />
Elective income 21,759 22,300<br />
Non-elective income 47,272 48,185<br />
Outpatient income 32,994 30,592<br />
A&E Income 9,061 8,326<br />
Other type of activity income 54,393 51,783<br />
Community income 47,200 -<br />
Private patient income 588 508<br />
Other non-protected clinical income 9,890 6,893<br />
Total income from activities 223,157 168,587<br />
Other operating income<br />
Research <strong>and</strong> development 504 489<br />
Education <strong>and</strong> training 11,708 11,165<br />
Donated assets <strong>and</strong> deferred income recognition 1,477 -<br />
Profit on disposal (non current assets) - 58<br />
Non-patient care services to other bodies 2,571 2,718<br />
Other income 4,260 7,854<br />
Total other operating income 20,520 22,284<br />
Total operating income 243,677 190,871<br />
Other income includes rent (£1.1m), staff recharges (£1.5m), nursery income (£0.4m), <strong>and</strong> catering income (£0.3m).<br />
<strong>2011</strong>/<strong>12</strong><br />
£000<br />
2002/03<br />
£000<br />
3.2 Private patient income<br />
Private patient income 588 224<br />
Total patient related income 223,157 83,880<br />
Private patient income (%) 0.3% 0.3%<br />
Section 44 of the NHS Act 2006 requires that the proportion of private patient income to the total patient related<br />
income of NHS foundation trusts should not exceed its proportion whilst the body was an NHS Trust in 2002/03,<br />
its base year. The Trust’s Private Patient Cap is set at 0.3% <strong>and</strong> was not exceeded during the year ended 31 March<br />
20<strong>12</strong>.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 103
ANNUAL ACCOUNTS<br />
3.3 Income by source<br />
<strong>2011</strong>/<strong>12</strong><br />
£000<br />
2010/11<br />
£000<br />
NHS Foundation Trusts 4,113 4,315<br />
NHS Trusts 1,059 403<br />
Strategic Health Authorities 11,367 11,189<br />
Primary Care Trusts 216,518 163,968<br />
Department of Health 541 28<br />
NHS Other 50 349<br />
Local Authorities 3,659 2,058<br />
Non NHS: Private Patients 588 508<br />
Non NHS: Overseas Patients 41 156<br />
NHS Injury Scheme (was Road Traffic Act) 830 684<br />
Other operating income 4,911 7,213<br />
Total 243,677 190,871<br />
NHS Injury Scheme income is subject to a nationally prescribed provision for doubtful debts of 10.5% (2010/11<br />
9.6%) to reflect expected rates of collection.<br />
4. Operating expenses<br />
<strong>2011</strong>/<strong>12</strong><br />
£000<br />
2010/11<br />
£000<br />
Services from other NHS Foundation Trusts 266 -<br />
Services from other NHS Trusts 558 -<br />
Services from other NHS Bodies 1 1<br />
Purchase of healthcare from non-NHS bodies 377 163<br />
Directors’ costs 1,220 1,317<br />
Non executive Directors’ costs <strong>12</strong>4 114<br />
Staff costs 157,471 <strong>12</strong>1,056<br />
Drugs costs 11,049 10,748<br />
Supplies <strong>and</strong> services - clinical (excluding drug costs) 14,741 11,263<br />
Supplies <strong>and</strong> services - general 1,765 1,469<br />
Establishment 3,054 2,399<br />
Research <strong>and</strong> development (non salary cost) 139 149<br />
Transport 1,780 1,294<br />
Premises 28,647 19,897<br />
Increase in bad debt provision 52 239<br />
Depreciation on property, plant <strong>and</strong> equipment 5,588 5,251<br />
Amortisation of Intangible Assets 423 5<strong>12</strong><br />
Impairments of Property, Plant <strong>and</strong> Equipment 916 5,172<br />
Audit fees 79 53<br />
NHSLA insurance premium 4,683 4,236<br />
Loss on Disposal of Plant & Equipment 2 65<br />
Other 2,131 2,395<br />
Total 235,066 187,793<br />
104 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
4.1.1 Operating lease rentals<br />
<strong>2011</strong>/<strong>12</strong> 2010/11<br />
£000 £000<br />
Hire of plant <strong>and</strong> machinery 370 332<br />
Hire of building 90 103<br />
460 435<br />
In addition to leases whose financial values are shown above, the Trust has a lease for Mary Seacole Nursing Home<br />
from Newlon Housing Trust for a building which have been leased for a number of years at a peppercorn rent.<br />
4.1.2 Operating lease commitments<br />
<strong>2011</strong>/<strong>12</strong> 2010/11<br />
L<strong>and</strong> <strong>and</strong> buildings Other leases Total Total<br />
£000 £000 £000 £000<br />
<strong>Annual</strong> commitments on leases expiring:<br />
Within 1 year 80 325 405 251<br />
Between 1 <strong>and</strong> 5 years 187 484 671 576<br />
Total 267 809 1,076 827<br />
4.3 Salary <strong>and</strong> pension entitlements of senior managers<br />
a) Remuneration<br />
Name <strong>and</strong> title<br />
<strong>2011</strong>/<strong>12</strong> <strong>2011</strong>/<strong>12</strong> <strong>2011</strong>/<strong>12</strong> 2010/11<br />
Directors Other Salary Salary<br />
salary remuneration (b<strong>and</strong>s of (b<strong>and</strong>s of<br />
£000 £000 £5,000) £5,000)<br />
Hallett N - Chief Executive 145-150 - 145-150 145-150<br />
Coakley J - Medical Director 90-95 105-110 200-205 200-205<br />
Farrar J - Director of Finance 130-135 - 130-135 130-135<br />
Panniker A - Director of Environment (until October <strong>2011</strong>) 55-60 - 55-60 95-100<br />
Clements C - Director of Workforce 95-100 - 95-100 95-100<br />
Fletcher T - Chief Operating Officer 110-115 - 110-115 110-115<br />
Sheldon C - Chief Nurse <strong>and</strong> Director of Governance 95-100 - 95-100 75-80<br />
Cassidy M - Chairman 40-45 - 40-45 40-45<br />
Hay S - Non Executive Director 10-15 - 10-15 10-15<br />
Keith M - Non Executive Director 10-15 - 10-15 10-15<br />
Stewart D - Non Executive Director 10-15 - 10-15 10-15<br />
Redmond I - Non Executive Director 10-15 - 10-15 10-15<br />
Griffiths C - Non Executive Director 10-15 - 10-15 10-15<br />
Sorensen E - Non Executive Director (until October <strong>2011</strong>) 5-10 - 5-10 10-15<br />
Sir John Gieve - Non Executive Director (from November <strong>2011</strong>) 5-10 - 5-10 n/a<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 105
ANNUAL ACCOUNTS<br />
b) Pension benefits<br />
Name <strong>and</strong> title Real Real Total Total Cash Cash Real Increase<br />
increase increase accrued accrued equivalent equivalent in cash<br />
in pension in lump sum pension at lump sum at transfer transfer equivalent<br />
at age 60 at age 60 31 March <strong>2011</strong> 31 March <strong>2011</strong> value at value at transfer<br />
31 March <strong>2011</strong> 31 March <strong>2011</strong> value<br />
(b<strong>and</strong>s of (b<strong>and</strong>s of (b<strong>and</strong>s of (b<strong>and</strong>s of £000 £000 £000<br />
£2500) £2500) £5000) £5000)<br />
Hallett N<br />
Chief Executive 0-2.5 2.5-5 65-70 195-200 1,383 1,271 84<br />
Coakley J<br />
Medical Director 0-2.5 2.5-5 75-80 235-240 1,675 1,558 82<br />
Farrar J<br />
Director of Finance 0-2.5 2.5-5 10-15 30-35 142 101 38<br />
Panniker A<br />
Director of Environment<br />
(until October <strong>2011</strong>) 0-2.5 2.5-5 10-15 30-35 194 146 44<br />
Clements C<br />
Director of Workforce 0-2.5 0-2.5 20-25 70-75 462 404 49<br />
Fletcher T<br />
Chief Operating Officer 0-2.5 0-2.5 25-30 75-80 368 290 71<br />
Sheldon C<br />
Chief Nurse <strong>and</strong><br />
Director of Governance 0-2.5 2.5-5 20-25 65-70 289 205 79<br />
There were no payments in the year in respect of “golden hellos”, compensation for loss of office, or benefits in kind for any<br />
of the senior managers. As Non Executive Directors do not receive pensionable remuneration, there are no entries in respect<br />
of pensions for Non Executive Directors.<br />
A Cash Equivalent Transfer Value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by<br />
a member at a particular point in time. The benefits valued are the member’s accrued benefits <strong>and</strong> any contingent spouse’s<br />
pension payable from the scheme. A CETV is a payment made by a pension scheme, or arrangement to secure pension<br />
benefits in another pension scheme or arrangement when the member leaves a scheme <strong>and</strong> chooses to transfer the<br />
benefits accrued in their former scheme. The pension figures shown relate to the benefits that the individual has accrued<br />
as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which the<br />
disclosure applies. The CETV amounts, <strong>and</strong> from 2004/05 the other pension amounts, include the value of any pension<br />
benefits in another scheme or arrangement which the individual has transferred to the NHS Pension Scheme. They also<br />
include any additional pension benefit accrued to the member as a result of their purchasing additional pensionable service<br />
in the scheme at their own cost. CETVs are calculated within the guidelines <strong>and</strong> framework prescribed by the Institute <strong>and</strong><br />
Faculty of Actuaries.<br />
Real Increase in CETV - This reflects the increase in CETV effectively funded by the employer. It takes account of the increase<br />
in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from<br />
another pension scheme or arrangement) <strong>and</strong> uses common market valuation factors for the start <strong>and</strong> end of the period.<br />
Real Increase in CETV for the current year may be different from the prior year. In July 2010 the Chancellor announced that<br />
the uprating (annual increase) of public sector pensions would change from the Retail Price Index (RPI) to the Consumer<br />
Prices Index (CPI). As a result the Government Actuaries Department undertook a review of all transfer factors.<br />
106 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
c) Median salary<br />
Reporting bodies are required to disclose the relationship between the remuneration of the highest-paid director in their<br />
organisation <strong>and</strong> the median remuneration of the organisation’s workforce.<br />
The b<strong>and</strong>ed remuneration of the highest-paid director in <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust in financial<br />
year <strong>2011</strong>/<strong>12</strong> was £202,500 (2010/11 £202,500). This was 6.2 times (2010/11; 6.8 times) the median remuneration of<br />
the workforce, which was £32,830 (2010/11; £29,939). In <strong>2011</strong>/<strong>12</strong>, no employees received remuneration in excess of the<br />
highest-paid director.<br />
Total remuneration includes salary, non-consolidated performance-related pay, benefits-in-kind as well as severance<br />
payments. It does not include employer pension contributions <strong>and</strong> the Cash Equivalent Transfer Value of pensions.<br />
5. Staff costs <strong>and</strong> staff numbers<br />
5.1 Staff costs<br />
<strong>2011</strong>/<strong>12</strong> 2010/11<br />
Permanently Other Total Total<br />
Employed<br />
£000 £000 £000 £000<br />
Salaries <strong>and</strong> wages 118,772 - 118,772 88,965<br />
Social Security costs 10,793 - 10,793 8,351<br />
Employer contributions to NHS Pensions Agency 13,474 - 13,474 9,740<br />
Agency/contract staff - 15,652 15,652 15,317<br />
143,039 15,652 158,691 <strong>12</strong>2,373<br />
5.2 Average number of persons employed<br />
<strong>2011</strong>/<strong>12</strong> 2010/11<br />
Permanently Other Total Total<br />
Employed<br />
Number Number Number Number<br />
Medical <strong>and</strong> dental 394 - 394 363<br />
Healthcare assistants <strong>and</strong> other support staff 249 - 249 155<br />
Nursing, midwifery <strong>and</strong> health visiting staff 1,089 - 1,089 803<br />
Nursing, midwifery <strong>and</strong> health visiting learners 29 - 29 6<br />
Scientific, therapeutic <strong>and</strong> technical staff 598 - 598 260<br />
Administration <strong>and</strong> estates 664 - 664 574<br />
Bank <strong>and</strong> agency staff - 324 324 321<br />
Other 7 - 7 91<br />
Total 3,030 324 3,354 2,573<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 107
ANNUAL ACCOUNTS<br />
5.3 Employee benefits<br />
There are no individual employee benefit costs for <strong>2011</strong>/<strong>12</strong> (2010/11 Nil).<br />
5.4 Retirements due to ill-health<br />
<strong>2011</strong>/<strong>12</strong> <strong>2011</strong>/<strong>12</strong> 2010/11 2010/11<br />
Number £000 Number £000<br />
Early retirements agreed on the grounds of ill-health 1 6 1 21<br />
5.5 Staff exit packages<br />
Number of Number of Total number of<br />
compulsory other departures exit packages<br />
redundancies agreed by cost b<strong>and</strong><br />
9. Intangible fixed assets<br />
All Intangible fixed assets relate to software licenses.<br />
9.1 <strong>2011</strong>/<strong>12</strong><br />
£000<br />
Gross cost at 1 April <strong>2011</strong> 4,162<br />
Additions - purchased 323<br />
Gross cost at 31 March 20<strong>12</strong> 4,485<br />
Amortisation at 1 April <strong>2011</strong> 3,420<br />
Provided during the year 423<br />
Amortisation at 31 March 20<strong>12</strong> 3,843<br />
Net book value<br />
- Purchased at 1 April <strong>2011</strong> 742<br />
- Purchased at 31 March 20<strong>12</strong> 642<br />
9.2 2010/11<br />
Gross cost at 1 April 2010 4,028<br />
Additions - purchased 134<br />
Gross cost at 31 March <strong>2011</strong> 4,162<br />
Amortisation at 1 April 2010 2,908<br />
Provided during the year 5<strong>12</strong><br />
Amortisation at 31 March <strong>2011</strong> 3,420<br />
Net book value<br />
- Purchased at 1 April 2010 1,<strong>12</strong>0<br />
- Purchased at 31 March <strong>2011</strong> 742<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 109
ANNUAL ACCOUNTS<br />
10. Property, plant <strong>and</strong> equipment<br />
10.1 As at 31 March 20<strong>12</strong><br />
L<strong>and</strong><br />
£000<br />
Buildings<br />
excluding<br />
dwellings<br />
£000<br />
Assets<br />
under<br />
construction<br />
£000<br />
Plant <strong>and</strong><br />
machinery<br />
£000<br />
Transport<br />
equipment<br />
£000<br />
Information<br />
technology<br />
£000<br />
Furniture<br />
& fittings<br />
£000<br />
Cost or valuation at 1 April <strong>2011</strong> 26,142 88,285 2,217 20,351 75 7,753 1,251 146,074<br />
Additions - purchased - 2,293 813 1,434 - 487 28 5,055<br />
Additions - donated - - - 1,152 - - - 1,152<br />
Other revaluations - 57 - - - - - 57<br />
Impairments - loss - (3,170) - - - - - (3,170)<br />
Reclassifications - 995 (1,546) 406 - 107 38 -<br />
Disposals - - - (1,787) - (26) - (1,813)<br />
Cost or valuation at 31 March 20<strong>12</strong> 26,142 88,460 1,484 21,556 75 8,321 1,317 147,355<br />
Total<br />
£000<br />
Depreciation at 1 April <strong>2011</strong> - 8,547 - 13,575 75 5,213 1,047 28,457<br />
Provided during the year - 2,751 - 1,869 - 863 105 5,588<br />
Disposals - - - (1,787) - (24) - (1,811)<br />
Depreciation at 31 March 20<strong>12</strong> - 11,298 - 13,657 75 6,052 1,152 32,234<br />
Net book value<br />
- Purchased at 1 April <strong>2011</strong> 26,142 77,966 2,217 3,754 - 2,540 176 1<strong>12</strong>,795<br />
- Donated at 1 April <strong>2011</strong> - 1,772 - 3,022 - - 28 4,822<br />
Total at 1 April <strong>2011</strong> 26,142 79,738 2,217 6,776 - 2,540 204 117,617<br />
Net book value<br />
- Purchased at 31 March 20<strong>12</strong> 26,142 75,435 1,484 4,372 - 2,269 141 109,843<br />
- Donated at 31 March 20<strong>12</strong> - 1,727 - 3,527 - - 24 5,278<br />
Total at 31 March 20<strong>12</strong> 26,142 77,162 1,484 7,899 - 2,269 165 115,<strong>12</strong>1<br />
Analysis of property, plant, <strong>and</strong> equipment <strong>2011</strong>/<strong>12</strong>:<br />
L<strong>and</strong><br />
£000<br />
Buildings<br />
excluding<br />
dwellings<br />
£000<br />
Assets<br />
under<br />
construction<br />
£000<br />
Plant <strong>and</strong><br />
machinery<br />
£000<br />
Transport<br />
equipment<br />
£000<br />
Information<br />
technology<br />
£000<br />
Furniture<br />
& fittings<br />
£000<br />
Net book value<br />
- Protected assets at 31 March 20<strong>12</strong> 26,142 77,162 - - - - - 103,304<br />
- Unprotected assets at<br />
31 March 20<strong>12</strong><br />
- - 1,484 7,899 - 2,269 165 11,817<br />
Total at 31 March 20<strong>12</strong> 26,142 77,162 1,484 7,899 - 2,269 165 115,<strong>12</strong>1<br />
Total<br />
£000<br />
110 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
10.2 As at 31 March <strong>2011</strong> (Restated)<br />
L<strong>and</strong><br />
£000<br />
Buildings<br />
excluding<br />
dwellings<br />
£000<br />
Assets<br />
under<br />
construction<br />
£000<br />
Plant <strong>and</strong><br />
machinery<br />
£000<br />
Transport<br />
equipment<br />
£000<br />
Information<br />
technology<br />
£000<br />
Furniture<br />
& fittings<br />
£000<br />
Cost or valuation at 1 April 2010 26,000 78,368 10,545 20,019 75 7,<strong>12</strong>2 1,224 143,353<br />
Additions - purchased - 4,204 1,453 776 - 456 20 6,909<br />
Additions - donated - 88 - 2,229 - - 7 2,324<br />
Other revaluations 142 1,755 - - - - - 1,897<br />
Impairments - loss - (5,662) - - - (29) - (5,691)<br />
Reclassifications - 9,532 (9,781) 45 - 204 - -<br />
Disposals - - - (2,718) - - - (2,718)<br />
Cost or valuation at 31 March <strong>2011</strong> 26,142 88,285 2,217 20,351 75 7,753 1,251 146,074<br />
Total<br />
£000<br />
Depreciation at 1 April 2010 - 5,954 - 14,502 75 4,388 940 25,859<br />
Provided during the year - 2,593 - 1,726 - 825 107 5,251<br />
Disposals - - - (2,653) - - (2,653)<br />
Depreciation at 31 March <strong>2011</strong> - 8,547 - 13,575 75 5,213 1,047 28,457<br />
Net book value<br />
- Purchased at 1 April 2010 26,000 70,607 10,545 4,382 - 2,734 260 114,528<br />
- Donated at 1 April 2010 - 1,807 - 1,135 - - 24 2,966<br />
Total at 1 April 2010 26,000 72,414 10,545 5,517 - 2,734 284 117,494<br />
Net book value<br />
- Purchased at 31 March <strong>2011</strong> 26,142 77,966 2,217 3,754 - 2,540 176 1<strong>12</strong>,795<br />
- Donated at 31 March <strong>2011</strong> - 1,772 - 3,022 - - 28 4,822<br />
Total at 31 March <strong>2011</strong> 26,142 79,738 2,217 6,776 - 2,540 204 117,617<br />
Analysis of property, plant, <strong>and</strong> equipment<br />
L<strong>and</strong><br />
£000<br />
Buildings<br />
excluding<br />
dwellings<br />
£000<br />
Assets<br />
under<br />
construction<br />
£000<br />
Plant <strong>and</strong><br />
machinery<br />
£000<br />
Transport<br />
equipment<br />
£000<br />
Information<br />
technology<br />
£000<br />
Furniture<br />
& fittings<br />
£000<br />
Net book value<br />
- Protected assets at 31 March <strong>2011</strong> 26,142 79,738 - - - - - 105,880<br />
- Unprotected assets at 31 March <strong>2011</strong> - - 2,217 6,776 - 2,540 204 11,737<br />
Total at 31 March <strong>2011</strong> 26,142 79,738 2,217 6,776 - 2,540 204 117,617<br />
Total<br />
£000<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 111
ANNUAL ACCOUNTS<br />
10.3 Assets held at market value<br />
At 31 March 20<strong>12</strong> the Trust held l<strong>and</strong> assets at market<br />
value for existing use of £26,142,000 (31 March <strong>2011</strong>,<br />
£26,142,000).<br />
10.4 Valuation of l<strong>and</strong> & buildings<br />
The buildings have been valued as at the 31 March 20<strong>12</strong><br />
using a Modern Equivalent Asset basis of valuation, as<br />
discounted for wear <strong>and</strong> tear.<br />
L<strong>and</strong> has been revalued at the 31 March 20<strong>12</strong> at market<br />
value for existing use.<br />
Both valuations were carried out by the District Valuer<br />
(DVS Property) whose address is the Westminster Valuation<br />
Office, Wingate House, London W1D 5BU.<br />
Buildings have estaimated useful economic lives ranging<br />
from 7 years to 60 years.<br />
10.5 Assets held under finance leases <strong>and</strong> hire<br />
purchase contracts at 31 March 20<strong>12</strong><br />
The Trust did not hold any finance leases or hire purchase<br />
contracts during <strong>2011</strong>/<strong>12</strong>.<br />
10.6 Donated assets<br />
Donated assets include £1,152,189 (£2,095,000 in<br />
2010/11) of equipment assets donated by GE Healthcare.<br />
We have restated the prior year figure to exclude £970,000<br />
of donated assets that related to assets donated in<br />
<strong>2011</strong>/<strong>12</strong>.<br />
11. Fixed asset investments<br />
There were no fixed asset investments held at 31 March<br />
20<strong>12</strong> (31 March <strong>2011</strong> - Nil).<br />
<strong>12</strong>. Inventories<br />
<strong>12</strong>.1 Inventories<br />
<strong>2011</strong>/<strong>12</strong> 2010/11<br />
£000 £000<br />
Drugs 810 819<br />
Consumables 181 <strong>12</strong>4<br />
Energy 130 82<br />
13. Trade <strong>and</strong> other receivables<br />
13.1 Amounts falling due within one year:<br />
31 March 20<strong>12</strong><br />
£000<br />
31 March <strong>2011</strong><br />
£000<br />
NHS receivables 5,323 4,398<br />
Provision for impaired<br />
(652) (619)<br />
receivables<br />
Prepayments 894 538<br />
Accrued income 3,562 2,966<br />
PDC receivable <strong>12</strong>1 209<br />
Other receivables 4,208 2,973<br />
Total 13,456 10,465<br />
13.2 Analysis of the provision for impaired receivables<br />
31 March 20<strong>12</strong><br />
£000<br />
31 March <strong>2011</strong><br />
£000<br />
At 1 April 619 394<br />
Arising during the year 52 239<br />
Utilised during the year (19) (14)<br />
At 31 March 652 619<br />
By age: 31 March 20<strong>12</strong><br />
£000<br />
31 March <strong>2011</strong><br />
£000<br />
Up to three months old 27 63<br />
In three to six months old 20 11<br />
Over six months old 605 545<br />
Total 652 619<br />
14. Other Financial Assets<br />
31 March 20<strong>12</strong><br />
£000<br />
31 March <strong>2011</strong><br />
£000<br />
Cost or valuation at 1 April 25 23<br />
(Disposals) / Additions (25) 2<br />
Cost or valuation at 31 March - 25<br />
Total at net realisable value 1,<strong>12</strong>1 1,025<br />
<strong>12</strong>.2 Inventories recognised in expenses<br />
31 March<strong>12</strong> 31 March11<br />
£000 £000<br />
Total Inventories recognised as an<br />
expense in the period 13,331 <strong>12</strong>,893<br />
1<strong>12</strong> <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
15. Cash <strong>and</strong> cash equivalents<br />
31 March 20<strong>12</strong><br />
£000<br />
31 March <strong>2011</strong><br />
£000<br />
Balance as at 1 April 17,088 16,535<br />
Net change in year 13,468 553<br />
Balance at 31 March 30,556 17,088<br />
Of which:<br />
Commercial banks <strong>and</strong> cash in h<strong>and</strong> 73 72<br />
Cash with the Government Banking Service 30,458 17,016<br />
Other current investments 25 -<br />
Total cash <strong>and</strong> cash equivalents in the<br />
Statement of Cash Flows<br />
30,556 17,088<br />
16. Liabilities<br />
16.1 (i) Current liabilities: Amounts falling due within one year<br />
31 March 20<strong>12</strong><br />
£000<br />
Restated<br />
31 March <strong>2011</strong><br />
£000<br />
NHS payables 5,201 1,531<br />
Trade payables - Capital 481 1,281<br />
Loans 257 257<br />
Other payables 7,638 5,205<br />
Payments received on account 164 1,044<br />
Tax payable 5,204 3,996<br />
Accruals 4,701 3,465<br />
Deferred income 5,403 3,104<br />
Provisions 1,685 638<br />
Total amounts falling due within one year 30,734 20,521<br />
16.1 (ii) Non current liabilities: Payables due after more than one year<br />
31 March 20<strong>12</strong><br />
£000<br />
31 March <strong>2011</strong><br />
£000<br />
Provisions 641 644<br />
Loans 3,794 4,051<br />
4,435 4,695<br />
16.1 (iii) Total payables 35,169 25,216<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 113
ANNUAL ACCOUNTS<br />
16.2 Loans - payment of principal falling due:<br />
31 March 20<strong>12</strong><br />
£000<br />
31 March <strong>2011</strong><br />
£000<br />
Within one year 257 257<br />
Between one <strong>and</strong> two years 257 257<br />
Between two <strong>and</strong> five years 664 717<br />
After five years 2,873 3,077<br />
Total 4,051 4,308<br />
Of which:<br />
Wholly repayable within 5 years 157 1,231<br />
Wholly repayable after 5 years, not by instalments - -<br />
Wholly or partially repayable after 5 years by instalments 3,894 3,077<br />
Total 4,051 4,308<br />
16.3 Prudential borrowing limit:<br />
Prudential Borrowing Limit set by Monitor 45,500 34,900<br />
Working Capital Facility Limit 8,500 8,500<br />
Total Prudential Borrowing Limit 54,000 43,400<br />
The Trust had a Prudential Borrowing Limit (PBL) of £54m in <strong>2011</strong>/<strong>12</strong> (£43.4m in 2010/11). The Trust did not draw<br />
down on its working capital facility druing the year ended 31 March 20<strong>12</strong> or during the year ended 31 March <strong>2011</strong>.<br />
The Trust is required to comply <strong>and</strong> remain within its PBL.This is made up of two elements :<br />
i) The maximum cumulative amount of borrowing. This is set by reference to the four ratio tests set out in Monitor’s<br />
Prudential Borrowing Code. The performance against these financial ratios over the past two years is as follows:<br />
Financial ratio<br />
Actual ratios<br />
<strong>2011</strong>/<strong>12</strong><br />
Approved<br />
PBL<br />
ratios<br />
<strong>2011</strong>/<strong>12</strong><br />
Actual ratios<br />
2010/11<br />
Approved PBL<br />
ratios 2010/11<br />
Minimum dividend cover 3.65 1.00 3.14 1.00<br />
Minimum interest cover 68.33 3.00 49.84 3.00<br />
Minimum debt service cover 30.40 2.00 22.99 2.00<br />
Maximum debt service to revenue 0.19% 2.50% 0.25% 2.50%<br />
ii) The amount of any working capital facility approved by Monitor.<br />
The Trust has an agreed working capital facility of £8.5m (£8.5m in 2010/11). The Trust did not draw down on its working<br />
capital facility during the year ended 31 March 20<strong>12</strong> or the year ended 31 March <strong>2011</strong>.<br />
Further information on the Prudential Borrowing Code <strong>and</strong> Compliance Framework can be found on Monitor’s website.<br />
114 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
17. Provisions for liabilities <strong>and</strong> charges<br />
Pensions<br />
relating<br />
to former<br />
Directors<br />
Pensions<br />
relating to<br />
former Staff<br />
Clinical<br />
negligence Redundancy Other<br />
31 March<br />
<strong>2011</strong><br />
Total<br />
31 March<br />
<strong>2011</strong><br />
Total<br />
£000 £000 £000 £000 £000 £000 £000<br />
At 1 April 82 607 68 - 525 1,282 898<br />
Arising during the year - - - 132 1,452 1,584 503<br />
Change in discount rate 3 23 - - - 26 -<br />
Utilised during the year (6) (41) (<strong>12</strong>) - (526) (585) (39)<br />
Reversed unused - - - - - - (102)<br />
Unwinding of discount 2 17 - - - 19 22<br />
At 31 March 81 606 56 132 1,451 2,326 1,282<br />
Within one year 6 41 56 132 1,451 1,686 638<br />
Between one <strong>and</strong> five years 22 151 - - - 173 168<br />
After five years 53 414 - - - 467 476<br />
Total 81 606 56 132 1,451 2,326 1,282<br />
Pension related provisions as at 31 March 20<strong>12</strong> included £687,000 relating to matters h<strong>and</strong>led by the NHS Pensions Agency<br />
(NHSPA). Other provisions include £119,000 relating to historic issues with our employee records system, <strong>and</strong> £<strong>12</strong>7,000 of<br />
carbon tax liabilities.<br />
18. Clinical negligence liability<br />
The amount provided by the NHSLA in respect of clinical negligence liabilities of the trust as at 31 March 20<strong>12</strong> is<br />
£29,089,314 (2010/11; £27,651,000).<br />
19. Movement in Public Dividend Capital<br />
<strong>2011</strong>/<strong>12</strong><br />
£000<br />
2010/11<br />
£000<br />
Public Dividend Capital as at 1 April 83,175 83,175<br />
New PDC received 925 -<br />
Public Dividend Capital as at 31 March 84,100 83,175<br />
The dividend paid for the year was £3.3m (2010/11 £3.5m). Further details on how the dividend was calculated on the basis<br />
set out in note 1.15.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 115
ANNUAL ACCOUNTS<br />
20. Notes to the cash flow statement<br />
20.1 Reconciliation of operating surplus to net cash inflow from operating activities:<br />
<strong>2011</strong>/<strong>12</strong><br />
£000<br />
Restated<br />
2010/11<br />
£000<br />
Total operating surplus 8,611 3,078<br />
Depreciation <strong>and</strong> amortisation 6,011 5,763<br />
Impairment 916 5,172<br />
Donated assets capitalised (1,152) (2,314)<br />
Increase in inventories (96) (138)<br />
(Increase)/decrease in receivables (4,690) 493<br />
Increase in payables 6,866 2,418<br />
Increase in provisions 1,043 384<br />
Transforming community services adjustment - (274)<br />
Other movements 3,999 (3,196)<br />
Net cash inflow from operating activities 21,507 11,386<br />
20.2 Reconciliation of net cash flow to movement in net debt<br />
<strong>2011</strong>/<strong>12</strong><br />
£000<br />
2010/11<br />
£000<br />
Increase in cash in the period 13,443 553<br />
Cash outflow from increase in liquid resources 257 259<br />
Change in net debt resulting from cash flows 13,700 8<strong>12</strong><br />
Net debt at 1 April <strong>12</strong>,806 11,994<br />
Net debt at 31 March 26,506 <strong>12</strong>,806<br />
20.3 Analysis of changes in net debt<br />
At 1 April <strong>2011</strong> Cash changes Non-cash At 31 March At 31 March<br />
in year changes in year 20<strong>12</strong> <strong>2011</strong><br />
£000 £000 £000 £000 £000<br />
GBS cash at bank 17,016 13,442 - 30,458 17,016<br />
Commercial cash at bank <strong>and</strong> in h<strong>and</strong> 72 1 - 73 72<br />
Debt due after one year (4,051) 257 257 (3,537) (4,050)<br />
Debt due within one year (257) 257 (257) (257) (257)<br />
Current asset investments - 25 - 25 -<br />
Other financial assets 25 (25) - - 25<br />
Total <strong>12</strong>,805 13,957 - 26,762 <strong>12</strong>,806<br />
21. Contractual capital commitments<br />
There were £1.3m of commitments under capital expenditure contracts as at 31 March 20<strong>12</strong> (31 March <strong>2011</strong>; £Nil).<br />
22. Contingent liabilities <strong>2011</strong>/<strong>12</strong> 2010/11<br />
£000 £000<br />
Liabilities to Third Parties Scheme (LTPS) member’s contribution (14) (58)<br />
Further details of the LTPS are in note 1.13(ii) to these <strong>accounts</strong><br />
116 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
23. Related party transactions<br />
Details of related party transactions with individuals are as follows:<br />
Payments to Income From<br />
Name <strong>and</strong> role Related party details related party related party<br />
£000 £000<br />
Andrew Panniker,<br />
Spouse Chief Executive,<br />
Director of Environment North Middlesex <strong>Hospital</strong> NHS Trust - 7<br />
Charlie Sheldon, Honorary Senior Lecturer, 26 50<br />
Chief Nurse<br />
City <strong>University</strong><br />
Charlie Sheldon, Honorary Visiting Reader, 2 -<br />
Chief Nurse<br />
London South Bank <strong>University</strong><br />
Government Departments <strong>and</strong> their agencies are considered by HM Treasury as being related parties. During the year<br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust has had a significant number of material transactions with Government<br />
Departments <strong>and</strong> their agencies. These entities are listed below:<br />
Name Relationship Income Expenditure Receivables Payables<br />
£000 £000 £000 £000<br />
East London NHS Foundation Trust Foundation Trust 4,028 242 88 90<br />
Barts <strong>and</strong> London NHS Trust Trust 638 4,937 320 926<br />
NHS Litigation Authority Insurer - 4,685 - 29<br />
NHS Pensions Agency Commissioner - 21,044 - 1,656<br />
NHS City <strong>and</strong> Hackney Commissioner 132,167 4,354 4,190 4,853<br />
Department of Health Commissioner 541 358 13 40<br />
NHS Enfield Commissioner 1,958 - 52 -<br />
NHS Haringey Commissioner 4,685 - 283 -<br />
NHS Islington Commissioner 4,177 - - 7<br />
London Borough of Hackney Commissioner 3,657 1,605 795 25<br />
NHS London SHA Commissioner 11,366 - 54 -<br />
NHS Newham Commissioner 3,701 - 762 -<br />
NHS Redbridge Commissioner 3,143 - 109 -<br />
South East Essex PCT Commissioner 2,493 - - 42<br />
NHS Tower Hamlets Commissioner 30,971 - 103 2<br />
NHS Waltham Forest Commissioner 7,152 - 447 -<br />
NHS Croydon Commissioner 16,636 - 57 -<br />
The Trust has also received revenue <strong>and</strong> capital payments from the <strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust<br />
Charitable Fund. The Charity is registered with the Charity Commission (Charity Number 1061659) <strong>and</strong> has its own Trustees<br />
drawn from the NHS Trust Board. It produces a set of annual <strong>accounts</strong> <strong>and</strong> an annual <strong>report</strong> (separate to that of the NHS<br />
Foundation Trust) <strong>and</strong> these documents are available on request from the Trust.<br />
24. Private Finance Initiative transactions<br />
The Foundation Trust has no PFI schemes.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 117
ANNUAL ACCOUNTS<br />
25. Financial instruments<br />
IAS 32 (Financial Instruments: Disclosure <strong>and</strong> Presentation), IAS 39 (Financial Instrument Recognition <strong>and</strong> Measurement) <strong>and</strong><br />
IFRS 7 (Financial Instruments: Disclosures) require disclosure of the role that financial instruments have played during the<br />
period in creating or changing the risks an entity faces in undertaking its activities.<br />
The Trust does not have any complex financial instruments <strong>and</strong> does not hold or issue financial instruments for speculative<br />
trading purposes. In light of the continuing service provider relationship the Trust has with primary care trusts <strong>and</strong> the way<br />
those primary care trusts are financed, the Trust is not exposed to the degree of financial risk faced by non NHS business<br />
entities.<br />
The Trust has limited powers to borrow or invest surplus funds <strong>and</strong> financial assets <strong>and</strong> liabilities are generated by day-to-day<br />
operational activities rather than being held to change the risks facing the Trust in undertaking its activities.<br />
The Finance <strong>and</strong> Perfomance Committee manages the Trust’s funding requirements <strong>and</strong> financial risks in line with the Board<br />
approved treasury policies <strong>and</strong> procedures <strong>and</strong> their delegated authorities.<br />
The Trust’s financial instruments comprise loans, provisions, cash at bank <strong>and</strong> in h<strong>and</strong> <strong>and</strong> various items, such as trade<br />
debtors <strong>and</strong> trade creditors, that arise directly from its operations. The main purpose of these financial instruments is to raise<br />
finance for the Trust’s operations.<br />
26.1 Financial assets<br />
Fixed rate Floating rate Non-interest bearing Total<br />
£000 £000 £000 £000<br />
At 31 March 20<strong>12</strong> 25 30,531 14,139 44,695<br />
At 31 March <strong>2011</strong> (Prior year) 25 17,088 9,653 26,766<br />
Financial assets consist of cash <strong>and</strong> cash equivalents <strong>and</strong> trade <strong>and</strong> other receivables less prepayments.<br />
26.2 Financial liabilities Fixed rate Non-interest bearing Total<br />
£000 £000 £000<br />
At 31 March 20<strong>12</strong> 3,275 21,302 24,577<br />
At 31 March <strong>2011</strong> (Prior year) 3,500 13,716 17,216<br />
Financial liabilities consist of current <strong>and</strong> non-current liabilities less deferred income, tax <strong>and</strong> provisions.<br />
26.3 Financial assets <strong>and</strong> liabilities<br />
At 31 March 20<strong>12</strong><br />
£000<br />
At 31 March <strong>2011</strong><br />
£000<br />
26.3 (i) Financial assets (book <strong>and</strong> fair value)<br />
Cash 30,531 17,088<br />
Receivables within 1 year: <strong>12</strong>,<strong>12</strong>8 9,362<br />
Receivables after 1 year: - Agreements with commissioners to cover provisions 311 291<br />
Other current investments 25 25<br />
Total 42,995 26,766<br />
26.3 (ii) Financial liabilities (book <strong>and</strong> fair value)<br />
Payables within 1 year (19,885) (<strong>12</strong>,265)<br />
Provisions under contract over 1 year (641) (644)<br />
Loans (4,051) (4,307)<br />
Total (24,577) (17,216)<br />
Notes<br />
a) Fair value is not significantly different from book value since, in the calculation of book value, the expected cash flows<br />
have been discounted by the HM Treasury’s discount rate of 2.2% in real terms (2010/11; 2.2%)<br />
118 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
27. Third party assets<br />
The Trust held £1,288 of patients’ monies at 31 March 20<strong>12</strong> (31 March <strong>2011</strong>; £1,353). This amount has been excluded from<br />
the cash at bank <strong>and</strong> in h<strong>and</strong> figure <strong>report</strong>ed in the Accounts.<br />
28. Intra-Government <strong>and</strong> other balances<br />
Receivables: amounts<br />
falling due within one year<br />
Payables: amounts<br />
falling due within one year<br />
At March 20<strong>12</strong> At March 20<strong>12</strong><br />
£000 £000<br />
28.1 Receivable <strong>and</strong> payable balances<br />
English NHS Foundation Trusts 174 217<br />
English NHS Trusts 367 1,233<br />
Department of Health 13 40<br />
English Strategic Health Authorities 54 1<br />
English Primary Care Trusts 7,922 4,909<br />
Other NHS WGA bodies 33 423<br />
Other WGA bodies 3 2<br />
Total 8,566 6,825<br />
28.2 Income <strong>and</strong> expenditure values for the year<br />
Income<br />
Year Ended March 20<strong>12</strong><br />
£000<br />
Expenditure<br />
Year Ended March 20<strong>12</strong><br />
£000<br />
English NHS Foundation Trusts 4,113 790<br />
English NHS Trusts 1,058 6,545<br />
Department of Health 541 358<br />
English Strategic Health Authorities 11,366 2<br />
English Primary Care Trusts 216,518 4,346<br />
NHS WGA bodies 11 5,594<br />
Other WGA bodies 39 35<br />
Total 233,646 17,670<br />
29. Losses <strong>and</strong> special payments<br />
Total<br />
Number<br />
£000<br />
Losses 19 34<br />
Special payments 2 9<br />
Total 21 43<br />
Losses have been calculated on an accruals basis but exclude provisions for future losses.<br />
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> 119
ANNUAL ACCOUNTS<br />
<strong>12</strong>0 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
<strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong> <strong>12</strong>1
ANNUAL ACCOUNTS<br />
<strong>12</strong>2 <strong>Annual</strong> <strong>report</strong> <strong>2011</strong>/<strong>12</strong>
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong><br />
<strong>Homerton</strong> Row London E9 6SR<br />
Tel: 020 8510 5555<br />
www.homerton.nhs.uk
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust <strong>Annual</strong> Report <strong>and</strong> Accounts <strong>2011</strong>/<strong>12</strong><br />
<strong>Homerton</strong> <strong>University</strong> <strong>Hospital</strong> NHS Foundation Trust <strong>Annual</strong> Report <strong>and</strong> Accounts <strong>2011</strong>/<strong>12</strong>