Sleep Diary Template
Sleep Diary Template
Sleep Diary Template

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
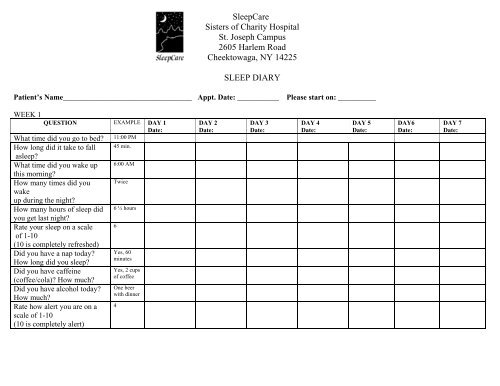
<strong>Sleep</strong>Care<br />
Sisters of Charity Hospital<br />
St. Joseph Campus<br />
2605 Harlem Road<br />
Cheektowaga, NY 14225<br />
SLEEP DIARY<br />
Patient’s Name__________________________________ Appt. Date: ___________ Please start on: __________<br />
WEEK 1<br />
QUESTION EXAMPLE DAY 1<br />
Date:<br />
What time did you go to bed 11:00 PM<br />
How long did it take to fall 45 min.<br />
asleep<br />
What time did you wake up 6:00 AM<br />
this morning<br />
How many times did you Twice<br />
wake<br />
up during the night<br />
How many hours of sleep did 6 ½ hours<br />
you get last night<br />
Rate your sleep on a scale 6<br />
of 1-10<br />
(10 is completely refreshed)<br />
Did you have a nap today<br />
How long did you sleep<br />
Did you have caffeine<br />
(coffee/cola) How much<br />
Did you have alcohol today<br />
How much<br />
Rate how alert you are on a<br />
scale of 1-10<br />
(10 is completely alert)<br />
Yes, 60<br />
minutes<br />
Yes, 2 cups<br />
of coffee<br />
One beer<br />
with dinner<br />
4<br />
DAY 2<br />
Date:<br />
DAY 3<br />
Date:<br />
DAY 4<br />
Date:<br />
DAY 5<br />
Date:<br />
DAY6<br />
Date:<br />
DAY 7<br />
Date:
<strong>Sleep</strong>Care<br />
St. Joseph Campus<br />
SLEEP DIARY<br />
Patient’s Name__________________________________<br />
WEEK 2<br />
QUESTION EXAMPLE DAY 1<br />
Date:<br />
What time did you go to bed 11:00 PM<br />
How long did it take to fall 45 min.<br />
asleep<br />
What time did you wake up 6:00 AM<br />
this morning<br />
How many times did you Twice<br />
wake<br />
up during the night<br />
How many hours of sleep did 6 ½ hours<br />
you get last night<br />
Rate your sleep on a scale 6<br />
of 1-10<br />
(10 is completely refreshed)<br />
Did you have a nap today<br />
How long did you sleep<br />
Did you have caffeine<br />
(coffee/cola) How much<br />
Did you have alcohol today<br />
How much<br />
Rate how alert you are on a<br />
scale of 1-10<br />
(10 is completely alert)<br />
Yes, 60<br />
minutes<br />
Yes, 2 cups<br />
of coffee<br />
One beer<br />
with dinner<br />
4<br />
DAY 2<br />
Date:<br />
DAY 3<br />
Date:<br />
DAY 4<br />
Date:<br />
DAY 5<br />
Date:<br />
DAY6<br />
Date:<br />
DAY 7<br />
Date: