MMR/Meningitis Form (PDF)
MMR/Meningitis Form (PDF) MMR/Meningitis Form (PDF)
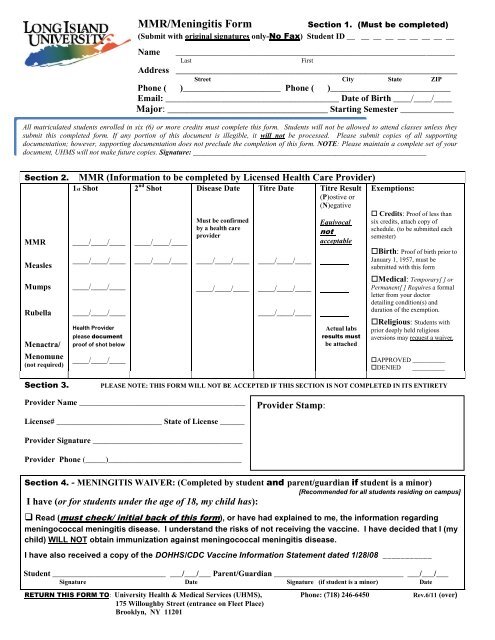
MMR/Meningitis Form Section 1. (Must be completed) (Submit with original signatures only-No Fax) Student ID __ __ __ __ __ __ __ __ __ Name _____________________________________________________________________ Last First Address __________________________________________________________ Street City State ZIP Phone ( )______________________ Phone ( )___________________________ Email: _______________________________________ Date of Birth ____/____/____ Major: _________________________________ Starting Semester ____________ All matriculated students enrolled in six (6) or more credits must complete this form. Students will not be allowed to attend classes unless they submit this completed form. If any portion of this document is illegible, it will not be processed. Please submit copies of all supporting documentation; however, supporting documentation does not preclude the completion of this form. NOTE: Please maintain a complete set of your document, UHMS will not make future copies. Signature: ________________________________________________________________ Section 2. MMR (Information to be completed by Licensed Health Care Provider) 1st Shot 2 nd Shot Disease Date Titre Date Titre Result (P)ostive or (N)egative MMR ____/____/____ ____/____/____ Measles Must be confirmed by a health care provider ____/____/____ ____/____/____ ____/____/____ ____/____/____ Mumps ____/____/____ ____/____/____ ____/____/____ Rubella ____/____/____ ____/____/____ Menactra/ Menomune (not required) Health Provider please document proof of shot below ____/____/____ Equivocal not acceptable Actual labs results must be attached Exemptions: Credits: Proof of less than six credits, attach copy of schedule. (to be submitted each semester) Birth: Proof of birth prior to January 1, 1957, must be submitted with this form Medical: Temporary[ ] or Permanent[ ] Requires a formal letter from your doctor detailing condition(s) and duration of the exemption. Religious: Students with prior deeply held religious aversions may request a waiver. APPROVED __________ DENIED __________ Section 3. PLEASE NOTE: THIS FORM WILL NOT BE ACCEPTED IF THIS SECTION IS NOT COMPLETED IN ITS ENTIRETY Provider Name _________________________________________ License# __________________________ State of License ______ Provider Stamp: Provider Signature _____________________________________ Provider Phone (_____)_________________________________ Section 4. - MENINGITIS WAIVER: (Completed by student and parent/guardian if student is a minor) [Recommended for all students residing on campus] I have (or for students under the age of 18, my child has): Read (must check/ initial back of this form), or have had explained to me, the information regarding meningococcal meningitis disease. I understand the risks of not receiving the vaccine. I have decided that I (my child) WILL NOT obtain immunization against meningococcal meningitis disease. I have also received a copy of the DOHHS/CDC Vaccine Information Statement dated 1/28/08 ___________ Student ____________________________ ___/___/___ Parent/Guardian ________________________________ ___/___/___ Signature Date Signature (if student is a minor) Date RETURN THIS FORM TO: University Health & Medical Services (UHMS), Phone: (718) 246-6450 Rev.6/11 (over) 175 Willoughby Street (entrance on Fleet Place) Brooklyn, NY 11201
<strong>MMR</strong>/<strong>Meningitis</strong> <strong>Form</strong><br />
Section 1. (Must be completed)<br />
(Submit with original signatures only-No Fax) Student ID __ __ __ __ __ __ __ __ __<br />
Name _____________________________________________________________________<br />
Last<br />
First<br />
Address __________________________________________________________<br />
Street City State ZIP<br />
Phone ( )______________________ Phone ( )___________________________<br />
Email: _______________________________________ Date of Birth ____/____/____<br />
Major: _________________________________ Starting Semester ____________<br />
All matriculated students enrolled in six (6) or more credits must complete this form. Students will not be allowed to attend classes unless they<br />
submit this completed form. If any portion of this document is illegible, it will not be processed. Please submit copies of all supporting<br />
documentation; however, supporting documentation does not preclude the completion of this form. NOTE: Please maintain a complete set of your<br />
document, UHMS will not make future copies. Signature: ________________________________________________________________<br />
Section 2. <strong>MMR</strong> (Information to be completed by Licensed Health Care Provider)<br />
1st Shot 2 nd Shot Disease Date Titre Date Titre Result<br />
(P)ostive or<br />
(N)egative<br />
<strong>MMR</strong> ____/____/____ ____/____/____<br />
Measles<br />
Must be confirmed<br />
by a health care<br />
provider<br />
____/____/____ ____/____/____ ____/____/____ ____/____/____<br />
Mumps ____/____/____ ____/____/____ ____/____/____<br />
Rubella ____/____/____ ____/____/____<br />
Menactra/<br />
Menomune<br />
(not required)<br />
Health Provider<br />
please document<br />
proof of shot below<br />
____/____/____<br />
Equivocal<br />
not<br />
acceptable<br />
Actual labs<br />
results must<br />
be attached<br />
Exemptions:<br />
Credits: Proof of less than<br />
six credits, attach copy of<br />
schedule. (to be submitted each<br />
semester)<br />
Birth: Proof of birth prior to<br />
January 1, 1957, must be<br />
submitted with this form<br />
Medical: Temporary[ ] or<br />
Permanent[ ] Requires a formal<br />
letter from your doctor<br />
detailing condition(s) and<br />
duration of the exemption.<br />
Religious: Students with<br />
prior deeply held religious<br />
aversions may request a waiver.<br />
APPROVED __________<br />
DENIED __________<br />
Section 3.<br />
PLEASE NOTE: THIS FORM WILL NOT BE ACCEPTED IF THIS SECTION IS NOT COMPLETED IN ITS ENTIRETY<br />
Provider Name _________________________________________<br />
License# __________________________ State of License ______<br />
Provider Stamp:<br />
Provider Signature _____________________________________<br />
Provider Phone (_____)_________________________________<br />
Section 4. - MENINGITIS WAIVER: (Completed by student and parent/guardian if student is a minor)<br />
[Recommended for all students residing on campus]<br />
I have (or for students under the age of 18, my child has):<br />
Read (must check/ initial back of this form), or have had explained to me, the information regarding<br />
meningococcal meningitis disease. I understand the risks of not receiving the vaccine. I have decided that I (my<br />
child) WILL NOT obtain immunization against meningococcal meningitis disease.<br />
I have also received a copy of the DOHHS/CDC Vaccine Information Statement dated 1/28/08 ___________<br />
Student ____________________________ ___/___/___ Parent/Guardian ________________________________ ___/___/___<br />
Signature Date Signature (if student is a minor) Date<br />
RETURN THIS FORM TO: University Health & Medical Services (UHMS), Phone: (718) 246-6450 Rev.6/11 (over)<br />
175 Willoughby Street (entrance on Fleet Place)<br />
Brooklyn, NY 11201
Section One: This section is to be filled our completely by the student. Your student identification number (SID) is required in order to process your<br />
information; no other defining information will be accepted. The demographic information is used for filing purposes and future communications,<br />
please print neatly. We require a local address, telephone number and an active email address. NOTE: Only three attempts will be made to inform<br />
you of missing information before a hold is placed on your account, which may prevent registration or continued access to classes.<br />
Section Two: <strong>MMR</strong> Requirements<br />
Section Four: MENINGOCOCCAL MENINGITIS Requirements<br />
(To be completed by a Licensed Health Care Provider)<br />
N.Y.S. Public Health Law 2165 requires college students enrolled for six<br />
or more chargeable credits to show proof of immunization against<br />
Measles, Mumps, and Rubella. Students born prior to January 1, 1957<br />
are exempt from this requirement.<br />
On July 22, 2003, Governor Pataki signed New York State Public Health<br />
Law (NYS PHL) §2167 requiring institutions, including colleges and<br />
universities, to distribute information about meningococcal disease and<br />
vaccination to all students meeting the enrollment criteria, whether they<br />
live on or off campus. This law is effective as of August 15, 2003.<br />
<strong>MMR</strong> (Combined Live Measles, Mumps, and Rubella<br />
Immunization). The first dose no more than 4 days prior to the first<br />
birthday. The second dose a minimum of 28 days after the first<br />
dose.<br />
Single Live Measles Immunization. The first dose no more than 4<br />
days prior to the first birthday. The second dose a minimum of 28<br />
days after the first dose. Physician statement of Measles disease<br />
(exact date required) is acceptable.<br />
Single Live Mumps Immunization. Dose no more than 4 days prior<br />
to the first birthday. Physician statement of Mumps disease (exact<br />
date required) is acceptable.<br />
Single Live Rubella (German Measles) Immunization. Dose no<br />
more than 4 days prior to the first birthday. Diagnosis of Rubella<br />
(German Measles) is not acceptable as proof of immunity.<br />
<br />
Serologic evidence of immunity (Titre, copy of actual report must<br />
EXEMPTIONS:<br />
be attached) is acceptable for Measles, Mumps, and Rubella.<br />
EQUIVOCAL TITRES ARE NOT ACCEPTABLE.<br />
If you are requesting an exemption, you must provide the requested<br />
proof and/or complete the required form(s).<br />
automatic.<br />
Section Three: Physician Information<br />
Approval is not<br />
Please note this section, must be filled out in its’ entirety, and is only<br />
accepted with original signatures. All the information in this section is<br />
required. <strong>Form</strong>s missing information from this section will not be<br />
accepted.<br />
<br />
<br />
<br />
<br />
<br />
<br />
Provider Name – Must be clearly printed and/or provided on via their<br />
stamp in the allocated area (stamp that cannot be read will be<br />
returned);<br />
License# - Must be clearly printed and/or provided via the doctor’s<br />
stamp;<br />
State of License – Must be provided and clearly printed in the<br />
allocated area;<br />
Provider Signature – No forms will be accepted without a<br />
doctor’s signature matching the license # provided;<br />
Provider Phone - Must be provided and clearly printed in the<br />
allocated area;<br />
Provider Stamp – This is the doctor’s stamp and not the facility, the<br />
stamp should be clearly placed in the space allocated;<br />
Colleges in New York State are required to maintain a record of the<br />
following for each student:<br />
1 A response to receipt of meningococcal disease and vaccine<br />
information signed by the student or student’s parent or guardian.<br />
This must include information on the availability and cost of<br />
meningococcal meningitis vaccine;<br />
AND EITHER<br />
A record of meningococcal meningitis immunization within the past<br />
10 years; OR<br />
<br />
An acknowledgement of meningococcal disease risks and refusal of<br />
meningococcal meningitis immunization signed by the student or<br />
student’s parent or guardian.<br />
MENINGOCOCCAL DISEASE RISKS:<br />
<strong>Meningitis</strong> is rare. However, when it strikes, its flu-like symptoms<br />
make diagnosis difficult. If not treated early, meningitis can lead to<br />
swelling of the fluid surrounding the brain and spinal column as well as<br />
severe and permanent disabilities, such as hearing loss, brain damage,<br />
seizures, limb amputation, and even death.<br />
Cases of meningitis among teens and young adults 15 to 24 years<br />
of age (the age of most college students) have more than doubled since<br />
1991. The disease strikes about 3,000 Americans each year and claims<br />
about 300 lives. Between 100 and 125 meningitis cases occur on college<br />
campuses and as many as 15 students will die from the disease.<br />
In February 2005, the CDC recommended a new vaccine, known as<br />
Menactra for use to prevent meningococcal disease in people 11-55<br />
years of age.<br />
The previously licensed version of this vaccine,<br />
Menomune is still available for this age group, as well as for children 2-<br />
10 years old and adults older than 55 years. Both vaccines are 90%<br />
effective in preventing the 4 kinds of the meningococcus germ (types A,<br />
C, Y, W-135) which cause about 70% of the disease in the United States.<br />
<strong>Meningitis</strong> vaccine is NOW available FREE via University Health &<br />
Medical Services and its partner The Brooklyn Hospital Center. It<br />
should also be available via your private health care provider. Cost<br />
varies along with coverage and range from $80-150.00.<br />
You can also find information about the disease at the New York State<br />
Department of Health Website: http://www.health.state.ny.us/ or the<br />
American College Health Association (ACHA) Website:<br />
WWW.ACHA.ORG.<br />
NOTE: This Section must be filled out by a verifiable licensed provider,<br />
preferably a MD, whose signature, stamp, and license is clearly<br />
documented on the form,<br />
I have read the above information and understand the risk<br />
of not having the vaccine. I have decided not to obtain<br />
immunization against the meningococcal meningitis disease.<br />
__________________________________________________<br />
Signature:<br />
Please note that according to NYS Public Health Law, no institutions shall permit any student to attend the institution in excess of 30 days without<br />
complying with this law. The 30-day period may be extended to 45 days for out-of-state student by completing a request for extension form.


