

National Project Implementation Plan - NVBDCP
National Project Implementation Plan - NVBDCP
National Project Implementation Plan - NVBDCP

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Type of<br />
Vector<br />
Borne<br />
Disease<br />
Description of the<br />
Vector and<br />
Causative Agent<br />
Description of the<br />
Infection and health<br />
impact<br />
Geographical<br />
dispersion<br />
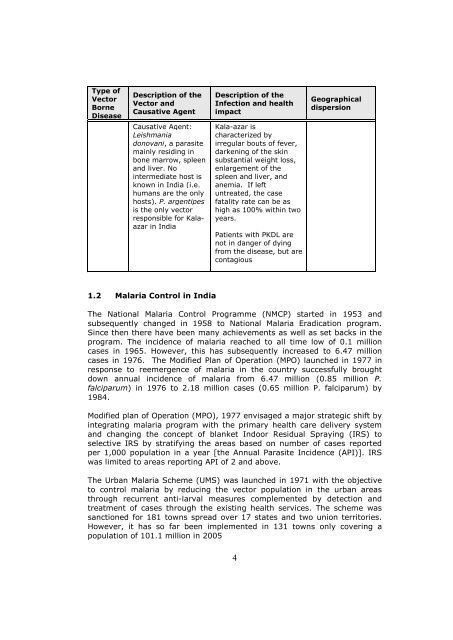
Causative Agent:<br />
Leishmania<br />
donovani, a parasite<br />
mainly residing in<br />
bone marrow, spleen<br />
and liver. No<br />
intermediate host is<br />
known in India (i.e.<br />
humans are the only<br />
hosts). P. argentipes<br />
is the only vector<br />
responsible for Kalaazar<br />
in India<br />
Kala-azar is<br />
characterized by<br />
irregular bouts of fever,<br />
darkening of the skin<br />
substantial weight loss,<br />
enlargement of the<br />
spleen and liver, and<br />
anemia. If left<br />
untreated, the case<br />
fatality rate can be as<br />
high as 100% within two<br />
years.<br />
Patients with PKDL are<br />
not in danger of dying<br />
from the disease, but are<br />
contagious<br />
1.2 Malaria Control in India<br />
The <strong>National</strong> Malaria Control Programme (NMCP) started in 1953 and<br />
subsequently changed in 1958 to <strong>National</strong> Malaria Eradication program.<br />
Since then there have been many achievements as well as set backs in the<br />
program. The incidence of malaria reached to all time low of 0.1 million<br />
cases in 1965. However, this has subsequently increased to 6.47 million<br />
cases in 1976. The Modified <strong>Plan</strong> of Operation (MPO) launched in 1977 in<br />
response to reemergence of malaria in the country successfully brought<br />
down annual incidence of malaria from 6.47 million (0.85 million P.<br />
falciparum) in 1976 to 2.18 million cases (0.65 million P. falciparum) by<br />
1984.<br />
Modified plan of Operation (MPO), 1977 envisaged a major strategic shift by<br />
integrating malaria program with the primary health care delivery system<br />
and changing the concept of blanket Indoor Residual Spraying (IRS) to<br />
selective IRS by stratifying the areas based on number of cases reported<br />
per 1,000 population in a year [the Annual Parasite Incidence (API)]. IRS<br />
was limited to areas reporting API of 2 and above.<br />
The Urban Malaria Scheme (UMS) was launched in 1971 with the objective<br />
to control malaria by reducing the vector population in the urban areas<br />
through recurrent anti-larval measures complemented by detection and<br />
treatment of cases through the existing health services. The scheme was<br />
sanctioned for 181 towns spread over 17 states and two union territories.<br />
However, it has so far been implemented in 131 towns only covering a<br />
population of 101.1 million in 2005<br />
4














