Current Treatment Strategies in Dermatology - The Dermatologist
Current Treatment Strategies in Dermatology - The Dermatologist
Current Treatment Strategies in Dermatology - The Dermatologist

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Supplement to<br />
Special<br />
Report<br />
®<br />
www.the-dermatologist.com<br />
Practical and Cl<strong>in</strong>ical Insights <strong>in</strong>to Today’s <strong>Dermatology</strong> Issues | August 2012
Special<br />
Report<br />
Contents<br />
3 Patient Resources<br />
When treat<strong>in</strong>g patients who present to you with conditions like acne, rosacea, psoriasis, sk<strong>in</strong> cancer and atopic dermatitis,<br />
there are several great patient support groups and websites you can recommend.<br />
Stefanie Tuleya, Executive Editor<br />
7 <strong>Current</strong> <strong>Treatment</strong> Options for Acne Vulgaris and Acne Rosacea<br />
A review of the proposed pathogenesis of these conditions as well as the many different treatment options available.<br />
L<strong>in</strong>dsay C. Strowd, MD<br />
15 <strong>The</strong> <strong>The</strong>rapeutic Approach to Psoriasis<br />
Recent research has shown the role that the immune system plays <strong>in</strong> the pathogenesis of this disease, which may lead<br />
to the development of immune-specific therapies. This article highlights current approaches <strong>in</strong> treat<strong>in</strong>g and manag<strong>in</strong>g<br />
patients with psoriasis.<br />
Alyssa S. Daniel, MD<br />
24 <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> for Sk<strong>in</strong> Cancer<br />
A review of novel approaches and comb<strong>in</strong>ation therapies to effectively manage sk<strong>in</strong> cancer.<br />
Jenna L. O’Neill, MD<br />
33 <strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
As the cause of the condition is considered multifactorial, the treatment plan should <strong>in</strong>clude comb<strong>in</strong>ation therapies and<br />
avoidance of triggers.<br />
Megan A. K<strong>in</strong>ney, MD, MHAM<br />
41 New Products<br />
42 Calendar of Events<br />
HMP Communications<br />
Editorial Staff<br />
Design & Production<br />
Bus<strong>in</strong>ess Staff<br />
83 General Warren Blvd,<br />
Suite 100<br />
Malvern, PA 19355<br />
(800) 237-7285<br />
(610) 560-0500<br />
Fax (610) 560-0501<br />
Executive Editor<br />
Stefanie Tuleya<br />
Assistant Editor<br />
Julia Ernst, MS<br />
Special Projects Editor<br />
Stephanie Wasek<br />
Creative Director<br />
Vic Geanopulos<br />
Art Director<br />
Karen Copestakes<br />
Production Manager<br />
Monica McLaughl<strong>in</strong><br />
Vice President/Group Publisher<br />
Christopher Ciraulo<br />
Publish<strong>in</strong>g Director<br />
Michael F. DiBella<br />
Publisher<br />
Sydney Slater<br />
Copyright 2012 © HMP Communications, LLC<br />
2 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
Patient Resources<br />
When treat<strong>in</strong>g patients who present to you with conditions like acne, rosacea, psoriasis, sk<strong>in</strong> cancer and<br />
atopic dermatitis, there are several great patient support groups and websites you can recommend.<br />
Stefanie Tuleya, Executive Editor<br />
In an effort to help patients cope with a new diagnosis or a<br />
chronic, long-term condition, referral to organizations or resources<br />
the patient can consult between office visits can be<br />
extremely valuable. <strong>The</strong>se organizations and resources can offer<br />
educational materials, support through contact with other patients<br />
and answers to frequently asked questions. Here is a look at<br />
some of the available resources to share with your patients.<br />
Acne<br />
<strong>The</strong> American Academy of <strong>Dermatology</strong> (AAD) offers AcneNet<br />
— www.sk<strong>in</strong>carephysicians.com/acnenet — which<br />
<strong>in</strong>cludes an overview of the causes of acne and articles about<br />
treatment and sk<strong>in</strong> care tips. <strong>The</strong> acne treatment section describes<br />
over-the-counter treatments and prescription medications,<br />
such as isotret<strong>in</strong>o<strong>in</strong>, oral antibiotics, oral contraceptives<br />
and topicals, and also <strong>in</strong>cludes a discussion of physical procedures<br />
from chemical peels to phototherapy. <strong>The</strong>re is also a<br />
section of the site dedicated to acne scars, <strong>in</strong>clud<strong>in</strong>g frequently<br />
asked questions and available treatments.<br />
Another site, www.acnemonth.com, which is supported by<br />
Galderma, conta<strong>in</strong>s <strong>in</strong>formation about National Acne Month,<br />
which is held <strong>in</strong> June. On this site, patients can learn about<br />
the causes of acne and treatments; it <strong>in</strong>cludes a section on<br />
how to talk to doctors about acne, with suggested questions<br />
they should ask and what questions from their doctors they<br />
should be prepared to answer. <strong>The</strong> Acne: Facts or Fiction page<br />
dispels several common acne myths. <strong>The</strong>re are tips for patients<br />
on how to care for their sk<strong>in</strong> and take control of their acne.<br />
In addition, there are videos from lead<strong>in</strong>g dermatologists that<br />
offer tips for parents on how to help their teens with acne.<br />
Groups like the NEA are great resources for patients.<br />
Atopic Dermatitis<br />
Eczema, particularly moderate to severe atopic dermatitis,<br />
can be very difficult for patients and their families to deal<br />
with on a daily basis. <strong>The</strong> burden can be attributed to pa<strong>in</strong>ful<br />
flares, difficulty sleep<strong>in</strong>g and sometimes embarrassment from<br />
the highly visible physical signs and symptoms.<br />
Help<strong>in</strong>g patients understand the condition and the best<br />
treatments and offer<strong>in</strong>g tips that help them comply with their<br />
treatments will go a long way <strong>in</strong> help<strong>in</strong>g them control flares<br />
and cope, both physically and psychologically.<br />
<strong>The</strong> National Eczema Association (NEA) organization supports<br />
patients with eczema and associated conditions. Its mission,<br />
as described on its website (www.nationaleczema.org), is<br />
to improve “the health and quality of life for <strong>in</strong>dividuals with<br />
eczema through research, support and education.”<br />
<strong>The</strong> NEA is a national, patient-oriented organization governed<br />
by a Board of Directors and guided by a Scientific Advisory<br />
Committee of physicians and scientists who donate<br />
their time and expertise.<br />
Through the site, visitors can sign up to receive the association’s<br />
newsletter, <strong>The</strong> Advocate. Patients can search the site<br />
for tips from others who also have eczema, watch treatment<br />
videos, f<strong>in</strong>d ways to get <strong>in</strong>volved <strong>in</strong> advocacy, download educational<br />
pamphlets for parents as well as educators and f<strong>in</strong>d<br />
<strong>in</strong>formation about current research.<br />
<strong>The</strong> NEA also offers programs like <strong>The</strong> Eczema & Sensitive-Sk<strong>in</strong><br />
Education (EASE) Program and the Seal of Acceptance<br />
program, which are designed to help identify products<br />
that are best for patients with eczema.<br />
Through the organization’s website, patients can access educational<br />
references about sk<strong>in</strong> care and treatment tips and a<br />
3D eczema photo library.<br />
<strong>The</strong> AAD also offers EczemaNet (www.sk<strong>in</strong>carephysicians.<br />
com/eczemanet), which <strong>in</strong>cludes background <strong>in</strong>formation on<br />
eczema, def<strong>in</strong>itions of types of eczema, how the condition is<br />
diagnosed, treatment overviews, tips for prevent<strong>in</strong>g flare-ups,<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 3
Patient Resources<br />
frequently-asked questions and news and articles on the topic.<br />
Various sections <strong>in</strong>clude reference guides, such as bath<strong>in</strong>g and<br />
moisturiz<strong>in</strong>g guidel<strong>in</strong>es, plus lists of products to avoid and tips<br />
specifically for atopic dermatitis patients.<br />
Psoriasis<br />
<strong>The</strong> National Psoriasis Foundation (NPF), whose mission<br />
is “to f<strong>in</strong>d a cure for psoriasis and psoriatic arthritis<br />
and to elim<strong>in</strong>ate their devastat<strong>in</strong>g effects through research,<br />
advocacy and education,” was established <strong>in</strong> October 1968.<br />
However, the organization, accord<strong>in</strong>g to press material<br />
from the NPF, actually started on August 29, 1966, when<br />
Beverly Foster’s husband placed a classified ad <strong>in</strong> a Portland,<br />
OR, newspaper ask<strong>in</strong>g people with psoriasis to call her so<br />
she would have others to talk with about her severe psoriasis.<br />
After receiv<strong>in</strong>g more than 100 calls <strong>in</strong> a week, Beverly<br />
Foster began organiz<strong>in</strong>g meet<strong>in</strong>gs and <strong>in</strong>itially formed the<br />
Psoriasis Society of Oregon, which eventually became the<br />
National Psoriasis Foundation, with a group of volunteers<br />
who are rais<strong>in</strong>g money to <strong>in</strong>crease awareness about psoriasis<br />
and help raise money and <strong>in</strong>terest for more research<br />
about the condition.<br />
This organization, which patients can learn more about by<br />
visit<strong>in</strong>g www.psoriasis.org, offers several programs and services<br />
for patients with psoriasis, lobbies on Capitol Hill and<br />
provides support to those liv<strong>in</strong>g with psoriatic diseases.<br />
On the website, patients can learn about psoriasis — from<br />
types of psoriasis, treatment options and answers to frequently<br />
asked questions to more <strong>in</strong>formation about their rights to<br />
healthcare. <strong>The</strong>re is <strong>in</strong>formation on how to get <strong>in</strong>volved with<br />
volunteer work, how to f<strong>in</strong>d a doctor and tips for navigat<strong>in</strong>g<br />
the healthcare system.<br />
<strong>The</strong> NPF works with <strong>in</strong>surance companies to reform restrictive<br />
policies that prevent psoriasis and psoriatic arthritis<br />
patients from gett<strong>in</strong>g the care they need. One such <strong>in</strong>itiative,<br />
its Access Action Guide, is a step-by-step guide for patients to<br />
access health care through <strong>in</strong>surance programs.<br />
As a member of the NPF, patients can connect with others<br />
liv<strong>in</strong>g with these conditions through message boards, networks,<br />
webcasts, mentor<strong>in</strong>g programs and more. Patients can<br />
also connect to the NPF through the organization’s social network<strong>in</strong>g<br />
sites on Twitter (www.twitter.com/NPF) and Facebook<br />
(www.facebook.com/NationalPsoriasis.Foundation).<br />
<strong>The</strong> NPS also has a site, www.psome.org, for children<br />
who have psoriasis or psoriatic arthritis. On this site, patients<br />
and their parents can connect with others who are <strong>in</strong><br />
the same situation and they can also have access to downloadable<br />
resources like handouts for schoolmates, teammates<br />
and others <strong>in</strong> the community to help expla<strong>in</strong> what<br />
the conditions are.<br />
Rosacea<br />
<strong>The</strong> National Rosacea Society (NRS), which was started<br />
<strong>in</strong> 1992 and celebrates its 20th anniversary this year, provides<br />
support to the estimated 16 million Americans who live with<br />
rosacea. Accord<strong>in</strong>g to the organization, which patients can<br />
learn more about at www.rosacea.org, the NRS uses education<br />
and advocacy to meet its mission, which is:<br />
• To raise awareness of rosacea.<br />
• To provide public health <strong>in</strong>formation on the disorder.<br />
• To encourage and support medical research that may lead to improvements<br />
<strong>in</strong> its management, prevention and potential cure.”<br />
<strong>The</strong> NRS also offers a grants program to encourage and<br />
support medical research to improve rosacea treatment, management<br />
and potential prevention. <strong>The</strong> program is supported<br />
entirely by donations.<br />
<strong>The</strong> group’s website offers patients everyth<strong>in</strong>g from an<br />
overview of treatment options to makeup tips and rosacea<br />
triggers to avoid. <strong>The</strong> NRS offers brochures, such as a<br />
“Rosacea Diary: An Easy Way to F<strong>in</strong>d and Avoid Your Personal<br />
Rosacea Triggers,” and its Rosacea Review newsletter,<br />
both of which patients can order onl<strong>in</strong>e. <strong>The</strong>re are several<br />
photos depict<strong>in</strong>g the types of rosacea, as well and before<br />
and after treatment photos.<br />
Sk<strong>in</strong> Cancer<br />
S<strong>in</strong>ce its found<strong>in</strong>g <strong>in</strong> 1979, the Sk<strong>in</strong> Cancer Foundation<br />
(www.sk<strong>in</strong>cancer.org) has worked to educate the public and<br />
the medical profession about sk<strong>in</strong> cancer, prevention by means<br />
of sun protection, the need for early detection, and prompt,<br />
effective treatment, accord<strong>in</strong>g to its website.<br />
Through the site, patients can access accurate <strong>in</strong>formation<br />
about diagnosis and treatment options — whether it’s<br />
act<strong>in</strong>ic keratosis, basal cell carc<strong>in</strong>oma, squamous cell carc<strong>in</strong>oma<br />
or melanoma. It offers sk<strong>in</strong> cancer facts, video descriptions,<br />
news and more. And, s<strong>in</strong>ce prevention is one of<br />
the Foundation’s ma<strong>in</strong> goals, there is a significant amount<br />
of <strong>in</strong>formation about self exam<strong>in</strong>ations, signs to look for<br />
and <strong>in</strong>formation about sun protective clothes and sunscreens.<br />
Patients can also f<strong>in</strong>d the Sk<strong>in</strong> Cancer Foundation<br />
on Facebook (www.facebook.com/sk<strong>in</strong>cancerfoundation)<br />
and Twitter (twitter.com/sk<strong>in</strong>cancerorg).<br />
<strong>The</strong> Mayo Cl<strong>in</strong>ic also offers a sk<strong>in</strong> cancer resource on<br />
its website (www.mayocl<strong>in</strong>ic.com/health/sk<strong>in</strong>-cancer/<br />
DS00190). This site organizes <strong>in</strong>formation by:<br />
• Basic, which <strong>in</strong>cludes <strong>in</strong>formation about def<strong>in</strong>itions,<br />
symptoms, how patients can prepare for appo<strong>in</strong>tments,<br />
treatment options, prevention tips and more.<br />
• In-Depth, which offers more detailed <strong>in</strong>formation about<br />
tests and diagnosis, how treatments like Mohs surgery<br />
work, and answers about sunscreens.<br />
• Multimedia, which <strong>in</strong>cludes images, videos and slideshows.<br />
• Expert Answers, which offers a Q&A about tann<strong>in</strong>g bed use.<br />
• Resources, which <strong>in</strong>cludes <strong>in</strong>formation about Mayo Cl<strong>in</strong>ic<br />
services and l<strong>in</strong>ks to other sites.<br />
<strong>The</strong> AAD offers Sk<strong>in</strong>CancerNet, which patients can access<br />
at www.sk<strong>in</strong>carephysicians.com/sk<strong>in</strong>cancernet. <strong>The</strong> site<br />
<strong>in</strong>cludes recent news about advances <strong>in</strong> treatments, <strong>in</strong>formation<br />
about what sk<strong>in</strong> cancer is, how it’s caused, prevention<br />
tips and <strong>in</strong>formation about diagnosis and treatment. It has a<br />
l<strong>in</strong>k for patients to sign up for a free, monthly e-newsletter<br />
from the AAD. n<br />
4 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> <strong>Treatment</strong> Options for Acne<br />
Vulgaris and Acne Rosacea<br />
A review of the proposed pathogenesis of these conditions as well as the many different treatment<br />
options available.<br />
L<strong>in</strong>dsay C. Strowd, MD<br />
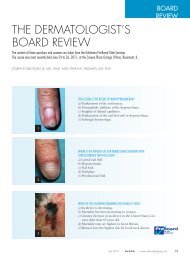
Figure 1. Inflammatory papules on the cheeks and periorbital sk<strong>in</strong>. <strong>The</strong>se papules are characteristic of both<br />
acne vulgaris and the papulopustular variant of acne rosacea.<br />
Photograph courtesy of Graham Library, Wake Forest Baptist Health Department of <strong>Dermatology</strong>.<br />
Acne vulgaris and acne rosacea are two dist<strong>in</strong>ct but<br />
related entities that affect more than 60 million<br />
Americans comb<strong>in</strong>ed and cost upward of $3 billion<br />
yearly. <strong>The</strong>se diseases have a significant, negative<br />
impact on quality of life. 1 <strong>The</strong> terms acne vulgaris and<br />
acne rosacea represent a group of diseases and disease subtypes<br />
with different cl<strong>in</strong>ical features and treatments. This article<br />
will briefly review the proposed pathogenesis of these<br />
conditions and cover the many different treatment options<br />
currently available.<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 7
<strong>Current</strong> <strong>Treatment</strong> Options For Acne Vulgaris And Acne Rosacea<br />
Pathogenesis and Classification<br />
<strong>The</strong> acne lesion orig<strong>in</strong>ates from the pilosebaceous unit of the<br />
sk<strong>in</strong>, which expla<strong>in</strong>s its predilection for more sebaceous sk<strong>in</strong><br />
like the face, chest and upper back. Shed kerat<strong>in</strong>ocytes form<br />
a plug at the level of the hair <strong>in</strong>fundibulum, which prevents<br />
sebum from be<strong>in</strong>g extruded to the sk<strong>in</strong> surface. <strong>The</strong> affected<br />
pilosebaceous unit expands until the comedo ruptures, creat<strong>in</strong>g<br />
<strong>in</strong>flammation. Because sebaceous glands are heavily <strong>in</strong>fluenced<br />
by hormonal stimulation, <strong>in</strong>creases <strong>in</strong> hormone levels (such as<br />
with adrenarche) often precipitate the development of acne.<br />
Proprionibacterium acnes (P. acnes) are Gram-positive rods found<br />
with<strong>in</strong> the pilosebaceous unit and contribute to acne formation<br />
by <strong>in</strong>duc<strong>in</strong>g comedo rupture and generat<strong>in</strong>g pro-<strong>in</strong>flammatory<br />
cytok<strong>in</strong>es. 2 Despite popular belief, there is no evidence<br />
to suggest that exogenous factors such as make-up or sk<strong>in</strong>care<br />
products contribute to acne development. 3<br />
Acne vulgaris can be organized <strong>in</strong>to two ma<strong>in</strong> categories<br />
based on lesion morphology: <strong>in</strong>flammatory and non-<strong>in</strong>flammatory,<br />
or comedonal. While a m<strong>in</strong>ority of patients will have,<br />
exclusively, one type of acne, the majority present with both<br />
types of lesions. <strong>The</strong>re is a wide spectrum of disease severity<br />
among patients, rang<strong>in</strong>g from mild comedonal acne to severe<br />
nodulocystic scarr<strong>in</strong>g acne. Several acne variants exist and <strong>in</strong>clude<br />
acne conglobata, acne fulm<strong>in</strong>ans, drug-<strong>in</strong>duced acne and<br />
acne <strong>in</strong> the sett<strong>in</strong>g of syndromes like SAPHO (synovitis, acne,<br />
pustulosis, hyperostosis, osteitis) and PAPA (pyogenic arthritis,<br />
pyoderma gangrenosum, acne). Acne conglobata, def<strong>in</strong>ed as<br />
severe nodulocystic acne without systemic manifestations, is<br />
often associated with dissect<strong>in</strong>g cellulitis of the scalp, hidradenitis<br />
suppurativa and pilar cysts, collectively known as the<br />
Compared to acne, rosacea has<br />
more variable presentations,<br />
and, <strong>in</strong> contrast to acne<br />
vulgaris, rosacea can have<br />
ocular <strong>in</strong>volvement.<br />
follicular occlusion tetrad. Acne fulm<strong>in</strong>ans is the most severe<br />
form, with large, dra<strong>in</strong><strong>in</strong>g, ulcerated nodules accompanied by<br />
systemic signs and symptoms such as fever, malaise, leukocytosis<br />
and elevated <strong>in</strong>flammatory markers. Drug-<strong>in</strong>duced acne<br />
has been reported with numerous medications but is relatively<br />
common with the use of steroids and steroid-derivatives, as<br />
well as lithium, iodides and bromides. 4<br />
Rosacea is another adnexal <strong>in</strong>flammatory disorder that often<br />
mimics acne vulgaris cl<strong>in</strong>ically but differs <strong>in</strong> epidemiology,<br />
pathogenesis and subtypes. While acne typically affects younger<br />
patients with any Fitzpatrick sk<strong>in</strong> type, the vast majority of patients<br />
with rosacea tend to be fair-sk<strong>in</strong>ned <strong>in</strong>dividuals <strong>in</strong> the<br />
third decade of life and older. Key elements of pathogenesis<br />
<strong>in</strong>clude the presence of <strong>in</strong>flammation <strong>in</strong> vascular and sk<strong>in</strong> tissue<br />
and vascular hyperreactivity. New studies are focus<strong>in</strong>g on the<br />
presence of antimicrobial and pro<strong>in</strong>flammatory canthelicid<strong>in</strong>s<br />
and their impact on the altered immune response seen <strong>in</strong> rosacea<br />
patients. Infectious agents such as Demodex folliculorum mites<br />
and Proprionibacterium acnes have also been implicated. 5<br />
Compared to acne, rosacea has more variable presentations,<br />
and, <strong>in</strong> contrast to acne vulgaris, rosacea can have<br />
ocular <strong>in</strong>volvement. Erythematotelangiectatic rosacea is<br />
the most common variant and is characterized by episodic<br />
flush<strong>in</strong>g and the presence of facial telangiectasias, giv<strong>in</strong>g the<br />
sk<strong>in</strong> an overall ruddy appearance. Patients often compla<strong>in</strong> of<br />
st<strong>in</strong>g<strong>in</strong>g and burn<strong>in</strong>g sensations. Papulopustular rosacea is<br />
the second most common subtype and more closely mimics<br />
acne vulgaris, with multiple <strong>in</strong>flammatory papules and<br />
pustules on the face. Phymatous rosacea is less common but<br />
can be extremely disfigur<strong>in</strong>g, with nodular enlargement of<br />
the nose along with <strong>in</strong>creased sebaceous gland production.<br />
Ocular rosacea can accompany other forms of rosacea or<br />
be the only cl<strong>in</strong>ical manifestation of disease. Patients compla<strong>in</strong><br />
of itch<strong>in</strong>g, burn<strong>in</strong>g and redness of the conjunctiva and<br />
lid marg<strong>in</strong>. Several rare variants of rosacea exist, analogous<br />
to acne variants discussed above. Granulomatous rosacea<br />
is a rare variant <strong>in</strong> which patients develop <strong>in</strong>durated firm<br />
papules and nodules on the face that can lead to scarr<strong>in</strong>g.<br />
Rosacea fulm<strong>in</strong>ans is another rare rosacea variant that, like<br />
acne fulm<strong>in</strong>ans, can have systemic complications and lead to<br />
severe scarr<strong>in</strong>g and disfigurement. 6<br />
Topical <strong>Treatment</strong>s<br />
Numerous topical medications have been studied and used<br />
extensively <strong>in</strong> the treatment of acne and rosacea. Topical treatments<br />
are the cornerstone of therapy for these conditions and<br />
are beneficial <strong>in</strong> that they deliver the drug directly to the sk<strong>in</strong><br />
while m<strong>in</strong>imiz<strong>in</strong>g the side effects of systemic medications.<br />
<strong>The</strong>re is a significant body of literature available on different<br />
topical medications for these entities, but there are relatively<br />
few head-to-head, double bl<strong>in</strong>d, randomized, controlled trials<br />
compar<strong>in</strong>g different topical acne and rosacea medications.<br />
Many studies compare an active drug to placebo, thereby<br />
mak<strong>in</strong>g it difficult to say whether one topical medication is<br />
truly more efficacious than another.<br />
<strong>The</strong> first group of medications used for acne and rosacea<br />
are topical antibiotics. This class of medications <strong>in</strong>cludes topical<br />
cl<strong>in</strong>damyc<strong>in</strong>, erythromyc<strong>in</strong>, metronidazole and dapsone.<br />
Topical antibiotics exert anti-microbial effects on P. acnes as<br />
well as anti-<strong>in</strong>flammatory effects. 2 <strong>The</strong>se medications are<br />
more commonly prescribed for <strong>in</strong>flammatory lesions of acne<br />
and rosacea as opposed to comedonal lesions.<br />
Topical cl<strong>in</strong>damyc<strong>in</strong> 1% is available <strong>in</strong> foam, gel, solution<br />
and lotion formulations as well as <strong>in</strong> comb<strong>in</strong>ation topical<br />
medications with benzoyl peroxide and with tret<strong>in</strong>o<strong>in</strong>. Topical<br />
cl<strong>in</strong>damyc<strong>in</strong> tends to be well tolerated by patients with<br />
8 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> <strong>Treatment</strong> Options For Acne Vulgaris And Acne Rosacea<br />
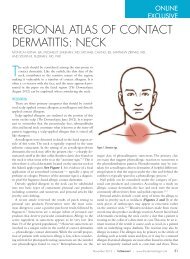
Figure 2. Open comedones of acne vulgaris on periorbital sk<strong>in</strong>.<br />
Photograph courtesy of Graham Library, Wake Forest Baptist Health Department of <strong>Dermatology</strong>.<br />
m<strong>in</strong>imal irritation and dryness. Systemic absorption is m<strong>in</strong>imized<br />
with topical application, which greatly decreases the<br />
risk of serious side effects such as pseudomembranous colitis.<br />
Topical erythromyc<strong>in</strong> is an older acne and rosacea medication<br />
that also works by <strong>in</strong>hibit<strong>in</strong>g the growth of P. acnes.<br />
Erythromyc<strong>in</strong> is available <strong>in</strong> a 2% concentration as an o<strong>in</strong>tment,<br />
gel, solution and <strong>in</strong> pads as well as <strong>in</strong> a 3% concentration<br />
comb<strong>in</strong>ed with benzoyl peroxide.<br />
Both topical cl<strong>in</strong>damyc<strong>in</strong> and erythromyc<strong>in</strong> products have<br />
been widely used for acne and, to a lesser degree, rosacea;<br />
however, there is grow<strong>in</strong>g evidence and concern about the<br />
development of P. acnes stra<strong>in</strong>s, which were resistant to these<br />
antibiotics. <strong>The</strong> body of evidence is somewhat conflict<strong>in</strong>g regard<strong>in</strong>g<br />
<strong>in</strong>creas<strong>in</strong>g rates of resistant bacteria, but most providers<br />
use these topical antibiotics as short-term treatment and<br />
usually avoid them as monotherapy.<br />
Topical metronidazole is an FDA-approved first-l<strong>in</strong>e treatment<br />
for rosacea, especially the papulopustular variant. Several<br />
studies have shown metronidazole to be significantly more effective<br />
than placebo <strong>in</strong> treat<strong>in</strong>g rosacea. 7,8 Both 0.75% and 1%<br />
concentrations are available <strong>in</strong> cream, gel and lotion formulations.<br />
Studies have shown that once-daily application of either<br />
concentration is equally efficacious to twice-daily application<br />
with no difference <strong>in</strong> efficacy between the two strengths.<br />
Topical dapsone is the newest topical antibiotic to be FDAapproved<br />
for the treatment of acne. Dapsone downregulates tumor<br />
necrosis factor, prostagland<strong>in</strong>s and leukotrienes and <strong>in</strong>hibits<br />
neutrophil function and migration. It is used <strong>in</strong> both oral and<br />
topical preparations for dermatologic conditions, although oral<br />
dapsone has serious potential risks, <strong>in</strong>clud<strong>in</strong>g methemoglob<strong>in</strong>emia<br />
and hemolytic anemia. Topical dapsone m<strong>in</strong>imizes these<br />
side effects while still target<strong>in</strong>g <strong>in</strong>flammatory acne lesions. In<br />
one study, twice-daily application of topical dapsone 5% gel<br />
resulted <strong>in</strong> a 50% decrease <strong>in</strong> <strong>in</strong>flammatory lesions. 2,9<br />
Topical ret<strong>in</strong>oids have been used for decades for both acne<br />
vulgaris and acne rosacea. Ret<strong>in</strong>oids treat acneiform lesions by<br />
reduc<strong>in</strong>g follicular kerat<strong>in</strong>ization, which prevents microcomdone<br />
and comedone formation. 2 Many studies have shown<br />
that comb<strong>in</strong><strong>in</strong>g topical ret<strong>in</strong>oids with other topical medications<br />
such as topical antibiotics and topical benzoyl peroxide<br />
or salicylic acid have a synergistic effect on acne lesions.<br />
Three topical ret<strong>in</strong>oids are currently approved by the FDA<br />
for acne: adapalene, tret<strong>in</strong>o<strong>in</strong> and tazarotene.<br />
Adapalene is a third-generation ret<strong>in</strong>oid that comes <strong>in</strong> 0.1%<br />
and 0.3% concentrations and <strong>in</strong> several vehicles, <strong>in</strong>clud<strong>in</strong>g gel<br />
and lotion. Adapalene is also available <strong>in</strong> a comb<strong>in</strong>ation product<br />
with benzoyl peroxide and has shown synergistic effects on<br />
acne lesions. 10 Studies show adapalene has similar efficacy to<br />
other topical ret<strong>in</strong>oids but causes significantly less sk<strong>in</strong> irritation,<br />
11 which is critically important when consider<strong>in</strong>g patient<br />
adherence to a topical treatment regimen.<br />
Tret<strong>in</strong>o<strong>in</strong> is a first-generation ret<strong>in</strong>oid that is available <strong>in</strong><br />
multiple concentrations, <strong>in</strong>clud<strong>in</strong>g 0.025%, 0.04%, 0.5% and<br />
0.1% as well as liquid, cream and gel vehicles. It is also available<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 9
<strong>Current</strong> <strong>Treatment</strong> Options For Acne Vulgaris And Acne Rosacea<br />
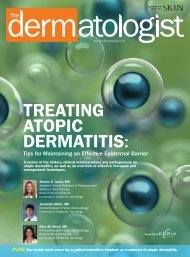
Figure 3. Histologic demonstration of a comedonal lesion. Large amounts of kerat<strong>in</strong>aceous debris fills a plugged<br />
pilosebaceous unit, associated with significant surround<strong>in</strong>g <strong>in</strong>flammatory <strong>in</strong>filtrate.<br />
Photograph courtesy of Graham Library, Wake Forest Baptist Health Department of <strong>Dermatology</strong>.<br />
as a comb<strong>in</strong>ation product with topical cl<strong>in</strong>damyc<strong>in</strong> 1%. Comb<strong>in</strong><strong>in</strong>g<br />
tret<strong>in</strong>o<strong>in</strong> and cl<strong>in</strong>damyc<strong>in</strong> results <strong>in</strong> greater reduction<br />
of acne lesions than either medic<strong>in</strong>e used alone. 12 Micronized<br />
tret<strong>in</strong>o<strong>in</strong> is a newer topical formulation designed for better sk<strong>in</strong><br />
penetration and reduced UV degradation along with less severe<br />
sk<strong>in</strong> irritation. 13,14<br />
Tazarotene is the third topical ret<strong>in</strong>oid approved for acne<br />
treatment and is a third-generation ret<strong>in</strong>oid. Tazarotene comes<br />
<strong>in</strong> 0.05% and 0.1% concentrations and is available as a cream or<br />
gel. Though older studies <strong>in</strong>itially showed topical tazarotene to<br />
be superior to the other topical ret<strong>in</strong>oids <strong>in</strong> acne lesion reduction,<br />
newer studies suggest it has similar efficacy to topical tret<strong>in</strong>o<strong>in</strong><br />
and adapalene but is associated with significantly more<br />
sk<strong>in</strong> irritation. 15,16<br />
Topical ret<strong>in</strong>oids are used much less frequently <strong>in</strong> acne rosacea<br />
and there is little evidence to provide direct support for<br />
their use for this condition. 17 Recently, one article showed<br />
that topical tret<strong>in</strong>o<strong>in</strong> and cl<strong>in</strong>damyc<strong>in</strong> used <strong>in</strong> comb<strong>in</strong>ation<br />
may improve the erythematotelangiectatic subtype but not<br />
the papulopustular subtype. 18<br />
Benzoyl peroxide and salicylic acid are two topical medications<br />
often used <strong>in</strong> comb<strong>in</strong>ation with topical antibiotics, topical<br />
ret<strong>in</strong>oids or both for treatment of acne. <strong>The</strong> synergistic effect<br />
of these medications is evident <strong>in</strong> the literature and reflected <strong>in</strong><br />
the <strong>in</strong>creas<strong>in</strong>g number of comb<strong>in</strong>ation acne medications. 19,20<br />
Benzoyl peroxide is thought to improve acne via its antibacterial<br />
actions aga<strong>in</strong>st P. acnes, while salicylic acid acts as both a<br />
keratolytic and an anti-<strong>in</strong>flammatory molecule. 21 <strong>The</strong> keratolytic<br />
properties of benzoyl peroxide may enhance the penetration<br />
of topical agents like antibiotics when applied <strong>in</strong> comb<strong>in</strong>ation.<br />
22 Comb<strong>in</strong>ation therapy with benzoyl peroxide and an<br />
antibiotic has also been shown to decrease the emergence of<br />
resistant stra<strong>in</strong>s. One study that compared a 5% benzoyl peroxide/cl<strong>in</strong>damyc<strong>in</strong><br />
gel and cl<strong>in</strong>damyc<strong>in</strong> monotherapy showed a<br />
> 1600% <strong>in</strong>crease of cl<strong>in</strong>damyc<strong>in</strong>-resistant P. acnes from basel<strong>in</strong>e<br />
<strong>in</strong> the monotherapy group over a 16-week period. 23 Benzoyl<br />
peroxide comb<strong>in</strong>ed with topical erythromyc<strong>in</strong> reduced papular<br />
lesions and Demodex populations and was comparable to topical<br />
metronidazole <strong>in</strong> rosacea patients. 20<br />
Both benzoyl peroxide and salicylic acid can result <strong>in</strong> sk<strong>in</strong><br />
irritation and dryness. Benzoyl peroxide is now an over-thecounter<br />
product and comes <strong>in</strong> a wide range of concentrations<br />
from 1% to 10%. Benzoyl peroxide is available as a topical<br />
gel, cream, lotion and solution as well as a wash. Physicians<br />
10 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> <strong>Treatment</strong> Options For Acne Vulgaris And Acne Rosacea<br />
should warn patients that benzoyl peroxide bleaches dyed fabrics.<br />
Studies have also shown benzoyl peroxide can produce an<br />
orange discoloration when comb<strong>in</strong>ed with sulfur-conta<strong>in</strong><strong>in</strong>g<br />
products and with topical dapsone 24 and can oxidize cl<strong>in</strong>damyc<strong>in</strong><br />
over time. 2 Salicylic acid is also available over-the-counter<br />
<strong>in</strong> a range of concentrations. Concentrations typically used<br />
on the face for acne are on the weaker end of this spectrum<br />
(0.5% to 3%). One study showed comb<strong>in</strong><strong>in</strong>g benzoyl peroxide<br />
and salicylic acid resulted <strong>in</strong> the greatest reduction of acne lesions,<br />
more than topical cl<strong>in</strong>damyc<strong>in</strong> or comb<strong>in</strong>ation topical<br />
cl<strong>in</strong>damyc<strong>in</strong> and benzoyl peroxide. 20<br />
Several other topical medications are used for acne and rosacea.<br />
Azaleic acid is a topical medication available <strong>in</strong> a 15%<br />
gel and a 20% cream for <strong>in</strong>flammatory acne and rosacea lesions.<br />
<strong>Current</strong>ly, only the 15% concentration is FDA approved<br />
for rosacea. Azelaic acid has anti-proliferative effects on kerat<strong>in</strong>ocytes,<br />
antimicrobial properties aga<strong>in</strong>st P. acnes and decreases<br />
sebum production. Studies have also shown azelaic acid to<br />
scavenge reactive oxygen species and <strong>in</strong>hibit UVB-produced<br />
pro-<strong>in</strong>flammatory cytok<strong>in</strong>es. 25 Several studies have shown azelaic<br />
acid to be significantly more effective than placebo <strong>in</strong> the<br />
treatment of rosacea. 7,8 Azelaic acid has the added benefit of<br />
be<strong>in</strong>g pregnancy class B, allow<strong>in</strong>g for use <strong>in</strong> pregnant patients.<br />
Sulfur-sodium sulfacetamide (SSS) is an older medication<br />
that has been approved by the FDA for acne and rosacea s<strong>in</strong>ce<br />
the 1950s. Sulfur and sodium sulfacetamide possess both anti-<strong>in</strong>flammatory<br />
and anti-bacterial properties aga<strong>in</strong>st P. acnes<br />
with moisturiz<strong>in</strong>g effects. 26 Along with topical metronidazole<br />
and azelaic acid, topical SSS has been extensively tested <strong>in</strong> rosacea<br />
patients. SSS is available <strong>in</strong> a lotion, cream, cleanser and<br />
foam. Newer formulations like the foam reduce lesion counts<br />
<strong>in</strong> both acne and rosacea patients while m<strong>in</strong>imiz<strong>in</strong>g the unpleasant<br />
sulfur odor associated with older formulations. 26,27,28<br />
Azelaic acid and SSS are alternative products for patients who<br />
cannot tolerate more irritat<strong>in</strong>g medications. <strong>The</strong>y can also be<br />
used <strong>in</strong> comb<strong>in</strong>ation with other topical agents.<br />
F<strong>in</strong>ally, topical calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors are sometimes prescribed<br />
for patients with steroid-<strong>in</strong>duced rosacea for their anti<strong>in</strong>flammatory<br />
properties. Topical pimecrolimus 1% cream and<br />
topical tacrolimus 1% o<strong>in</strong>tment both significantly decrease lesion<br />
counts <strong>in</strong> rosacea and are well-tolerated. 29 Other studies<br />
have reported topical calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors can <strong>in</strong>duce rosacealike<br />
dermatitis. 30 Topical z<strong>in</strong>c is a lesser known adjunct treatment<br />
for acne, but there are few studies exam<strong>in</strong><strong>in</strong>g its effectiveness.<br />
31 Botanical products have not been extensively studied <strong>in</strong><br />
acne and rosacea patients; most of the studies available are small<br />
case series or are underpowered. Topical tea tree oil 5% gel has<br />
been shown to be comparable to 5% topical benzoyl peroxide,<br />
but, aga<strong>in</strong>, no large studies have been completed. 7<br />
Oral <strong>Treatment</strong> Options<br />
Oral medications are another major treatment option for<br />
acne and rosacea. 32 Oral antibiotics are commonly prescribed<br />
for both conditions and are considered first-l<strong>in</strong>e therapy for<br />
moderate to severe disease. Due to their popularity, there is a<br />
Figure 4. Multiple <strong>in</strong>flammatory papules and nodules<br />
coalesc<strong>in</strong>g <strong>in</strong>to plaques on the cheeks and ch<strong>in</strong> of this<br />
patient with severe nodulocystic acne.<br />
Photograph courtesy of Graham Library, Wake Forest<br />
Baptist Health Department of <strong>Dermatology</strong>.<br />
concern about whether prolonged antibiotic therapy leads to<br />
development of antibiotic-resistant P. acnes. Most prescribers<br />
try to m<strong>in</strong>imize the risk of resistance by comb<strong>in</strong><strong>in</strong>g oral antibiotics<br />
with topical ret<strong>in</strong>oids and benzoyl peroxide and giv<strong>in</strong>g<br />
these medications for a limited time. 33,34<br />
Several different classes of oral antibiotics have been<br />
studied, <strong>in</strong>clud<strong>in</strong>g tetracycl<strong>in</strong>es. Tetracycl<strong>in</strong>es are a class of<br />
antibiotics, which, when given at anti-microbial doses, b<strong>in</strong>d<br />
to the 50S ribosome subunit of bacteria such as P. acnes<br />
and are bactericidal. Tetracycl<strong>in</strong>es also have important anti<strong>in</strong>flammatory<br />
effects; they downregulate <strong>in</strong>flammatory cytok<strong>in</strong>es,<br />
impede neutrophil chemotaxis and <strong>in</strong>hibit certa<strong>in</strong><br />
matrix metalloprote<strong>in</strong>ases. 2<br />
Doxycycl<strong>in</strong>e is a second-generation tetracycl<strong>in</strong>e that<br />
comes <strong>in</strong> 50-mg, 75-mg and 100-mg tablets and is available<br />
<strong>in</strong> an enteric-coated form. Doxycycl<strong>in</strong>e has been shown<br />
to be more effective than placebo <strong>in</strong> the treatment of both<br />
acne and rosacea. Orig<strong>in</strong>ally, doxycycl<strong>in</strong>e was prescribed <strong>in</strong><br />
100-mg to 200-mg daily doses, but studies have shown that<br />
lower doses of doxycycl<strong>in</strong>e, such as 40 mg daily, are just as<br />
effective at treat<strong>in</strong>g rosacea but with less toxicity. 8 A subantimicrobial<br />
dose of doxycycl<strong>in</strong>e is available specifically for<br />
acne and rosacea use (40-mg tablet) and is FDA approved<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 11
<strong>Current</strong> <strong>Treatment</strong> Options For Acne Vulgaris And Acne Rosacea<br />
Figure 5. This patient suffers from rh<strong>in</strong>ophymatous<br />
rosacea with erythema and enlargement of the<br />
sebaceous glands <strong>in</strong> the nose caus<strong>in</strong>g nasal deformity.<br />
Photograph courtesy of Graham Library, Wake Forest<br />
Baptist Health Department of <strong>Dermatology</strong>.<br />
for use for up to 12 months. Doxycycl<strong>in</strong>e can cause gastro<strong>in</strong>test<strong>in</strong>al<br />
symptoms <strong>in</strong> up to a third of patients but can be<br />
taken with food. Other side effects <strong>in</strong>clude photosensitivity,<br />
candidiasis, esophagitis and benign <strong>in</strong>tracranial hypertension.<br />
Tetracycl<strong>in</strong>es are contra<strong>in</strong>dicated <strong>in</strong> children under 8 years<br />
of age due to risk of teeth discoloration. 2,35<br />
M<strong>in</strong>ocycl<strong>in</strong>e is another second-generation tetracycl<strong>in</strong>e used <strong>in</strong><br />
both acne and rosacea. M<strong>in</strong>ocycl<strong>in</strong>e comes <strong>in</strong> 50-mg and 100-<br />
mg tablets or capsules and is typically dosed at 100 mg to 200<br />
mg daily. <strong>The</strong>re is now an extended-release version that is meant<br />
to be dosed at 1 mg/kg/day and, therefore, comes <strong>in</strong> a variety of<br />
strengths (45-, 55-, 65-, 80-, 90-, 105, 115-, 135-mg tablets). M<strong>in</strong>ocycl<strong>in</strong>e<br />
can cause vertigo, photosensitivity, benign <strong>in</strong>tracranial<br />
hypertension, drug-<strong>in</strong>duced lupus and sk<strong>in</strong> pigmentation. 2<br />
Macrolide antibiotics used to be commonly prescribed for<br />
acne patients, but <strong>in</strong>creas<strong>in</strong>g P. acnes resistance has limited their<br />
use. 2 Azithromyc<strong>in</strong> is a second-generation macrolide with a<br />
long half-life (68 hours) and comparable efficacy to doxycycl<strong>in</strong>e.<br />
It is considered safe to use <strong>in</strong> pregnant and breastfeed<strong>in</strong>g<br />
women and is Pregnancy Class B. Cephalex<strong>in</strong> and<br />
cl<strong>in</strong>damyc<strong>in</strong> are also occasionally used for acne treatment, but<br />
risk of pseudomembranous colitis prevents them from be<strong>in</strong>g<br />
first-l<strong>in</strong>e agents.<br />
Oral hormonal agents have ga<strong>in</strong>ed popularity <strong>in</strong> off-label<br />
use for acne, particularly <strong>in</strong> older patients. Adult acne tends to<br />
affect the lower face and neck and most women with adult<br />
acne actually have normal levels of circulat<strong>in</strong>g androgens. 3<br />
Anti-androgens are the most common class of hormonal<br />
agents and <strong>in</strong>clude androgen receptor blockers, <strong>in</strong>hibitors of<br />
peripheral androgen metabolism and <strong>in</strong>hibitors of androgens<br />
via effects on the ovaries or pituitary gland. 31 One metaanalysis<br />
of anti-androgen medications used for acne suggested<br />
eth<strong>in</strong>yl estradiol plus cyproterone acetate was the most effective<br />
agent; however, all agents studied were significantly better<br />
than placebo. 33 Oral spironolactone is an aldosterone antagonist<br />
that was orig<strong>in</strong>ally used as a potassium-spar<strong>in</strong>g diuretic<br />
but is also an anti-androgen that <strong>in</strong>hibits sebaceous gland<br />
activity. Spironolactone decreases 5-alpha reductase activity,<br />
which is <strong>in</strong>creased <strong>in</strong> acne-prone sk<strong>in</strong>. Spironolactone also<br />
<strong>in</strong>creases steroid hormone b<strong>in</strong>d<strong>in</strong>g globul<strong>in</strong>, which decreases<br />
levels of free testosterone. 3 <strong>The</strong>se effects make spironolactone<br />
a good choice for women with hormonal acne. Spironolactone<br />
is dosed between 25 mg and 200 mg daily, though most<br />
women will respond to 75-mg/day to 100-mg/day dos<strong>in</strong>g.<br />
Side effects <strong>in</strong>clude hypotension, diuresis, hyperkalemia, gynecomastia<br />
and decreased libido. <strong>The</strong>re is a black box warn<strong>in</strong>g<br />
on spironolactone regard<strong>in</strong>g the risk of breast carc<strong>in</strong>oma,<br />
though long-term studies have not shown an <strong>in</strong>creased risk. 3<br />
Oral isotret<strong>in</strong>o<strong>in</strong> is a first generation ret<strong>in</strong>oid with a halflife<br />
of 20 hours that has been used for decades to treat severe<br />
acne that is resistant to topical and other oral medications.<br />
This medication is usually dosed between 40 mg to 80 mg per<br />
day for 4 to 6 months, with the goal cumulative dose be<strong>in</strong>g<br />
150 mg/kg. Oral isotret<strong>in</strong>o<strong>in</strong> works on acne by decreas<strong>in</strong>g the<br />
activity of sebaceous glands as well as provid<strong>in</strong>g anti-proliferative<br />
effects on kerat<strong>in</strong>ocytes. <strong>The</strong> benefit of this medication is<br />
that it has a very high response rate <strong>in</strong> patients who have failed<br />
other first and second-l<strong>in</strong>e treatments.<br />
However, isotret<strong>in</strong>o<strong>in</strong> use comes with many potential side<br />
effects and is Catergory X, strictly contra<strong>in</strong>dicated <strong>in</strong> pregnancy<br />
due to high rate of birth defects. Due to its potential<br />
teratogenicity, all patients <strong>in</strong> the United States on this medication<br />
must enroll <strong>in</strong> the government drug-monitor<strong>in</strong>g program<br />
iPledge, and females must be on two forms of contraception<br />
while on isotret<strong>in</strong>o<strong>in</strong>. <strong>The</strong> most common side effects<br />
are dry sk<strong>in</strong>, dry lips and mucosal surfaces, arthralgia and hypertriglyceridemia;<br />
these tend to be dose-dependent. Numerous<br />
other side effects have been reported with isotret<strong>in</strong>o<strong>in</strong>,<br />
<strong>in</strong>clud<strong>in</strong>g pseudotumor cerebri, <strong>in</strong>flammatory bowel disease<br />
and <strong>in</strong>creased suicidality.<br />
<strong>The</strong> <strong>in</strong>creased risk of suicide is hotly debated <strong>in</strong> the literature.<br />
In a large cohort study from Sweden, the risk of suicide<br />
peaked 6 months after start<strong>in</strong>g treatment with isotret<strong>in</strong>o<strong>in</strong><br />
and fell to expected levels 3 years after treatment. Patients <strong>in</strong><br />
this study with a history of suicide attempts before start<strong>in</strong>g<br />
12 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> <strong>Treatment</strong> Options For Acne Vulgaris And Acne Rosacea<br />
Table 1. Medications Commonly Employed for Acne<br />
Drug Category Active Drug Common Brand Names<br />
Topical ret<strong>in</strong>oid Tret<strong>in</strong>o<strong>in</strong> + Ret<strong>in</strong>-A 0.025%, 0.05%, 0.1%; Avita 0.025%;<br />
Atral<strong>in</strong> 0.05%<br />
Adapalene + Differ<strong>in</strong> 0.1%, 0.3%<br />
Tazarotene *<br />
Tazorac 0.05%, 0.1%; Fabior<br />
Topical antibiotic Erythromyc<strong>in</strong> Akne-Myc<strong>in</strong>, Erygel, Emgel<br />
Cl<strong>in</strong>damyc<strong>in</strong><br />
Cleoc<strong>in</strong> T, Evocl<strong>in</strong><br />
Benzoyl peroxide Benzoyl peroxide Numerous: Proactiv, Clearasil, Oxy, others<br />
Fixed comb<strong>in</strong>ation products<br />
Benzoyl peroxide + antibiotic Benzoyl peroxide + erythromyc<strong>in</strong> Benzamyc<strong>in</strong><br />
Benzoyl peroxide + cl<strong>in</strong>damyc<strong>in</strong><br />
Benzacl<strong>in</strong>, Duac, Acanya<br />
Benzoyl peroxide + ret<strong>in</strong>oid Benzoyl peroxide + adapalene Epiduo<br />
Ret<strong>in</strong>oid + antibiotic Tret<strong>in</strong>o<strong>in</strong> + cl<strong>in</strong>damyc<strong>in</strong> Ziana, Velt<strong>in</strong><br />
Oral antibiotic Erythromyc<strong>in</strong> EES, Eryped, Ery-tab<br />
Tetracycl<strong>in</strong>e<br />
Sumyc<strong>in</strong><br />
Doxycycl<strong>in</strong>e<br />
Vibramyc<strong>in</strong>, Doryx, Adoxa<br />
M<strong>in</strong>ocycl<strong>in</strong>e<br />
Dynac<strong>in</strong>, M<strong>in</strong>oc<strong>in</strong>, Solodyn<br />
Systemic ret<strong>in</strong>oid Isotret<strong>in</strong>o<strong>in</strong> Accutane, Amnesteem, Sotret, Claravis, Absorica<br />
Source: Drugs@FDA (http://www.accessdata.fda.gov/scripts/cder/drugsatfda/)<br />
+ Pregnancy category C; *Pregnancy category X<br />
isotret<strong>in</strong>o<strong>in</strong> made fewer attempts dur<strong>in</strong>g treatment than those<br />
whose behavior started dur<strong>in</strong>g treatment. 31 In review<strong>in</strong>g the<br />
literature, there is no direct evidence show<strong>in</strong>g a clear l<strong>in</strong>k between<br />
isotret<strong>in</strong>o<strong>in</strong> and <strong>in</strong>creased suicidality.<br />
See Table 1 above for list of medications commonly used<br />
to treat acne. 36<br />
Procedural <strong>Treatment</strong> Options<br />
Epidemiologic data shows the vast majority of acne and<br />
rosacea patients are treated with topical and oral medications.<br />
<strong>The</strong>re is a grow<strong>in</strong>g body of literature to support procedural<br />
treatments as adjunctive therapy <strong>in</strong> these conditions. Photodynamic<br />
therapy (PDT) uses a comb<strong>in</strong>ation of a photosensitizer<br />
and UV light to produce reactive oxygen species, which<br />
target specific cells. P. acnes produce protophorphyr<strong>in</strong> IX and<br />
coproporphyr<strong>in</strong> III with<strong>in</strong> sebaceous glands, act<strong>in</strong>g as an endogenous<br />
photosensitizer.<br />
Exposure to certa<strong>in</strong> light wavelengths causes destruction of<br />
P. acnes with resolution of <strong>in</strong>flammatory acne lesions. Peak absorption<br />
of porphyr<strong>in</strong>s occurs <strong>in</strong> the blue light spectrum (415<br />
nm) and red light spectrum (630 nm). Both blue and red light<br />
have been studied <strong>in</strong> treatment of acne and both have demonstrated<br />
significant improvement. 37 Multiple studies have<br />
exam<strong>in</strong>ed the use of exogenous 5-am<strong>in</strong>olevul<strong>in</strong>ic acid (ALA)<br />
as a photosensitizer followed by laser treatment for acne. One<br />
study showed us<strong>in</strong>g ALA prior to <strong>in</strong>tense pulsed light (IPL)<br />
laser was more effective than IPL alone for acne lesions.<br />
Other studies show that relatively short <strong>in</strong>cubation with ALA<br />
(15 to 60 m<strong>in</strong>utes) followed by blue light is also an effective acne<br />
treatment. Other procedures use lasers, which directly destroy<br />
sebaceous glands for acne and rosacea. <strong>The</strong>se lasers are near<strong>in</strong>frared<br />
lasers with spectra between 1300 and 1600 nm. One<br />
study us<strong>in</strong>g an <strong>in</strong>frared laser showed 98% reduction of <strong>in</strong>flammatory<br />
acne lesions after four treatments. Diode lasers (810-900<br />
nm) have also shown to effectively destroy sebaceous glands. 37<br />
IPL effectively treats telangiectasias and flush<strong>in</strong>g seen <strong>in</strong> erythematotelangiectatic<br />
rosacea. 38 Phymatous rosacea can be difficult<br />
to treat us<strong>in</strong>g topical and oral medications. Many patients can<br />
benefit from ablative laser resurfac<strong>in</strong>g with Erb:YAG or carbon<br />
dioxide laser. Salicylic acid peels, glycolic acid peels and microdermabrasion<br />
have all been published as treatments for acne, although<br />
there are few randomized studies or studies compar<strong>in</strong>g<br />
these treatments to topical acne medications. 39-42<br />
Conclusion<br />
Acne and rosacea are common dermatologic conditions that<br />
have a major psychosocial impact on patients. Over the past several<br />
decades, new research has helped elucidate pathogenic factors<br />
important <strong>in</strong> these conditions, although the exact pathogenesis<br />
rema<strong>in</strong>s unknown. 43,44 First-l<strong>in</strong>e treatment for both conditions<br />
<strong>in</strong>volves the use of topical and oral medications. Often, topical<br />
and oral medications used <strong>in</strong> comb<strong>in</strong>ation achieve better, more<br />
rapid lesion clearance. Topical ret<strong>in</strong>oids, antibiotics and many<br />
other compounds like benzoyl peroxide, salicylic acid, azelaic acid<br />
and sulfur sulfacetamide have proven efficacious. Oral antibiotics,<br />
particulary tetracycl<strong>in</strong>es, can be used at antimicrobial doses for<br />
acne and at sub-antimicrobial doses for rosacea. Careful thought<br />
needs to be given to the treatment duration with oral antibiot-<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 13
<strong>Current</strong> <strong>Treatment</strong> Options For Acne Vulgaris And Acne Rosacea<br />
ics to prevent P. acnes resistance. For severe acne, oral isotret<strong>in</strong>o<strong>in</strong><br />
rema<strong>in</strong>s an excellent treatment option but requires careful discussion<br />
of toxicity and meticulous follow-up. Procedural treatments<br />
are a grow<strong>in</strong>g trend <strong>in</strong> the management of acne and rosacea, with<br />
photodynamic therapy and lasers target<strong>in</strong>g vessels and sebaceous<br />
glands show<strong>in</strong>g significant efficacy. Knowledge of all the different<br />
treatment options for acne and rosacea allows the provider to tailor<br />
each <strong>in</strong>dividual’s treatment regimen and to provide significant<br />
improvement <strong>in</strong> these disease entities. n<br />
Dr. Strowd is with the department of dermatology at Wake Forest<br />
University School of Medic<strong>in</strong>e <strong>in</strong> W<strong>in</strong>ston-Salem, NC.<br />
Disclosure: Dr. Strowd does not have any <strong>in</strong>dustry relationships<br />
or f<strong>in</strong>ancial conflicts of <strong>in</strong>terest to disclose.<br />
References<br />
1. Thomas DR. Psychosocial effects of acne. J Cutan Med Surg. 2004;8 Suppl 4:3-5.<br />
2. Mays RM, Gordon RA, Wilson JM, Silapunt S. New antibiotic therapies<br />
for acne and rosacea. Dermatol <strong>The</strong>r. 2012 Jan-Feb; 25(1):23-37.<br />
3. Kim GK, Del Rosso JQ. Oral spironolactone <strong>in</strong> post-teenage female patients<br />
with acne vulgaris: Practical considerations for the cl<strong>in</strong>ical based on<br />
current data and cl<strong>in</strong>ical experience. J Cl<strong>in</strong> Aesthet Dermatol. 2012 March;<br />
5(3):37-50.<br />
4. Bolognia JL, Jorizzo JL, Rap<strong>in</strong>i RP eds. <strong>Dermatology</strong> 2nd Edition, Elsivier,<br />
England; Chapter 37: Acne Vulgaris, p. 495-508.<br />
5. Forton FM. Papulopustular rosacea, sk<strong>in</strong> immunity and Demodex: pityriasis<br />
folliculorum as a miss<strong>in</strong>g l<strong>in</strong>k. J Eur Acad Dermatol Venereol. 2012 Jan;<br />
26(1):19-28.<br />
6. Bolognia J, Jorizzo JL, Rap<strong>in</strong>i RP eds. <strong>Dermatology</strong> 2nd Edition, Elsivier,<br />
England; Chapter 38: Rosacea and Related Disorders, p. 509-516.<br />
7. Emer J, Waldorf H, Berson D. Botanicals and anti-<strong>in</strong>flammatories: natural<br />
<strong>in</strong>gredients for rosacea. Sem<strong>in</strong> Cutan Med Surg. 2011 Sep; 30(3):148-155.<br />
8. Van Zuuren EJ, Kramer SF, Carter BR, Graber MA, Fedorowicz Z. Effective<br />
and evidence-based management strategies for rosacea: Summary of a<br />
Cochrane systematic review. Br J Dermatol. 2011 Oct; 165(4):760-781.<br />
9. Stotland M, Shalita AR, Kissl<strong>in</strong>g RF. Dapsone 5% gel: A review of its<br />
efficacy and safety <strong>in</strong> the treatment of acne vulgaris. Am J Cl<strong>in</strong> Dermatol.<br />
2009;10(4):221-227.<br />
10. Kircik LH. Synergy and its cl<strong>in</strong>ical relevance <strong>in</strong> topical acne therapy. J Cl<strong>in</strong><br />
Aesthet Dermatol. 2011 Nov; 4(11): 30-33.<br />
11. Goh CL, Tang MB, Briantais P, Kaoukhov A, Soto P. Adapalene gel 0.1%<br />
is better tolerated than tret<strong>in</strong>o<strong>in</strong> gel 0.025% among healthy volunteers of<br />
various ethnic orig<strong>in</strong>s. J Dermatol Treat. 2009;20(5):282-288.<br />
12. Jarrat MT, Brundage T. Efficacy and safety of cl<strong>in</strong>damyc<strong>in</strong>-tret<strong>in</strong>o<strong>in</strong> gel<br />
versus cl<strong>in</strong>damyc<strong>in</strong> or tret<strong>in</strong>o<strong>in</strong> alne <strong>in</strong> acne vulgaris: a randomized, doublebl<strong>in</strong>d,<br />
vehicle-controlled study. J Drugs Dermatol. 2012 Mar;11(3):318-326.<br />
13. Del Rosso JO, Harper J, Pillai R, Moore R. Tret<strong>in</strong>o<strong>in</strong> photostability: comparison<br />
of micronized tret<strong>in</strong>o<strong>in</strong> (0.05%) gel and tret<strong>in</strong>o<strong>in</strong> (0.025%) gel follow<strong>in</strong>g<br />
exposure to ultraviolet a light. J Cl<strong>in</strong> Aesthet Dermatol. 2012 Jan; 5(1):27-29.<br />
14. Lucky AW, Sugarman J. Comparison of micronized tret<strong>in</strong>o<strong>in</strong> gel 0.05%<br />
and tret<strong>in</strong>o<strong>in</strong> gel microsphere 0.1% <strong>in</strong> young adolescents with acne: a post<br />
hoc analysis of efficacy and tolerability data. Cutis 2011 Jun; 87(6):305-310.<br />
15. Thiboutot D, Arsonnaud S, Soto P. Efficacy and tolerability of adapalene<br />
0.3% gel compared to tazarotene 0.1% gel <strong>in</strong> the treatment of acne vulgaris.<br />
J Drugs Dermatol. 2008 Jun;7(6 Suppl):s3-10.<br />
16. Kakita L. Tazarotene versus tret<strong>in</strong>o<strong>in</strong> or adapalene <strong>in</strong> the treatment of acne<br />
vulgaris. J Am Acad Dermatol. 2000 Aug;43(2 Pt 3):S51-54.<br />
17. Parodi A, Drago F, Paol<strong>in</strong>o S, Cozzani E, Gallo R. <strong>Treatment</strong> of rosacea.<br />
Ann Dermatol Venereol. 2011 Nov;138 Suppl 3:S211-4.<br />
18. Chang AL, Alora-Palli M, Lima XT, et al. A randomized, double-bl<strong>in</strong>d,<br />
placebo-controlled, pilot study to assess the efficacy and safety of cl<strong>in</strong>damyc<strong>in</strong><br />
1.2% and tret<strong>in</strong>o<strong>in</strong> 0.025% comb<strong>in</strong>ation gel for the treatment of acne rosacea<br />
over 12 weeks. J Drugs Dermatol. 2012 Mar; 11(3):333-339.<br />
19. Oztürkcan S, Ermertcan AT, Sah<strong>in</strong> MT, Afşar FS. Efficiency of benzoyl<br />
peroxide-erythromyc<strong>in</strong> gel <strong>in</strong> comparison with metronidazole gel <strong>in</strong> the<br />
treatment of acne rosacea. J Dermatol. 2004 Aug;31(8):610-617.<br />
20. Seidler EM, Kimball AB. Meta-analysis compar<strong>in</strong>g efficacy of benzoyl peroxide,<br />
cl<strong>in</strong>damyc<strong>in</strong>, benzoyl peroxide with salicylic acid, and comb<strong>in</strong>ation benzoyl<br />
peroxide/cl<strong>in</strong>damyc<strong>in</strong> <strong>in</strong> acne. J Am Acad Dermatol. 2010 Jul;63(1):52-62.<br />
21. Van Scott EJ, Yu RJ. Hyperkerat<strong>in</strong>ization, corneocyte cohesion, and alpha<br />
hydroxyacids. J Am Acad Dermatol. 1984 Nov; 11(5): 867–879.<br />
22. Waller JM, Dreher F, Behnam S, et al. ‘Keratolytic’ properties of benzoyl<br />
peroxide and ret<strong>in</strong>oic acid resemble salicylic acid <strong>in</strong> man. Sk<strong>in</strong> Pharmacol<br />
Physiol. 2006;19(5):283–289.<br />
23. Cunliffe WJ, Holland KT, Bojar R, Levy SF. A randomized, double-bl<strong>in</strong>d<br />
comparison of a cl<strong>in</strong>damyc<strong>in</strong> phosphate/benzoyl peroxide gel formulation and a<br />
match<strong>in</strong>g cl<strong>in</strong>damyc<strong>in</strong> gel with respect to microbiologic activity and cl<strong>in</strong>ical efficacy<br />
<strong>in</strong> the topical treatment of acne vulgaris. Cl<strong>in</strong> <strong>The</strong>r. 2002;24(7):1117–1133.<br />
24. Dub<strong>in</strong>a MI, Fleischer AB. Interaction of topical sulfacetamide and topical<br />
dapsone with benzoyl peroxide. Arch Dermatol. 2009;145(9):1027-1029.<br />
25. Mastrofrancesco A, Ottaviani M, Aspite N, et al. Azelaic acid modulates<br />
the <strong>in</strong>flammatory response <strong>in</strong> normal human kerat<strong>in</strong>ocytes through PPARgamma<br />
activation. Exp Dermatol. 2010 Sep;19(9):813-820.<br />
26. Del Rosso JQ. <strong>The</strong> use of sodium sulfacetamide 10%-sulfur 5% emollient<br />
foam <strong>in</strong> the treatment of acne vulgaris. J Cl<strong>in</strong> Aesthet Dermatol. 2009<br />
August; 2(8):26-29.<br />
27. Draelos ZD. <strong>The</strong> multifunctionality of 10% sodium sulfacetamide, 5%<br />
sulfur emollient foam <strong>in</strong> the treatment of <strong>in</strong>flammatory facial dermatoses. J<br />
Drugs Dermatol. 2010 Mar;9(3):234-236.<br />
28. Trumbore MW, Goldste<strong>in</strong> JA, Gurge RM. <strong>Treatment</strong> of papulopustular<br />
rosacea with sodium sulfacetamide 10%/sulfer 5% emollient foam. J Drugs<br />
Dermatol. 2009 Mar;8(3):299-304.<br />
29. Kim MB, Kim GW, Park HJ, et al. Pimecrolimus 1% cream for the treatment<br />
of rosacea. J Dermatol. 2011 Dec;38(12):1135-1139.<br />
30. Teraki Y, Hitomi K, Sato U et al. Tacrolimus-<strong>in</strong>duced rosacea-like dermatitis:<br />
A cl<strong>in</strong>ical analysis of 16 cases associated with tacrolimus o<strong>in</strong>tment<br />
application. <strong>Dermatology</strong>. 2012 May 22. (Epub ahead of pr<strong>in</strong>t).<br />
31. Gamble R, Dunn J, Dawson A, et al. Topical antimicrobial treatment of acne<br />
vulgaris: an evidence-based review. Am J Cl<strong>in</strong> Dermatol. 2012 Jun 1; 13(3):141-52.<br />
32. Kort<strong>in</strong>g HC, Schöllmann C. <strong>Current</strong> topical and systemic approaches to<br />
treatment of rosacea. J Eur Acad Dermatol Venereol. 2009 Aug; 23(8):876-882.<br />
33. Simpson RC, Gr<strong>in</strong>dlay DJ, Williams HC. What’s new <strong>in</strong> acne An analysis<br />
of systematic reviews and cl<strong>in</strong>ically significant trials published <strong>in</strong> 2010-2011.<br />
Cl<strong>in</strong> Exp Dermatol. 2011 Dec; 36(8):840-843.<br />
34. Leyden JJ, Preston N, Osborn C, Gottschalk AR. In-vivo effectiveness of<br />
adapalene 0.1%/benzoyl peroxide 2.5% gel on antibiotic-sensitive and resistant<br />
Propionibacterium acnes. J Cl<strong>in</strong> Aesthet Dermatol. 2011 May; 4(5):22-26.<br />
35. Schnopp C, Mempel M. Acne vulgaris <strong>in</strong> children and adolescents. M<strong>in</strong>erva<br />
Pediatr. 2011 Aug;63(4):293-304.<br />
36. Ho B, Friedlander SF. Develop<strong>in</strong>g an acne treatment plan for pediatric<br />
and adolescent patients. Derm for the Pediatrician. 2012 Aug;1(2):19-25.<br />
37. Gold MH. Acne and PDT: new techniques with lasers and light sources.<br />
Lasers Med Sci. 2007 Jun; 22(2):67-72.<br />
38. Bikowski JB, Goldman MP. Rosacea: where are we now J Drugs Dermatol.<br />
2004 May-Jun; 3(3):251-261.<br />
39. Garg VK, S<strong>in</strong>ha S, Sarkar R. Glycolic acid peels versus salicylic-mandelic<br />
acid peels <strong>in</strong> active acne vulgaris and post-acnescarr<strong>in</strong>g and hyperpigmentation:<br />
a comparative study. Dermatol Surg. 2009 Jan;35(1):59-65.<br />
40. Lee SH, Huh CH, Park KC, Youn SW. Effects of repetitive superficial<br />
chemical peels on facial sebum secretion <strong>in</strong> acne patients. J Eur Acad Dermatol<br />
Venereol. 2006 Sep;20(8):964-968.<br />
41. Kempiak SJ, Uebelhoer N. Superficial chemical peels and microdermabrasion<br />
for acne vulgaris. Sem<strong>in</strong> Cutan Med Surg. 2008 Sep;27(3):212-220.<br />
42. Dréno B, Fischer TC, Peros<strong>in</strong>o E, et al. Expert op<strong>in</strong>ion: efficacy of superficial<br />
chemical peels <strong>in</strong> active acne management--what can we learn from<br />
the literature today Evidence-based recommendations. J Eur Acad Dermatol<br />
Venereol. 2011 Jun;25(6):695-704.<br />
43. Fleischer AB Jr. Inflammation <strong>in</strong> rosacea and acne: Implications for patient<br />
care. J Drugs Dermatol. 2011 Jun;10(6):614-620.<br />
44. Yamasaki K, Gallo RL. Rosacea as a disease of cathelicid<strong>in</strong>s and sk<strong>in</strong> <strong>in</strong>nate<br />
immunity. J Investig Dermatol Symp Proc. 2011 Dec;15(1):12-15.<br />
14 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>The</strong> <strong>The</strong>rapeutic<br />
Approach to Psoriasis<br />
Recent research has shown the role that the immune system plays <strong>in</strong> the pathogenesis of this disease,<br />
which may lead to the development of immune-specific therapies. This article highlights current approaches<br />
<strong>in</strong> treat<strong>in</strong>g and manag<strong>in</strong>g patients with psoriasis.<br />
Alyssa S. Daniel, MD<br />
Figure 1. Cl<strong>in</strong>ical view of plaque-type psoriasis with well-demarcated plaques and overly<strong>in</strong>g adherent scale.<br />
Psoriasis is a chronic, immune mediated, <strong>in</strong>flammatory<br />
sk<strong>in</strong> condition with a genetic susceptibility pattern<br />
and several environmental triggers. It is characterized<br />
by the hyperproliferation of kerat<strong>in</strong>ocytes, dilation of<br />
blood vessels and an <strong>in</strong>flammatory <strong>in</strong>filtrate, all of which are<br />
potential targets for treatment. Psoriasis is associated with<br />
key comorbidities <strong>in</strong>clud<strong>in</strong>g cardiovascular disease, metabolic<br />
dysfunction, depression and psoriatic arthritis. 1 <strong>The</strong>re has<br />
been a great deal of research recently to elucidate the role<br />
that the immune system plays <strong>in</strong> the pathogenesis of this disease<br />
and to develop immune-specific therapies. This article<br />
will highlight current approaches <strong>in</strong> treat<strong>in</strong>g and manag<strong>in</strong>g<br />
patients with psoriasis.<br />
Epidemiology<br />
<strong>The</strong> prevalence of psoriasis was most recently approximated<br />
to affect around 3% of the US population. 2 This figure varies<br />
considerably worldwide. In certa<strong>in</strong> Asian, African, African-<br />
American and Norwegian Lapp populations, the prevalence<br />
may be much lower. 3 Psoriasis has a bimodal age distribution<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 15
<strong>The</strong> <strong>The</strong>rapeutic Approach to Psoriasis<br />
Figure 2. Histology of psoriasis.<br />
with a peak <strong>in</strong> the 2nd and 6th decades of life. 3-7 Three quarters<br />
of new cases occur before the age of 40. 7 <strong>The</strong> prevalence<br />
of the disease appears to be equal among women and men.<br />
Early childhood psoriasis is relatively rare but there are reported<br />
cases of even <strong>in</strong>fantile psoriasis. 8<br />
Psoriasis is a polygenetic disorder. Approximately 70% of<br />
children with psoriasis have a positive family history. 9 Many<br />
gene l<strong>in</strong>kage studies and more recent genome-wide association<br />
studies have identified at least n<strong>in</strong>e gene loci that are<br />
associated with a higher risk for develop<strong>in</strong>g psoriasis. <strong>The</strong>se<br />
are designated PSORS1-PSORS9. 10-20 <strong>The</strong> natural history of<br />
psoriasis is variable, usually chronic with <strong>in</strong>termittent flares. 21<br />
Pathogenesis<br />
<strong>The</strong> underly<strong>in</strong>g etiology of psoriasis is still at the center<br />
of heated debates. Prior to the 1980s, psoriasis was regarded<br />
as a disease of epidermal dysfunction with several epidermal<br />
mediators be<strong>in</strong>g at the center of the pathogenesis, <strong>in</strong>clud<strong>in</strong>g<br />
cyclic AMP, eicosanoids, prote<strong>in</strong> k<strong>in</strong>ase C, phospholipase C,<br />
polyam<strong>in</strong>es and transform<strong>in</strong>g growth factor (TGF)-α. 22 More<br />
recently, the pathogenesis has been clearly related, <strong>in</strong> some part,<br />
to T-cell immune dysfunction. Studies look<strong>in</strong>g at the association<br />
between psoriasis and major histocompatibility complex<br />
(MHC) alleles and disease improvement with therapies that<br />
affect T-cell function make it apparent that T cells likely play a<br />
direct role. 23,24 Additional support for this correlation <strong>in</strong>clude<br />
animal models show<strong>in</strong>g that xenograft transplantation of un<strong>in</strong>volved<br />
human psoriatic sk<strong>in</strong> can <strong>in</strong>duce psoriatic lesions on<br />
immunodeficient mice when given the donors’ activated T<br />
cells. 25 Barrier ma<strong>in</strong>tenance may be a contribut<strong>in</strong>g factor <strong>in</strong><br />
the pathogenesis as well. 26<br />
Cl<strong>in</strong>ical Implications<br />
Psoriasis is a papulosquamous sk<strong>in</strong> condition with hallmark<br />
erythematous, well-demarcated, silver-scal<strong>in</strong>g papules and<br />
plaques. <strong>The</strong>se plaques can localize to sights of trauma, a cl<strong>in</strong>ical<br />
f<strong>in</strong>d<strong>in</strong>g referred to as the Koebner phenomenon. 27 <strong>The</strong>re<br />
are several cl<strong>in</strong>ical variants, <strong>in</strong>clud<strong>in</strong>g chronic plaque, guttate,<br />
erythrodermic, pustular and <strong>in</strong>verse psoriasis. Locations such<br />
as the scalp, nails and tongue, also known as annulus migrans,<br />
can also be affected by psoriasis.<br />
Comorbidities are frequently seen at <strong>in</strong>creased rates <strong>in</strong><br />
psoriatic patients compared to the general population. <strong>The</strong>se<br />
patients have higher rates of hypertension, left ventricular hypertrophy,<br />
obesity and diabetes. <strong>The</strong>y also are more likely to<br />
engage <strong>in</strong> risky behaviors such as smok<strong>in</strong>g and alcohol use. 28<br />
Psoriatic arthritis is also a complication. Approximately<br />
one-third of patients with psoriasis will also develop pso-<br />
16 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>The</strong> <strong>The</strong>rapeutic Approach to Psoriasis<br />
Biologics for Psoriasis: A Review of Recent Research and News<br />
recent observational study, published onl<strong>in</strong>e ahead of pr<strong>in</strong>t <strong>in</strong> the Journal of Dermatologic <strong>Treatment</strong>, compared<br />
A cl<strong>in</strong>ical improvement and treatment satisfaction with biologic versus other therapies <strong>in</strong> patients with plaque psoriasis.<br />
A group of European dermatologists reported disease severity before and after start<strong>in</strong>g current therapy; dermatologists<br />
and patients reported treatment satisfaction. Of 2,151 patients, 453 were undergo<strong>in</strong>g treatment with topicals, 666 with<br />
phototherapy, 683 with conventional systemic therapies and 349 with biologics. A significantly greater improvement <strong>in</strong><br />
disease severity was observed <strong>in</strong> the biologics group (70% before to 15% after treatment) compared to topicals (22%<br />
to 10%), phototherapy (20% to 11%) and conventional systemic therapy (49% to 15%) (all P≤0.03). A greater number<br />
of patients and dermatologists also reported greater satisfaction with biologic therapy over other therapies. Significantly<br />
more patients (59%) receiv<strong>in</strong>g biologics were satisfied with treatment versus topicals (45%), phototherapy (34%), or conventional<br />
systemic treatment (50%) (all P
<strong>The</strong> <strong>The</strong>rapeutic Approach to Psoriasis<br />
riatic arthritis. 29 This usually presents after sk<strong>in</strong> lesions are<br />
first seen, but, <strong>in</strong> a m<strong>in</strong>ority of patients, the arthritis precedes<br />
the sk<strong>in</strong> lesions. <strong>The</strong> most common presentation is that of a<br />
mono- and asymmetric oligoarthritis lead<strong>in</strong>g to the classic<br />
sausage digit deformity. 30<br />
Topical <strong>The</strong>rapies<br />
Vitam<strong>in</strong> D Analogues<br />
Topical vitam<strong>in</strong> D3 analogues were first <strong>in</strong>troduced <strong>in</strong><br />
the 1990s. <strong>The</strong> mechanism of action is not entirely understood,<br />
but they seem to affect the proliferation and<br />
differentiation of kerat<strong>in</strong>ocytes and have immunomodulat<strong>in</strong>g<br />
effects as well. <strong>The</strong>y may also <strong>in</strong>duce apoptosis of<br />
psoriatic kerat<strong>in</strong>ocytes. 31<br />
Most studies of topical D3 have exam<strong>in</strong>ed patients with<br />
chronic plaque psoriasis, but there should be caution <strong>in</strong> us<strong>in</strong>g<br />
this <strong>in</strong> patients who have extensive body surface area<br />
<strong>in</strong>volvement, as there is an <strong>in</strong>creased risk of hypercalcemia<br />
and hypercalciuria. Otherwise, the medication is safe and<br />
well tolerated (although there may be some irritation) and<br />
should be considered first l<strong>in</strong>e <strong>in</strong> most patients with mild to<br />
moderate plaque psoriasis. 32 A systematic review that aimed<br />
A review of the literature<br />
on the efficacy of clobetasol<br />
propionate o<strong>in</strong>tment<br />
compared to other clobetasol<br />
preparations found no<br />
difference <strong>in</strong> efficacy<br />
rates among the different<br />
formulations.<br />
to provide evidence-based recommendations about the use<br />
of vitam<strong>in</strong> D analogues found them to be a cost effective,<br />
safe treatment, but efficacy is <strong>in</strong>creased nearly twice as much<br />
when topical corticosteroids were added as concomitant<br />
therapies. 33 Calcipotriol/calcipotriene is available <strong>in</strong> the<br />
United States <strong>in</strong> cream, o<strong>in</strong>tment, foam and solution forms.<br />
Calcitriol o<strong>in</strong>tment is available <strong>in</strong> the United States, while<br />
tacalcitol and calcitriol are available <strong>in</strong> Europe and may be<br />
more potent than calcipotriol/calcipotriene. Calcipotriol/<br />
calcipotriene is typically used twice daily at the concentration<br />
of 50 μg/g. Most studies with calcipotriol have limited<br />
the use to no more than 100 grams/week to protect aga<strong>in</strong>st<br />
side effects. It is pregnancy category C.<br />
Topical Steroids<br />
Topical corticosteroids are among the oldest treatments<br />
available for psoriasis. Corticosteroids b<strong>in</strong>d to the cytoplasmic<br />
corticosteroid receptor and translocate <strong>in</strong>to the nucleus; this<br />
downstream effect <strong>in</strong>hibits transcription of key genes needed<br />
to promote the <strong>in</strong>flammatory response. Corticosteroids also<br />
act to <strong>in</strong>hibit proliferation and promote vasoconstriction. 34<br />
A systematic review exam<strong>in</strong>ed 51 randomized controlled<br />
trials of mild to severe chronic plaque psoriasis where topical<br />
corticosteroids were used as the <strong>in</strong>itial treatment. Most treatment<br />
time for studies was 4 weeks. <strong>The</strong> results were highly<br />
variable, with 30% to 90% of patients show<strong>in</strong>g at least 50%<br />
<strong>in</strong>itial improvement for mild to severe psoriasis, 7% to 85%<br />
achiev<strong>in</strong>g at least 75% improvement and 55% to 85% experienc<strong>in</strong>g<br />
at least 90% improvement. Occlusive measures were<br />
associated with better response, and <strong>in</strong>termittent ma<strong>in</strong>tenance<br />
therapy appeared to provide longer remission times. 35<br />
More potent topical steroids are be<strong>in</strong>g used than <strong>in</strong> the<br />
past, 36 although it’s not clear if higher potency steroids are<br />
actually more effective. One study estimated that the effective<br />
concentrations <strong>in</strong> the sk<strong>in</strong> of hydrocortisone 2.5% o<strong>in</strong>tment,<br />
triamc<strong>in</strong>olone 0.1% o<strong>in</strong>tment, clobetasol 0.05% foam and betamethasone<br />
0.1% cream to oral prednisone. Hydrocortisone<br />
2.5% o<strong>in</strong>tment, triamc<strong>in</strong>olone 0.1% o<strong>in</strong>tment and clobetasol<br />
0.05% foam were predicted to provide greater levels of potency<br />
<strong>in</strong> the sk<strong>in</strong> <strong>in</strong> comparison to oral prednisone. 37<br />
<strong>The</strong>re are a wide variety of formulations of topical corticosteroids,<br />
<strong>in</strong>clud<strong>in</strong>g o<strong>in</strong>tments, creams, solutions, foams, gels<br />
and sprays. It was once common practice to choose the o<strong>in</strong>tment<br />
formulation, as it was thought to be more potent and,<br />
thus, more efficacious. A review of the literature on the efficacy<br />
of clobetasol propionate o<strong>in</strong>tment compared to other<br />
clobetasol preparations found no difference <strong>in</strong> efficacy rates<br />
among the different formulations. <strong>The</strong> authors concluded that<br />
patient preference should be forefront <strong>in</strong> decision mak<strong>in</strong>g<br />
because, ultimately, patient compliance with the formulation<br />
that is chosen will largely dictate how effective treatment is. 38<br />
<strong>The</strong> side effects of topical steroid therapy <strong>in</strong>clude sk<strong>in</strong><br />
atrophy, telangiectasias, easy bruis<strong>in</strong>g, acneiform eruptions,<br />
<strong>in</strong>creased risk for sk<strong>in</strong> <strong>in</strong>fections and allergic contact dermatitis.<br />
<strong>The</strong>re has been much debate about the risks of suppression<br />
of the hypothalamic-pituitary-adrenal axis. 38,39 In a<br />
recent review on the risk for adrenal suppression and sk<strong>in</strong><br />
atrophy by Castela et al, higher-potency steroids were associated<br />
with measurable decreased levels of morn<strong>in</strong>g cortisol<br />
levels, thus suggest<strong>in</strong>g adrenal suppression; however, none<br />
of these measurable cases had any cl<strong>in</strong>ical manifestations of<br />
adrenal suppression. With once-daily application of topical<br />
steroids, the <strong>in</strong>cidence of sk<strong>in</strong> atrophy was 1.9%. 40 Topical<br />
steroids are pregnancy category C.<br />
Topical Ret<strong>in</strong>oids<br />
Ret<strong>in</strong>oids are vitam<strong>in</strong> A derivative hormones. Ret<strong>in</strong>oids<br />
decrease epidermal proliferation and reduce <strong>in</strong>flammation.<br />
<strong>The</strong> only topical ret<strong>in</strong>oid approved for psoriasis is tazarotene;<br />
18 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
Brief Summary of Prescrib<strong>in</strong>g Information for STELARA ® (ustek<strong>in</strong>umab)<br />
STELARA ® Injection, for subcutaneous use<br />
See package <strong>in</strong>sert for Full Prescrib<strong>in</strong>g Information<br />
INDICATIONS AND USAGE: STELARA ® is <strong>in</strong>dicated for the treatment of adult<br />
patients (18 years or older) with moderate to severe plaque psoriasis who are<br />
candidates for phototherapy or systemic therapy. CONTRAINDICATIONS:<br />
Cl<strong>in</strong>ically significant hypersensitivity to ustek<strong>in</strong>umab or to any of the excipients<br />
(see Warn<strong>in</strong>gs and Precautions). WARNINGS AND PRECAUTIONS: Infections<br />
STELARA ® may <strong>in</strong>crease the risk of <strong>in</strong>fections and reactivation of latent<br />
<strong>in</strong>fections. Serious bacterial, fungal, and viral <strong>in</strong>fections were observed <strong>in</strong><br />
subjects receiv<strong>in</strong>g STELARA ® (see Adverse Reactions). STELARA ® should not be<br />
given to patients with any cl<strong>in</strong>ically important active <strong>in</strong>fection. STELARA ® should<br />
not be adm<strong>in</strong>istered until the <strong>in</strong>fection resolves or is adequately treated. Instruct<br />
patients to seek medical advice if signs or symptoms suggestive of an <strong>in</strong>fection<br />
occur. Exercise caution when consider<strong>in</strong>g the use of STELARA ® <strong>in</strong> patients with<br />
a chronic <strong>in</strong>fection or a history of recurrent <strong>in</strong>fection. Serious <strong>in</strong>fections requir<strong>in</strong>g<br />
hospitalization occurred <strong>in</strong> the psoriasis development program. <strong>The</strong>se serious<br />
<strong>in</strong>fections <strong>in</strong>cluded cellulitis, diverticulitis, osteomyelitis, viral <strong>in</strong>fections,<br />
gastroenteritis, pneumonia, and ur<strong>in</strong>ary tract <strong>in</strong>fections. <strong>The</strong>oretical Risk for<br />
Vulnerability to Particular Infections Individuals genetically deficient <strong>in</strong> IL-12/<br />
IL-23 are particularly vulnerable to dissem<strong>in</strong>ated <strong>in</strong>fections from mycobacteria<br />
(<strong>in</strong>clud<strong>in</strong>g nontuberculous, environmental mycobacteria), salmonella (<strong>in</strong>clud<strong>in</strong>g<br />
nontyphi stra<strong>in</strong>s), and Bacillus Calmette-Guer<strong>in</strong> (BCG) vacc<strong>in</strong>ations. Serious<br />
<strong>in</strong>fections and fatal outcomes have been reported <strong>in</strong> such patients. It is not<br />
known whether patients with pharmacologic blockade of IL-12/IL-23 from<br />
treatment with STELARA ® will be susceptible to these types of <strong>in</strong>fections.<br />
Appropriate diagnostic test<strong>in</strong>g should be considered, e.g., tissue culture, stool<br />
culture, as dictated by cl<strong>in</strong>ical circumstances. Pre-treatment Evaluation for<br />
Tuberculosis Evaluate patients for tuberculosis <strong>in</strong>fection prior to <strong>in</strong>itiat<strong>in</strong>g<br />
treatment with STELARA ® . Do not adm<strong>in</strong>ister STELARA ® to patients with active<br />
tuberculosis. Initiate treatment of latent tuberculosis prior to adm<strong>in</strong>ister<strong>in</strong>g<br />
STELARA ® . Consider anti-tuberculosis therapy prior to <strong>in</strong>itiation of STELARA ® <strong>in</strong><br />
patients with a past history of latent or active tuberculosis <strong>in</strong> whom an adequate<br />
course of treatment cannot be confirmed. Patients receiv<strong>in</strong>g STELARA ® should<br />
be monitored closely for signs and symptoms of active tuberculosis dur<strong>in</strong>g and<br />
after treatment. Malignancies STELARA ® is an immunosuppressant and may<br />
<strong>in</strong>crease the risk of malignancy. Malignancies were reported among subjects<br />
who received STELARA ® <strong>in</strong> cl<strong>in</strong>ical studies (see Adverse Reactions). In rodent<br />
models, <strong>in</strong>hibition of IL-12/IL-23p40 <strong>in</strong>creased the risk of malignancy (see<br />
Noncl<strong>in</strong>ical Toxicology). <strong>The</strong> safety of STELARA ® has not been evaluated <strong>in</strong><br />
patients who have a history of malignancy or who have a known malignancy.<br />
Hypersensitivity Reactions Hypersensitivity reactions, <strong>in</strong>clud<strong>in</strong>g anaphylaxis<br />
and angioedema, have been reported post-market<strong>in</strong>g. If an anaphylactic or other<br />
cl<strong>in</strong>ically significant hypersensitivity reaction occurs, discont<strong>in</strong>ue STELARA ®<br />
and <strong>in</strong>stitute appropriate therapy (see Adverse Reactions). Reversible<br />
Posterior Leukoencephalopathy Syndrome One case of reversible posterior<br />
leukoencephalopathy syndrome (RPLS) was observed dur<strong>in</strong>g the cl<strong>in</strong>ical<br />
development program which <strong>in</strong>cluded 3523 STELARA ® -treated subjects. <strong>The</strong><br />
subject, who had received 12 doses of STELARA ® over approximately two years,<br />
presented with headache, seizures and confusion. No additional STELARA ®<br />
<strong>in</strong>jections were adm<strong>in</strong>istered and the subject fully recovered with appropriate<br />
treatment. RPLS is a neurological disorder, which is not caused by demyel<strong>in</strong>ation<br />
or a known <strong>in</strong>fectious agent. RPLS can present with headache, seizures,<br />
confusion and visual disturbances. Conditions with which it has been associated<br />
<strong>in</strong>clude preeclampsia, eclampsia, acute hypertension, cytotoxic agents and<br />
immunosuppressive therapy. Fatal outcomes have been reported. If RPLS is<br />
suspected, STELARA ® should be discont<strong>in</strong>ued and appropriate treatment<br />
adm<strong>in</strong>istered. Immunizations Prior to <strong>in</strong>itiat<strong>in</strong>g therapy with STELARA ® , patients<br />
should receive all immunizations appropriate for age as recommended by<br />
current immunization guidel<strong>in</strong>es. Patients be<strong>in</strong>g treated with STELARA ® should<br />
not receive live vacc<strong>in</strong>es. BCG vacc<strong>in</strong>es should not be given dur<strong>in</strong>g treatment<br />
with STELARA ® or for one year prior to <strong>in</strong>itiat<strong>in</strong>g treatment or one year follow<strong>in</strong>g<br />
discont<strong>in</strong>uation of treatment. Caution is advised when adm<strong>in</strong>ister<strong>in</strong>g live<br />
vacc<strong>in</strong>es to household contacts of patients receiv<strong>in</strong>g STELARA ® because of the<br />
potential risk for shedd<strong>in</strong>g from the household contact and transmission to<br />
patient. Non-live vacc<strong>in</strong>ations received dur<strong>in</strong>g a course of STELARA ® may not<br />
elicit an immune response sufficient to prevent disease. Concomitant <strong>The</strong>rapies<br />
<strong>The</strong> safety of STELARA ® <strong>in</strong> comb<strong>in</strong>ation with other immunosuppressive agents<br />
or phototherapy has not been evaluated. Ultraviolet-<strong>in</strong>duced sk<strong>in</strong> cancers<br />
developed earlier and more frequently <strong>in</strong> mice genetically manipulated to be<br />
deficient <strong>in</strong> both IL-12 and IL-23 or IL-12 alone (see Noncl<strong>in</strong>ical Toxicology).<br />
ADVERSE REACTIONS: <strong>The</strong> follow<strong>in</strong>g serious adverse reactions are discussed<br />
elsewhere <strong>in</strong> the label: Infections (see Warn<strong>in</strong>gs and Precautions); Malignancies<br />
(see Warn<strong>in</strong>gs and Precautions); and RPLS (see Warn<strong>in</strong>gs and Precautions).<br />
Cl<strong>in</strong>ical Studies Experience Because cl<strong>in</strong>ical trials are conducted under widely<br />
vary<strong>in</strong>g conditions, adverse reaction rates observed <strong>in</strong> the cl<strong>in</strong>ical trials of a drug<br />
cannot be directly compared to rates <strong>in</strong> the cl<strong>in</strong>ical trials of another drug and may<br />
not reflect the rates observed <strong>in</strong> practice. <strong>The</strong> safety data reflect exposure to<br />
STELARA ® <strong>in</strong> 3117 psoriasis subjects, <strong>in</strong>clud<strong>in</strong>g 2414 exposed for at least<br />
STELARA ® (ustek<strong>in</strong>umab)<br />
6 months, 1852 exposed for at least one year,1650 exposed for at least two<br />
years, 1129 exposed for at least three years, and 619 exposed for at least four<br />
years. Adverse reactions listed below are those that occurred at a rate of at least<br />
1% and at a higher rate <strong>in</strong> the STELARA ® groups than the placebo group dur<strong>in</strong>g<br />
the placebo-controlled period of STUDY 1 and STUDY 2 (see Cl<strong>in</strong>ical Studies).<br />
<strong>The</strong> numbers (percentages) of adverse reactions reported for placebo-treated<br />
patients (n=665), patients treated with 45 mg STELARA ® (n=664), and patients<br />
treated with 90 mg STELARA ® (n=666), respectively, were: Nasopharyngitis: 51<br />
(8%), 56 (8%), 49 (7%); Upper respiratory tract <strong>in</strong>fection: 30 (5%), 36 (5%), 28<br />
(4%); Headache: 23 (3%), 33 (5%), 32 (5%); Fatigue: 14 (2%), 18 (3%), 17 (3%);<br />
Diarrhea: 12 (2%), 13 (2%), 13 (2%); Back pa<strong>in</strong>: 8 (1%), 9 (1%), 14 (2%);<br />
Dizz<strong>in</strong>ess: 8 (1%), 8 (1%), 14 (2%); Pharyngolaryngeal pa<strong>in</strong>: 7 (1%), 9 (1%), 12<br />
(2%); Pruritus: 9 (1%), 10 (2%), 9 (1%); Injection site erythema: 3 (
STELARA ® (ustek<strong>in</strong>umab)<br />
Allergen Immunotherapy STELARA ® has not been evaluated <strong>in</strong> patients who<br />
have undergone allergy immunotherapy. STELARA ® may decrease the protective<br />
effect of allergen immunotherapy (decrease tolerance) which may <strong>in</strong>crease the<br />
risk of an allergic reaction to a dose of allergen immunotherapy. <strong>The</strong>refore,<br />
caution should be exercised <strong>in</strong> patients receiv<strong>in</strong>g or who have received allergen<br />
immunotherapy, particularly for anaphylaxis. USE IN SPECIFIC POPULATIONS:<br />
Pregnancy Pregnancy Category B <strong>The</strong>re are no studies of STELARA ® <strong>in</strong> pregnant<br />
women. STELARA ® should be used dur<strong>in</strong>g pregnancy only if the potential benefit<br />
justifies the potential risk to the fetus. No teratogenic effects were observed <strong>in</strong><br />
the developmental and reproductive toxicology studies performed <strong>in</strong> cynomolgus<br />
monkeys at doses up to 45 mg/kg ustek<strong>in</strong>umab, which is 45 times (based on<br />
mg/kg) the highest <strong>in</strong>tended cl<strong>in</strong>ical dose <strong>in</strong> psoriasis patients (approximately<br />
1 mg/kg based on adm<strong>in</strong>istration of a 90 mg dose to a 90 kg psoriasis patient).<br />
Ustek<strong>in</strong>umab was tested <strong>in</strong> two embryo-fetal development toxicity studies.<br />
Pregnant cynomolgus monkeys were adm<strong>in</strong>istered ustek<strong>in</strong>umab at doses up to<br />
45 mg/kg dur<strong>in</strong>g the period of organogenesis either twice weekly via<br />
subcutaneous <strong>in</strong>jections or weekly by <strong>in</strong>travenous <strong>in</strong>jections. No significant<br />
adverse developmental effects were noted <strong>in</strong> either study. In an embryo-fetal<br />
development and pre- and post-natal development toxicity study, three groups<br />
of 20 pregnant cynomolgus monkeys were adm<strong>in</strong>istered subcutaneous doses of<br />
0, 22.5, or 45 mg/kg ustek<strong>in</strong>umab twice weekly from the beg<strong>in</strong>n<strong>in</strong>g of<br />
organogenesis <strong>in</strong> cynomolgus monkeys to Day 33 after delivery. <strong>The</strong>re were no<br />
treatment-related effects on mortality, cl<strong>in</strong>ical signs, body weight, food<br />
consumption, hematology, or serum biochemistry <strong>in</strong> dams. Fetal losses occurred<br />
<strong>in</strong> six control monkeys, six 22.5 mg/kg-treated monkeys, and five 45 mg/kgtreated<br />
monkeys. Neonatal deaths occurred <strong>in</strong> one 22.5 mg/kg-treated monkey<br />
and <strong>in</strong> one 45 mg/kg-treated monkey. No ustek<strong>in</strong>umab-related abnormalities<br />
were observed <strong>in</strong> the neonates from birth through six months of age <strong>in</strong> cl<strong>in</strong>ical<br />
signs, body weight, hematology, or serum biochemistry. <strong>The</strong>re were no<br />
treatment-related effects on functional development until wean<strong>in</strong>g, functional<br />
development after wean<strong>in</strong>g, morphological development, immunological<br />
development, and gross and histopathological exam<strong>in</strong>ations of offspr<strong>in</strong>gs by the<br />
age of 6 months. Nurs<strong>in</strong>g Mothers Caution should be exercised when STELARA ®<br />
is adm<strong>in</strong>istered to a nurs<strong>in</strong>g woman. <strong>The</strong> unknown risks to the <strong>in</strong>fant from<br />
gastro<strong>in</strong>test<strong>in</strong>al or systemic exposure to ustek<strong>in</strong>umab should be weighed aga<strong>in</strong>st<br />
the known benefits of breast-feed<strong>in</strong>g. Ustek<strong>in</strong>umab is excreted <strong>in</strong> the milk of<br />
lactat<strong>in</strong>g monkeys adm<strong>in</strong>istered ustek<strong>in</strong>umab. IgG is excreted <strong>in</strong> human milk, so<br />
it is expected that STELARA ® will be present <strong>in</strong> human milk. It is not known if<br />
ustek<strong>in</strong>umab is absorbed systemically after <strong>in</strong>gestion; however, published data<br />
suggest that antibodies <strong>in</strong> breast milk do not enter the neonatal and <strong>in</strong>fant<br />
circulation <strong>in</strong> substantial amounts. Pediatric Use Safety and effectiveness of<br />
STELARA ® <strong>in</strong> pediatric patients have not been evaluated. Geriatric Use Of the<br />
3117 psoriasis subjects exposed to STELARA ® , a total of 183 were 65 years or<br />
older, and 21 subjects were 75 years or older. Although no differences <strong>in</strong> safety<br />
or efficacy were observed between older and younger subjects, the number of<br />
subjects aged 65 and over is not sufficient to determ<strong>in</strong>e whether they respond<br />
differently from younger subjects. OVERDOSAGE: S<strong>in</strong>gle doses up to 4.5 mg/kg<br />
<strong>in</strong>travenously have been adm<strong>in</strong>istered <strong>in</strong> cl<strong>in</strong>ical studies without dose-limit<strong>in</strong>g<br />
toxicity. In case of overdosage, it is recommended that the patient be monitored<br />
for any signs or symptoms of adverse reactions or effects and appropriate<br />
symptomatic treatment be <strong>in</strong>stituted immediately. PATIENT COUNSELING<br />
INFORMATION: “See FDA-approved patient label<strong>in</strong>g (Medication Guide).”<br />
Instruct patients to read the Medication Guide before start<strong>in</strong>g STELARA ® therapy<br />
and to reread the Medication Guide each time the prescription is renewed.<br />
Infections Inform patients that STELARA ® may lower the ability of their immune<br />
system to fight <strong>in</strong>fections. Instruct patients of the importance of communicat<strong>in</strong>g<br />
any history of <strong>in</strong>fections to the doctor, and contact<strong>in</strong>g their doctor if they develop<br />
any symptoms of <strong>in</strong>fection. Malignancies Patients should be counseled about the<br />
risk of malignancies while receiv<strong>in</strong>g STELARA ® . Allergic Reactions Advise<br />
patients to seek immediate medical attention if they experience any symptoms<br />
of serious allergic reactions.<br />
Prefilled Syr<strong>in</strong>ge Manufactured by: Janssen Biotech, Inc., Horsham, PA 19044,<br />
License No. 1864 at Baxter Pharmaceutical Solutions, Bloom<strong>in</strong>gton, IN 47403<br />
Vial Manufactured by: Janssen Biotech, Inc., Horsham, PA 19044, License No.<br />
1864 at Cilag AG, Schaffhausen, Switzerland<br />
© Janssen Biotech, Inc. 2012<br />
25ST12104<br />
it is as effective as topical vitam<strong>in</strong> D analogues but more irritat<strong>in</strong>g.<br />
41 Us<strong>in</strong>g tazarotene <strong>in</strong> comb<strong>in</strong>ation with topical steroids<br />
appears to be more effective and decreases the irritation seen<br />
with topical ret<strong>in</strong>oids alone. 34 Tazarotene comes <strong>in</strong> 0.05% and<br />
0.01% as a cream, gel or jelly.<br />
Only up to 20% of body surface area should be treated,<br />
which makes this less useful for patients with diffuse disease.<br />
Because it is irritat<strong>in</strong>g, tazarotene should not be used <strong>in</strong> patients<br />
who are eythrodermic. It is pregnancy category X; regular<br />
pregnancy tests are very important, as well as counsel<strong>in</strong>g<br />
any woman of childbear<strong>in</strong>g potential about contraception.<br />
Topical Calc<strong>in</strong>eur<strong>in</strong> Inhibitors<br />
Calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors h<strong>in</strong>der the activity of calc<strong>in</strong>eur<strong>in</strong>,<br />
a phosphorylase enzyme that is needed for successful T-cell<br />
differentiation. Calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors <strong>in</strong>hibit T-cell function<br />
and <strong>in</strong>flammation. Calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors are effective<br />
for facial and flexural psoriasis. 42 It is a safe treatment but<br />
should be avoided <strong>in</strong> patients with sk<strong>in</strong> barrier dysfunction,<br />
as they are at risk for <strong>in</strong>creased systemic absorption. It is<br />
pregnancy category C.<br />
[Calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors are]<br />
a safe treatment but should<br />
be avoided <strong>in</strong> patients with<br />
sk<strong>in</strong> barrier dysfunction, as<br />
they are at risk for <strong>in</strong>creased<br />
systemic absorption.<br />
Anthral<strong>in</strong><br />
Anthral<strong>in</strong> is one of the oldest psoriatic medications. It <strong>in</strong>hibits<br />
epidermal and T-lymphocyte proliferation. <strong>The</strong> use of<br />
this medication is limited because of the complexity of application<br />
and the propensity of anthral<strong>in</strong> to sta<strong>in</strong> whatever it<br />
touches. Short-contact 0.3% anthral<strong>in</strong> o<strong>in</strong>tment for 10 m<strong>in</strong>utes<br />
daily comb<strong>in</strong>ed with a topical steroid, ret<strong>in</strong>oid or UV<br />
light regimen seems to have beneficial results. 43 Anthral<strong>in</strong><br />
comes <strong>in</strong> a cream formulation. <strong>The</strong> limitations <strong>in</strong>clude patient<br />
compliance, local sk<strong>in</strong> irritation and mess of application. This<br />
drug is pregnancy category C.<br />
Phototherapy<br />
Phototherapy has long been a very useful treatment option<br />
for psoriasis. <strong>Treatment</strong> options range from broad-band<br />
ultraviolet B therapy (BB-UVB), narrowband ultraviolet B<br />
therapy (NB-UVB), photochemotherapy with UVA and ei-<br />
20 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>The</strong> <strong>The</strong>rapeutic Approach to Psoriasis<br />
ther an oral or topical dose of psoralen UVA1. More recently,<br />
excimer laser has ga<strong>in</strong>ed FDA approval.<br />
NB-UVB is more effective at sub-erythmogenic doses than<br />
BB-UVB. 44 <strong>The</strong> efficacy of psoralen UVA (PUVA) therapy<br />
and NB-UVB has also been compared; PUVA is better at<br />
clear<strong>in</strong>g psoriasis, fewer sessions are needed and longer-last<strong>in</strong>g<br />
clearance is achieved. 45 However, there is an <strong>in</strong>creased risk of<br />
carc<strong>in</strong>ogenicity follow<strong>in</strong>g PUVA treatment. 46 <strong>The</strong> safety data<br />
for NB-UVB has not been fully determ<strong>in</strong>ed due to a lack of<br />
prospective studies. Excimer (308 nm) laser is a safe and effective<br />
treatment for psoriasis; a number of different protocols<br />
evaluated by Mudigonda et al showed no significant differences<br />
<strong>in</strong> the protocol used to <strong>in</strong>itiate treatment. 47<br />
<strong>The</strong> contra<strong>in</strong>dication of us<strong>in</strong>g<br />
methotrexate <strong>in</strong> comb<strong>in</strong>ation<br />
with oral ret<strong>in</strong>oids has been<br />
reevaluated. <strong>The</strong> comb<strong>in</strong>ation<br />
may provide benefit for<br />
patients with recalcitrant<br />
disease.<br />
Systemic Medications<br />
Systemic medications for severe psoriasis <strong>in</strong>clude methotrexate,<br />
cyclospor<strong>in</strong>e and oral ret<strong>in</strong>oids. Methotrexate <strong>in</strong>hibits<br />
dihydrofolate reductase, <strong>in</strong>hibit<strong>in</strong>g kerat<strong>in</strong>ocyte proliferation<br />
and immune function. Methotrexate is <strong>in</strong>dicated for severe<br />
plaque psoriasis and psoriatic arthritis and is adm<strong>in</strong>istered by<br />
once-weekly dos<strong>in</strong>g. Side effects <strong>in</strong>clude gastro<strong>in</strong>test<strong>in</strong>al upset,<br />
leucopenia, thrombocytopenia, renal failure, photosensitivity,<br />
fatigue and alopecia. 48 Pulmonary toxicity may occur.<br />
Side effects can be lessened by folic acid supplementation, 49<br />
although more recent conflict<strong>in</strong>g reports note the efficacy of<br />
methotrexate may be decreased secondary to folic acid supplementation.<br />
50 Hepatotoxity is a risk associated with cumulative<br />
dose. It used to be common practice to obta<strong>in</strong> liver<br />
biopsies once a cumulative dose of 1.5 grams was reached,<br />
but more recent evidence shows this is excessive <strong>in</strong> patients<br />
with no risk factors for liver disease. 51 Monitor<strong>in</strong>g blood cell<br />
counts, serum creat<strong>in</strong><strong>in</strong>e levels and liver enzymes is recommended.<br />
52 Methotrexate is pregnancy category X.<br />
Cyclospor<strong>in</strong>e is a calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitor adm<strong>in</strong>istered systemically<br />
and is <strong>in</strong>dicated for severe plaque psoriasis. Lowdose<br />
cyclospor<strong>in</strong>e, 2 mg/kg/day is useful; with the addition<br />
of topical corticosteroids, patients do significantly better still. 53<br />
It is a medication that works well as an <strong>in</strong>itial therapy until<br />
a safer ma<strong>in</strong>tenance therapy can be implemented. Cyclospor<strong>in</strong>e<br />
has nephrotoxic effects; blood pressure and renal function<br />
should be closely monitored while on this medication. <strong>The</strong><br />
dermatologist should also monitor liver function tests, serum<br />
lipids and serum electrolytes, especially magnesium levels. 52<br />
Cyclopsor<strong>in</strong>e is pregnancy category C.<br />
Systemic ret<strong>in</strong>oids have the same mechanism of action and<br />
effects as topical ret<strong>in</strong>oids. Acitret<strong>in</strong> is available <strong>in</strong> the United<br />
States and is <strong>in</strong>dicated for severe psoriasis. In a study look<strong>in</strong>g<br />
at the use of high-dose therapy, def<strong>in</strong>ed as approximately<br />
50mg/day versus low-dose therapy, patients <strong>in</strong> the low-dose<br />
treatment group had better results, likely secondary to better<br />
tolerability and adherence. 54 Serum triglyceride levels, liver<br />
enzymes, serum creat<strong>in</strong><strong>in</strong>e and screen<strong>in</strong>g for the development<br />
of hyperostosis is important. 52 Ret<strong>in</strong>oids have teratogenic effects,<br />
so screen<strong>in</strong>g for pregnancy is crucial and counsel<strong>in</strong>g is<br />
very important. With so many other non-teratogenic treatments<br />
available, the use of acitret<strong>in</strong> <strong>in</strong> women of childbear<strong>in</strong>g<br />
potential is discouraged.<br />
<strong>The</strong> contra<strong>in</strong>dication of us<strong>in</strong>g methotrexate <strong>in</strong> comb<strong>in</strong>ation<br />
with oral ret<strong>in</strong>oids has been reevaluated. <strong>The</strong> comb<strong>in</strong>ation<br />
may provide benefit for patients with recalcitrant disease.<br />
<strong>The</strong>re may be no added toxicity of us<strong>in</strong>g the comb<strong>in</strong>ation, as<br />
long as care <strong>in</strong> monitor<strong>in</strong>g patients is taken. 55<br />
Biologic <strong>The</strong>rapies<br />
An important group of biologic therapies, tumor necrosis<br />
factor alpha (TNF-α) <strong>in</strong>hibitors, have made an enormous impact<br />
<strong>in</strong> the treatment of patients with severe psoriasis. Etanercept<br />
was approved for psoriatic arthritis <strong>in</strong> 2002 and for<br />
moderate to severe psoriasis <strong>in</strong> 2004. It is a fusion prote<strong>in</strong><br />
TNF-α receptor to the Fc portion of IgG1. 56 <strong>The</strong> recommended<br />
dos<strong>in</strong>g regimen starts with twice-weekly 50-mg<br />
subcutaneous <strong>in</strong>jections and decreases to once a week after<br />
12 weeks. 57 Adalimumab was approved by the FDA for psoriatic<br />
arthritis <strong>in</strong> 2005 and for moderate to severe psoriasis <strong>in</strong><br />
2008. It is a fully human anti-TNF monoclonal antibody. 56<br />
<strong>The</strong> recommended dose is an 80-mg subcutaneous load<strong>in</strong>g<br />
dose followed by subcutaneous doses every other week of 40<br />
mg. 55 Infliximab, a mouse-human IgG1 chimeric anti-TNF<br />
monoclonal antibody, was approved for psoriatic arthritis <strong>in</strong><br />
2005 and for moderate to severe plaque psoriasis <strong>in</strong> 2006. 54<br />
Recommended dos<strong>in</strong>g starts at a dose of 5 mg/kg via <strong>in</strong>travenous<br />
<strong>in</strong>fusion at weeks 0, 2 and 6 and then cont<strong>in</strong>ued every<br />
8 weeks. 57 Golimumab is, at the time this article was written,<br />
FDA-approved for psoriatic arthritis only. It is a human IgGk<br />
antibody. <strong>The</strong> recommended dos<strong>in</strong>g is 50 mg <strong>in</strong>jected subcutaneously<br />
at monthly <strong>in</strong>tervals. 58<br />
Ustek<strong>in</strong>umab ga<strong>in</strong>ed FDA approval for the treatment of<br />
moderate to severe plaque psoriasis <strong>in</strong> 2009. It is a human<br />
IgG1 monoclonal antibody that b<strong>in</strong>ds the p40 subunit of IL-<br />
12 and IL-23. 59 IL-23 promotes the differentiation and proliferation<br />
of Th17 cells. 60 <strong>The</strong> effectiveness of ustek<strong>in</strong>umab<br />
highlighted the importance of Th17 cells <strong>in</strong> the pathogenesis<br />
of psoriasis. <strong>The</strong> recommended dos<strong>in</strong>g is 45 mg <strong>in</strong>jected subcutaneously<br />
for patients weigh<strong>in</strong>g less than 100 kg and 90 mg<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 21
<strong>The</strong> <strong>The</strong>rapeutic Approach to Psoriasis<br />
for patients weigh<strong>in</strong>g greater than 100 kg. This dose is repeated<br />
at week 4 and then ma<strong>in</strong>tenance doses are given every<br />
12 weeks thereafter. 61<br />
In terms of efficacy, adalimumab and <strong>in</strong>fliximab appear<br />
to be more effective than etanercept and methotrexate. 62,63<br />
Although the approved biologics are considered safe, effective<br />
and well tolerated, serious complications may occur, <strong>in</strong>clud<strong>in</strong>g<br />
demyel<strong>in</strong>ization, <strong>in</strong>fection, tuberculosis, malignancy,<br />
lymphoma, cardiovascular outcomes and hepatitis. 64 <strong>The</strong> approved<br />
biologics for psoriasis are all pregnancy category B.<br />
Alefecept and efalizumab were previously approved biologic<br />
therapies. Alefecept was voluntarily discont<strong>in</strong>ued and efalizumab<br />
was withdrawn after four reported cases of progressive<br />
multifocal leukoencephalopathy. 57<br />
Special Considerations<br />
Scalp Psoriasis<br />
A review of 18 randomized control trials about the success<br />
of topical corticosteroid therapy for scalp psoriasis shows<br />
that 40% to 70% of patients experienced more than 75%<br />
improvement and 43% to 90% experienced more than 90%<br />
<strong>in</strong>itial improvement. Topical steroids still seem to be a successful<br />
treatment option <strong>in</strong> these patients. <strong>The</strong>re may also be a role<br />
for add<strong>in</strong>g excimer 308 nm lasers. 65<br />
Nail Psoriasis<br />
Nail psoriasis often is very concern<strong>in</strong>g for the patient and<br />
one of the most difficult forms of psoriasis to treat. Methotrexate<br />
is frequently used to treat nail psoriasis. With the<br />
emergence of biologics, recent data suggests that they also are<br />
effective <strong>in</strong> treat<strong>in</strong>g nail psoriasis. 66,67<br />
Conclusion<br />
<strong>The</strong> therapeutic approach to psoriasis needs to be <strong>in</strong>dividualized<br />
to each patient, as there are many different, effective<br />
treatment options available. Generally, comb<strong>in</strong>ation therapies<br />
allow for the synergistic effects of multiple therapies and fewer<br />
side effects with lower doses. This will, hopefully, <strong>in</strong>crease<br />
patients’ compliance with any regimen. <strong>The</strong> risk vs. benefit<br />
from any medication must be discussed and unique patient<br />
characteristics must be <strong>in</strong>corporated when choos<strong>in</strong>g a medication<br />
to decrease adverse effects. n<br />
Dr. Daniel is with the department of dermatology at Wake Forest<br />
University School of Medic<strong>in</strong>e <strong>in</strong> W<strong>in</strong>ston-Salem, NC.<br />
Disclosure: Dr. Daniel has no conflicts of <strong>in</strong>terest to report.<br />
References<br />
1. Onumah N, Kircik LH. Psoriasis and its comorbidities. J Drugs Dermatol.<br />
2012; 11(5 suppl):s5-10.<br />
2. Kurd SK, Gelfand JM. <strong>The</strong> prevalence of previously diagnosed and undiagnosed<br />
psoriasis <strong>in</strong> US adults: results from NHANES 2003-2004. J Am Acad<br />
Dermatol. 2009; 60(2):218-224.<br />
3. Christophers E. Psoriasis - epidemiology and cl<strong>in</strong>ical spectrum. Cl<strong>in</strong> Exp<br />
Dermatol. 2001;26(4):314-320.<br />
4. Burch PR, Rowell, NR. Mode of <strong>in</strong>heritance <strong>in</strong> psoriasis. Arch Dermatol.<br />
1981;117(5):251-252.<br />
5. Smith AE, Kassab JY, Rowland Payne CM, Beer WE. Bimodality <strong>in</strong><br />
age of onset of psoriasis, <strong>in</strong> both patients and their relatives. <strong>Dermatology</strong>.<br />
1993;186(3):181-186.<br />
6. Ferrandiz C, Pujol RM, Garcia-Patos V, Bordas X, Smandia JA. Psoriasis of<br />
early and late onset: a cl<strong>in</strong>ical and epidemiologic study from Spa<strong>in</strong>. J Am Acad<br />
Dermatol. 2002;46(6):867-873.<br />
7. Hanseler T, Christopher E. Psoriasis of early and late onset: characterization<br />
of two types of psoriasis vulgaris. J Am Acad Dermatol. 1985;13(3):450-456.<br />
8. Dibi A, Jabourik F, Bentahila A. Psoriasis <strong>in</strong> <strong>in</strong>fants about five cases. Arch<br />
Pediatr. 2012;19(2):220-223.<br />
9. Morris A, Rogers M, Fischer G, Williams K. Childhood psoriasis: a cl<strong>in</strong>ical<br />
review of 1262 cases. Pediatr Dermatol. 2001;18(3):188-198.<br />
10. Capon F, Bijlmakers MJ, Wolf N, et al. Identification of ZNF313/<br />
RNF114 as a novel psoriasis susceptibility gene. Hum Mol Genet.<br />
2008;17(13):1938–1945.<br />
11. Capon F, Novelli G, Sempr<strong>in</strong>i S, et al. Search<strong>in</strong>g for psoriasis susceptibility<br />
genes <strong>in</strong> Italy: genome scan and evidence for a new locus on chromosome 1.<br />
J Invest Dermatol 1999;112(1):32-35.<br />
12. Cargill M, Schrodi SJ, Chang M, et al. A large-scale genetic association<br />
study confirms IL12B and leads to the identification of IL23R as psoriasis<br />
risk genes. Am J Hum Genet. 2007;80(2):273–290.<br />
13. Ell<strong>in</strong>ghaus E, Ell<strong>in</strong>ghaus D, Stuart PE, et al. Genome-wide association<br />
study identifies a psoriasis susceptibility locus at TRAF3IP2. Nat Genet.<br />
2010;42(11):991–995.<br />
14. Huffmeier U, Uebe S, Ekici AB, et al. Common variants at TRAF3IP2<br />
are associated with susceptibility to psoriatic arthritis and psoriasis. Nat Genet.<br />
2010;42(11):996–999.<br />
15. Nair RP, Henseler T, Jenisch S, et al. Evidence for two psoriasis susceptibility<br />
loci (HLA and 17q) and two novel candidate regions (16q and 20p) by<br />
genome-wide scan. Hum Mol Genet. 1997;6(8):1349-1356.<br />
16. Genetic Analysis of Psoriasis Consortium & the Wellcome Trust Case<br />
Control Consortium 2, Strange A, Capon F, et al. A genome-wide association<br />
study identifies new psoriasis susceptibility loci and an <strong>in</strong>teraction between<br />
HLA-C and ERAP1. Nat Genet. 2010;42(11):985–990.<br />
17. Stuart PE, Nair RP, Ell<strong>in</strong>ghaus E, et al. Genome-wide association<br />
analysis identifies three psoriasis susceptibility loci. Nat Genet.<br />
2010;42(11):1000–1004.<br />
18. Sun LD, Cheng H, Wang ZX et al. Association analyses identify six<br />
new psoriasis susceptibility loci <strong>in</strong> the Ch<strong>in</strong>ese population. Nat Genet.<br />
2010;42(11):1005–1009.<br />
19. Tomfohrde J, Silverman A, Barnes R, et al. Gene for familial psoriasis<br />
susceptibility mapped to the distal end of human chromosome 17q. Science.<br />
1994;264(5162):1141-1145.<br />
20. Zhang XJ, Huang W, Yang S et al. Psoriasis genome-wide association study<br />
identifies susceptibility variants with<strong>in</strong> LCE gene cluster at 1q21. Nat Genet.<br />
2009;41(2):205–210.<br />
21. Farber EM, Nall LM. <strong>The</strong> natural history of psoriasis <strong>in</strong> 5600 patients.<br />
Dermatologica 1974;148(1);1-18.<br />
22. Voorhees JJ: Pathophysiology of psoriasis. Annu Rev Med. 1977;28:467-473<br />
23. Lowes MA, Bowcock AM, Krueger JG. Pathogenesis and therapy of psoriasis.<br />
Nature. 2010;445(7130):866–873.<br />
24. Schwarz T. 25 years of UV-<strong>in</strong>duced immunosuppression mediated by T<br />
cells-from disregarded T suppressor cells to highly respected regulatory T<br />
cells. Photochem Photobiol. 2008;84(1):10–18.<br />
25. Wrone-Smith T, Nickoloff BJ. Dermal <strong>in</strong>jection of immunocytes <strong>in</strong>duces<br />
psoriasis. J Cl<strong>in</strong> Invest .1996;98(8):1878–1887<br />
26. Bergboer JG, Zeeuwen PL, Scalwijk J. Genetics of psoriasis: Evidence of<br />
epistatic <strong>in</strong>teraction between sk<strong>in</strong> barrier abnormalities and immune deviation.<br />
J Invest Dermatol. May 2012. doi: 10.1038/jid.2012.167.<br />
27. Waisman M. Historical note: Koebner on the isomorphic phenomenon.<br />
Arch Dermatol. 1981;117(7):415.<br />
28. Fernandez-Torres RM, Paradela S, Fanseca E. Psoriasis <strong>in</strong> patients older<br />
than 65 years. A comparative study with younger adult psoriatic patients. J<br />
Nutr Health Ag<strong>in</strong>g. 2012;16(6):586-591.<br />
29. Catanoso M, Pipitone N, Salvar<strong>in</strong>i C. Epidemiology of psoriatic arthritis.<br />
Reumatismo. 2012; 64(2):66.<br />
30. Moll JMH: Psoriatic arthropathy. In: Mier PD, van de Kerkhof PCM, ed.<br />
Textbook of <strong>Dermatology</strong>, Ed<strong>in</strong>burgh: Churchill Liv<strong>in</strong>gstone; 1986:55-82.<br />
22 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>The</strong> <strong>The</strong>rapeutic Approach to Psoriasis<br />
31. Tiberio R, Buzzo C, Pertusi G, et al. Calcipotriol <strong>in</strong>duces apoptosis <strong>in</strong> psoriatic<br />
kerit<strong>in</strong>ocytes. Cl<strong>in</strong> Exp Dermatol. 2009;34(8):e972-974.Epub 2009 Sep 15.<br />
32. Berth-Jones J, Hutch<strong>in</strong>son PE. Vitam<strong>in</strong> D analogues and psoriasis. Br J<br />
Dermatol. 1992;127(2):71-78.<br />
33. Devaux S, Castela A, Archier E, et al. Topical vitam<strong>in</strong> D analogues alone or<br />
<strong>in</strong> association with topical steroids: a systemic review. Acad of Venereol. 2012;26<br />
Suppl 3:52-60.<br />
34. Noris D. Mechanisms of action of topical therapies and the rationale for<br />
comb<strong>in</strong>ation therapy. J Am Acad Dermatol. 2005;53(1 Suppl 1):S17-25.<br />
35. Castela E, Archier E, Devaux S, et al. Topical corticosteroids <strong>in</strong> plaque<br />
psoriasis: a systemic review of efficacy and treatment modalities. J Eur Acad<br />
Dermatol Venereol. 2012;26 Suppl 3:36-46.<br />
36. Strowd L, Yentzer D, Fleischer A, Feldman SR. Increas<strong>in</strong>g use of more<br />
potent treatments for psoriasis. J Am Acad Dermatol. 2009;60 (3):478-481.<br />
37. McCla<strong>in</strong> RW, Yentzer BA, Feldman SR. Comparison of sk<strong>in</strong> concentrations<br />
follow<strong>in</strong>g topical versus oral corticosteroid treatment: reconsider<strong>in</strong>g the<br />
treatment of common <strong>in</strong>flammatory <strong>in</strong>flammatory dermatoses. J Drugs Dermatol.<br />
2009;8(12);1076-1079.<br />
38. War<strong>in</strong>o L, Balkrishnan R, Feldman SR. Clobetasol propionate for psoriasis:<br />
are o<strong>in</strong>tments really more potent J Drugs Dermatol. 2006;5(6):527-532.<br />
39. Katz HI, Hien NT, Prawer SE, Mastbaum LI, Mooney JJ, Samson CR.<br />
Superpotent topical steroid treatment of psoriasis vulgaris- cl<strong>in</strong>ical efficacy<br />
and adrenal function. J Am Acad Dermatol. 1987;16(4):804-811.<br />
40. Castela E, Archier E, Devaux S, et al. Topical corticosteroids <strong>in</strong> plaque psoriasis:<br />
a systemic review of risk for adrenal axis suppression and sk<strong>in</strong> atrophy. J<br />
Eur Acad Dermatol Venereol. 2012;26 Suppl 3:47-51.<br />
41. Bailey J, Whitehair B. Topical treatments of chronic plaque psoriasis. Am<br />
Fam Phsyician. 2010;81(5):596.<br />
42. Gribetz C, L<strong>in</strong>g M, Lebwohl M, et al. Pimecrolimus cream 1% <strong>in</strong> the<br />
treatment of <strong>in</strong>tertrig<strong>in</strong>ous psoriasis: a double bl<strong>in</strong>d, randomized study. J Am<br />
Acad Dermatol. 2004;51(5):731-738.<br />
43. Lowe N, Ashton R, Koudsi H, Verschoore M, Schaefer H. Anthral<strong>in</strong> for<br />
psoriasis: short-contact anthral<strong>in</strong> therapy compared with conventional topical<br />
steroid and conventional anthral<strong>in</strong>. J Am Acad Dermatol. 1984;10(1)1:69-72.<br />
44. Walters IB, Burack LH, Coven TR, Gilleaudeau P, Krueger JG. Suberythmogenic<br />
narrow-band UVB is markedly more effective than conventional UVB<br />
<strong>in</strong> treatment of psoriasis vulgaris. J Am Acad Dermatol. 1999;40(6 Pt 1):893-900.<br />
45. Archier E, Devaux S, Castela E, et al. Efficacy of psoralen UVA therapy vs<br />
narrowband UVB therapy <strong>in</strong> chronic plaque psoriasis: a systematic literature<br />
review. J Eur Acad Dermatol Venereol. 2012;26 Suppl3:11-21.<br />
46. Archier E, Devaux S, Castela E, et al. Carc<strong>in</strong>ogenic risks of psoaralen UVA<br />
therapy and narrowband UVB <strong>in</strong> chronic plaque psoriasis: a systematic literature<br />
review. J Eur Acad Dermatol Venereol. 2012;26 Suppl3:22-31.<br />
47. Mudigonda T, Dabade TS, Feldman SR. A review of protocols for 308 nm<br />
excimer laser phototherapy <strong>in</strong> psoriasis. J Drugs Dermatol. 2012;11(1):92-97.<br />
48. Gilani S, Khan D, Kahn F, Ahmed M. Adverse effects of low dose<br />
methotrexate <strong>in</strong> rheumatoid arthristis patients. J Coll Physicians Surg Pak.<br />
2012;22(2):101-104.<br />
49. Morgan SL, Baggott JE. Folate supplementation dur<strong>in</strong>g methotrexate<br />
therapy for rheumatoid arthritis. Cl<strong>in</strong> Exp Rheumatol. 2010;28(5 Suppl<br />
61):S102-109.<br />
50. Salim A, Tan E, Ilchyshyn A, Berth-Jones J. Folic acid supplementation<br />
dur<strong>in</strong>g treatment of psoriasis with methotrexate: A randomized, double-bl<strong>in</strong>d,<br />
placebo-controlled trial. Br J Dermatol. 2006;154(6):1169-1174.<br />
51. Thomas JA, Aithal GP. Monitor<strong>in</strong>g liver function dur<strong>in</strong>g methotrexate<br />
therapy for psoriasis: are rout<strong>in</strong>e biopsies really necessary Am J Cl<strong>in</strong> Dermatol.<br />
2005;6(6):357-363.<br />
52. Dubertret L. Ret<strong>in</strong>oids, methotrexate and cyclopspor<strong>in</strong>e. Curr Probl Dermatol.<br />
2009;38:79-94.<br />
53. Vena G, Galluccio A, Pezza M, Vestita M, Cassano N. Comb<strong>in</strong>ed treatment<br />
with low-dose cyclospor<strong>in</strong>e and calicipotriol/ betamethasone dipropionate<br />
o<strong>in</strong>tment for moderate-to-severe- plaque psoriasis: a randomized control<br />
open label study. J Dermatolog Treat. 2012;23(4):255-260.<br />
54. Haushalter K, Murad EJ, Dabade TS, Rowell R, Pearce DJ, Feldman SR.<br />
Efficacy of low-dose acitret<strong>in</strong> <strong>in</strong> the treatment of psoriasis. J Dermatolog Treat.<br />
2011 Jul 25. [epub ahead of pr<strong>in</strong>t].<br />
55. Searles AD, Lee AD, Feldman SR. Is concomitant use of methotrexate and<br />
oral ret<strong>in</strong>oids dangerous A review of the data regard<strong>in</strong>g this comb<strong>in</strong>ation. J<br />
Am Acad Dermatol. 2011;64(4):791-793.<br />
56. Mössner R, Schön MP, Reich K. Tumor necrosis factor antagonists <strong>in</strong> the<br />
therapy of psoriasis. Cl<strong>in</strong> Dermatol. 2008;26(5):486-502.<br />
57. Herrier RN. Advances <strong>in</strong> the treatment of moderate-to-severe plaque<br />
psoriasis. Am J Health Syst Pharm. 2011;68(9):795-806.<br />
58. Boyce EG, Halilovic J, Stan-Ugbene O. Golimumab: Review of the efficacy<br />
and tolerability of a recently approved tumor necrosis factor-α <strong>in</strong>hibitor.<br />
Cl<strong>in</strong> <strong>The</strong>r. 2010;32(10):1681-1703.<br />
59. Kurzeja M, Rudnicka L, Olszewska M. New <strong>in</strong>terleuk<strong>in</strong>-23 pathway <strong>in</strong>hibitors<br />
<strong>in</strong> dermatology: ustek<strong>in</strong>umab, briak<strong>in</strong>umab, and secuk<strong>in</strong>umab. Am J<br />
Cl<strong>in</strong> Dermatol. 2011;12(2):113-125.<br />
60. Lee E, Trepicchio WL, Oestreicher JL, et al. Increased expression of <strong>in</strong>terleuk<strong>in</strong><br />
23 p19 and p40 <strong>in</strong> lesional sk<strong>in</strong> of patients with psoriasis vulgaris. J Exp<br />
Med. 2004;199(1):125-130.<br />
61. Krulig E, Gordon KB. Ustek<strong>in</strong>umab: an evidence-based review of its effectiveness<br />
<strong>in</strong> the treatment of psoriasis. Core Evid. 2010;5:11-22.<br />
62. S<strong>in</strong>gnorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without<br />
head-to-head trials: a method for match<strong>in</strong>g-adjusted <strong>in</strong>direct comparisons<br />
applied to psoriasis treatment with adalimumab or etanercept. Pharmaoconomics.<br />
2010;28(10):935-945.<br />
63. Bansback N, Sizto S, Sun H et al. Efficacy of systemic treatments for moderate<br />
to severe plaque psoriasis. <strong>Dermatology</strong>. 2009;219(3):209-18.<br />
64. Papp KA, Dekoven J, Parsons L, et al. Biologic therapy <strong>in</strong> psoriasis: perspectives<br />
on associated risks and patient management. J Cutan Med Surg.<br />
2012;16(3):153-168.<br />
65. Wong JW, Kamangar F Nguyen R, Koo Y. Excimer laser therapy for hairl<strong>in</strong>e<br />
psoriasis: a useful addition to the scalp psoriasis treatment algorithm. Sk<strong>in</strong><br />
<strong>The</strong>rapy Lett. 2012;17(5):6-9.<br />
66. Kahl C, Hansen B, Reich K. Nail psoriasis — An ignored disorder. Pathogenesis,<br />
diagnosis and therapy. Hautarzt. 2012;63(3):184-191.<br />
67. Sánchez-Regaña M, Sola-Ortigosa J, Als<strong>in</strong>a-Gibert M, Vidal-Fernández<br />
M, Umbert-Millet P. Nail psoriasis: a retrospective study on the effectiveness<br />
of systemic treatment (classical and biological therapy). J Eur Acad Dermatol<br />
Venereol. 2011;25(5):579-586.<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 23
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> for<br />
Sk<strong>in</strong> Cancer<br />
A review of novel therapuetic approaches and comb<strong>in</strong>ation treatments to effectively manage sk<strong>in</strong> cancer.<br />
Jenna L. O’Neill, MD<br />
however, these treatment modalities are not without potential<br />
side effects. Novel therapeutic approaches and comb<strong>in</strong>ation<br />
therapies are often utilized <strong>in</strong> the treatment of sk<strong>in</strong> cancer,<br />
which may be challeng<strong>in</strong>g but reward<strong>in</strong>g.<br />
Figure 1. Basal cell carc<strong>in</strong>oma.<br />
Photo courtesy of Daniel Pearce, MD<br />
Sk<strong>in</strong> cancer is the most common type of cancer worldwide.<br />
<strong>The</strong> <strong>in</strong>cidence rates of both melanoma and nonmelanoma<br />
sk<strong>in</strong> cancers (NMSC) are <strong>in</strong>creas<strong>in</strong>g, 1-3<br />
which is a significant public health problem. <strong>The</strong> biologic<br />
behavior of sk<strong>in</strong> cancer ranges from slow-grow<strong>in</strong>g, locally<br />
<strong>in</strong>vasive cutaneous malignancy to locally aggressive tumors<br />
that may metastasize. Melanoma is associated with significant<br />
mortality when not treated early, and death from melanoma<br />
tends to occur at a younger age than for many other cancers. 4<br />
If detected early, sk<strong>in</strong> cancer is curable by surgical excision<br />
or destructive modalities. <strong>The</strong> ideal treatment for NMSC<br />
should provide complete tumor eradication with the lowest<br />
risk of recurrence and use the most cost effective method<br />
with acceptable cosmetic outcome. 5 Mohs micrographic surgery<br />
is used for <strong>in</strong>traoperative marg<strong>in</strong> assessment and for tissue<br />
preservation <strong>in</strong> cosmetically sensitive areas such as the face.<br />
Despite the success of surgical <strong>in</strong>tervention for sk<strong>in</strong> cancers,<br />
there are drawbacks, such as the need for local anesthesia, potential<br />
risk of <strong>in</strong>fection and scarr<strong>in</strong>g. Patient and/or tumor<br />
characteristics may necessitate other treatment methods if surgical<br />
<strong>in</strong>tervention is not a viable option. <strong>Treatment</strong> options for<br />
melanoma and NMSC target<strong>in</strong>g molecular defects <strong>in</strong> tumor<br />
cells may allow for treatment without the need for surgery;<br />
Non-Melanoma Sk<strong>in</strong> Cancer<br />
Basal cell carc<strong>in</strong>oma<br />
Basal cell carc<strong>in</strong>oma (BCC) is the most common malignancy<br />
worldwide, with an <strong>in</strong>cidence of 146 per 100,000 <strong>in</strong>dividuals<br />
<strong>in</strong> the United States. 6 BCC typically affects middle<br />
age and older adults, most commonly on the head and neck,<br />
followed by the trunk. Ultraviolet (UV) radiation is thought<br />
to play a role <strong>in</strong> the development of both BCC and squamous<br />
cell carc<strong>in</strong>oma (SCC). A higher <strong>in</strong>cidence of NMSC<br />
is reported <strong>in</strong> fair-sk<strong>in</strong>ned <strong>in</strong>dividuals, <strong>in</strong> those with greater<br />
outdoor exposure and <strong>in</strong> latitudes closer to the equator. 7,8 <strong>The</strong><br />
<strong>in</strong>cidence of BCC is <strong>in</strong>creased <strong>in</strong> patients with basal cell nevus<br />
syndrome, also known as Gorl<strong>in</strong> syndrome, <strong>in</strong> which mutations<br />
<strong>in</strong> the PTCH gene result <strong>in</strong> upregulation of the sonic<br />
hedgehog signal<strong>in</strong>g pathway and subsequent development of<br />
multiple BCCs beg<strong>in</strong>n<strong>in</strong>g <strong>in</strong> childhood or early adulthood.<br />
<strong>Treatment</strong> of BCC may vary by cl<strong>in</strong>ical subtype. Superficial<br />
BCC, which presents as an erythematous, scal<strong>in</strong>g telangiectatic<br />
plaque often on the trunk or extremities, may be treated<br />
with topical therapy or via electrodesiccation and curettage,<br />
while nodular BCC is typically excised surgically. More aggressive<br />
or poorly def<strong>in</strong>ed tumors are best treated with Mohs<br />
micrographic surgery. While BCC has an exceed<strong>in</strong>gly low<br />
potential for metastasis, local tissue destruction may be extensive<br />
<strong>in</strong> advanced or aggressive malignancies and may result <strong>in</strong><br />
considerable morbidity.<br />
Squamous cell carc<strong>in</strong>oma<br />
SCC presents as a scal<strong>in</strong>g, p<strong>in</strong>k to red papule, plaque or<br />
nodule that may be crusted or ulcerated, most frequently on<br />
the head and neck or other chronically sun-exposed sites. <strong>The</strong><br />
development of SCC is more strongly l<strong>in</strong>ked to UV exposure<br />
<strong>in</strong> comparison to BCC, <strong>in</strong> particular to chronic sun exposure.<br />
It is generally accepted that SCC occurs on a cont<strong>in</strong>uum<br />
with premalignant lesions conf<strong>in</strong>ed to the epidermis, such<br />
as act<strong>in</strong>ic keratoses (AKs). 9 Patients with AKs are 10 to 15<br />
times more likely to develop SCC compared to those without<br />
AKs. Bowen’s disease, a form of SCC <strong>in</strong> situ, typically<br />
24 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> In <strong>Dermatology</strong>: Sk<strong>in</strong> Cancer<br />
Table I. Indications for Mohs Micrographic Surgery<br />
Recurrent tumor<br />
High-risk anatomic location (periorificial)<br />
Anatomic sites where tissue preservation is imperative (eg, digits, genitalia)<br />
Aggressive histologic subtype<br />
Size > 2cm <strong>in</strong> diameter<br />
Poorly def<strong>in</strong>ed cl<strong>in</strong>ical borders<br />
Per<strong>in</strong>eural <strong>in</strong>vasion<br />
Figure 2. Keratoacanthoma type squamous cell<br />
carc<strong>in</strong>oma.<br />
Photo courtesy of Daniel Pearce, MD and Philip Williford, MD<br />
presents as a well-demarcated, brightly erythematous scal<strong>in</strong>g<br />
plaque. Keratoacanthoma (KA) may be a well-differentiated<br />
form of SCC, which rapidly enlarges over several weeks and<br />
may spontaneously <strong>in</strong>volute. Due to their propensity to cause<br />
tissue destruction and reports of metastasis, KAs are often<br />
treated surgically. Human papillomavirus is another important<br />
pathogenic factor implicated <strong>in</strong> some, if not all, cases of<br />
SCC. In addition, SCC is more common than BCC <strong>in</strong> immunosuppressed<br />
patients, <strong>in</strong>clud<strong>in</strong>g transplant recipients and<br />
<strong>in</strong>dividuals with HIV. In contrast to BCC, SCC is associated<br />
with a small but significant risk of metastasis, typically to regional<br />
lymph nodes. Prompt treatment with negative surgical<br />
marg<strong>in</strong>s is essential to m<strong>in</strong>imize morbidity of both the malignancy<br />
and its treatment.<br />
Surgical <strong>Treatment</strong><br />
Wide local excision is the primary treatment for NMSC,<br />
with a cure rate approach<strong>in</strong>g 90% or greater at 5 years. 10,11<br />
Optimal marg<strong>in</strong>s for excision of SCC are 4 mm for lesions<br />
less than 2 cm <strong>in</strong> greatest diameter and 6 mm for lesions<br />
larger than 2 cm. National Comprehensive Cancer Network<br />
(NCCN) guidel<strong>in</strong>es recommend 4-mm marg<strong>in</strong>s for excision<br />
of primary low-risk BCC. 12 A meta-analysis recommended<br />
3-mm surgical marg<strong>in</strong>s for BCC, with a cure rate of 95% for<br />
Figure 3. Melanoma on the right lower eyelid.<br />
Photo courtesy of Graham Dermatopathology Library<br />
lesions less than 2 cm <strong>in</strong> diameter. 5 Curettage and electrodessication<br />
is another treatment modality that <strong>in</strong>volves tumor destruction<br />
and has a comparable cure rate to excision for treatment<br />
of low-risk NMSC. 13 NCCN guidel<strong>in</strong>es recommend<br />
curettage and electrodesiccation for low-risk primary BCC<br />
or SCC on non hair-bear<strong>in</strong>g sites. If curettage is performed<br />
to the level of subcutaneous fat, complete surgical excision<br />
should be undertaken.<br />
Mohs micrographic surgery is a specialized surgical and<br />
pathologic technique that offers <strong>in</strong>traoperative histologic exam<strong>in</strong>ation<br />
of 100% of the tissue marg<strong>in</strong>s. This is a dist<strong>in</strong>ct<br />
advantage over conventional excision with frozen or paraff<strong>in</strong><br />
embedded sections, <strong>in</strong> which only a small proportion of the<br />
total peripheral marg<strong>in</strong> is exam<strong>in</strong>ed via th<strong>in</strong>, cross-sectional<br />
slices of tissue <strong>in</strong> a “bread loaf” technique. Mohs micrographic<br />
surgery offers the lowest recurrence rate and smallest defect<br />
size <strong>in</strong> the treatment of BCC and SCC and is the treatment<br />
of choice for recurrent tumors. 10,11,14,15 Generally accepted<br />
<strong>in</strong>dications for Mohs micrographic surgery also <strong>in</strong>clude: size<br />
> 2cm <strong>in</strong> diameter, high-risk anatomic location, per<strong>in</strong>eural<br />
<strong>in</strong>vasion and poorly def<strong>in</strong>ed cl<strong>in</strong>ical borders (see Table I). 16<br />
Mohs surgery is time-consum<strong>in</strong>g and very expensive and may<br />
require coord<strong>in</strong>ation with another physician to perform the<br />
reconstruction after negative marg<strong>in</strong>s are atta<strong>in</strong>ed. <strong>The</strong>refore,<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 25
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> In <strong>Dermatology</strong>: Sk<strong>in</strong> Cancer<br />
Mohs surgery should be reserved for high-risk tumors or<br />
when excision with standard marg<strong>in</strong>s would result <strong>in</strong> excessive<br />
tissue loss at sensitive anatomic sites.<br />
Non-Surgical <strong>Treatment</strong><br />
Radiation therapy (RT) is a valuable adjunctive therapy <strong>in</strong><br />
patients with residual positive tumor marg<strong>in</strong>s after extensive<br />
Mohs surgery or wide excision or <strong>in</strong> patients with high-risk<br />
tumors or extensive per<strong>in</strong>eural tumor <strong>in</strong>filtration. 17 Narrow<br />
radiation field marg<strong>in</strong>s of 1 cm to 2 cm are utilized; examples<br />
of dose and treatment schedules are provided <strong>in</strong> the NCCN<br />
guidel<strong>in</strong>es for treatment of NMSC. 12 RT is also utilized <strong>in</strong><br />
patients <strong>in</strong> whom surgical <strong>in</strong>tervention is not a viable option,<br />
either due to patient or tumor characteristics or both. A recent<br />
retrospective study demonstrated a 10-year relapse-free<br />
survival of 80.4% <strong>in</strong> patients with <strong>in</strong>operable SCC treated<br />
with superficial radiotherapy. 18 Irradiation of nodal bas<strong>in</strong>s <strong>in</strong><br />
conjunction with regional lymph node dissection improved<br />
Prevention and early detection<br />
of NMSC are key. Frequent<br />
monitor<strong>in</strong>g of patients with<br />
NMSC, <strong>in</strong>clud<strong>in</strong>g full sk<strong>in</strong><br />
exam<strong>in</strong>ation and counsel<strong>in</strong>g<br />
about the importance of daily<br />
sun protection, is imperative.<br />
survival compared to surgery alone <strong>in</strong> one study of 122 patients<br />
with metastatic spread of SCC to lymph nodes. 19 Adjuvant<br />
RT may also be utilized <strong>in</strong> cases of <strong>in</strong>operable lymph<br />
node disease.<br />
Photodynamic therapy (PDT) is a novel therapeutic method<br />
that uses a photosensitiz<strong>in</strong>g agent such as δ-am<strong>in</strong>olevul<strong>in</strong>ic<br />
acid (δ-ALA), which preferentially localizes to diseased cells.<br />
Topical application is followed by exposure to a light source<br />
with resultant selective cytotoxicity of tumor cells. PDT is<br />
FDA-approved for the treatment of act<strong>in</strong>ic keratoses and has<br />
also demonstrated efficacy <strong>in</strong> the treatment of SCC <strong>in</strong> situ 20,21<br />
and superficial BCC. 22,23 Methyl-am<strong>in</strong>olevul<strong>in</strong>ic acid (MAL),<br />
the methyl ester of ALA, has been used after curettage for<br />
nodular BCC, with equivalent recurrence rates to standard<br />
excision. 24,25 PDT has been used more recently as adjunctive<br />
therapy <strong>in</strong> the treatment of large non-melanoma sk<strong>in</strong> cancers<br />
prior to surgical removal. 26 Intraoperative PDT has been proposed<br />
as a means to decrease recurrence rates of NMSC after<br />
Mohs surgery <strong>in</strong> patients with extensive field cancerization. 27<br />
Cryosurgery may also be utilized for superficially <strong>in</strong>vasive<br />
NMSC, either as monotherapy or <strong>in</strong> comb<strong>in</strong>ation<br />
with topical chemotherapeutic agents. Cryosurgery and<br />
curettage has an excellent cure rate and cosmetic outcome<br />
for select tumors. 28,29 A comb<strong>in</strong>ation of cryosurgery and<br />
topical imiquimod, termed “immunocryosurgery,” has<br />
been employed with acceptable response rates. 30,31 Topical<br />
imiquimod 5% cream is an immune response modifier<br />
that activates the <strong>in</strong>nate and adaptive arms of the immune<br />
response via toll-like receptor 7 (TLR7). Imiquimod has<br />
been used alone <strong>in</strong> the treatment of nodular BCC, with<br />
complete clearance rates of 78% even with <strong>in</strong>tensive daily<br />
dos<strong>in</strong>g regimens. 32,33 Response rates for nodular BCC are<br />
greatly improved with pre-treatment curettage followed by<br />
imiquimod 5 times a week for 6 weeks. 34 Immunocryosurgery<br />
35,36 or imiquimod alone 37-39 may also be used for SCC<br />
<strong>in</strong> situ with excellent results.<br />
Vismodegib, a novel oral small-molecule <strong>in</strong>hibitor of smoothened<br />
(SMO), was recently approved by the FDA for metastatic<br />
or locally advanced BCC. SMO is normally <strong>in</strong>hibited by patched<br />
homologue 1 (PTCH), which is mutated <strong>in</strong> the majority of BCC<br />
and <strong>in</strong> patients with Gorl<strong>in</strong> syndrome. This mutation results <strong>in</strong><br />
constitutive activation of the Hedgehog signal<strong>in</strong>g pathway and<br />
unchecked tumor growth. Vismodegib is adm<strong>in</strong>istered orally at<br />
a dose of 150 mg daily. Early studies <strong>in</strong> patients with metastatic<br />
and locally advanced BCC demonstrated promis<strong>in</strong>g results, with<br />
response rates of 30 % and 43%, respectively, <strong>in</strong> 96 patients <strong>in</strong> an<br />
open-label, Phase II trial. 40,41 A randomized, double-bl<strong>in</strong>d, placebo-controlled<br />
trial of vismodegib <strong>in</strong> 41 patients with Gorl<strong>in</strong><br />
syndrome demonstrated a decrease <strong>in</strong> new BCCs as well as a<br />
decrease <strong>in</strong> size of exist<strong>in</strong>g BCCs. 42 <strong>Treatment</strong> with vismodegib<br />
is associated with a high rate of adverse events, most commonly<br />
dysgeusia and hair and weight loss, which necessitated discont<strong>in</strong>uation<br />
of therapy <strong>in</strong> 54% of patients enrolled <strong>in</strong> the latter study. 42<br />
<strong>The</strong> potential benefits of treatment must be weighed with these<br />
potentially serious adverse events. Careful patient selection will<br />
be imperative when utiliz<strong>in</strong>g this agent.<br />
Oral ret<strong>in</strong>oids, specifically acitret<strong>in</strong>, have been used as<br />
chemoprevention <strong>in</strong> patients at risk for develop<strong>in</strong>g multiple<br />
or aggressive SCCs, especially solid organ transplant recipients.<br />
43-45 Acitret<strong>in</strong> is typically adm<strong>in</strong>istered at the lowest effective<br />
dose <strong>in</strong> order to m<strong>in</strong>imize side effects, which <strong>in</strong>clude<br />
cheilitis, headache, photosensitivity, palmoplantar desquamation,<br />
epistaxis, musculoskeletal symptoms and elevated triglycerides.<br />
44 Abnormalities <strong>in</strong> liver enzymes were not observed<br />
<strong>in</strong> a systematic review of controlled trials of acitret<strong>in</strong><br />
for chemoprevention <strong>in</strong> transplant recipients. 45 Importantly,<br />
after discont<strong>in</strong>uation of acitret<strong>in</strong>, SCC development recurs. In<br />
organ transplant recipients at high risk for NMSC, chang<strong>in</strong>g<br />
the immunosuppressive regimen from a calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitor<br />
to sirolimus, a mammalian target of rapamyc<strong>in</strong> (mTOR)<br />
<strong>in</strong>hibitor with anti-tumor effects, may reduce the number of<br />
new cutaneous malignancies. 46<br />
Prevention and early detection of NMSC are key. Frequent<br />
monitor<strong>in</strong>g of patients with NMSC, <strong>in</strong>clud<strong>in</strong>g full<br />
26 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> In <strong>Dermatology</strong>: Sk<strong>in</strong> Cancer<br />
Table II. Major Prognostic Factors for Melanoma<br />
Breslow depth: >1mm high risk<br />
Male gender<br />
Advanced age<br />
Ulceration<br />
Anatomic site: head/neck and trunk high risk vs. extremities<br />
Number of <strong>in</strong>volved lymph nodes<br />
Site of distant metastases: visceral metastases high risk vs. sk<strong>in</strong>, subcutaneous, lymph nodes<br />
Table III. Surgical Marg<strong>in</strong>s for Primary Melanoma<br />
Thickness<br />
Marg<strong>in</strong>s (cm)<br />
In situ 0.5<br />
< 1 mm 1<br />
1– 4 mm 1 to 2*<br />
> 4 mm ≥ 2cm<br />
* AAD Task Force suggests a 1 cm marg<strong>in</strong> for tumors < 2 mm <strong>in</strong> depth.<br />
sk<strong>in</strong> exam<strong>in</strong>ation and counsel<strong>in</strong>g about the importance<br />
of daily sun protection, is imperative. Daily use of broadspectrum<br />
sunscreen with SPF 30 or greater is recommended<br />
by the American Academy of <strong>Dermatology</strong>; sun-protective<br />
cloth<strong>in</strong>g and avoidance dur<strong>in</strong>g peak sun hours also play an<br />
important role.<br />
Melanoma<br />
It is estimated that 76,250 men and women will be diagnosed<br />
with, and 9,180 will die from, melanoma <strong>in</strong> 2012. 2 <strong>The</strong><br />
<strong>in</strong>cidence and mortality rate from melanoma have <strong>in</strong>creased<br />
<strong>in</strong> recent decades. 1 Melanocytes are neural crest-derived cells<br />
that normally reside <strong>in</strong> the basal layer of the epidermis and<br />
produce melan<strong>in</strong>. <strong>The</strong> pathogenesis of melanoma is complex<br />
and is thought to <strong>in</strong>volve evasion of the host immune response<br />
by cancer cells. When detected early, melanoma is curable<br />
by wide excision. Delays <strong>in</strong> diagnosis and treatment may<br />
result <strong>in</strong> local <strong>in</strong>vasion of melanoma and distant metastases,<br />
typically to regional lymph nodes and visceral organs <strong>in</strong>clud<strong>in</strong>g<br />
the lungs, liver, bones and bra<strong>in</strong>. In contrast to most other<br />
solid organ tumors, melanoma recurrence may present many<br />
years after <strong>in</strong>itial diagnosis and complete surgical resection.<br />
Metastatic melanoma is exceptionally resistant to treatment<br />
with conventional chemotherapy and the prognosis rema<strong>in</strong>s<br />
very poor, despite advances <strong>in</strong> our knowledge of melanoma<br />
pathogenesis. Recent molecular genetic studies have revealed<br />
mutations <strong>in</strong> melanoma cells that may be specifically targeted<br />
<strong>in</strong> the treatment of advanced melanoma. <strong>The</strong> mitogen-activated<br />
prote<strong>in</strong> k<strong>in</strong>ase (MAPK) pathway plays a crucial role <strong>in</strong><br />
regulat<strong>in</strong>g cell proliferation, survival and differentiation. <strong>The</strong><br />
BRAF gene, which encodes a prote<strong>in</strong> k<strong>in</strong>ase upstream regulator<br />
of MAPK, harbors an activat<strong>in</strong>g mutation <strong>in</strong> 40% to 60%<br />
of melanomas. 47,48<br />
Like other malignancies, the development of <strong>in</strong>vasive melanoma<br />
is thought to progress through a step-wise process with<br />
accumulation of mutations with<strong>in</strong> melanoma cells, which are<br />
<strong>in</strong>fluenced by both genetic and environmental factors. Melanoma<br />
<strong>in</strong> situ (MIS) is a proliferation of atypical melanocytes<br />
conf<strong>in</strong>ed to the epidermis and may precede the development<br />
of melanoma. Melanoma may arise with<strong>in</strong> a pre-exist<strong>in</strong>g nevus,<br />
but more than half of melanomas arise de novo. Four<br />
major subtypes have been described: superficial spread<strong>in</strong>g,<br />
nodular, acral lentig<strong>in</strong>ous and lentigo maligna melanoma. Regardless<br />
of subtype, prognosis is primarily determ<strong>in</strong>ed by the<br />
Breslow thickness, or depth of <strong>in</strong>vasion, of the tumor. Breslow<br />
depth is important for determ<strong>in</strong><strong>in</strong>g excisional marg<strong>in</strong>s<br />
and tumor stag<strong>in</strong>g and is the strongest predictor of melanoma<br />
mortality. Additional predictors of poor prognosis <strong>in</strong> melanoma<br />
are male gender, presence of ulceration and distant metastases<br />
(see Table II).<br />
28 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> In <strong>Dermatology</strong>: Sk<strong>in</strong> Cancer<br />
Psychosocial Issues In Familial Melanoma<br />
<strong>The</strong> Sk<strong>in</strong> Cancer page from the National Cancer Institute (NCI) offers patients with both non-melanoma sk<strong>in</strong> cancer<br />
(NMSC) and melanoma a variety of resources, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong>formation about treatment, cl<strong>in</strong>ical trials, statistics and<br />
more. <strong>The</strong> page on the genetics of sk<strong>in</strong> cancer <strong>in</strong>cludes <strong>in</strong>formation about the structure and function of the sk<strong>in</strong>, cl<strong>in</strong>ical<br />
presentations of NMSC and melanoma, rare sk<strong>in</strong> cancer syndromes and psychosocial issues <strong>in</strong> familial melanoma.<br />
<strong>The</strong> <strong>in</strong>formation on the psychosocial issues was updated very recently, at the end of July 2012, and discusses <strong>in</strong>terest<br />
<strong>in</strong> and motivation for genetic test<strong>in</strong>g to determ<strong>in</strong>e risk of melanoma and the behavior of <strong>in</strong>dividuals found to be at a<br />
high risk for the most serious type of sk<strong>in</strong> cancer. <strong>The</strong> update comes on the heels of a number of new studies about<br />
genetic and lifestyle factors that may contribute to melanoma risk, as well as a new app that may aid <strong>in</strong> personal sk<strong>in</strong><br />
cancer screen<strong>in</strong>gs.<br />
Limited Data, Conflict<strong>in</strong>g Results<br />
<strong>The</strong> review of the psychosocial issues <strong>in</strong> <strong>in</strong>dividuals with a family history of melanoma is written for healthcare professionals<br />
and is <strong>in</strong>tended to help elucidate the factors <strong>in</strong>volved <strong>in</strong> an <strong>in</strong>dividual’s perception of his or her risk, desire to<br />
undergo genetic test<strong>in</strong>g, and prevention practices, all <strong>in</strong> an effort to decrease the rates of melanoma among family<br />
members of patients.<br />
Accord<strong>in</strong>g to the authors of this review, the motivations for and <strong>in</strong>terest <strong>in</strong> genetic test<strong>in</strong>g for melanoma have not been<br />
extensively studied, but the general f<strong>in</strong>d<strong>in</strong>gs note there is a high — but not universal — <strong>in</strong>terest <strong>in</strong> genetic test<strong>in</strong>g, and<br />
<strong>in</strong>dividuals at a high risk for melanoma are able to articulate the benefits of test<strong>in</strong>g. <strong>The</strong>y also note ‘a relative lack’ of<br />
exam<strong>in</strong>ation of the potential limitations of test<strong>in</strong>g and reasons to forgo test<strong>in</strong>g. <strong>The</strong> most important factor that <strong>in</strong>fluences<br />
an <strong>in</strong>dividual’s desire to be tested for melanoma susceptibility is be<strong>in</strong>g a parent; many studies reveal that <strong>in</strong>dividuals<br />
with children are more likely to be tested, primarily to determ<strong>in</strong>e the relative risk to their offspr<strong>in</strong>g. <strong>The</strong> research that<br />
focuses on <strong>in</strong>dividuals who have undergone genetic test<strong>in</strong>g for melanoma reveals conflict<strong>in</strong>g evidence. Most studies<br />
have shown no <strong>in</strong>crease <strong>in</strong> psychological distress, like anxiety and depression.<br />
Protective behaviors before and after screen<strong>in</strong>g for genetic susceptibility have been exam<strong>in</strong>ed slightly more extensively.<br />
Generally, <strong>in</strong>dividuals who are identified as hav<strong>in</strong>g an <strong>in</strong>creased risk for melanoma from genetic test<strong>in</strong>g are more likely<br />
to <strong>in</strong>crease the frequency of several protective behaviors: sunscreen use, self-exams for sk<strong>in</strong> changes and sk<strong>in</strong> checks<br />
by a physician.<br />
Several demographic factors may <strong>in</strong>crease these proactive behaviors <strong>in</strong> an <strong>in</strong>dividual who has been identified by<br />
genetic test<strong>in</strong>g for a higher risk of melanoma. Adoption of protective behaviors is more likely <strong>in</strong> <strong>in</strong>dividuals with a<br />
familial risk of melanoma who are older, female and more confident <strong>in</strong> their ability to practice such behaviors. In addition,<br />
regular sunscreen use has been correlated to higher levels of education, higher self-efficacy for sun protection<br />
and higher perceived melanoma risk.<br />
<strong>The</strong> Psychosocial Issues <strong>in</strong> Familial Melanoma page briefly discusses the efficacy of <strong>in</strong>terventions about sun protection<br />
and screen<strong>in</strong>g <strong>in</strong> family members of melanoma patients. <strong>The</strong> results of exist<strong>in</strong>g studies are also <strong>in</strong>consistent. One study<br />
with sibl<strong>in</strong>gs utilized telephone messages and tailored pr<strong>in</strong>t materials about risk reduction and screen<strong>in</strong>g recommendations;<br />
the control group received standard-of-care physician recommendations that patients tell family members about<br />
their diagnosis. That study showed an <strong>in</strong>crease <strong>in</strong> knowledge about melanoma, confidence <strong>in</strong> see<strong>in</strong>g a dermatologist<br />
for a sk<strong>in</strong> check and greater self-exam practices <strong>in</strong> the <strong>in</strong>tervention group. Another study that utilized a similar <strong>in</strong>tervention<br />
<strong>in</strong> family members of melanoma patients showed a near two-fold <strong>in</strong>crease <strong>in</strong> sk<strong>in</strong> exam<strong>in</strong>ations by a healthcare<br />
provider <strong>in</strong> the <strong>in</strong>tervention group but failed to show a change <strong>in</strong> sunscreen behaviors <strong>in</strong> either group.<br />
To learn more about this data from the NCI, and for additional resources, please visit www.cancer.gov/cancertopics/<br />
types/sk<strong>in</strong>. For more <strong>in</strong>formation about the recent developments <strong>in</strong> the understand<strong>in</strong>g of the genetic and lifestyle risk<br />
factors for NMSC and melanoma, please visit www.the-dermatologist.com.<br />
— Julia Ernst, MS, Assistant Editor<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 29
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> In <strong>Dermatology</strong>: Sk<strong>in</strong> Cancer<br />
Surgical <strong>Treatment</strong><br />
Biopsy technique is essential <strong>in</strong> evaluat<strong>in</strong>g a suspicious<br />
lesion for accurate diagnosis and measurement of Breslow<br />
depth <strong>in</strong> the event of a melanoma diagnosis. Excisional biopsy<br />
technique with narrow marg<strong>in</strong>s of surround<strong>in</strong>g sk<strong>in</strong><br />
is preferred, unless lesion size or location prevents it. Follow<strong>in</strong>g<br />
histologic diagnosis, wide local excision is the preferred<br />
treatment method, with marg<strong>in</strong>s based on Breslow<br />
depth (see Table III). <strong>The</strong> use of Mohs micrographic surgery<br />
<strong>in</strong> the treatment of melanoma rema<strong>in</strong>s controversial,<br />
due, <strong>in</strong> part, to concern about the difficulty <strong>in</strong> detect<strong>in</strong>g<br />
abnormal melanocytes <strong>in</strong> frozen sections. Various modifications<br />
have been proposed to address this issue, <strong>in</strong>clud<strong>in</strong>g<br />
the use of <strong>in</strong>traoperative immunosta<strong>in</strong><strong>in</strong>g for melanoma<br />
markers such as MelanA/MART1 49 and the use of modified<br />
or “slow” Mohs with permanent paraff<strong>in</strong>-embedded<br />
tissue sections for tumors with ill-def<strong>in</strong>ed marg<strong>in</strong>s or for<br />
tissue spar<strong>in</strong>g <strong>in</strong> sensitive anatomic sites. 50 Local tumor recurrence,<br />
sometimes after many months or years, cont<strong>in</strong>ues<br />
after these techniques.<br />
Sk<strong>in</strong> cancers may be curable<br />
when detected early and<br />
adequately treated, but the<br />
prognosis for advanced<br />
cutaneous malignancies<br />
is poor.<br />
Patients with melanomas greater than 1 mm <strong>in</strong> thickness<br />
may be considered for sent<strong>in</strong>el lymph node biopsy (SLNB),<br />
which provides prognostic <strong>in</strong>formation by detect<strong>in</strong>g melanoma<br />
spread to regional lymph nodes. 51 This practice rema<strong>in</strong>s<br />
controversial among dermatologists, as subsequent complete<br />
lymph node dissection for metastatic disease is not without<br />
potential morbidity and has not demonstrated survival benefit<br />
over observation. 52<br />
Adjuvant <strong>The</strong>rapies<br />
Non-<strong>in</strong>vasive methods for treat<strong>in</strong>g lentigo maligna (a type<br />
of MIS) with ill-def<strong>in</strong>ed tumor marg<strong>in</strong>s or extensive <strong>in</strong>volvement<br />
of sensitive anatomic sites have been proposed as a tissue-spar<strong>in</strong>g<br />
technique. A review of treatment options for lentigo<br />
maligna recommends the use of imiquimod cream with<br />
great caution due to short follow-up times and the possibility<br />
of an <strong>in</strong>vasive component not detected on biopsy. 53 Radiation<br />
therapy (RT) has also been proposed for large lentigo<br />
maligna or lentigo maligna melanoma lesions on the face or<br />
<strong>in</strong> elderly patients who may not be able to tolerate surgery,<br />
with reported cure rates greater than 90%. 54,55 Palliative RT<br />
may be used <strong>in</strong> patients with symptomatic metastatic disease,<br />
particularly <strong>in</strong>operable bra<strong>in</strong> metastases. Curative resection of<br />
stable metastatic lesions, such as distant nodes or isolated visceral<br />
tumors, should be considered for appropriate patients.<br />
Several approaches to systemic adjuvant therapy have been<br />
tried <strong>in</strong> patients with high risk or metastatic melanoma, <strong>in</strong>clud<strong>in</strong>g<br />
traditional chemotherapy, immunotherapy and vacc<strong>in</strong>ation.<br />
Unfortunately, these treatments have generally failed<br />
to show any significant survival benefit.<br />
In 2011, the FDA approved two targeted therapies for<br />
metastatic melanoma, represent<strong>in</strong>g a significant advance <strong>in</strong><br />
melanoma treatment. Ipilimumab is a monoclonal antibody<br />
directed aga<strong>in</strong>st cytotoxic T lymphocyte-associated antigen<br />
4 (CTLA-4), which downregulates T cell activation.<br />
By block<strong>in</strong>g CTLA-4, ipilimumab promotes T-cell mediated<br />
anti-tumor immunity. Ipilimumab is adm<strong>in</strong>istered by<br />
<strong>in</strong>travenous <strong>in</strong>fusion once every 3 weeks for a total of four<br />
doses. A randomized phase III trial demonstrated prolonged<br />
survival <strong>in</strong> 676 patients with advanced melanoma treated<br />
with ipilimumab compared to patients receiv<strong>in</strong>g a peptide<br />
vacc<strong>in</strong>e (10 months vs 6.4 months, respectively, P
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> In <strong>Dermatology</strong>: Sk<strong>in</strong> Cancer<br />
to develop therapies that provide susta<strong>in</strong>ed responses and high<br />
response rates with favorable side effects profiles. A f<strong>in</strong>al note<br />
is the importance of close follow-up to detect recurrent or<br />
metastatic melanoma; patients diagnosed with melanoma are<br />
at an <strong>in</strong>creased risk of develop<strong>in</strong>g a second primary melanoma.<br />
Counsel<strong>in</strong>g melanoma patients and their first-degree<br />
relatives about this risk and the importance of daily sun protection<br />
is essential.<br />
Conclusion<br />
Sk<strong>in</strong> cancer is the most common cancer worldwide,<br />
caus<strong>in</strong>g significant morbidity and consum<strong>in</strong>g substantial<br />
healthcare resources. Sk<strong>in</strong> cancers may be curable when<br />
detected early and adequately treated, but the prognosis for<br />
advanced cutaneous malignancies is poor. Various surgical<br />
and non-surgical therapeutic options exist for both melanoma<br />
and NMSC, with novel targeted therapies emerg<strong>in</strong>g<br />
for patients with advanced disease. <strong>The</strong> choice of therapy<br />
and determ<strong>in</strong>ation of therapeutic goals and expectations<br />
should be discussed with the patient and his or her family<br />
to optimize treatment outcomes. A multidiscipl<strong>in</strong>ary<br />
approach is often critical for patients with advanced cutaneous<br />
malignancy, with <strong>in</strong>put from oncology, radiology,<br />
surgery and otolaryngology colleagues. F<strong>in</strong>ally, prevention<br />
of sk<strong>in</strong> cancer is paramount; every patient encounter may<br />
be viewed as an opportunity to educate patients about the<br />
importance of daily sun protection.n<br />
Dr. O’Neill is with the department of dermatology at Wake Forest<br />
University School of Medic<strong>in</strong>e <strong>in</strong> W<strong>in</strong>ston-Salem, NC.<br />
Disclosure: Dr. O’Neill does not have any <strong>in</strong>dustry relationships<br />
or f<strong>in</strong>ancial conflicts of <strong>in</strong>terest to disclose.<br />
References<br />
1. Lens MB, Dawes M. Global perspectives of contemporary epidemiological<br />
trends of cutaneous malignant melanoma. Br J Dermatol. 2004;150:179-185.<br />
2. U.S. National Institutes of Health. SEER stat fact sheets: Melanoma of the<br />
sk<strong>in</strong>. National Cancer Institute 2011. Accessibility verified June 22, 2012. Available<br />
at: http://seer.cancer.gov/statfacts/html/melan.html#<strong>in</strong>cidence-mortality<br />
3. Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic review of worldwide<br />
<strong>in</strong>cidence of nonmelanoma sk<strong>in</strong> cancer. Br J Dermatol. 2012;166:1069.<br />
4. We<strong>in</strong>stock MA. Epidemiology, etiology and control of melanoma. Med<br />
Health R I. 2001;84:234-236.<br />
5. Gulleth Y, Goldberg N, Silverman RP, Gastman BR. What is the best surgical<br />
marg<strong>in</strong> for a basal cell carc<strong>in</strong>oma: A meta-analysis of the literature. Plast<br />
Reconstr Surg. 2010;126(4):1222-31.<br />
6. Staples M, Marks R, Giles G. Trends <strong>in</strong> the <strong>in</strong>cidence of nonmelanoma<br />
sk<strong>in</strong> cancer (NMSC) treated <strong>in</strong> Australia 1985-1995: Are primary prevention<br />
programs start<strong>in</strong>g to have an effect Int J Cancer. 1998;78:144-8.<br />
7. Urbach F. Incidence of nonmelanoma sk<strong>in</strong> cancer. Dermatol Cl<strong>in</strong>.<br />
1991;9(4):751–5.<br />
8. Gloster HM, Brodland DG Jr. <strong>The</strong> epidemiology of sk<strong>in</strong> cancer. Dermatol<br />
Surg. 1996;22(3):217–26.<br />
9. Czarnecki D, Meehan CJ, Bruce F, Culjak G. <strong>The</strong> majority of cutaneous<br />
squamous cell carc<strong>in</strong>omas arise <strong>in</strong> act<strong>in</strong>ic keratoses. J Cutan Med Surg.<br />
2002;6(3):207-9.<br />
10. Rowe DE, Carroll RJ, Day CL Jr. Long-term recurrence rates <strong>in</strong> previously<br />
untreated (primary) basal cell carc<strong>in</strong>oma: Implications for patient follow-up.<br />
J Dermatol Surg Oncol. 1989;15(3):315-28.<br />
11. Mosterd K, Krekels GA, Nieman FH, et al. Surgical excision versus Mohs<br />
micrographic surgery for primary and recurrent basal-cell carc<strong>in</strong>oma of the<br />
face: A prospective randomised controlled trial with 5-years’ follow-up. Lancet<br />
Oncol. 2008;9(12):1149-56.<br />
12. Miller SJ, Alam M, Andersen J, et al. Basal cell and squamous cell sk<strong>in</strong><br />
cancers. J Natl Compr Canc Netw. 2010;8:836-64<br />
13. Reschly MJ, Shenefelt PD. Controversies <strong>in</strong> sk<strong>in</strong> surgery: Electrodessication<br />
and curettage versus excision for low-risk, small, well-differentiated<br />
squamous cell carc<strong>in</strong>omas. J Drugs Dermatol. 2010;9(7):773-6.<br />
14. Stegman SJ, Tromovitch TA. Modern chemosurgery--microscopically<br />
controlled excision. West J Med. 1980;132(1):7-12.<br />
15. Rowe DE, Carroll RJ, Day CL Jr. Mohs surgery is the treatment of choice<br />
for recurrent (previously treated) basal cell carc<strong>in</strong>oma. J Dermatol Surg Oncol.<br />
1989;15(4):424-31.<br />
16. Bolognia JL, Jorizzo JL, Rap<strong>in</strong>i RP. <strong>Dermatology</strong>. St. Louis, Missouri:<br />
Mosby/Elsevier, 2008. Second edition.<br />
17. Han A, Ratner D. What is the role of adjuvant radiotherapy <strong>in</strong> the treatment<br />
of cutaneous squamous cell carc<strong>in</strong>oma with per<strong>in</strong>eural <strong>in</strong>vasion Cancer.<br />
2007;109(6):1053-9.<br />
18. Barysch MJ, Eggmann N, Beyeler M, Panizzon RG, Seifert B, Dummer R.<br />
Long-term recurrence rate of large and difficult to treat cutaneous squamous<br />
cell carc<strong>in</strong>omas after superficial radiotherapy. <strong>Dermatology</strong>. 2012;224(1):59-65.<br />
19. Wang JT, Palme CE, Morgan GJ, Gebski V, Wang AY, Veness MJ. Predictors<br />
of outcome <strong>in</strong> patients with metastatic cutaneous head and neck squamous<br />
cell carc<strong>in</strong>oma <strong>in</strong>volv<strong>in</strong>g cervical lymph nodes: Improved survival with the<br />
addition of adjuvant radiotherapy. Head Neck. 2011 Nov 23. doi: 10.1002/<br />
hed.21965. [Epub ahead of pr<strong>in</strong>t]<br />
20. Morton CA, Whitehurst C, Moseley H, McColl JH, Moore JV, Mackie<br />
RM. Comparison of photodynamic therapy with cryotherapy <strong>in</strong> the treatment<br />
of Bowen’s disease. Br J Dermatol. 1996;135:766-771.<br />
21. Cox NH, Eedy DJ, Morton CA. Guidel<strong>in</strong>es for management of Bowen’s<br />
disease: 2006 update. Br J Dermatol. 2007;156:11-21.<br />
22. Marmur ES, Schmults CD, Goldberg DJ. A review of laser and photodynamic<br />
therapy for the treatment of nonmelanoma sk<strong>in</strong> cancer. Dermatol Surg.<br />
2004;30:264-271.<br />
23. Morton CA, McKenna KE, Rhodes LE. Guidel<strong>in</strong>es for topical photodynamic<br />
therapy: Update. Br J Dermatol. 2008;159:1245-1266.<br />
24. Horn M, Wolf P, Wulf HC, et al. Topical methyl am<strong>in</strong>olaevul<strong>in</strong>ate photodynamic<br />
therapy <strong>in</strong> patients with basal cell carc<strong>in</strong>oma prone to complications<br />
and poor cosmetic outcome with conventional treatment. Br J Dermatol. 2003;<br />
149: 1242-1249.<br />
25. V<strong>in</strong>ciullo C, Elliott T, Francis D, et al. Photodynamic therapy with topical<br />
methyl am<strong>in</strong>olaevul<strong>in</strong>ate for “difficult-to-treat” basal cell carc<strong>in</strong>oma. Br J<br />
Dermatol. 2005;152:765-772.<br />
26. Jeremic G, Brandt MG, Jordan K, Doyle PC, Yu E, Moore CC. Us<strong>in</strong>g<br />
photodynamic therapy as a neoadjuvant treatment <strong>in</strong> the surgical excision of<br />
nonmelanotic sk<strong>in</strong> cancers: Prospective study. J Otolaryngol Head Neck Surg.<br />
2011; 40 Suppl 1: S82-9.<br />
27. Marmur ES, Nolan KA, Henry M. Intraoperative photodynamic therapy: A<br />
description of a new adjuvant technique for patients with nonmelanoma sk<strong>in</strong><br />
cancer. Dermatol Surg. 2012 May 18. doi: 10.1111/j.1524-4725.2012.02433.x.<br />
[Epub ahead of pr<strong>in</strong>t]<br />
28. Peikert JM. Prospective trial of curettage and cryosurgery <strong>in</strong> the management<br />
of non-facial, superficial, and m<strong>in</strong>imally <strong>in</strong>vasive basal and squamous cell<br />
carc<strong>in</strong>oma. Int J Dermatol. 2011;50(9):1135-8.<br />
29. L<strong>in</strong>demalm-Lundstam B, Dalenbäck J. Prospective follow-up after<br />
curettage-cryosurgery for scalp and face sk<strong>in</strong> cancers. Br J Dermatol.<br />
2009;161(3):568-76.<br />
30. Gaitanis G, Nomikos K, Vava E, Alexopoulos EC, Bassukas ID. Immunocryosurgery<br />
for basal cell carc<strong>in</strong>oma: Results of a pilot, prospective, open-label<br />
study of cryosurgery dur<strong>in</strong>g cont<strong>in</strong>ued imiquimod application. J Eur Acad<br />
Dermatol Venereol. 2009;23(12):1427-31.<br />
31. Gaitanis G, Alexopoulos EC, Bassukas ID. Cryosurgery is more effective<br />
<strong>in</strong> the treatment of primary, non-superficial basal cell carc<strong>in</strong>omas when applied<br />
dur<strong>in</strong>g and not prior to a five week imiquimod course: A randomized,<br />
prospective, open-label study. Eur J Dermatol. 2011;21(6):952-8.<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 31
<strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> In <strong>Dermatology</strong>: Sk<strong>in</strong> Cancer<br />
32. Eigentler TK, Kam<strong>in</strong> A, Weide BM, et al. A Phase III, randomized, open<br />
label study to evaluate the safety and efficacy of imiquimod 5% cream applied<br />
thrice weekly for 8 and 12 weeks <strong>in</strong> the treatment of low-risk nodular basal<br />
cell carc<strong>in</strong>oma. J Am Acad Dermatol. 2007;57(4):616-21.<br />
33. Shumack S, Rob<strong>in</strong>son J, Kossard S, et al. Efficacy of topical 5% imiquimod<br />
cream for the treatment of nodular basal cell carc<strong>in</strong>oma: comparison of dos<strong>in</strong>g<br />
regimens. Arch Dermatol. 2002;138(9):1165-71.<br />
34. Neville JA, Williford PM, Jorizzo JL. Pilot study us<strong>in</strong>g topical imiquimod<br />
5% cream <strong>in</strong> the treatment of nodular basal cell carc<strong>in</strong>oma after <strong>in</strong>itial treatment<br />
with curettage. J Drugs Dermatol. 2007;6(9):910-4.<br />
35. Gaitanis G, Mitsou G, Tsiouri G, Alexis I, Bassukas ID. Cryosurgery dur<strong>in</strong>g<br />
imiquimod cream treatment (“immunocryosurgery”) for Bowen’s disease<br />
of the sk<strong>in</strong>: A case series. Acta Derm Venereol. 2010;90(5):533-4.<br />
36. MacFarlane DF, El Tal AK. Cryoimmunotherapy: Superficial basal cell<br />
cancer and squamous cell carc<strong>in</strong>oma <strong>in</strong> situ treated with liquid nitrogen followed<br />
by imiquimod. Arch Dermatol. 2011;147(11):1326-7.<br />
37. Rosen T, Hart<strong>in</strong>g M, Gibson M. <strong>Treatment</strong> of Bowen’s disease with topical<br />
5% imiquimod cream: Retrospective study. Dermatol Surg. 2007;33(4):427-432.<br />
38. Patel GK, Goodw<strong>in</strong> R, Chawla M, et al. Imiquimod 5% cream monotherapy<br />
for cutaneous squamous cell carc<strong>in</strong>oma <strong>in</strong> situ (Bowen’s disease):<br />
A randomized, double-bl<strong>in</strong>d, placebo-controlled trial. J Am Acad Dermatol.<br />
2006;54(6):1025-1032.<br />
39. Mackenzie-Wood A, Kossard S, de Launey J, Wilk<strong>in</strong>son B, Owens ML.<br />
Imiquimod 5% cream <strong>in</strong> the treatment of Bowen’s disease. J Am Acad Dermatol.<br />
2001;44:462-70.<br />
40. Von Hoff DD, LoRusso PM, Rud<strong>in</strong> CM, et al. Inhibition of the hedgehog<br />
pathway <strong>in</strong> advanced basal-cell carc<strong>in</strong>oma. N Engl J Med. 2009;361(12):1164-72.<br />
41. Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib<br />
<strong>in</strong> advanced basal-cell carc<strong>in</strong>oma. N Engl J Med. 2012;366(23):2171-9.<br />
42. Tang JY, Mackay-Wiggan JM, Aszterbaum M, et al. Inhibit<strong>in</strong>g the hedgehog<br />
pathway <strong>in</strong> patients with the basal cell nevus syndrome. N Engl J Med.<br />
2012;366(23):2180-2188.<br />
43. Bouwes Bav<strong>in</strong>ck JN, Tieben LM, van der Woude FJ, et al. Prevention of<br />
sk<strong>in</strong> cancer and reduction of keratotic sk<strong>in</strong> lesions dur<strong>in</strong>g acitret<strong>in</strong> therapy<br />
<strong>in</strong> renal transplant patients: A double-bl<strong>in</strong>d, placebo-controlled study. J Cl<strong>in</strong><br />
Oncol. 1995;13:1933-1938.<br />
44. George R, Weightman W, Russ GR, Bannister KM, Mathew TH. Acitret<strong>in</strong><br />
for chemoprevention of non-melanoma sk<strong>in</strong> cancers <strong>in</strong> renal transplant<br />
recipients. Australas J Dermatol. 2002;43:269–73.<br />
45. Chen K, Craig JC, Shumack S. Oral ret<strong>in</strong>oids for the prevention of sk<strong>in</strong><br />
cancers <strong>in</strong> solid organ transplant recipients: A systematic review of randomized<br />
controlled trials. Br J Dermatol. 2005;152(3):518-23.<br />
46. Campbell SB, Walker R, Tai SS, Jiang Q, Russ GR. Randomized controlled<br />
trial of sirolimus for renal transplant recipients at high risk for nonmelanoma<br />
sk<strong>in</strong> cancer. Am J Transplant. 2012 May;12(5):1146-56. doi:<br />
10.1111/j.1600-6143.2012.04004.x. Epub 2012 Mar 15.<br />
47. Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene <strong>in</strong> human<br />
cancer. Nature. 2002;417:949-54.<br />
48. Curt<strong>in</strong> JA, Fridlyand J, Kageshita T, et al. Dist<strong>in</strong>ct sets of genetic alterations<br />
<strong>in</strong> melanoma. N Engl J Med. 2005;353:2135-47.<br />
49. Zalla MJ, Lim KK, Dicaudo DJ, Gagnot MM. Mohs micrographic excision<br />
of melanoma us<strong>in</strong>g immunosta<strong>in</strong>s. Dermatol Surg. 2000;26(8):771-84.<br />
50. Shumaker PR, Kelley B, Swann MH, Greenway HT Jr. Modified Mohs<br />
micrographic surgery for periocular melanoma and melanoma <strong>in</strong> situ: Longterm<br />
experience at Scripps Cl<strong>in</strong>ic. Dermatol Surg. 2009;35(8):1263-70.<br />
51. Morton DL, Chan AD. <strong>The</strong> concept of sent<strong>in</strong>el node localization: How it<br />
started. Sem<strong>in</strong> Nucl Med. 2000;30:4-10.<br />
52. Morton DL, Thompson JF, Cochran AJ, et al. Sent<strong>in</strong>el-node biopsy or<br />
nodal observation <strong>in</strong> melanoma. N Engl J Med. 2006;355(13):1307-17.<br />
53. Erickson C, Miller SJ. <strong>Treatment</strong> options <strong>in</strong> melanoma <strong>in</strong> situ: Topical<br />
and radiation therapy, excision and Mohs surgery. Int J Dermatol.<br />
2010;49(5):482-91.<br />
54. Farshad A, Burg G, Panizzon R, Dummer R. A retrospective study<br />
of 150 patients with lentigo maligna and lentigo maligna melanoma and<br />
the efficacy of radiotherapy us<strong>in</strong>g Grenz or soft X-rays. Br J Dermatol.<br />
2002;146(6):1042-6.<br />
55. Schmid-Wendtner MH, Brunner B, Konz B, et al. Fractionated radiotherapy<br />
of lentigo maligna and lentigo maligna melanoma <strong>in</strong> 64 patients. J Am<br />
Acad Dermatol. 2000;43(3):477-82.<br />
56. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab<br />
<strong>in</strong> patients with metastatic melanoma. N Engl J Med. 2010;363:711-23.<br />
57. Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbaz<strong>in</strong>e for<br />
previously untreated metastatic melanoma. N Engl J Med. 2011;364(26):2517-26.<br />
58. Bollag G, Hirth P, Tsai J, et al. Cl<strong>in</strong>ical efficacy of a RAF <strong>in</strong>hibitor needs<br />
broad target blockade <strong>in</strong> BRAF-mutant melanoma. Nature. 2010;467:596-9.<br />
59. Chapman PB, Hauschild A, Robert C, et al. Improved survival with<br />
vemurafenib <strong>in</strong> melanoma with BRAF V600E mutation. N Engl J Med.<br />
2011;364:2507-16.<br />
60. Sosman JA, Jim KB, Schuchter L, et al. Survival <strong>in</strong> BRAF V600-mutant advanced<br />
melanoma treated with vemurafenib. N Engl J Med. 2012;366:707-14.<br />
32 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis<br />
<strong>Treatment</strong>: More Than Just Steroids<br />
As the cause of the condition is considered multifactorial, the treatment plan should <strong>in</strong>clude comb<strong>in</strong>ation<br />
therapies and avoidance of triggers.<br />
Megan A. K<strong>in</strong>ney, MD, MHAM<br />
Atopic dermatitis is a common chronic or chronically<br />
relaps<strong>in</strong>g <strong>in</strong>flammatory sk<strong>in</strong> disease that affects<br />
approximately 18% to 25% of the pediatric<br />
population and causes psychosocial morbidity,<br />
impaired quality of life and a heavy economic burden. <strong>The</strong><br />
disease presents with pruritus plus an eruption consist<strong>in</strong>g<br />
of scaly to lichenified plaques most commonly manifest<strong>in</strong>g<br />
<strong>in</strong> the sk<strong>in</strong> creases (although <strong>in</strong> <strong>in</strong>fants it is more common<br />
on the face), and, generally dry sk<strong>in</strong> and possible associated<br />
allergic symptoms (see Figures 1 and 2). In fact,<br />
the progression from atopic dermatitis to asthma to allergic<br />
rh<strong>in</strong>itis is called the “atopic march,” though patients can<br />
present with these conditions <strong>in</strong> any order or all at once.<br />
While AD much more characteristically develops <strong>in</strong> childhood,<br />
a small portion of patients may develop the disease<br />
<strong>in</strong> adulthood. AD can be associated with elevated IgE levels<br />
and multiple gene mutations that can cause changes <strong>in</strong><br />
the sk<strong>in</strong> barrier itself. <strong>The</strong> condition is likely a product of<br />
gene-environment <strong>in</strong>teraction.<br />
Traditional treatment of AD is multifactorial and based on<br />
severity. Patients should avoid triggers such as allergens, rough<br />
cloth<strong>in</strong>g, stressors and bacteria on the sk<strong>in</strong> through the use of<br />
bleach baths and antibacterial soaps, and practice good sk<strong>in</strong><br />
care habits with frequent application of emollients and use of<br />
mild soaps. For the aforementioned plaques, topical corticosteroids<br />
are first-l<strong>in</strong>e treatment with potency based on severity<br />
and thickness of plaques. Most agree that supplementation of<br />
topical calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors like pimecrolimus and tacrolimus,<br />
can aid <strong>in</strong> long-term management of moderate AD. Light<br />
therapy may also be of benefit. For severe recalcitrant AD,<br />
oral systemic medications may be necessary, with cyclospor<strong>in</strong>,<br />
azathiopr<strong>in</strong>e, mycophenolate mofetil and methotrexate<br />
used most commonly. Smaller numbers of patients have also<br />
been treated with biologics. Prednisone is generally not recommended<br />
for AD unless done <strong>in</strong> a shorter taper to another<br />
steroid-spar<strong>in</strong>g systemic agent, given its side effect profile and<br />
propensity to cause AD to flare more severely with its discont<strong>in</strong>uation.<br />
Multiple <strong>in</strong>tegrative treatments are also employed <strong>in</strong><br />
the treatment of AD. 1<br />
A review of current literature shows that current studies<br />
trend away from topical steroids and toward novel modalities,<br />
Figure 1. Lichenified, excoriated eczematous plaques<br />
<strong>in</strong> a child with atopic dermatitis.<br />
Figure 2. <strong>The</strong> antecubital region is a common place<br />
for atopic dermatitis.<br />
some of which may be unexpected. S<strong>in</strong>ce the cause of the<br />
disease is considered multifactorial, a treatment plan should be<br />
implemented <strong>in</strong> lieu of a s<strong>in</strong>gle miracle cream. This article will<br />
explore these current trends <strong>in</strong> categories.<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 33
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
Am<strong>in</strong>o acids<br />
Filaggr<strong>in</strong><br />
Endoproteases<br />
Profilaggr<strong>in</strong><br />
Stratum corneum<br />
Granular layer<br />
Sp<strong>in</strong>ous layer<br />
Cornified cell envelope<br />
-80% Loricr<strong>in</strong><br />
-Involucr<strong>in</strong><br />
Lipid bilayer<br />
Corneocyte<br />
Corneodesmosomes<br />
Lamellar granules<br />
-Lipid precursors<br />
-Antimicrobial peptides<br />
-Proteases<br />
Basal layer<br />
Figure 3. Sk<strong>in</strong> Barrier<br />
With<strong>in</strong> the stratum corneum, the lipid bilayer between the corneocytes is created by planar lamellae sheets<br />
of ceramides, cholesterol and free fatty acids. With<strong>in</strong> the cornified cell envelope is loricr<strong>in</strong> and <strong>in</strong>volucr<strong>in</strong>.<br />
Profilaggr<strong>in</strong> is cleaved by proteases at the junction of the granular layer and the stratum corneum to create<br />
filaggr<strong>in</strong> which bundles kerat<strong>in</strong> and flattens corneocytes. <strong>The</strong> filaggr<strong>in</strong> is then broken down <strong>in</strong>to am<strong>in</strong>o acids which<br />
aid <strong>in</strong> reta<strong>in</strong><strong>in</strong>g moisture. Corneodesmosomes create the tight junctions hold<strong>in</strong>g the corneocytes together.<br />
Sk<strong>in</strong> Barrier<br />
Protect<strong>in</strong>g and rebuild<strong>in</strong>g the sk<strong>in</strong> barrier has become<br />
part of the bread-and-butter treatment regimen for atopic<br />
dermatitis. Many patients with AD have been shown to have<br />
a mutation <strong>in</strong> FLG, which codes for filaggr<strong>in</strong>, which aggregates<br />
kerat<strong>in</strong>, a large component of the stratum corneum<br />
(see Figure 3). In between the cells of the epidermis, the<br />
kerat<strong>in</strong>ocytes, there are lipid molecules — <strong>in</strong>clud<strong>in</strong>g ceramides<br />
— that fill <strong>in</strong> the gaps and help to ma<strong>in</strong>ta<strong>in</strong> the barrier.<br />
With less filaggr<strong>in</strong>, the barrier becomes broken allow<strong>in</strong>g for<br />
water loss and the entry of antigens and <strong>in</strong>fectious organisms.<br />
Recent studies have demonstrated that apply<strong>in</strong>g ceramide-conta<strong>in</strong><strong>in</strong>g<br />
emollients can help restore the sk<strong>in</strong> barrier.<br />
<strong>The</strong>se studies evaluated the ceramide topical <strong>in</strong> all age<br />
groups, but a recent study evaluated this topical solely <strong>in</strong> the<br />
pediatric population and further supported <strong>in</strong>corporation<br />
of ceramide-dom<strong>in</strong>ant topicals as an <strong>in</strong>tegral component <strong>in</strong><br />
AD therapy either as monotherapy or comb<strong>in</strong>ation therapy. 2<br />
<strong>The</strong>se topicals not only replace what is lost; they actually<br />
improve kerat<strong>in</strong>ocyte lipid biosynthesis, which may further<br />
improve the epidermal barrier. 3 This molecule has so far<br />
only been available <strong>in</strong> lotion or cream form, but recently a<br />
ceramide hyaluronic acid foam has been developed that may<br />
have the benefits of ceramides with <strong>in</strong>creased compliance<br />
given the foam vehicle. 4 Alternatively, patients may be able<br />
to obta<strong>in</strong> the benefits of ceramides even without apply<strong>in</strong>g<br />
a topical therapy. Consum<strong>in</strong>g dietary sph<strong>in</strong>golipids has suggested<br />
an upregulation <strong>in</strong> the synthesis of ceramides <strong>in</strong> sk<strong>in</strong>. 5<br />
Also, an oral collagen tripeptide has undergone <strong>in</strong>itial animal<br />
studies and shown improvement <strong>in</strong> sk<strong>in</strong> dryness. 6<br />
While ceramides have been the primary focus, other possible<br />
molecules to enhance the sk<strong>in</strong> barrier are also be<strong>in</strong>g<br />
studied. Topical urea may enhance barrier function because it<br />
has anti-microbial properties; it also upregulates filaggr<strong>in</strong> and<br />
production of other components of the sk<strong>in</strong> barrier. 7<br />
Recent studies suggest that upregulat<strong>in</strong>g filaggr<strong>in</strong> levels <strong>in</strong><br />
the sk<strong>in</strong> by 5% to 10% may improve cl<strong>in</strong>ical management of<br />
patients with AD; this may, therefore, become a more focused<br />
therapeutic target for treatment. Several compounds already<br />
shown to <strong>in</strong>crease FLG gene expression <strong>in</strong>clude oleanolic<br />
acid and ursolic acid. 8<br />
While FLG is most prom<strong>in</strong>ent <strong>in</strong> the literature, known upregulated<br />
genes <strong>in</strong> AD <strong>in</strong>clude <strong>in</strong>volucr<strong>in</strong>, a small prote<strong>in</strong>-rich<br />
region (SPRR) 2C gene and alternative pathway kerat<strong>in</strong> 16.<br />
All were shown to be decreased <strong>in</strong> lesional sk<strong>in</strong> after treatment<br />
with pimecrolimus. <strong>Treatment</strong>s target<strong>in</strong>g genes lends to<br />
a new avenue to improve the sk<strong>in</strong> barrier. 9<br />
Lastly, recent studies <strong>in</strong> standard treatments of care have determ<strong>in</strong>ed<br />
that while topical corticosteroids may be a more<br />
effective anti-<strong>in</strong>flammatory, they reduce the rate limit<strong>in</strong>g enzymes<br />
for lipid synthesis and the expression of <strong>in</strong>volucr<strong>in</strong> and<br />
SPRRs <strong>in</strong> the sk<strong>in</strong> (which covalently b<strong>in</strong>ds ceramides), thus<br />
<strong>in</strong>hibit<strong>in</strong>g the restoration of the sk<strong>in</strong> barrier. This confirms<br />
that calc<strong>in</strong>eur<strong>in</strong> <strong>in</strong>hibitors (such as pimecrolimus, which was<br />
the comparison treatment <strong>in</strong> this study) are a better option for<br />
long-term ma<strong>in</strong>tenance therapy. 10<br />
Fight<strong>in</strong>g Infectious Organisms<br />
Breakdown of the sk<strong>in</strong> barrier allows easier access for <strong>in</strong>fectious<br />
organisms. Practitioners offer many recommendations<br />
34 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
for decreas<strong>in</strong>g bacteria generally on the sk<strong>in</strong>, <strong>in</strong>clud<strong>in</strong>g antibacterial<br />
soaps, oral and topical antibiotics and bleach baths.<br />
Children with atopic dermatitis have been found to be<br />
more prone to <strong>in</strong>fectious diseases <strong>in</strong> general; they are more<br />
frequently hospitalized than children without AD, and the<br />
most common reason for hospitalization is pneumonia. Children<br />
with AD also commonly suffer from chronic diarrhea,<br />
and studies have confirmed that Staphylococcus aureus is more<br />
commonly found <strong>in</strong> their stool. Some believe that S. aureus <strong>in</strong><br />
the GI tract can stimulate atopic sk<strong>in</strong> changes. 11<br />
Probiotic supplementation has been suggested as a way to<br />
deliver additional microorganisms to the GI tract and, <strong>in</strong> several<br />
studies, have been shown to prevent AD. 12,13 Addition of<br />
other microorganisms may aid <strong>in</strong> elim<strong>in</strong>at<strong>in</strong>g the <strong>in</strong>test<strong>in</strong>al<br />
overgrowth of S. aureus. Follow<strong>in</strong>g a similar belief, Jang et al<br />
argue that the addition of lactic acid bacteria (LAB) may also<br />
aid <strong>in</strong> prevention and treatment of allergic diseases. Previous<br />
studies have shown the LAB, Lactobacillus plantarum, isolated<br />
from the traditional Korean food kimchi, reduce allergen-<strong>in</strong>duced<br />
airway hypersensitivity and histam<strong>in</strong>e release. By isolat<strong>in</strong>g<br />
Lactobacillus plantarum K-1, they found that pro<strong>in</strong>flammatory<br />
cytok<strong>in</strong>es and scratch<strong>in</strong>g behavior <strong>in</strong> mice was reduced,<br />
<strong>in</strong>dicat<strong>in</strong>g this may be a future treatment for allergic conditions<br />
such as AD. 14<br />
While the changes <strong>in</strong> the gut mentioned above are new<br />
discoveries, it is well known that high levels of S. aureus are<br />
found on the sk<strong>in</strong> of patients with atopic dermatitis. A recent<br />
study analyzed the susceptibilities of the S.aureus isolated on<br />
patients with super<strong>in</strong>fected AD versus controls and found that<br />
there is <strong>in</strong>creased resistance to cl<strong>in</strong>damyc<strong>in</strong> (the most commonly<br />
prescribed antibiotic for these patients) on the sk<strong>in</strong> of<br />
patients with AD <strong>in</strong> comparison to controls. This may lead to<br />
changes <strong>in</strong> cl<strong>in</strong>ical practice to prescribe someth<strong>in</strong>g else like<br />
trimethoprim/sulfmethoxazole as a first l<strong>in</strong>e empiric antimicrobial<br />
choice, although culture-driven antibiotic choices for<br />
super<strong>in</strong>fected AD should be encouraged. 15<br />
However, others do not necessarily recommend the use of<br />
oral antibiotics for secondarily impetig<strong>in</strong>ized AD, even with<br />
culture-proven MRSA. In an argument support<strong>in</strong>g decreased<br />
antimicrobial peptides associated with AD, one group treated<br />
patients with impetig<strong>in</strong>ized AD with a comb<strong>in</strong>ation therapy<br />
of topical corticosteroids, antihistam<strong>in</strong>es and oral cephalex<strong>in</strong><br />
(which would not cover MRSA). <strong>The</strong>y saw improvement<br />
even <strong>in</strong> patients harbor<strong>in</strong>g cephalex<strong>in</strong>-resistent MRSA. This<br />
supports the belief that S. aureus is a trigger for AD and that<br />
calm<strong>in</strong>g <strong>in</strong>flammation restores natural anti-microbial peptides<br />
(AMPs) that can then adequately fight off the secondary impetig<strong>in</strong>ization.<br />
This was supported by a quantified <strong>in</strong>crease <strong>in</strong><br />
defens<strong>in</strong>s after treatment. 16<br />
A new alternative that may be on the horizon is the addition<br />
of an antimicrobial component to cloth<strong>in</strong>g. In one study,<br />
chitosan was <strong>in</strong>corporated <strong>in</strong>to cotton cloth<strong>in</strong>g. <strong>The</strong> chitosanimpregnated<br />
cloth<strong>in</strong>g significantly reduced S. aureus bacterial<br />
content specifically and not all bacteria. 17<br />
In addition to secondary <strong>in</strong>fection by bacteria, viral exanthems<br />
may also be associated with eczema; molluscum<br />
contagiosum is commonly seen <strong>in</strong> conjunction with atopic<br />
dermatitis. In some patients, this eczematous eruption may<br />
be a secondary id reaction to the primary <strong>in</strong>fection. Given<br />
the vicious cycle of topical steroids caus<strong>in</strong>g progression of<br />
the molluscum when try<strong>in</strong>g to treat the associated eczematous<br />
reaction, it is recommended to treat the id reaction with<br />
topical emollients. If patients are severely symptomatic, short<br />
courses of topical steroids may be used, but limit<strong>in</strong>g their<br />
duration is important, as steroid use can delay the resolution<br />
of molluscum contagiosum. 18<br />
Environment<br />
While environment provides the source for all <strong>in</strong>fectious<br />
agents, it can also affect patients with AD <strong>in</strong> other ways. Epidemiologic<br />
studies have shown that higher-<strong>in</strong>come countries<br />
have a decreased frequency of <strong>in</strong>fections and an <strong>in</strong>creased rate<br />
of allergic diseases. 12 Some argue that better hygiene has led<br />
to less exposure to antigens early <strong>in</strong> life.<br />
In addition to frequency, a recently published questionnaire<br />
study revealed several environmental factors associated<br />
with severity of AD. Though a causal relationship could not<br />
be demonstrated, these environmental factors could perhaps<br />
trigger an <strong>in</strong>dividual’s genetic predisposition for the disease.<br />
Factors associated with AD severity <strong>in</strong>cluded <strong>in</strong>door remodel<strong>in</strong>g,<br />
those liv<strong>in</strong>g <strong>in</strong> an apartment, higher household <strong>in</strong>come<br />
and higher educational status of the mother. 19 Another study<br />
found that, <strong>in</strong> children with AD, cat and daycare exposure actually<br />
reduced the risk of develop<strong>in</strong>g asthma <strong>in</strong> early childhood.<br />
20 Another study showed allergic AD may be more of<br />
a result of house mites enter<strong>in</strong>g through the defective sk<strong>in</strong><br />
barrier, stimulat<strong>in</strong>g an immune response. <strong>The</strong>re is much controversy<br />
over whether food allergies contribute to AD; this<br />
will be discussed <strong>in</strong> a later section. 21<br />
<strong>The</strong> use of humidifiers is often recommended, as they can<br />
moisten the dry air, especially associated with heat<strong>in</strong>g, <strong>in</strong> the<br />
home. Studies from Korea discuss an <strong>in</strong>stance where biocides<br />
mixed <strong>in</strong> the water of humidifiers caused a fatal pulmonary<br />
syndrome <strong>in</strong> both children and pregnant women. While it is<br />
not suggested that patients are at risk for <strong>in</strong>haled biocides, it<br />
is important for the cl<strong>in</strong>ician to remember that patients with<br />
AD may have more of a chance of exposure to humidified<br />
aerosols when compared with the general population. 22<br />
Psychological Issues<br />
Sleep Deprivation<br />
AD is not just a sk<strong>in</strong> disease. <strong>The</strong> pruritus associated with<br />
AD and the appearance of sk<strong>in</strong> lesions can have a significant<br />
impact psychologically. Recent studies <strong>in</strong> itch with AD confirm<br />
that <strong>in</strong>tensity of pruritus correlated with decl<strong>in</strong><strong>in</strong>g quality<br />
of life and depressive symptoms. In addition, patients experienc<strong>in</strong>g<br />
sleep deprivation with AD attributed it to nighttime<br />
itch. Sleep deprivation can even occur at the onset of the<br />
disease. 23 Use of sleep<strong>in</strong>g pills has been shown to improve<br />
quality of life and depressive symptoms greatly. 24<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 35
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
ADHD<br />
A study <strong>in</strong> Taiwan recently found an <strong>in</strong>creased risk of attention-deficit/hyperactivity<br />
disorder (ADHD) <strong>in</strong> patients<br />
with pediatric allergy disorders. Of note, the ma<strong>in</strong> contribut<strong>in</strong>g<br />
disorder was allergic rh<strong>in</strong>itis, but bronchial asthma was<br />
also determ<strong>in</strong>ed to be a risk factor for ADHD. Atopic dermatitis<br />
was only determ<strong>in</strong>ed to be a risk factor <strong>in</strong> association<br />
with allergic rh<strong>in</strong>itis but was not an <strong>in</strong>dependent risk factor.<br />
25 Because of the atopic triad, cl<strong>in</strong>icians should be aware<br />
of this psychiatric co-association.<br />
Stress<br />
While there are no randomized controlled studies,<br />
stress has been suspected to worsen AD. Multiple techniques<br />
of relaxation are present <strong>in</strong> the literature <strong>in</strong>clud<strong>in</strong>g<br />
massage, hypnosis, biofeedback and progressive muscle<br />
relaxation. Small studies have <strong>in</strong>dicated improvement<br />
<strong>in</strong> AD with massage. 13<br />
One study looked at Dead Sea climatotherapy. In this study,<br />
patients were treated at a spa hotel near the Dead Sea. <strong>Treatment</strong><br />
consisted of bath<strong>in</strong>g <strong>in</strong> the Dead Sea and then expos<strong>in</strong>g<br />
the sk<strong>in</strong> to UV radiation. <strong>The</strong> treatment environment was also<br />
kept stress-free. Us<strong>in</strong>g the SCORAD <strong>in</strong>dex for disease severity<br />
and the Sk<strong>in</strong>dex-29 score for quality of life, the treatment<br />
regimen did show significant improvement <strong>in</strong> both modalities,<br />
but confound<strong>in</strong>g variables such as feel<strong>in</strong>g as though one<br />
is on vacation may skew these results. 26<br />
In addition to caus<strong>in</strong>g<br />
the patient psychological<br />
distress, AD also causes<br />
family stress.<br />
In addition to caus<strong>in</strong>g the patient psychological distress,<br />
AD also causes the family stress. Patient education programs<br />
have shown to be successful <strong>in</strong> improv<strong>in</strong>g patient disease and<br />
psychological well be<strong>in</strong>g. Schut et al recently demonstrated<br />
that parents with little social support or parents with high<br />
active problem solv<strong>in</strong>g behavior would likely benefit more<br />
from such programs and that such patients and their parents<br />
should be offered this additional education for greater success<br />
<strong>in</strong> treat<strong>in</strong>g AD. 27<br />
Positive Re<strong>in</strong>forcement<br />
Because AD is more commonly a pediatric disease, psychological<br />
approaches to treatment should also take the<br />
child’s m<strong>in</strong>dset <strong>in</strong>to account. Most children strongly dislike<br />
the sticky o<strong>in</strong>tments and gooey creams prescribed. Poor adherence<br />
to topical treatments leads to worse outcomes and<br />
possibly progression to a systemic medication with greater<br />
side effects. Us<strong>in</strong>g positive re<strong>in</strong>forcement techniques may<br />
<strong>in</strong>crease motivation to use topical medications. For example,<br />
sticker charts have been shown to improve outcomes <strong>in</strong> other<br />
chronic diseases that require long-term compliance with<br />
treatment regimens. 28<br />
Integrative Medic<strong>in</strong>e<br />
<strong>The</strong>re are scores of recommendations when one considers<br />
<strong>in</strong>tegrative treatments. We will focus on some of the most<br />
recent research on oatmeal, silk, cloth<strong>in</strong>g and traditional Ch<strong>in</strong>ese<br />
medic<strong>in</strong>e (TCM).<br />
Oatmeal<br />
Oatmeal has been shown to <strong>in</strong>herently possess antioxidant<br />
and anti-<strong>in</strong>flammatory properties, and studies have shown<br />
that us<strong>in</strong>g a topical formulation of colloidal oatmeal, avenanthramide,<br />
restores the cutaneous barrier, alleviat<strong>in</strong>g symptoms.<br />
Some studies offer this as adjunctive treatment to limit topical<br />
steroids, but others suggest that apply<strong>in</strong>g oatmeal to a damaged<br />
epidermal barrier may lead to oat allergy. 29-32<br />
Silk and Other Textiles<br />
Silk and similar materials have been a ma<strong>in</strong>stay <strong>in</strong> <strong>in</strong>tegrative<br />
medic<strong>in</strong>e. Recently, oral adm<strong>in</strong>istration of silk peptides to mice<br />
was shown to decrease IgE levels <strong>in</strong> an atopic dermatitis mouse<br />
model. This may be an <strong>in</strong>dication that silk has the ability to modulate<br />
the immunological T-helper cell (Th1/Th2) balance. 33<br />
Studies have also looked at more traditional use of silk as<br />
textiles. Certa<strong>in</strong> fabrics can be irritat<strong>in</strong>g to the sk<strong>in</strong>. Some have<br />
proposed silk as a softer alternative; <strong>in</strong> atopic dermatitis, however,<br />
this textile is not always practical, as it can reduce transpiration<br />
and may still cause irritation. Knitted silk alternatives,<br />
however, some impregnated with an antimicrobial component,<br />
have been shown to, at times, demonstrate a reduction <strong>in</strong> pruritus<br />
and severity of AD by SCORAD <strong>in</strong>dex. This <strong>in</strong>itial success<br />
spawned the development of a synthetic silk-like fabric, which<br />
has been cleared by the FDA as a Class I medical device for use<br />
by patients with AD. <strong>The</strong> fabric is even be<strong>in</strong>g used <strong>in</strong> bedd<strong>in</strong>g<br />
and has been marketed to prevent bacterial <strong>in</strong>fections (as they<br />
have an antimicrobial coat<strong>in</strong>g), absorb perspiration and serous<br />
exudates and reduce sk<strong>in</strong> irritation. lead<strong>in</strong>g to reduced disease<br />
severity and pruritus and improved quality of life. 34<br />
A silver-loaded cellulose fabric with <strong>in</strong>corporated seaweed<br />
was also shown to decrease the modified SCORAD atopic<br />
dermatitis <strong>in</strong>dex, trans-epidermal water loss and the patient’s<br />
subjective severity of their AD compared to cotton cloth<strong>in</strong>g. 35<br />
Traditional Ch<strong>in</strong>ese Medic<strong>in</strong>e<br />
<strong>The</strong>re has been an <strong>in</strong>creas<strong>in</strong>g trend <strong>in</strong> medic<strong>in</strong>e to use herbal<br />
medications. and trends <strong>in</strong> the treatment of atopic dermatitis<br />
are no different. TCM is based <strong>in</strong> more than 2,000 years<br />
of experience <strong>in</strong> herbal medic<strong>in</strong>es, acupuncture, massage and<br />
36 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
diet. <strong>The</strong> difficulties with exam<strong>in</strong><strong>in</strong>g the safety and efficacy of<br />
the medications is that many herbs are comb<strong>in</strong>ed and dosed<br />
differently with each <strong>in</strong>dividual patient, mak<strong>in</strong>g randomized<br />
controlled studies difficult. Standardized treatment across the<br />
board contra<strong>in</strong>dicates the <strong>in</strong>dividualized treatment that is the<br />
basis of TCM. Of the randomized controlled studies that do<br />
exist, some benefit has been seen and most authors offer TCM<br />
as an alternative treatment for refractory AD. It must be noted<br />
that TCM can still have adverse effects. <strong>The</strong> most common side<br />
effect with oral medications was an elevation <strong>in</strong> liver function<br />
tests. Also, secondary to a lack of monitor<strong>in</strong>g by the FDA, some<br />
topical formulations have actually been found to conta<strong>in</strong> dexamethasone<br />
at vary<strong>in</strong>g concentrations with no <strong>in</strong>dication on the<br />
label that they <strong>in</strong>clude corticosteroids. Some were even found<br />
to have concentrations of topical corticosteroids higher than<br />
the highest potency steroid available <strong>in</strong> the United States. This<br />
could be hazardous, especially if used <strong>in</strong> conjunction with a<br />
potent prescribed topical steroid. 13 A novel herbal medication,<br />
KIOM-MA and its fermented product, KIOM-MA128, consist<br />
of a mixture of herbs <strong>in</strong>clud<strong>in</strong>g Glycyrrhizae radix, Polygoni<br />
cuspidati rhizoma, Sophorae radix, Cnidii rhizoma, and Arctii fructus.<br />
This oral medication was tested <strong>in</strong> an atopic dermatitis mouse<br />
model and was shown to improve AD by decreas<strong>in</strong>g plasma IgE,<br />
scratch<strong>in</strong>g behavior and sk<strong>in</strong> severity. <strong>The</strong> fermented version<br />
was found to actually be more effective. Topical formulations<br />
are also <strong>in</strong> development. 36<br />
Nutrition<br />
Nutrition and its relationship with AD is a controversial<br />
topic with dermatologists and primary care physicians. In<br />
the literature, discrepancies rema<strong>in</strong> about when to <strong>in</strong>troduce<br />
new foods and which foods to expose to the newborn.<br />
Roduit et al found that <strong>in</strong>troduction of diverse complementary<br />
foods and yogurt with<strong>in</strong> the first year of life actually<br />
might have a protective effect aga<strong>in</strong>st the development of<br />
AD. A reduction <strong>in</strong> the risk of AD onset after the first year of<br />
life was found. 37 Early <strong>in</strong>troduction of cow’s milk and different<br />
<strong>in</strong>fant formulas and their association with the development<br />
of AD is also controversial. For breast-feed<strong>in</strong>g mothers,<br />
maternal diet supplementation has also been <strong>in</strong>vestigated.<br />
Upon review of current literature, the American Academy<br />
of Pediatrics suggests that lactat<strong>in</strong>g mothers avoid peanuts<br />
and tree nuts <strong>in</strong> <strong>in</strong>fants with a high risk for develop<strong>in</strong>g AD.<br />
<strong>The</strong>y should also consider elim<strong>in</strong>ation of eggs, cow’s milk<br />
and fish. <strong>The</strong> World Health Organization (WHO) recommends<br />
breastfeed<strong>in</strong>g children up to age 2. Limited research<br />
<strong>in</strong> the area has not determ<strong>in</strong>ed whether or not breastfeed<strong>in</strong>g<br />
has a protective role aga<strong>in</strong>st development of AD. 38<br />
A recent review of studies us<strong>in</strong>g dietary supplements <strong>in</strong><br />
children with atopic dermatitis unfortunately showed no<br />
benefit <strong>in</strong> improv<strong>in</strong>g AD with oral supplementation of olive<br />
oil, corn oil, oral z<strong>in</strong>c sulphate, selenium, selenium plus vitam<strong>in</strong><br />
E, vitam<strong>in</strong> D, sea buckthorn seed oil, sea buckthorn pulp<br />
oil, hempseed oil, sunflower oil and DHA. Two small studies<br />
with fish oil did <strong>in</strong>dicate some slight improvement <strong>in</strong> pruritus<br />
and quality of life with AD, but larger trials would have to<br />
be completed to make any recommendations to the general<br />
public. 39 Another study showed that a comb<strong>in</strong>ation supplement<br />
conta<strong>in</strong><strong>in</strong>g five polyunsaturated fatty acids, vitam<strong>in</strong> C,<br />
vitam<strong>in</strong> E and z<strong>in</strong>c demonstrated significant improvement <strong>in</strong><br />
patient symptoms. <strong>The</strong> idea beh<strong>in</strong>d supplement<strong>in</strong>g polyunsaturated<br />
fatty acids is that they have been employed <strong>in</strong> restor<strong>in</strong>g<br />
the stratum corneum and sk<strong>in</strong> barrier. 13 Other supplements<br />
such as vitam<strong>in</strong> B6, vitam<strong>in</strong> D, folic acid, vitam<strong>in</strong><br />
B12 and z<strong>in</strong>c have been studied <strong>in</strong> solitary. Vitam<strong>in</strong> B6 or<br />
Nutrition and its<br />
relationship with AD is a<br />
controversial topic with<br />
dermatologists and primary<br />
care physicians.<br />
pyroxid<strong>in</strong>e is an essential cofactor for many biochemical reactions<br />
<strong>in</strong> the body and it was suspected that a diet deficient<br />
<strong>in</strong> this vitam<strong>in</strong> might lead to AD. While deficiencies themselves<br />
were not studied, there was no improvement <strong>in</strong> AD<br />
with supplementation of vitam<strong>in</strong> B6. Vitam<strong>in</strong> D has been<br />
thought to be promis<strong>in</strong>g <strong>in</strong> the treatment of AD, as it can<br />
<strong>in</strong>duce kerat<strong>in</strong>ocytes, <strong>in</strong>crease synthesis of platelet-derived<br />
growth factor, facilitate wound heal<strong>in</strong>g, decrease synthesis of<br />
<strong>in</strong>flammatory cytok<strong>in</strong>es, and promote cathelicid<strong>in</strong> expression.<br />
Studies have confirmed that patients with milder AD<br />
do have higher levels of vitam<strong>in</strong> D and that supplement<strong>in</strong>g<br />
vitam<strong>in</strong> D stimulates production of cathelicid<strong>in</strong>. However,<br />
there have been <strong>in</strong>consistencies with both supplementation<br />
of vitam<strong>in</strong> D for treatment of AD and vitam<strong>in</strong> D deficiency<br />
associated with AD. 40<br />
Another study looked at folic acid versus IgE levels <strong>in</strong> patients<br />
with atopic dermatitis. IgE levels were correlated with<br />
AD severity and were most <strong>in</strong>creased <strong>in</strong> patients with allergic<br />
rh<strong>in</strong>itis. Previous studies have suggested that low serum folate<br />
levels may contribute to the risk of high IgE levels. This study,<br />
however, did not f<strong>in</strong>d similar results, although patients with<br />
AD did have lower levels of folic acid than controls. More<br />
studies would need to be done <strong>in</strong> order to recommend folic<br />
acid supplementation <strong>in</strong> patients with AD. 41 Kiefte-de Jong<br />
looked at plasma levels of both folic acid and vitam<strong>in</strong> B-12<br />
dur<strong>in</strong>g pregnancy and found that elevations dur<strong>in</strong>g the first<br />
trimester were associated with the development of atopic dermatitis<br />
<strong>in</strong> offspr<strong>in</strong>g, but not wheez<strong>in</strong>g or shortness of breath.<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 37
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
Though similar studies have shown conflict<strong>in</strong>g results, they<br />
br<strong>in</strong>g to light that this should be taken <strong>in</strong>to consideration<br />
before <strong>in</strong>stitution of government-mandated folic acid fortification.<br />
42 Vitam<strong>in</strong> B12 or cobalam<strong>in</strong> has also been theorized to<br />
treat AD through its known function of suppress<strong>in</strong>g <strong>in</strong>flammatory<br />
cytok<strong>in</strong>es. A study with topical vitam<strong>in</strong> B12 demonstrated<br />
improvement <strong>in</strong> AD. It has also been suggested that<br />
patients with AD may have decreased z<strong>in</strong>c levels.<br />
New Tricks<br />
Pruritus, which is commonly associated with AD, can<br />
be difficult to control. Oral antihistam<strong>in</strong>es are not usually<br />
effective, as the itch associated with AD is not generally<br />
mediated by histam<strong>in</strong>e release. Topical corticosteroids<br />
are also not always effective and there is the added effect<br />
of th<strong>in</strong>n<strong>in</strong>g the normal sk<strong>in</strong> with chronic use. Chronic<br />
itch<strong>in</strong>g can cause atopic dermatitis to worsen, re-start<strong>in</strong>g<br />
the itch-scratch cycle after <strong>in</strong>duction therapy is complete.<br />
Takeuci et al compared the use of tacrolimus versus emollients<br />
as ma<strong>in</strong>tenance therapy <strong>in</strong> patients who had already<br />
undergone <strong>in</strong>duction therapy with topical steroids. <strong>The</strong>y<br />
found that 100% of the emollient group had recurrence of<br />
pruritus, while only 24% of the tacrolimus group did. This<br />
argues that tacrolimus may be a better option for ma<strong>in</strong>tenance<br />
therapy <strong>in</strong> patients with AD. 43<br />
Tacrolimus is already a ma<strong>in</strong>stay treatment <strong>in</strong> AD as a<br />
non-steroid o<strong>in</strong>tment that does not have the same side effect<br />
profile as topical steroids. Despite this, patients have<br />
difficulty apply<strong>in</strong>g the sticky o<strong>in</strong>tment and some compla<strong>in</strong><br />
of local side effects like burn<strong>in</strong>g, warmth and redness with<br />
the medication. To alleviate some of these local side effects,<br />
a study compared tacrolimus-loaded lipid-nanoparticles<br />
head-to-head with standard tacrolimus. <strong>The</strong> tacrolimusloaded<br />
lipid-nanoparticles better targeted the deeper layers<br />
of the sk<strong>in</strong>, which is desirable. <strong>The</strong> worry with deeper<br />
penetration is more systemic side effects, but this didn’t<br />
seem to be the case <strong>in</strong> animal models. <strong>The</strong>se nanoparticles,<br />
which were delivered <strong>in</strong> a gel vehicle, may be a better alternative<br />
to a greasy o<strong>in</strong>tment. 44<br />
Ustek<strong>in</strong>umab, a relatively new biologic FDA-approved for<br />
psoriasis, is a monoclonal antibody with aff<strong>in</strong>ity for the p40<br />
subunit of <strong>in</strong>terleuk<strong>in</strong> 12 (IL-12) and IL-23. <strong>The</strong>se <strong>in</strong>terleuk<strong>in</strong>s<br />
promote proliferation of IL-17 through stimulation of<br />
T-helper 17 (TH17) cells. AD is also associated with TH17<br />
cells, possibly suggest<strong>in</strong>g a common pathway for both <strong>in</strong>flammatory<br />
conditions. Puja et al speculated this to be the<br />
case and had success <strong>in</strong> treat<strong>in</strong>g one patient with resistant<br />
AD with ustek<strong>in</strong>umab. 45<br />
Monitor<strong>in</strong>g Severity of AD<br />
Many have noted the presence of an <strong>in</strong>fra-auricular fissure <strong>in</strong><br />
patients with AD. Kwatra et al took this cl<strong>in</strong>ical f<strong>in</strong>d<strong>in</strong>g a step<br />
further and found depth of the fissure to be associated with the<br />
severity of AD. This bedside cl<strong>in</strong>ical assessment has been found to<br />
be helpful assess<strong>in</strong>g AD severity across all age groups. 46<br />
Severe Cases<br />
A pilot study was recently completed with apremilast, an oral<br />
phosphdiesterase (PDE) <strong>in</strong>hibitor, for the treatment of AD <strong>in</strong><br />
adults. Results were promis<strong>in</strong>g, with reductions <strong>in</strong> pruritus,<br />
Eczema Area Severity Index (EASI) and the <strong>Dermatology</strong> Life<br />
Quality Index (DLQI) scores depend<strong>in</strong>g on dos<strong>in</strong>g at 3 and<br />
6 months. <strong>The</strong> leukocytes <strong>in</strong> patients with AD have elevated<br />
levels of PDE type 4 when compared to controls and this elevation<br />
leads to hyperactivity of leukocytes and <strong>in</strong>flammation.<br />
Oral PDE4 <strong>in</strong>hibitors have been studied for other conditions<br />
such as asthma, psoriasis, psoriatic arthritis and chronic obstructive<br />
pulmonary disease (COPD), but this is the first use of this<br />
medication for AD. 47<br />
Extracorporeal photochemotherapy is a procedure where<br />
the patient’s blood goes through a process called leukophoresis,<br />
which removes the patient’s white blood cells while<br />
the red blood cells and plasma are returned to the patient.<br />
<strong>The</strong> white blood cells are treated with UVA radiation for<br />
several cycles and then returned to the patient. <strong>The</strong> process<br />
has been a treatment for cutaneous T-cell lymphoma, but<br />
Consider<strong>in</strong>g the environment<br />
outside patients’ bodies and<br />
also what they are putt<strong>in</strong>g <strong>in</strong>to<br />
their bodies through nutrition<br />
may help <strong>in</strong> prevent<strong>in</strong>g flares<br />
or the disease itself.<br />
has more recently been studied as a potentially successful<br />
long-term treatment to stabilize AD <strong>in</strong> patients with severe<br />
disease that has been resistant to other systemic therapies<br />
without the immunosuppression that makes other systemic<br />
medications risky. 48<br />
Cyclospor<strong>in</strong> is a systemic agent used for the treatment<br />
of severe resistant atopic dermatitis. Subcutaneous allergen<br />
immunotherapy (SCIT) is a process of subcutaneously adm<strong>in</strong>ister<strong>in</strong>g<br />
gradually <strong>in</strong>creas<strong>in</strong>g doses of allergens to patients<br />
with allergic conditions to reduce cl<strong>in</strong>ical symptoms<br />
from exposure to the allergen over time. Allergic responses<br />
to common environmental allergens can be responsible<br />
for the chronicity of AD. Us<strong>in</strong>g house dust mite extract <strong>in</strong><br />
patients with known hypersensitivity for SCIT comb<strong>in</strong>ed<br />
with cyclospor<strong>in</strong>e, Nahm and Kim saw cl<strong>in</strong>ical improvements<br />
<strong>in</strong> all patients treated offer<strong>in</strong>g this <strong>in</strong>itial study for<br />
this comb<strong>in</strong>ed treatment option. 49<br />
38 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
On the Horizon<br />
Recent studies have suggested that sprout<strong>in</strong>g of epidermal<br />
nerves is seen with the pruritus associated with AD.<br />
Nerve growth factor (NGF), released by kerat<strong>in</strong>ocytes, is<br />
a major growth factor regulat<strong>in</strong>g these new nerve connections,<br />
and <strong>in</strong>creased levels of this molecule have been<br />
seen <strong>in</strong> AD patients. A nerve repulsion factor, epidermal<br />
semaphor<strong>in</strong> 3A (Sema3A), acts <strong>in</strong> opposition to NGF<br />
and the two are said to work together as axonal guidance<br />
molecules. Sema3A is found <strong>in</strong> decreased concentrations<br />
<strong>in</strong> AD patients and could be a new target for calm<strong>in</strong>g<br />
pruritus associated with anti-histam<strong>in</strong>e resistant itch. Initial<br />
animal studies with an o<strong>in</strong>tment conta<strong>in</strong><strong>in</strong>g Sema3A<br />
have so far shown positive results. 50<br />
In a separate study, Samukawa et al looked at another possible<br />
new treatment modality, red g<strong>in</strong>seng extract (RGE), and<br />
its effect on NGF. In a study where 2,4-d<strong>in</strong>itrofluorobenzene<br />
was applied to mouse ears to <strong>in</strong>duce pruritus, the 1% RGE<br />
was shown to be just as effective as tacrolimus <strong>in</strong> attenuat<strong>in</strong>g<br />
NGF, while dexamethasone was less effective. RGE also <strong>in</strong>hibited<br />
histam<strong>in</strong>e-<strong>in</strong>duced vascular permeability and the same<br />
result was observed cl<strong>in</strong>ically, with a decrease <strong>in</strong> scratch<strong>in</strong>g<br />
behavior by mice. 51<br />
Fucoidan, a sulphated polysaccharide extracted from<br />
brown seaweed known to have anti-allergic and immunologic<br />
activities, was recently tested for the treatment of<br />
AD <strong>in</strong> a mouse model. It was compared topically headto-head<br />
with dexamethasone and was shown to be just as<br />
effective both symptomatically and histologically, show<strong>in</strong>g<br />
a decreased number of mast cells and decreased thickness<br />
of epidermis. 52<br />
Peroxisome proliferator-activated receptors (PPARs) are<br />
nuclear receptors that have long been known to be associated<br />
with adipocytes and <strong>in</strong>volved <strong>in</strong> <strong>in</strong>sul<strong>in</strong> sensitization<br />
and adipogenesis, but have more recently been seen to be <strong>in</strong>volved<br />
<strong>in</strong> anti-<strong>in</strong>flammatory activity. In an AD mouse model,<br />
topical application of a PPARα activator showed cl<strong>in</strong>ical<br />
improvement <strong>in</strong> dermatitis, reduced <strong>in</strong>flammatory <strong>in</strong>filtrate<br />
<strong>in</strong> the dermis and decl<strong>in</strong>e of serum IgE elevation. <strong>The</strong>refore,<br />
a topical PPARα activator could be a topical steroid alternative<br />
<strong>in</strong> the future. 53<br />
Lastly, a new non-steroidal topical medication currently referred<br />
to as WBI-1001 has been shown to be efficacious <strong>in</strong><br />
treat<strong>in</strong>g mild to severe atopic dermatitis after completion of<br />
a multi-center Phase IIB randomized, parallel-group, doublebl<strong>in</strong>d,<br />
placebo-controlled trial. Only a s<strong>in</strong>gle-center, 4-week<br />
trial had been completed previously, so, after further test<strong>in</strong>g, this<br />
may be a new non-steroidal topical treatment on the horizon. 54<br />
Conclusions<br />
For patients with AD, the future looks promis<strong>in</strong>g. While<br />
this update only skims the surface of the current literature<br />
explor<strong>in</strong>g new and different treatment modalities <strong>in</strong> AD,<br />
consider<strong>in</strong>g a treatment plan — versus a s<strong>in</strong>gle ‘miracle’<br />
cream — and focus<strong>in</strong>g on rebuild<strong>in</strong>g the sk<strong>in</strong> barrier seem<br />
to be the current treatment trends. F<strong>in</strong>d<strong>in</strong>g medications<br />
that patients will use with a lesser side effect profile than<br />
topical and oral corticosteroids and go<strong>in</strong>g back to our<br />
roots <strong>in</strong> medic<strong>in</strong>e with TCM and <strong>in</strong>tegrative medic<strong>in</strong>e may<br />
cause less co-morbidities to our patients. Consider<strong>in</strong>g the<br />
environment outside patients’ bodies and also what they<br />
are putt<strong>in</strong>g <strong>in</strong>to their bodies through nutrition may help <strong>in</strong><br />
prevent<strong>in</strong>g flares or the disease itself. It is also important to<br />
consider the psychological effects of AD on both patients<br />
and those around them when try<strong>in</strong>g to implement successful<br />
treatment. F<strong>in</strong>d<strong>in</strong>g new ways of us<strong>in</strong>g the tried and true<br />
medications and treatment modalities can help recalcitrant<br />
cases. Lastly, better understand<strong>in</strong>g of AD on the molecular<br />
and genetic level gives us a positive outlook of what’s on<br />
the horizon. n<br />
Dr. K<strong>in</strong>ney is with the Wake Forest Baptist Health Department<br />
of <strong>Dermatology</strong> <strong>in</strong> W<strong>in</strong>ston-Salem, NC.<br />
Disclosure: Dr. K<strong>in</strong>ney has no conflicts of <strong>in</strong>terest to report.<br />
References<br />
1. Bieber T, Bussmann C. Atopic dermatitis. In: Bolognia JL, Jorizzo, JL, Schafer<br />
JV. <strong>Dermatology</strong> (3rd Edition). Elsevier; 2012.<br />
2. Kircik LH, Del Rosso JQ. Nonsteroidal treatment of atopic dermatitis<br />
<strong>in</strong> pediatric patients with a ceramide-dom<strong>in</strong>ant topical emulsion formulated<br />
with an optimized ratio of physiological lipids. J Cl<strong>in</strong> Aesthet Dermatol.<br />
2011;4(12): 25-31.<br />
3. Popa I, Remoue N, Osta B, et al. <strong>The</strong> lipid alterations <strong>in</strong> the stratum corneum<br />
of dogs with atopic dermatitis are alleviated by topical application of<br />
a sph<strong>in</strong>golipid-conta<strong>in</strong><strong>in</strong>g emulsion. Cl<strong>in</strong> Exp Dermatol. 2012;37(6):665-71.<br />
4. Pacha O, Hebert AA. Treat<strong>in</strong>g atopic dermatitis: safety, efficacy, and patient<br />
acceptabolity of a ceramide hyaluronic acid emollient foam. Cl<strong>in</strong> Cosmet Investig<br />
Dermatol. 2012;5:39-42.<br />
5. Duan J, Sugawara T, Hirose M, et al. Dietary sph<strong>in</strong>golipids improve sk<strong>in</strong><br />
barrier functions via the upregulation of ceramide synthases <strong>in</strong> the epidermis.<br />
Exp Dermatol. 2012;21(6):448-52.<br />
6. Okawa T, Yamaguchi Y, Takada S, et al. Oral adm<strong>in</strong>istration of collagen<br />
tripeptide improves dryness and pruritus <strong>in</strong> the acetone-<strong>in</strong>duced dry sk<strong>in</strong><br />
model. J Dermatol Sci. 2012;66(2):136-43.<br />
7. Grether-Beck S, Felsner I, Brenden H, et al. Urea uptake enhances barrier<br />
function and antimicrobial defense <strong>in</strong> humans by regulat<strong>in</strong>g epidermal gene<br />
expression. J Invest Dermatol. 2012;132(6):1561-72.<br />
8. McGrath J. Profilaggr<strong>in</strong>, dry sk<strong>in</strong>, and atopic dermatitis risk: size matters. J<br />
Invest Dermatol. 2012;132(1):10-1.<br />
9. Grzanka A, Zebracka-Gala J, Rachowska R, Bozek A, Kowalska M, Jarzab J.<br />
<strong>The</strong> effect of pimecrolimus on expression of genes associated with sk<strong>in</strong> barrier<br />
dysfunction <strong>in</strong> atopic dermatitis sk<strong>in</strong> lesions. Exp Dermatol. 2012;21(3):184-8.<br />
10. Jensen JM, Scheer A, Wanke C, et al. Gene expression is differently affected<br />
by pimecrolimus and betamethasone <strong>in</strong> lesional sk<strong>in</strong> of atopic dermatitis.<br />
Allergy. 2012;67(3):413-23.<br />
11. Rotsztejn H, Frankowska J, Kamer B, Trznadel-Grodzka E. Infection cases<br />
<strong>in</strong> <strong>in</strong>fants and small children with atopic dermatitis-own observations. Postepy<br />
Hig Med Dosw. 2012;66(0):96-103.<br />
12. Pelucchi C, Chatenoud L, Turati F, et al. Probiotics supplementation dur<strong>in</strong>g<br />
pregnancy or <strong>in</strong>fancy for the prevention of atopic dermatitis: a metaanalysis.<br />
Epidemiology. 2012;23(3):402-14.<br />
13. D<strong>in</strong>icola C, Kekevian A, Chang C. Integrative medic<strong>in</strong>e as adjunct therapy<br />
<strong>in</strong> the treatment of atopic dermatitis- the role of traditional ch<strong>in</strong>ese medic<strong>in</strong>e,<br />
dietary supplements, and other modalities. Cl<strong>in</strong> Rev Allergy Immunol.<br />
2012 Jun 4 (onl<strong>in</strong>e).<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 39
<strong>Current</strong> Trends <strong>in</strong> Atopic Dermatitis <strong>Treatment</strong>: More Than Just Steroids<br />
14. Jang SE, Tr<strong>in</strong>h HT, Chung YH, Han MJ, Kim DH. Inhibitory effect of<br />
lactobacillus plantarium K-1 on passive cutaneous anaphylaxis reaction and<br />
scratch<strong>in</strong>g behavior <strong>in</strong> mice. Arch Pharm Res. 2011;34(12):2117-23.<br />
15. Bell MC, Stoval SH, Scurlock AM, Perry TT, Jones SM, Harik<br />
NS. Address<strong>in</strong>g antimicrobial resistance to treat children with atopic<br />
dermatitis <strong>in</strong> a tertiary pediatric allergy cl<strong>in</strong>ic. Cl<strong>in</strong> Pediatr. 2012 Apr<br />
18 (Epub).<br />
16. Travers JB, Kozman A, Yao Y, et al. <strong>Treatment</strong> outcomes of secondarily imptig<strong>in</strong>ized<br />
pediatric atopic dermatitis lesions and the role of oral antibiotics.<br />
Pediatr Dermatol. 2012;29(3):2809-96.<br />
17. Tavaria FK, Soares JC, Reis IL, Paulo MH, Malcata FX, P<strong>in</strong>tado ME.<br />
Chitosan: antimicrobial action upon staphylococci after impregnation onto<br />
cotton fabric. J Appl Microbiol. 2012;122(5):1034-41.<br />
18. Naetchiporouk E, Cohen BA. Recogniz<strong>in</strong>g and manag<strong>in</strong>g eczematous<br />
id reactions to molluscum contagiosum virus <strong>in</strong> children. Pediatrics, 2012;<br />
129(4):e1072-5.<br />
19. Lee JH, Suh J, Kim EH, et al. Surveillance of home environment <strong>in</strong><br />
children with atopic dermatitis: a questionnaire survery. Asia Pac Allergy.<br />
2012;2(1):59-66.<br />
20. Gaff<strong>in</strong> JM, Spergel JM, Boguniewicz M, et al. Effect of cat and daycare<br />
exposures on the risk of asthma <strong>in</strong> children with atopic dermatitis. Allergy<br />
Astham Proc. 2012;33(3):282-8.<br />
21. Fujano N, Incorvaia C. Dissect<strong>in</strong>g the causes of atopic dermatitis <strong>in</strong> children:<br />
less foods, more mites. Allergol Int. 2012;61(2):231-43.<br />
22. Kim EH, Ahn K, Cheong HK. Use of humidifiers with children suffer<strong>in</strong>g<br />
from atopic dermatitis. Environ Health Toxicol. 2012;27:e2012004.<br />
23. Anuntaseree W, Sangsupawanich P, Osmond C, Mo-Suwan L, Vasiknanonte<br />
P, Choprapawon C. Sleep quality <strong>in</strong> <strong>in</strong>fants with atopic dermatitis: a community-based,<br />
birth cohort study. Asian Pac J Allergy Immunol. 2012;30(1):26-31.<br />
24. Chrostowska-Plak D, Reich A, Szepietowski JC. Relationship between<br />
itch and psychological status of patients with atopic dermatitis. J Eur Acad<br />
Dermatol Venereol. 2012 May 23 (Epub).<br />
25. Shyu CS, L<strong>in</strong> HK, L<strong>in</strong> CH, Fu LS. Prevelence of attention-deficit/hyperactivity<br />
disorder <strong>in</strong> patients with pediatric allergic disorders: a nationwide,<br />
population-based study. J Microbiol Immunol Infect. 2012;45(3):237-42.<br />
26. Adler-Cohen C, Czarnowicki T, Dreiher J, Ruzicka T, Ingber A, Harari<br />
M. Climatotherapy at the dead sea: an effective treatment modality for atopic<br />
dermatitis with significant positive impact on quality of life. Dermatitis.<br />
2012;23(2):75-80.<br />
27. Schut C, Mahmutovic V, Gieler U, Kupfer J. Patient education programs<br />
for childhood atopic dermatitis: who is <strong>in</strong>terested J Dtsch Dermatol Ges. 2012<br />
Apr 18 (Epub).<br />
28. Luersen K, Davis SA, Kaplan SG, Abel TD, W<strong>in</strong>chester WW, Feldman SR.<br />
Sticker charts: a method for improv<strong>in</strong>g adherence to treatment of chronic<br />
disease <strong>in</strong> children. Pediatr Dermatol. 2012;29(4): 403-408.<br />
29. Pazyar N, Yaghoobi R, Kazerouni A, Feily A. Oatmeal <strong>in</strong> dermatology:<br />
a brief review. Indian J Dermatol Venereol Leprol. [serial onl<strong>in</strong>e] 2012[cited<br />
2012 Jun 19];78(2):142-5. Available from: http://www.ijdvl.com/text.<br />
asp2012/78/2/142/93629.<br />
30. Sur R, Nigam A, Grote D, Liebel F, Southall MD. Avenanthramides, polyphenols<br />
from oats, exhibit anti-<strong>in</strong>flammatory and anti-itch activity. Arch Dermatol<br />
Res. 2008;300:569-74.<br />
31. Pigatto P, Bigardi A, Caputo R, et al. An evaluation of the allergic contact<br />
dermatitis potential of colloidal gra<strong>in</strong> suspensions. Am J Contact Dermat.<br />
1997;8:207-9<br />
32. Boussault P, Léauté-Labrèze C, Saubusse E, et al. Oat sensitization <strong>in</strong> children<br />
with atopic dermatitis: Prevalence, risks and associated factors. Allergy.<br />
2007;62:1251-6;quiz 82-3<br />
33. Ikegawa Y, Sato S, Lim G, Hur W, Tanaka K, Komori M, Takenaka S, Taira<br />
T. Amelioration of the progression of an atopic dermatitis-like sk<strong>in</strong> lesion<br />
by silk peptide and identification of functional peptides. Biosci Biotechnol<br />
Biochem. 2012;76(3):473-7.<br />
34. Ricci G, Neri I, Ricci L, Patrizi A. Silk fabrics <strong>in</strong> the management of<br />
atopic dermatitis. Sk<strong>in</strong> <strong>The</strong>rapy Lett. 2012;17(3):5-7.<br />
35. Park KY, Jang WS, Yang GW, et al. A pilot study of silver-loaded cellulose<br />
fabric with <strong>in</strong>corporated seaweed for the treatment of atopic dermatitis. Cl<strong>in</strong><br />
Exp Dermatol. 2012;37(5): 512-5.<br />
36. Chung TH, Kang TJ, Cho WK, et al. Effectiveness of novel herbal<br />
medic<strong>in</strong>e, KIOM-MA, and its bioconversion product, KIOM-MIA128,<br />
on the treatment of atopic dermatitis. Evid Based Complement Alternat Med.<br />
2012;2012:762918 (Epub).<br />
37. Roduit C, Frei R, Loss G, et al. Protection Aga<strong>in</strong>st Allergy-Study <strong>in</strong> Rural<br />
Environments study group. Development of atopic deratitis accord<strong>in</strong>g to<br />
age of onset and association with early-life exposures. J Allergy Cl<strong>in</strong> Immunol.<br />
2012;130(1):130-136.<br />
38. Lien TY, Goldman RD. Breastfeed<strong>in</strong>g and maternal diet <strong>in</strong> atopic dermatitis.<br />
Cam Fam Physician. 2011;57(12):1403-5.<br />
39. Bath-Hextall FJ, Jenk<strong>in</strong>son C, Humphreys R, Williams HC. Dietary<br />
supplements for established atopic eczema. Cochrane Database Syst Rev.<br />
2012;2:CD005205.<br />
40. Benson AA, Toh JA, Vernon N, Jariwala SP. <strong>The</strong> role of vitam<strong>in</strong><br />
D <strong>in</strong> the immunopathogenesis of allergic sk<strong>in</strong> diseases. Allergy.<br />
2012;67(3):296-301.<br />
41. Shaheen MA, Attia EA, Louka ML, Bareedy N. Study of the role of serum<br />
folic acid <strong>in</strong> atopic dermatitis: a correlation with serum IgE and disease severity.<br />
Indian J Dermatol. 2011;56(6):673-7.<br />
42. Kiefte-de Jong JC, Timmermans S, Jaddoe VW, et al. High circulat<strong>in</strong>g<br />
folate and vitam<strong>in</strong> B-12 concentrations <strong>in</strong> women dur<strong>in</strong>g pregnancy are associated<br />
with <strong>in</strong>creased prevalence of atopic dermatitis <strong>in</strong> their offspr<strong>in</strong>g. J<br />
Nutr. 2012;142(4):731-8.<br />
43. Takeuchi S, Saeki H, Tokunaga S, et al. A randomized, open-label, multicenter<br />
trial of topical tacrolimus for the treatment of pruritus <strong>in</strong> patients with<br />
atopic dermatitis. Ann Dermatol. 2012;24(2):144-50.<br />
44. Pople PV, S<strong>in</strong>gh KK. Target<strong>in</strong>g tacrolimus to deeper layers of sk<strong>in</strong> with<br />
improved safety for treatment of atopic dermatitis- Part II: In vivo assessment<br />
of dermatopharmacok<strong>in</strong>etics, biodistribution and efficacy. Int J Pharm.<br />
2012;434(1-2):70-9.<br />
45. Puya R, Alvarez-López M, Velez A, Casas Asuncion E, Moreno JC. <strong>Treatment</strong><br />
of severe refractory adult atopic dermatitis with ustek<strong>in</strong>umab. Int J Dermatol.<br />
2012;51(1):115-6.<br />
46. Kwatra SG, Tey HL, Dabade T, Chan YH, Yosipovitch G. <strong>The</strong> <strong>in</strong>fra-auricular<br />
fissure: a bedside marker of disease severity <strong>in</strong> patients with atopic<br />
dermatitis. J Am Acad Dermatol. 2012;66(6):1009-10.<br />
47. Samaro A, Berry TM, Goreshi R, Simpson EL. A pilot study of an oral<br />
phosphodiesterase <strong>in</strong>hibitor (Apremilast) for atopic dermatitis <strong>in</strong> adults. Arch<br />
Dermatol. 2012 Apr 16 (Epub).<br />
48. Rubegni P, Poggiali S, Ceven<strong>in</strong>i G, et al. Long term follow-up results on<br />
severe recalcitrant atopic dermatitis treated with extracorporeal phototherapy.<br />
J Eur Acad Dermatol Venereol. 2012 Apr 28 (Epub).<br />
49. Nahm DH, Kim ME. <strong>Treatment</strong> of severe atopic dermatitis with a comb<strong>in</strong>ation<br />
of subcutaneous allergen immunotherapy allergen immunotherapy<br />
and cyclospor<strong>in</strong>. Yonsei Med J. 2012;53(1):158-63.<br />
50. Negi O, Tom<strong>in</strong>aga M, Tengara S, et al. Topically applied semaphor<strong>in</strong><br />
3A o<strong>in</strong>tment <strong>in</strong>hibits scratch<strong>in</strong>g behavior and improves sk<strong>in</strong> <strong>in</strong>flammation<br />
<strong>in</strong> NC/Nga mice with atopic dermatitis. J Dermatol Sci.<br />
2012;66(1):37-43.<br />
51. Samukawa K, Izumi Y, Shiota M, et al. Red g<strong>in</strong>seng <strong>in</strong>hibits scratch<strong>in</strong>g<br />
behavior assicated with atopic dermatitis <strong>in</strong> experimental animal models. J<br />
Pharmacol Sci. 2012;118(3):391-400.<br />
52. Yang JH. Topical application of fucoidan improves atopic dermatitis symptoms<br />
on NC/Nga mice. Phytother Res. 2012 Mar 19 (Epub).<br />
53. Chiba T, Takeuchi S, Esaki H, et al. Topical application of PPAPα<br />
(but not β/δ or ϒ) suppresses atopic dermatitis <strong>in</strong> NC/Nga mice. Allergy.<br />
2012;67(7):936-42.<br />
54. Bissonnette R, Poul<strong>in</strong> Y, Zhou Y, et al. Efficacy and safety of topical WBI-<br />
1001 <strong>in</strong> patients with mild to severe atopic dermatitis; results from a 12-week,<br />
multicentre, randomized, placebo-controlled double-bl<strong>in</strong>d trial. Br J Dermatol.<br />
2012;166(4):853-60.<br />
40 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
New Products<br />
Topix Pharmaceuticals Introduces Replenix<br />
Clarify<strong>in</strong>g Brighten<strong>in</strong>g Polish<br />
<strong>The</strong> new Replenix Clarify<strong>in</strong>g<br />
Brighten<strong>in</strong>g Polish from Topix<br />
Pharmaceuticals is a mild cleanser<br />
with exfoliat<strong>in</strong>g microbeads that<br />
is designed to ref<strong>in</strong>e sk<strong>in</strong> “gently<br />
and effectively.”<br />
<strong>The</strong> Brighten<strong>in</strong>g Polish has<br />
smooth<strong>in</strong>g, soften<strong>in</strong>g, exfoliat<strong>in</strong>g,<br />
brighten<strong>in</strong>g and purify<strong>in</strong>g qualities<br />
and <strong>in</strong>cludes <strong>in</strong>gredients such as<br />
glycolic and salicylic acids, arbut<strong>in</strong>,<br />
bisabolol, CoQ10, green tea polyphenols<br />
and vitam<strong>in</strong> C. <strong>The</strong> Brighten<strong>in</strong>g<br />
Polish helps slough away surface<br />
sk<strong>in</strong> cells <strong>in</strong> order to enhance<br />
texture, suppleness and moisture<br />
levels while dim<strong>in</strong>ish<strong>in</strong>g f<strong>in</strong>e l<strong>in</strong>es<br />
and wr<strong>in</strong>kles, all without irritation.<br />
<strong>The</strong> new Brighten<strong>in</strong>g Polish from<br />
Topix Pharmaceuticals is both paraben-free<br />
and non-comedogenic. It is<br />
suitable for all sk<strong>in</strong> types.<br />
Replenix Clarify<strong>in</strong>g Brighten<strong>in</strong>g Polish sells for $32.40 and<br />
can be purchased through a variety of websites.<br />
For more <strong>in</strong>formation, please visit www.topixpharm.com. n<br />
Liftactiv Serum 10 from<br />
Vichy Laboratories<br />
LiftActiv Serum 10 is a new antiag<strong>in</strong>g<br />
serum from Vichy Laboratories<br />
that firms, tightens and softens the sk<strong>in</strong>.<br />
LiftActiv Serum 10 comb<strong>in</strong>es<br />
Rhamnose <strong>in</strong> a 10% concentration<br />
with hyaluronic acid, ceramides and<br />
antioxidant-rich Vichy <strong>The</strong>rmal Water.<br />
Rhamnose is a naturally derived plant<br />
sugar that is proven to stimulate rejuvenation<br />
of all sk<strong>in</strong> surface layers simultaneously,<br />
accord<strong>in</strong>g to the company.<br />
LiftActiv Serum 10 results <strong>in</strong> a cl<strong>in</strong>ically proven reduction of<br />
the appearance of the four ma<strong>in</strong> types of facial wr<strong>in</strong>kles (eye<br />
contours, crow’s feet, forehead wr<strong>in</strong>kles and laugh l<strong>in</strong>es) after<br />
one month, accord<strong>in</strong>g to the company. In addition, the new<br />
LiftActiv Serum 10 from Vichy Laboratories reduces the appearance<br />
of pores. <strong>The</strong> Serum is gentle enough for all sk<strong>in</strong> types.<br />
<strong>The</strong> Vichy LiftActiv Serum 10 will be available <strong>in</strong> September<br />
2012 for $52. It can be purchased at select CVS, Duane<br />
Reade and Walgreens locations.<br />
For more <strong>in</strong>formation, please visit www.vichyusa.com. n<br />
Polish and Plump Peel is a Two-<br />
Step Anti-Wr<strong>in</strong>kle System<br />
<strong>The</strong> new Polish and Plump Peel from HydroPeptide is a microdermabrasion<br />
peel system that <strong>in</strong>cludes two anti-wr<strong>in</strong>kle systems.<br />
<strong>The</strong> first peel, Anti-Wr<strong>in</strong>kle Polish<strong>in</strong>g Crystals, conta<strong>in</strong>s<br />
vitam<strong>in</strong> C for collagen support and works to destroy reactive<br />
oxidiz<strong>in</strong>g agents and promote sk<strong>in</strong> tone consistency by <strong>in</strong>hibit<strong>in</strong>g<br />
melan<strong>in</strong> production. <strong>The</strong> second peel, the Anti-Wr<strong>in</strong>kle<br />
Plump<strong>in</strong>g Activator, conta<strong>in</strong>s lactic acid, which sloughs away<br />
dead sk<strong>in</strong> cells, dim<strong>in</strong>ishes dryness, promotes a more uniform<br />
complexion and primes the sk<strong>in</strong> for hydration, and has an additional<br />
wr<strong>in</strong>kle-smooth<strong>in</strong>g boost because of the trylagen and<br />
SNAP 8 peptides, accord<strong>in</strong>g to the company.<br />
<strong>The</strong> new Polish and Plump Peel from HydroPeptide is<br />
available for $68. It can be purchased at spas nationwide and<br />
onl<strong>in</strong>e at www.hydropeptide.com.<br />
For more <strong>in</strong>formation, please visit www.hydropeptide.com. n<br />
Glytone Anti-Ag<strong>in</strong>g<br />
Night Cream Improves<br />
Deep L<strong>in</strong>es, Wr<strong>in</strong>kles<br />
Glytone has released its new Anti-<br />
Ag<strong>in</strong>g Night Cream, a new night<br />
cream <strong>in</strong>dicated for daily use.<br />
<strong>The</strong> Anti-Ag<strong>in</strong>g Night Cream, the<br />
latest addition to Glytone’s antioxidant<br />
anti-ag<strong>in</strong>g range of products, is<br />
formulated with natural peptides,<br />
antioxidants and glycolic acid. <strong>The</strong><br />
Anti-Ag<strong>in</strong>g Night Cream is designed<br />
to improve the appearance of deep l<strong>in</strong>es and wr<strong>in</strong>kles and<br />
<strong>in</strong>crease the production of the prote<strong>in</strong>s that preserve and<br />
strengthen the epidermal layers of the sk<strong>in</strong>.<br />
<strong>The</strong> new Anti-Ag<strong>in</strong>g Night Cream from Glytone is available<br />
exclusively through physicians. It has a suggested retail<br />
price of $89 for 1.0 fl. oz./30 mL.<br />
For more <strong>in</strong>formation, and to locate a physician, please visit<br />
www.glytone-usa.com. n<br />
www.the-dermatologist.com<br />
August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> 41
Calendar of Events<br />
September 27 to 30, 2012<br />
Prague, Czech Republic — <strong>The</strong> 21st European Academy of <strong>Dermatology</strong> and Venereology Congress - Sk<strong>in</strong> is Vital - to be held at<br />
the Prague Congress Centre <strong>in</strong> Prague, Czech Republic. <strong>The</strong> 21st EADV Congress offers a platform for dissem<strong>in</strong>at<strong>in</strong>g scientific and<br />
practical knowledge among dermato-venereology professionals.<br />
For more <strong>in</strong>formation, please visit www.eadv.org.<br />
October 4 to 7, 2012<br />
Las Vegas, NV — <strong>The</strong> Fall Cl<strong>in</strong>ical <strong>Dermatology</strong> Conference to be held at the Encore at the Wynn <strong>in</strong> Las Vegas, NV. This 4-day<br />
conference is designed to provide <strong>in</strong>creased knowledge for the practic<strong>in</strong>g dermatologist by present<strong>in</strong>g a comprehensive update on<br />
the diagnosis and treatment of a variety of conditions related to medical, surgical and cosmetic dermatology. <strong>The</strong> program offers daily<br />
lectures, panels, live patient workshops and Q&A sessions.<br />
For more <strong>in</strong>formation, please visit www.cl<strong>in</strong>icaldermconf.org.<br />
October 11 to 14, 2012<br />
Atlanta, GA — <strong>The</strong> 2012 Annual Meet<strong>in</strong>g of the American Society for Dermatologic Surgery to be held at the Hyatt Regency<br />
<strong>in</strong> Atlanta, GA. This is an educational forum for dermatologists committed to excellence <strong>in</strong> cosmetic, medical, reconstructive and<br />
Mohs procedures.<br />
For more <strong>in</strong>formation, please visit www.asds.net.<br />
October 19 to 21, 2012<br />
San Francisco, CA — <strong>The</strong> Women’s & Pediatric <strong>Dermatology</strong> Sem<strong>in</strong>ar 2012 to be held at the Grand Hyatt San Francisco <strong>in</strong> San<br />
Francisco, CA. This conference will explore the chief cl<strong>in</strong>ical topics relevant to sk<strong>in</strong> diseases <strong>in</strong> women and children. <strong>Dermatologist</strong>s,<br />
pediatricians, OB/GYNs and other healthcare providers who manage these conditions are <strong>in</strong>vited to attend.<br />
For more <strong>in</strong>formation, please visit http://bit.ly/xB89a3.<br />
October 24 to 27, 2012<br />
Durban, South Africa — <strong>The</strong> International Society of <strong>Dermatology</strong>’s 3rd Annual Cont<strong>in</strong>ental Congress of <strong>Dermatology</strong> and the 65th<br />
National Congress of the DSSA to be held <strong>in</strong> Durban, South Africa. This conference allows dermatologists from all over the world to<br />
<strong>in</strong>teract and attend sessions encompass<strong>in</strong>g all fields of dermatology, with <strong>in</strong>formation presented by lead<strong>in</strong>g dermatologists.<br />
For more <strong>in</strong>formation, please visit www.pedsderm.net.<br />
Calendar of Events Submissions<br />
Send <strong>in</strong>formation to:<br />
Stefanie Tuleya<br />
<strong>The</strong> <strong>Dermatologist</strong><br />
83 General Warren Blvd., Ste. 100<br />
Malvern, PA 19355<br />
stuleya@hmpcommunications.com<br />
42 August 2012 <strong>The</strong> <strong>Dermatologist</strong> ® <strong>Current</strong> <strong>Treatment</strong> <strong>Strategies</strong> <strong>in</strong> <strong>Dermatology</strong> www.the-dermatologist.com
, LLC