ESD Brochure (PDF 881.5 KB) - ERBE Elektromedizin GmbH
ESD Brochure (PDF 881.5 KB) - ERBE Elektromedizin GmbH
ESD Brochure (PDF 881.5 KB) - ERBE Elektromedizin GmbH

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
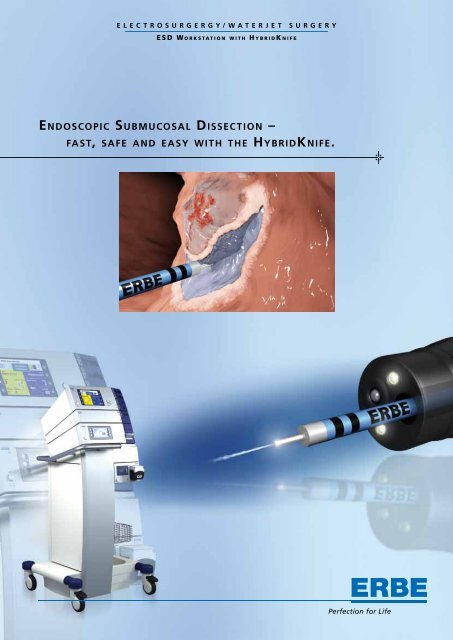
E L E C T R O S U R G E R G Y / W A T E R J E T S U R G E R Y<br />
E S D W o r k s t a t i o n w i t h H y b r i d K n i f e<br />
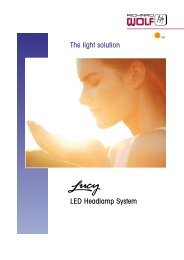
Endoscopic Submucosal Dissec tion –<br />
fast, safe and easy with the HybridKnife.
introduction<br />
<strong>ERBE</strong> TechnOLOgy<br />
Endoscopic submucosal resection spares the patient<br />
open surgery and with it possible intra- and postoperative<br />
complications. Using the EMR (endoscopic<br />
mucosal resection) and the <strong>ESD</strong> (endoscopic submucosal<br />
dissection) methods, such minimally invasive<br />
interventions have found application for the treatment<br />
of early carcinomas, adenomas and lesions in<br />
the gastrointestinal tract in general for some years.<br />
<strong>ERBE</strong> <strong>Elektromedizin</strong> has advanced the development<br />
of this precise <strong>ESD</strong> method in collaboration with<br />
leading Japanese and European experts. Safety aspects<br />
have been improved considerably, the surgical<br />
procedure has been simplified, and operating times<br />
have been reduced.<br />
Internationally renowned gastroenterologists already<br />
work using this method. More and more users<br />
convinced of its merits will adopt it, applying it for<br />
lesions of the stomach and increasingly also of the<br />
colon and the esophagus.<br />
With its VIO GI workstation, Erbe <strong>Elektromedizin</strong><br />
has established itself in the field of gastroenterology<br />
worldwide and has many years of profound know<br />
how in interventional endoscopy.<br />
The system consists of the VIO electrosurgical unit,<br />
which acts as the master module, as well as an Argon<br />
Plasma Coagulation unit for devitalizing gastrointestinal<br />
structures and coagulating diffuse bleeding.<br />
The <strong>ERBE</strong>JET 2 waterjet surgical unit is a new, additional<br />
system component for <strong>ESD</strong>.<br />
Both technologies, electrosurgery and waterjet surgery,<br />
are activated and applied using the <strong>ERBE</strong> HybridKnife as<br />
a combination instrument. For the first time, all working<br />
steps involved in the <strong>ESD</strong> procedure can be performed<br />
with just one instrument: marking of the resection margin,<br />
elevation of the mucosa, incision/dissection of the submucosa<br />
and coagulation of the resection bed.<br />
In this brochure we wish to demonstrate to you the<br />
advantages of the <strong>ESD</strong> method using the Hybrid-<br />
Knife, describe the steps involved in the procedure,<br />
and provide you with additional information and<br />
useful adviced.<br />
Medical progress never stands still. Thus we not only<br />
aim to provide what is currently the most effective,<br />
state-of-the-art procedure for endoscopic resection.<br />
We will continue to keep abreast of clinical insights<br />
and incorporate them into our research and development<br />
so that you obtain even better results in the<br />
treatment of your patients in the future.<br />
Important note<br />
<strong>ERBE</strong> <strong>Elektromedizin</strong> <strong>GmbH</strong> has taken the greatest possible<br />
care when compiling these recommendations.<br />
Nevertheless, it is impossible to exclude the possibility<br />
that errors may be contained herein. The information<br />
and recommendations given here may not be construed<br />
as constituting any basis for any claims against <strong>ERBE</strong><br />
<strong>Elektromedizin</strong> <strong>GmbH</strong>. Should legal regulations stipulate<br />
liability, such liability shall be limited to intentional<br />
misconduct or gross negligence.<br />
The data respecting recommended settings, areas of<br />
application, application duration or the use of instruments<br />
is based on clinical experience, although it is<br />
important to remember that individual centers and<br />
physicians may favor settings which differ from the recommended<br />
settings given here. All values are merely<br />
guidelines and their applicability must be verified by the<br />
operator. Depending on the circumstances, it may be<br />
necessary to deviate from the values and settings given<br />
in this brochure.<br />
Medical science is subject to a process of permanent<br />
change based on research and clinical experience. It<br />
may therefore also be appropriate to deviate from the<br />
values and settings given in this brochure on the basis<br />
of the results of such research and experience.<br />
02 HybridKnife
<strong>ERBE</strong> VIO electrosurgical unit<br />
ENDO CUT Q<br />
This electrosurgical unit provides the cutting and coagulation<br />
modes necessary to obtain the tissue effects<br />
required for <strong>ESD</strong> and EMR.<br />
ENDO CUT Q<br />
DRY CUT<br />
FORCED COAG<br />
The ENDO CUT Q fractionated cutting mode with alternating<br />
cutting and coagulating cycles was specifically developed<br />
for endoscopic interventions. The ENDO CUT Q<br />
is employed for snare ablation as well as circular incision<br />
and resection of lesions using an electrosurgical cutting<br />
electrode.<br />
The voltage and arc regulation which the VIO generator<br />
technology features allow for high quality and reproducible<br />
cutting effects. During the entire cutting process,<br />
controlled cutting and reliable hemostasis as well as low<br />
risk of perforation are ensured. The principle – as much<br />
coagulation as necessary (prevention of bleeding), as little<br />
as possible (prevention of perforation).<br />
U<br />
Voltage<br />
Figure 1:<br />
GI workstation: VIO 200 D electrosurgical<br />
unit, APC 2 Argon Plasma<br />
Coagulation unit, <strong>ERBE</strong>JET 2 waterjet<br />
surgical unit and EIP 2 endoscopic<br />
irrigation pump<br />
Coagulation cycle<br />
Cutting cycle<br />
t<br />
Time<br />
Figure 2:<br />
ENDO CUT Q fractionated cut<br />
The alternating cutting and coagulation cycles which<br />
characterize ENDO CUT Q can be varied dependent on<br />
size, shape and localization of the lesion in question – in<br />
terms of levels of effect, cutting duration and cutting interval.<br />
(For more detailed information on ENDO CUT Q<br />
consult <strong>ERBE</strong> brochure no. 85800-117.)<br />
HybridKnife<br />
03
DRY CUT<br />
<strong>ERBE</strong>JET 2 waterjet surgical unit<br />
This mode provides a cut with high coagulation effect and<br />
ensures reliable hemostasis even when relatively large<br />
blood vessels are involved. Reproducible effects with<br />
low degree of smoke plume formation can be obtained<br />
through voltage regulation.<br />
In numerous disciplines, waterjet surgery has clear<br />
advantages over alternative surgical procedures. Its<br />
classic application is hepatic surgery. <strong>ERBE</strong> has gathered<br />
many years of experience with this technology<br />
– in other surgical disciplines as well.<br />
Figure 1:<br />
Marking of the lesion margin<br />
Figure 3:<br />
Layer-specific elevation of the mucosa<br />
using the waterjet<br />
FORCED COAG<br />
Marking of the lesion is carried out using FORCED COAG.<br />
During resection, bleeding can be coagulated using the<br />
FORCED COAG mode and also any necessary post-coagulation<br />
of the resection bed.<br />
APC 2 Argon Plasma Coagulation<br />
Apart from classic electrosurgical modes, another GI module,<br />
the APC 2 Argon Plasma Coagulation unit, provides<br />
safe methods for marking the lesion margins and can also be<br />
used for hemostasis during and after the resection process.<br />
The APC 2 unit enables non-contact coagulation; thus<br />
there is no risk of tissue adhesion. Coagulation depth is limited,<br />
controlled and homogenous. This almost completely<br />
rules out any risk of perforation. The resection bed can be<br />
coagulated with the APC completely and homogenously.<br />
The waterjet pressure can be adjusted from effect 1 to effect<br />
80 (this corresponds approximately to 1-80 bar). For<br />
gastroenterology applications, an effect between 10 and<br />
50 should be selected for the specific organ in question.<br />
Please consult the table on page 10 for precise setting recommendations.<br />
At low effect settings blood vessels and<br />
nerves are spared, as are adjacent tissue structures and organs,<br />
for the waterjet procedure works tissue-selectively<br />
without producing any thermal effects.<br />
These very features are what makes waterjet technology<br />
ideally suited for mucosal elevation before endoscopic resection:<br />
the selective waterjet penetrates the mucosa and<br />
separates the tissue layers without use of needles while<br />
respecting anatomical layers. The separation medium accumulates<br />
in the submucosa located beneath the mucosa,<br />
forming a fluid cushion between the mucosa and the muscularis.<br />
The mucosa with the infiltrated lesion is elevated<br />
and can be resected without the muscularis being injured.<br />
For further information on waterjet surgery, argon plasma<br />
coagulation and the endoscopic irrigation pump please go<br />
to www.erbe-med.com or consult individual brochures.<br />
Figure 2:<br />
Surface coagulation with APC 2<br />
04 HybridKnife
HybridKnife<br />
The flexible, multi-function probe combines both technologies,<br />
electrosurgery and waterjet surgery, in one<br />
instrument. The four working steps – marking, elevation,<br />
incision/dissection and coagulation – require no change<br />
of instrument.<br />
The variably adjustable tip of the HybridKnife has a diameter<br />
of 0.7 mm and a micro-capillary.<br />
For the various segments of the gastrointestinal<br />
tract we recommend using needles in the following<br />
lengths:<br />
Figure 3:<br />
Needleless elevation of mucosa<br />
using the HybridKnife<br />
Stomach, approx. 3 mm<br />
Colon, approx. 1.5 mm<br />
Esophagus, approx. 2 mm<br />
The probe has an overall length of 190 cm; its external<br />
diameter of 2.3 mm makes it suitable for use with any<br />
standard endoscope.<br />
Needleless waterjet elevation raises the mucosa particularly<br />
quickly and it creates a considerably larger fluid cushion<br />
than one created by conventional needle injection.<br />
Figure 4:<br />
HybridKnife, I-type<br />
Figure 5:<br />
HybridKnife, T-type<br />
Figure 1:<br />
Elevation using waterjet function<br />
Figure 6:<br />
HybridKnife, O-type<br />
Figure 2:<br />
Marking, incision/dissection and coagulation using the electrosurgical<br />
electrode tip which varies in length and finds versatile application in<br />
the esophagus, stomach and colon<br />
HybridKnife<br />
05
PROCEDURE<br />
Figures 1+2:<br />
Piecemeal method used in EMR for<br />
relatively large lesions<br />
EMR and <strong>ESD</strong> are interventional procedures for<br />
treating early carcinomas and lesions which potentially<br />
constitute focal carcinomas. The prerequisite<br />
for a curative approach is complete resection of the<br />
lesion (R0 resection).<br />
Limits of EMR<br />
Using the EMR method, only lesions measuring up to 2 cm<br />
can be removed en bloc. For lesions with a diameter of<br />
more than 2 cm, only successive partial resection (piecemeal<br />
method) is possible using the EMR method. The disadvantage<br />
is that EMR harbors the risk of lesions larger<br />
than 2 cm in diameter not being ablated completely with<br />
a safe resection margin and carcinogenic cells remaining<br />
in the mucosa.<br />
When <strong>ESD</strong> is used, the lesion can be resected en bloc<br />
with a safe resection margin. From this perspective it is<br />
plausible that in the case of EMR, the recurrence rate is<br />
much higher than for the more precise but more difficult<br />
to learn <strong>ESD</strong> method.<br />
Figures 3+4:<br />
Complete resection of lesion using<br />
<strong>ESD</strong> with R0 approach<br />
<strong>ESD</strong> method using the HybridKnife<br />
The advantages of the <strong>ESD</strong> method developed by <strong>ERBE</strong><br />
derive from synergetic utilization of waterjet technology<br />
in connection with electrosurgery.<br />
The individual working steps – marking, elevation, incision/dissection<br />
and coagulation – can be performed with<br />
the multi-function HybridKnife without change of instrument<br />
while achieving the highest possible degree of<br />
safety.<br />
06 HybridKnife
The working steps<br />
Figure 1:<br />
Marking<br />
Step 1: Marking<br />
Before elevation, the lateral safety margin is marked with<br />
coagulation points at smallest possible intervals with the<br />
lesion demonstrating a peripheral zone of 5-7 mm. The<br />
APC non-contact method using the PULSED APC mode is<br />
also suitable for this procedure.<br />
Step 2: Elevation<br />
The HybridKnife is positioned on the mucosa with a slight<br />
amount of pressure and an application angle of approx.<br />
20°. The waterjet penetrates the soft mucosa and accumulates<br />
in the collagenous fibers of the submucosa, which<br />
becomes bloated in a pillow-like fashion. The muscularis,<br />
which lies below the submucosa, is not penetrated until<br />
considerably higher amounts of pressure are reached than<br />
those required to penetrate the mucosa. Tissue elevation<br />
occurs on the basis of differing tissue consistencies layer-selectively<br />
and safely and, when performed properly,<br />
without any risk of perforating the organ.<br />
Figure 2:<br />
Elevation<br />
The “cushioned” submucosa forms a safety margin to the<br />
muscularis, thus minimizing the risk of perforation during<br />
initial and circular incision of the lesion when the <strong>ESD</strong><br />
method is used and when the EMR snare ablation method<br />
is employed. The submucosal cushion also provides protection<br />
against thermal damage of the muscularis.<br />
The cushion remains intact during dissection and resection<br />
and additional fluid can be added if necessary to ensure<br />
its protective function throughout the entire course<br />
of the <strong>ESD</strong> procedure. Since the blood vessels are compressed<br />
by the fluid cushion, risk of bleeding is minimized.<br />
The operation can be performed with little bleeding and a<br />
good view of the target area.<br />
Figure 3:<br />
Incision/dissection<br />
Step 3: Incision/dissection<br />
VIO modes ENDO CUT Q and DRY CUT, which are used<br />
for initial and circular incision and resection of the lesion,<br />
provide optimal cutting features.<br />
Figure 4:<br />
Coagulation<br />
Step 4: Coagulation<br />
Blood vessels and leakages are coagulated during and<br />
after resection with FORCED COAG. Hemostasis is enhanced<br />
by the compressive fluid cushion.<br />
You will find recommendations for settings on page 10.<br />
HybridKnife<br />
07
APPLICATION<br />
In the following we wish to take a closer look at some<br />
special aspects concerning elevation and dissection<br />
of the mucosa and demonstrate some further advantages<br />
of the <strong>ESD</strong> method using the HybridKnife.<br />
Diagnosis/localization<br />
Reduction of bleeding<br />
During elevation of the mucosa, initial diagnostic prognoses<br />
in terms of tumor infiltration can be made because tumor-infiltrated<br />
lesions which occur in the colon in particular<br />
cannot be elevated. Should no elevation be detected<br />
during waterjet activation, despite having set the effect<br />
correctly, this is indicative of a tumor which has infiltrated<br />
deeper tissue layers. In this case, the indication for curative<br />
<strong>ESD</strong> is no longer given.<br />
Through the water pressure, small capillary blood vessels<br />
within the submucosa cushion are compressed. The result:<br />
bleeding is reduced and the view of the target area<br />
remains unimpaired.<br />
Unlike needle injection, use of the waterjet practically<br />
rules out risk of injury to blood vessels. This aspect ensures<br />
additional reduction of possible bleeding.<br />
An additional diagnostic tool which facilitates the detection<br />
and visual identification of tumor boundaries is a<br />
contrast medium which can be added to the separation<br />
medium. The altered tissue of the lesion already becomes<br />
visible through elevation alone. However, the contrast<br />
medium makes the difference between healthy and pathological<br />
tissue even more distinct.<br />
Should any bleeding nevertheless occur, it can be rinsed<br />
using the waterjet and coagulated afterwards electrosurgically.<br />
Figure 1:<br />
The tumor is visualized using<br />
contrast medium<br />
Figure 2:<br />
Reduction of bleeding, thus good<br />
view of the operating field<br />
08 HybridKnife
Protection against perforation<br />
R0 resection of relatively large lesions<br />
In the case of needle injection, the separation medium is<br />
injected underneath the mucosa. Here the risk of injuring<br />
blood vessels arises.<br />
When performing the needle-injection procedure, a<br />
change of instrument is required if fluid is added in the<br />
course of the intervention, and thus the tendency is to<br />
perform resection using a less pronounced submucosal<br />
cushion. This in turn increases the risk of thermal and mechanical<br />
perforation of the muscularis.<br />
Using the <strong>ESD</strong> method, large-surface tissue lesions can<br />
also be resected en bloc. The resection bed has a smooth<br />
resection surface which heals homogenously and with<br />
practically no scarring approximately 4 weeks post-operatively.<br />
Since waterjet elevation can be performed at any time, it<br />
is possible to keep the cushion volume constant during<br />
and after dissection and resection. Thus the safety margin<br />
to the muscularis is preserved.<br />
Figure 1:<br />
Waterjet elevation is possible at<br />
all times<br />
Figure 2:<br />
Homogenous resection bed<br />
free of bleeding after <strong>ESD</strong> with<br />
HybridKnife<br />
Aspects of cost<br />
The separation medium used for <strong>ERBE</strong>JET 2, a common<br />
physiological saline solution, is much more cost-economic<br />
than the solution enriched with additives which is used for<br />
needle injection. Administering needle injections requires<br />
force, in particular when fluids with a high degree of viscosity<br />
are involved. And a further aspect of cost-efficiency<br />
is that when using the waterjet method, no additional personnel<br />
is required for assisting in the elevation process.<br />
As a multi-function probe, the HybridKnife performs all<br />
four working steps: marking, elevation, incision/dissection<br />
and coagulation. No additional two-channel endoscope is<br />
needed for performing <strong>ESD</strong> with the HybridKnife; a singlechannel<br />
endoscope fulfills all the requirements.<br />
HybridKnife<br />
09
RECOMMENDED SETTINGS<br />
The following tables give you guideline values for<br />
the various gastrointestinal segments. These values<br />
should provide you with some orientation in selecting<br />
settings for waterjet pressure and CUT and<br />
COAG modes.<br />
<strong>ERBE</strong>JET 2<br />
VIO system<br />
ESOPHAGUS<br />
Mucosal elevation<br />
Effect: 30-50<br />
Marking<br />
PULSED APC, 20 Watts<br />
FORCED COAG, effect 1, 20 Watts<br />
Incision/dissection<br />
ENDO CUT Q, effect 2, cutting duration 3, cutting interval 3<br />
DRY CUT, effect 2, 80 Watts (higher degree of hemostasis)<br />
Coagulation<br />
FORCED COAG, effect 2, 60 Watts<br />
STOMACH<br />
Mucosal elevation<br />
Effect: 30-50<br />
Marking<br />
PULSED APC, 20 Watts<br />
FORCED COAG, effect 1, 20 Watts<br />
Incision/dissection<br />
ENDO CUT Q, effect 2, cutting duration 3, cutting interval 3<br />
DRY CUT, effect 2, 80 Watts (higher degree of hemostasis)<br />
Coagulation<br />
FORCED COAG, effect 2, 60 Watts<br />
right COLON<br />
Mucosal elevation<br />
Effect: 10-15<br />
Marking<br />
PULSED APC, 20 Watts<br />
FORCED COAG, Effekt 1, 20 Watts<br />
Incision/dissection<br />
ENDO CUT Q, effect 2, cutting duration 3, cutting interval 3<br />
DRY CUT, effect 2, 80 Watts (higher degree of hemostasis)<br />
Coagulation<br />
FORCED COAG, effect 2, 60 Watts<br />
rectum<br />
left COLON<br />
Mucosal elevation<br />
Effect: 20-30<br />
Marking<br />
PULSED APC, 20 Watts<br />
FORCED COAG, Effekt 1, 20 Watts<br />
Incision/dissection<br />
ENDO CUT Q, effect 2, cutting duration 3, cutting interval 3<br />
DRY CUT, effect 2, 80 Watts (higher degree of hemostasis)<br />
Coagulation<br />
FORCED COAG, effect 2, 60 Watts<br />
10 HybridKnife
advise on use<br />
BIBLIOGRAPHY<br />
On the basis of previous applications we have gathered<br />
some valuable experience which should help<br />
simplify the use of the HybridKnife for you.<br />
Position of the patient<br />
The patient should always be positioned in such a way<br />
that gravity causes the lesion to fall away from the wall.<br />
Kaehler GF, Sold MG, Fischer K, Post S, Enderle M. Selective fluid<br />
cushion in the submucosal layer by water jet: advantage for endoscopic<br />
mucosal resection. European Surgical Research 2007; 39:<br />
93-97.<br />
Schumacher B. Therapie von Magenadenomen und Frühkarzinomen.<br />
Endoluminal Therapy of Adenoma and Early Stomach Cancer. Endoskopie<br />
heute 2007; 20(4):236-240.<br />
Flexible endoscope with transparent cap<br />
We recommend using an elastic, transparent cap which is<br />
placed on the distal end of the endoscope. This ensures<br />
a better view of the resection surface and the already resected<br />
mucosa segment can be kept away from the lens<br />
and the tip of the instrument in this way.<br />
Distance between marking points<br />
We recommend as short a distance as possible, with the<br />
individual marking points being 2-3 mm apart. This facilitates<br />
a good overview of the operating site and increases<br />
the reliability of R0 resection.<br />
Schumacher B, Neuhaus H, Enderle MD. Utilisation expérimentale<br />
d’un nouvel instrument de mucosectomie. Acta Endoscopica 2007;<br />
37(5):673-678.<br />
Schumacher B, Deinert K, Philipper M, Neuhaus H. Experimetal<br />
testing of a new Hybrid Knife for endoscopic submucosal dissection<br />
(<strong>ESD</strong>) in the esophagus. Gastrointestinal Endoscopy 2007; 65(5):<br />
AB278.<br />
Fernandez-Esparrach G, Matthes E, Maurice D, Enderle MD,<br />
Thompson CC, Carr-Locke D. A Novel Device for Endoscopic Submucosal<br />
Dissection That Combines Water-Jet Submucosal Hydrodissection<br />
and Elevation with Electrocautery. Gastrointestinal Endoscopy<br />
2008; 67(5):AB141.<br />
Extension of elevation<br />
The lesion need not be completely elevated before dissection<br />
is performed. When using the <strong>ESD</strong> method, it can<br />
prove advantageous to alternate between elevation and<br />
dissection in segments.<br />
Adding another dye (such as indigo carmine) to the NaCl<br />
solution may be helpful as a means of improving contrast.<br />
Ryou M, Shaikh SN, Yao M, Fernandez-Esparrach G, Henry FP,<br />
Kochevar I, Maurice D, Matthes EL, Enderle MD, Carr-Locke DL,<br />
Redmond RW, Christopher C. Thompson CC. Next Generation Access<br />
and Closure for NOTES: Tissue-Selective Hydro-Dissection for<br />
Efficient Gastric Flap Access with Photochemical Tissue Bonding for<br />
Secure Closure. Gastroenterology 2008; 134(4):A105.<br />
Sold MG, Grobholz R, Post S, Enderle MD, Kaehler GF. Submucosal<br />
cushioning with water jet before endoscopic mucosal resection:<br />
Which fluids are effective Surgical Endoscopy 2008; 22: 443-447.<br />
Yahagi N, Neuhaus H, Schumacher B, Neugebauer A, Kaehler GF,<br />
Schenk M, Fischer K, Fujishiro M, Enderle MD. Comparison of Standard<br />
Endoscopic Submucosal Dissection (<strong>ESD</strong>) Versus an Optimized <strong>ESD</strong><br />
Technique for Colon: An animal study. Endoscopy, 2009, accepted.<br />
Kähler et al. Combination of Water-Jet Dissection and Needle-Knife<br />
as a HybridKnife Simplifies Endoscopic Submucosal Dissection. Surgical<br />
Endoscopy 2009, accepted.<br />
Neuhaus H, Mayershofer R, Wirths K, Seelhoff A, Vieth M, Schumacher<br />
B. First clinical trial of endoscopic submucosal resection<br />
(<strong>ESD</strong>) of early gastric neoplasia with a water-jet HybridKnife (<strong>ESD</strong>H).<br />
Abstract accepted for DDW 2009.<br />
Neuhaus H, Wirths K, Schenk M, Enderle MD, Schumacher B. Randomized<br />
controlled study of endoscopic mucosal resection (EMR)<br />
versus endoscopic submucosal dissection with a water-jet Hybrid-<br />
Knife (<strong>ESD</strong>H) of esophageal lesions in a porcine model. Gastrointestinal<br />
Endoscopy 2009 Mar 13 (Epub ahead of print).<br />
Hyett B, Maurice, D, Matthes E, Carr-Locke D. Needle-Less Elevation<br />
for Endoscopic Mucosal Resection (EMR) in the Esophagus,<br />
Stomach and Colon. Abstract accepted for DDW 2009.<br />
HybridKnife<br />
11
<strong>ERBE</strong> <strong>Elektromedizin</strong> <strong>GmbH</strong><br />
Waldhoernlestraße 17<br />
72072 Tuebingen<br />
Germany<br />
Phone +49 7071 755-0<br />
Fax +49 7071 755-179<br />
info@erbe-med.com<br />
www.erbe-med.com<br />
85800-123 12.10 © <strong>ERBE</strong> <strong>Elektromedizin</strong> <strong>GmbH</strong> 2010