Guide to Managing Hepatitis C With Pegylated Interferons - CECity
Guide to Managing Hepatitis C With Pegylated Interferons - CECity
Guide to Managing Hepatitis C With Pegylated Interferons - CECity

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
This Special Report was<br />
supported by an<br />
educational grant from<br />
Schering <strong>Hepatitis</strong><br />
Innovations<br />
BROUGHT TO YOU BY THE PUBLISHER OF<br />
gastroendonews.com<br />
FACULTY<br />
Ira M. Jacobson, MD<br />
Vincent As<strong>to</strong>r Professor of Clinical<br />
Medicine<br />
Chief, Division of Gastroenterology<br />
and Hepa<strong>to</strong>logy<br />
Weill Medical College of Cornell<br />
University<br />
NewYork Presbyterian Hospital<br />
(Weill Cornell campus)<br />
New York, New York<br />
Dr. Jacobson is on the speaker’s<br />
bureau for Gilead Sciences and<br />
Schering-Plough, and is a consultant<br />
for Akros Pharma, Amgen, Cen<strong>to</strong>cor,<br />
InterMune, Ortho Biotech, Prometheus<br />
Labora<strong>to</strong>ries, Schering-Plough, and<br />
Valeant Pharmaceuticals. He has<br />
received grants/research support from<br />
InterMune, Isis Pharmaceuticals,<br />
Prometheus Labora<strong>to</strong>ries, Ribozyme<br />
Pharmaceuticals, and Schering-Plough.<br />
F. Fred Poordad, MD<br />
Assistant Professor of Medicine<br />
UCLA School of Medicine<br />
Associate Direc<strong>to</strong>r, Hepa<strong>to</strong>logy and<br />
Liver Transplantation<br />
Cedars-Sinai Medical Center<br />
Los Angeles, California<br />
Dr. Poordad is on the speaker’s<br />
bureau for Ortho Biotech, Roche<br />
Pharmaceuticals, and Schering-Plough,<br />
and is a consultant for Schering-<br />
Plough, Salix, and Prometheus Labora<strong>to</strong>ries.<br />
He has received grants/research<br />
support from Ribapharm, Roche<br />
Pharmaceuticals, and Schering-Plough.<br />
Jointly sponsored by the<br />
University of Kentucky<br />
and McMahon<br />
Publishing Group<br />
<strong>Guide</strong> <strong>to</strong> <strong>Managing</strong> <strong>Hepatitis</strong> C<br />
<strong>With</strong> <strong>Pegylated</strong> <strong>Interferons</strong><br />
NEEDS STATEMENT<br />
A CCREDITATION AND DESIG-<br />
NATION STATEMENTS<br />
This activity has been planned and implemented<br />
in accordance with the Essential Areas and policies<br />
of the Accreditation Council for Continuing Medical<br />
Education (ACCME) through the joint sponsorship of<br />
the University of Kentucky College of Medicine and<br />
McMahon Publishing Group. The University of Kentucky<br />
College of Medicine is accredited by the<br />
ACCME <strong>to</strong> provide continuing medical education for<br />
physicians.<br />
The University of Kentucky College of Medicine<br />
designates this educational activity for a maximum of<br />
1 category 1 credit <strong>to</strong>ward the AMA Physician’s<br />
Recognition Award. Each physician should claim<br />
only those hours of credit actually spent in the educational<br />
activity.<br />
TARGET AUDIENCE<br />
This educational program is intended for gastroenterologists.<br />
LEARNING OBJECTIVES<br />
After completing this educational activity, the participant<br />
should be able <strong>to</strong>:<br />
1 Describe the goals of peginterferon–ribavirin therapy<br />
for HCV infection.<br />
2 Define early virologic response, sustained virologic<br />
response, and the best predic<strong>to</strong>r of sustain virologic<br />
response, as related <strong>to</strong> peginterferon–<br />
ribavirin combination treatment for patients with<br />
HCV infection.<br />
3 Review clinical and patient fac<strong>to</strong>rs that make a difference<br />
in individualizing patient care and that<br />
influence therapeutic outcomes.<br />
CME CERTIFIED APRIL 2004<br />
Combination therapy with pegylated interferon<br />
and ribavirin enables clinicians <strong>to</strong> cure many<br />
patients infected with the hepatitis C virus (HCV)<br />
who may have otherwise progressed from an HCV<br />
infection <strong>to</strong> cirrhosis and, subsequently, hepa<strong>to</strong>cellular<br />
carcinoma. Yet, because many fac<strong>to</strong>rs influence<br />
efficacy and therapeutic outcomes, clinicians<br />
must educate themselves with regard <strong>to</strong> the use of<br />
this combination therapy in order target therapy<br />
<strong>to</strong>ward patients most likely <strong>to</strong> obtain benefit from it.<br />
METHOD OF PARTICIPATION<br />
This activity should take approximately 1 hour <strong>to</strong><br />
complete. The participant should, in order, read the<br />
objectives and monograph, answer the multiplechoice<br />
post-test, and complete the answer form, registration,<br />
and evaluation on page 8. This credit is valid<br />
through April 30, 2005.<br />
DISCLOSURE OF UNLABELED<br />
USE<br />
This educational activity contains discussion of<br />
published and/or investigational uses of peginterferon;<br />
some uses of these agents have not been<br />
approved by the Food and Drug Administration.<br />
Please refer <strong>to</strong> the official prescribing information for<br />
each product for discussion of approved indications,<br />
contraindications, and warnings.<br />
DISCLOSURE OF FINANCIAL<br />
INTEREST<br />
All faculty members participating in continuing<br />
medical education programs sponsored by the University<br />
of Kentucky Colleges of Pharmacy and Medicine<br />
Continuing Education Office are expected <strong>to</strong><br />
disclose any real or perceived conflict of interest related<br />
<strong>to</strong> the content of their presentations. Faculty disclosures<br />
are included herein.<br />
The University of Kentucky College of Medicine<br />
presents this activity for educational purposes<br />
only. Participants are expected <strong>to</strong> use their own<br />
expertise and judgment while engaged in the practice<br />
of medicine. The content of this educational<br />
activity is provided solely by the faculty, who have<br />
been selected because of recognized expertise in<br />
the field.<br />
Release Date: April 2004 Expiration Date: April 30, 2005
Introduction<br />
Recent therapeutic advances in the management of patients<br />
with hepatitis C virus (HCV) infection have raised the bar for<br />
expected outcomes. The best example of this has been the use<br />
of pegylated interferons. The majority of patients infected with<br />
HCV who have been treated with a combination of peginterferon<br />
and ribavirin have had sustained virologic response (SVR).<br />
<strong>With</strong> increasing experience indicating the rarity of virologic<br />
relapse in patients with SVR, clinicians are now able <strong>to</strong> include<br />
“cure of infection” among the goals of treatment. 1,2 While the<br />
National Institutes of Health’s Consensus Development Conference<br />
Statement on the Management of <strong>Hepatitis</strong> C suggests<br />
that all patients with hepatitis C could be considered as potential<br />
candidates for this therapy, 3 many patients infected with<br />
HCV represent complicated cases that require individualized<br />
attention with tailored dosing, careful moni<strong>to</strong>ring, and management<br />
of side effects. Therefore, clinicians need <strong>to</strong> consider individual<br />
patient characteristics <strong>to</strong> target therapy <strong>to</strong>ward those at<br />
greatest risk of progressive liver disease, with diligent attention<br />
<strong>to</strong> maximizing its <strong>to</strong>lerability.<br />
Maximizing Therapeutic Outcomes<br />
Ira M. Jacobson, MD<br />
Vincent As<strong>to</strong>r Professor of Clinical Medicine<br />
Chief, Division of Gastroenterology and Hepa<strong>to</strong>logy<br />
Weill Medical College of Cornell University<br />
NewYork Presbyterian Hospital (Weill Cornell campus)<br />
New York, New York<br />
Target Patient Population<br />
To maximize the benefits of peginterferon–ribavirin combination<br />
therapy, clinicians need <strong>to</strong> evaluate each candidate for<br />
symp<strong>to</strong>ms, degree of liver disease, risk of future progression,<br />
likelihood of response <strong>to</strong> therapy, and likelihood of <strong>to</strong>lerating<br />
therapy. Liver biopsy continues <strong>to</strong> play a major role in patient<br />
evaluation, although there is increasing interest in serum fibrosis<br />
assays and further data are awaited. Patients with HCV who<br />
are at particular risk of progressive fibrosis include those who<br />
Table 1. Key Definitions Used in Clinical Studies 7<br />
Negative predictive value: the chance of nonresponse<br />
<strong>to</strong> antiviral therapy in patients who have not achieved<br />
an early virologic response (EVR) by 12 weeks of<br />
treatment.<br />
Positive predictive value: the chance of achieving a<br />
sustained virologic response (SVR) in patients who<br />
have achieved an EVR.<br />
are over 40 years of age at the time of infection, and have a his<strong>to</strong>ry<br />
of alcoholism, persistently elevated levels of alanine<br />
transaminase (ALT) and aspartate transaminase (AST), coinfection<br />
with HIV, and a significant degree of necroinflamma<strong>to</strong>ry<br />
activity and fibrosis on liver biopsy. In addition, males and those<br />
patients with a body mass index >25 kg/m 2 appear <strong>to</strong> have an<br />
enhanced risk of progressive fibrosis. 4-6<br />
Many hepa<strong>to</strong>logists recommend liver biopsy even in patients<br />
whose liver enzyme levels are normal, because some such<br />
patients still have significant liver injury. Thus, the liver biopsy<br />
specimen can provide crucial information <strong>to</strong> help the clinician<br />
and the patient move <strong>to</strong> the next step. If the biopsy specimen indicates<br />
more than minimal fibrosis, then the patient should be treated.<br />
Even patients with minimal fibrosis should be informed of the<br />
option of treatment, since some of them may wish <strong>to</strong> attempt <strong>to</strong><br />
eradicate their infection. Some hepa<strong>to</strong>logists currently question<br />
the need for biopsy in selected patients, such as those with HCV<br />
genotype 2 or 3 and no evidence of cirrhosis, because therapy<br />
offers such a high chance of cure (80%). When therapy is decided<br />
upon, the duration of treatment is determined by the patient’s<br />
HCV genotype: for example, 24 weeks of therapy for HCV genotypes<br />
2 and 3, and 48 weeks for HCV genotype 1.<br />
Role of Early Virologic Response<br />
Once antiviral therapy has been started, the treating clinician<br />
can predict the chance of a patient achieving an SVR. Recently<br />
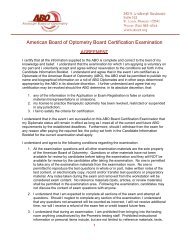
Table 2. Early Virologic Response (EVR) and Treatment Outcome:<br />
Peginterferon alfa-2b 1.5 mcg/kg + ribavirin 800 mg/d<br />
Viral Load Week EVR NPV PPV<br />
PCR neg 4 29% 59% 89%<br />
≥3 log10 drop 4 51% 75% 82%<br />
≥2 log10 drop 4 63% 87% 78%<br />
≥1 log10 drop 4 74% 95% 70%<br />
PCR neg 12 60% 91% 84%<br />
≥3 log10 drop 12 70% 95% 75%<br />
≥2 log10 drop 12 74% 100% 72%<br />
≥1 log10 drop 12 82% 100% 66%<br />
PCR neg 24 64% 99% 81%<br />
— — EVR Total % NR/No EVR %SVR/EVR<br />
2<br />
EVR, early virologic response; NPV, negative predictive value; NR, no response; PPV, positive predictive value; PCR neg, polymerase chain reaction negativity;<br />
SVR, sustained virologic response.<br />
Based on Hepa<strong>to</strong>logy 2003;38:645-652.
published data support the use of early virologic response<br />
(EVR) measurements as a means of predicting which patients<br />
will achieve SVR.<br />
This was the conclusion of data analysis from the trial by<br />
Manns et al, 1 which studied the combination of peginterferon<br />
alfa-2b and ribavirin. Davis et al evaluated EVR rates at 4, 12,<br />
and 24 weeks of therapy. The goal of the study was <strong>to</strong> help<br />
clinicians decide which HCV patients would benefit most from<br />
continued therapy, and <strong>to</strong> avoid the continuation of treatment in<br />
as many nonresponders as possible without depriving patients<br />
who might still have a realistic chance of SVR.<br />
The authors found that the time point that provided the greatest<br />
positive predictive value and negative predictive value for<br />
SVR among the definitions of EVR was ≥2 log10, or a hundredfold<br />
drop in viral load at 12 weeks of therapy (Tables 1 and 2). 7<br />
A ≥2 log10 drop in viral load at 12 weeks provided a 72% positive<br />
predictive value and a 100% negative predictive value. If a<br />
patient achieved an EVR at 12 weeks of therapy, there was a<br />
72% chance of achieving an SVR at the end of therapy. However,<br />
if a patient failed <strong>to</strong> achieve an EVR, the likelihood of a subsequent<br />
SVR during the trial was zero—there were no patients<br />
who achieved SVR among those who did not have a ≥2 log10<br />
drop at 12 weeks of therapy.<br />
Looking at the specific patient numbers, Davis et al 7 found<br />
that 380 of the 511 patients (74%) treated with 1.5 mcg/kg of<br />
peginterferon alfa-2b weekly plus 800 mg per day of ribavirin<br />
during the trial achieved an EVR (defined as ≥2 log10 drop in<br />
viral load at 12 weeks); again, the majority of patients (72%)<br />
went on <strong>to</strong> achieve an SVR. In contrast, none of the 131 patients<br />
who failed <strong>to</strong> achieve an EVR at 12 weeks achieved an SVR.<br />
In another trial, by Fried et al, 2 which studied the combination<br />
of peginterferon alfa-2a and ribavirin, 86% of patients treated<br />
with 180 mcg peginterferon alfa-2a once weekly plus 1,000 mg<br />
or 1,200 mg per day ribavirin (depending on body weight)<br />
achieved an EVR, which was defined as ≥2 log10 drop in viral<br />
load at 12 weeks. 8 In the Fried study, the positive predictive<br />
value was 65% (ie, 65% of those who achieved optimal EVR at<br />
12 weeks went on <strong>to</strong> achieve an SVR). The negative predictive<br />
value was approximately 97% (ie, 3% of those who did not<br />
achieve EVR at 12 weeks went on <strong>to</strong> achieve an SVR).<br />
When one is considering whether or not <strong>to</strong> terminate therapy<br />
based on EVR, these analyses support the 12-week time point<br />
as the best time <strong>to</strong> use in clinical practice. If a patient has mild<br />
fibrosis and virologic eradication is the sole goal of therapy,<br />
s<strong>to</strong>pping therapy can be considered appropriate at that time<br />
point in light of these data.<br />
Importance of Adherence<br />
Because of the significance of obtaining an EVR, clinicians<br />
need <strong>to</strong> educate patients about the importance of adhering <strong>to</strong><br />
their therapeutic regimen, particularly during the initial 12-<br />
week period.<br />
Using the Manns et al trial data, 1 Davis et al found that if a<br />
patient <strong>to</strong>ok ≥80% of the peginterferon dose and ≥80% of the<br />
ribavirin dose during the first 12 weeks of therapy, the patient’s<br />
response rate was optimal. 7 However, if the patient <strong>to</strong>ok
On the basis of this analysis, some clinicians would recommend<br />
continuing therapy beyond the 12-week time point, for as<br />
long as 6 <strong>to</strong> 12 months, in patients with advanced fibrosis who<br />
have failed <strong>to</strong> achieve an EVR, as defined by ≥2 log10 drop in<br />
viral load, <strong>to</strong> potentially maximize the his<strong>to</strong>logic benefit.<br />
Maintenance Therapy<br />
There are ongoing investigations that take this concept a<br />
step further—continuing therapy beyond the 12-month treatment<br />
period in a maintenance form of therapy. The rationale behind<br />
this approach is that if 6 <strong>to</strong> 12 months of treatment can reduce<br />
inflammation and fibrosis, perhaps further treatment would provide<br />
further benefit. To date, the only published prospective trial<br />
on maintenance therapy has indicated a significant reduction in<br />
inflamma<strong>to</strong>ry scores and a trend <strong>to</strong>ward less fibrosis. 12 Currently,<br />
there are 3 ongoing studies exploring maintenance therapy—<br />
HALT-C (<strong>Hepatitis</strong> C Antiviral Long-Term Treatment Against<br />
Cirrhosis), which is evaluating peginterferon alfa-2a plus ribavirin,<br />
COPILOT (Colchicine Versus PEG-Intron Long-Term),<br />
and EPIC (Evaluation of PEG-Intron in Chronic <strong>Hepatitis</strong> C Cirrhosis).<br />
The latter 2 studies are evaluating peginterferon alfa-2b;<br />
all 3 of the maintenance trials are evaluating lower dosing regimens.<br />
Nezam H. Afdhal, MD, presented preliminary data from<br />
the COPILOT trial at the 2002 American Association for the<br />
Study of Liver Diseases meeting, which indicated the possible<br />
beginning of a trend <strong>to</strong>ward fewer significant clinical events in<br />
patients treated with peginterferon alfa-2b, given at a dose of<br />
0.5 mcg/kg once weekly, than in those treated with colchicine<br />
0.6 mg twice daily. 13 Further data are awaited.<br />
Treatment Algorithm<br />
All patients infected with HCV and treated with peginterferon–ribavirin<br />
combination therapy should be evaluated for success<br />
of therapy based on the optimal EVR at 12 weeks (Figure<br />
2). If a patient has a ≥2 log10 drop in HCV RNA, or HCV RNA is<br />
undetectable, treatment should be continued. The continuation<br />
of treatment beyond 24 weeks is determined based on the<br />
patient’s genotype: HCV genotype 1 patients should continue<br />
therapy for 48 weeks if HCV RNA is negative; if HCV RNA is still<br />
positive at week 24, cessation of therapy should be considered.<br />
Generally, HCV genotype 2 and 3 patients should s<strong>to</strong>p therapy<br />
at 24 weeks if HCV RNA is negative. One possible exception <strong>to</strong><br />
this rule might be patients with cirrhosis, but this is a controversial<br />
issue. Patients with METAVIR scores of F3 or F4 beyond 12<br />
weeks, even if no EVR was demonstrated, might be treated<br />
longer <strong>to</strong> accrue additional his<strong>to</strong>logic benefit. Similarly, patients<br />
defined as late responders might benefit from treatment for<br />
more than a year; but this is unproven. At the end of treatment<br />
in responders, qualitative testing, with either PCR or transcription<br />
mediated amplification (TMA), should be performed. Testing<br />
should be repeated 6 months later <strong>to</strong> assess patient<br />
outcome.<br />
Conclusion<br />
To maximize the benefits of peginterferon–ribavirin combination<br />
therapy in the HCV-infected patient, clinicians should first<br />
educate the patient on the importance of adhering <strong>to</strong> the therapeutic<br />
regimen, and then measure the patient’s EVR at the 12-<br />
week time point. The EVR rate can reliably predict therapeutic<br />
outcomes and can serve as the basis for avoiding unnecessary<br />
continuation of therapy in those patients least likely <strong>to</strong> benefit<br />
from it. There is some preliminary evidence 12,13 that prolonging<br />
therapy in selected patients, or placing patients on maintenance<br />
therapy, may be considered <strong>to</strong> reduce inflammation and,<br />
potentially, prevent progression of fibrosis. At least 3 multicenter<br />
studies on maintenance therapy with peginterferon are in<br />
progress. The concept of prolonging therapy beyond 48 weeks<br />
in late responders, prior nonresponders, or prior relapsers<br />
requires additional evaluation.<br />
Week 12:<br />
Quantitative HCV RNA testing (determine EVR)<br />
Patient Management Issues<br />
F. Fred Poordad, MD<br />
Assistant Professor of Medicine<br />
UCLA School of Medicine<br />
Associate Direc<strong>to</strong>r, Hepa<strong>to</strong>logy and Liver Transplantation<br />
Cedars-Sinai Medical Center<br />
Los Angeles, California<br />
To maximize the likelihood of achieving an SVR in patients<br />
infected with HCV taking peginterferon–ribavirin combination<br />
therapy, clinicians need <strong>to</strong> carefully moni<strong>to</strong>r for and treat disease<br />
complications and medication side effects that might<br />
hamper treatment success. Such complications and side<br />
effects can lead <strong>to</strong> decreased adherence <strong>to</strong> the therapeutic regimen—dose<br />
reductions and premature discontinuation of therapy<br />
(Table 3). 1,2 This decreased adherence <strong>to</strong> the treatment<br />
regimen, in turn, lessens the efficacy of therapy and the likelihood<br />
of achieving an SVR. 1,14,15 Following is an overview of<br />
some of the more common side effects of interferon therapy<br />
and treatment options.<br />
Table 3. The Frequency of Therapeutic Adjustments<br />
In Patients Treated <strong>With</strong> Peginterferon and<br />
Ribavirin<br />
Peginterferon<br />
alfa-2a Plus<br />
Ribavirin (%)<br />
Dose Modifications 32 42<br />
Premature<br />
Discontinuation<br />
10 14<br />
Adverse Events 7 12<br />
Labora<strong>to</strong>ry<br />
Abnormalities<br />
3 2<br />
Peginterferon<br />
alfa-2b Plus<br />
Ribavirin (%)<br />
Based on Lancet 2001;358:959-965 and N Engl J Med 2002;347:975-982.<br />
Depression<br />
Depression is a significant comorbid fac<strong>to</strong>r <strong>to</strong> consider when<br />
treating HCV-infected patients. Depression is uncovered in one<br />
third of patients at the time of diagnosis of HCV infection. 14 The<br />
reasons for the high rate of depression in this population may in<br />
part be related <strong>to</strong> fatigue or patients’ concerns about their<br />
future health. 16 In addition, interferon treatment can contribute<br />
<strong>to</strong> depression in HCV-infected patients. However, depression<br />
can be treated and should not be a limiting fac<strong>to</strong>r for the treatment<br />
of patients with HCV with peginterferon–ribavirin combination<br />
therapy. 3<br />
There are several theories as <strong>to</strong> what causes depression in<br />
HCV-infected patients treated with interferon. Sero<strong>to</strong>nin depletion<br />
is one of them. Sero<strong>to</strong>nin is one of the important molecules<br />
involved in the pathogenesis of depression. Interferon-related<br />
depression is thought <strong>to</strong> occur through sero<strong>to</strong>nin depletion via<br />
depletion of tryp<strong>to</strong>phan, the substrate required for sero<strong>to</strong>nin<br />
production. Tryp<strong>to</strong>phan has <strong>to</strong> compete competitively with an<br />
active transport mechanism <strong>to</strong> get in<strong>to</strong> the brain <strong>to</strong> produce<br />
sero<strong>to</strong>nin. <strong>Interferons</strong>, interleukin-2, and other cy<strong>to</strong>kines deplete<br />
the peripheral tryp<strong>to</strong>phan supply, and, as a result, the brain has<br />
less substrate <strong>to</strong> form sero<strong>to</strong>nin. The selective sero<strong>to</strong>nin reuptake<br />
inhibi<strong>to</strong>rs (SSRIs) are often effective in treating depression<br />
in HCV-infected patients being treated with interferon, which<br />
supports the idea that sero<strong>to</strong>nin is involved.<br />
Class Effect<br />
There are no data directly comparing the efficacy or side<br />
effects of peginterferon alfa-2a and peginterferon alfa-2b that<br />
demonstrate one induces a higher incidence of depression<br />
than the other. Although the frequency of depression differed<br />
between the 2 trials of peginterferon (eg, 22% in the peginterferon<br />
alfa-2a trial and 31% in the peginterferon alfa-2b trial), 1,2<br />
there were important differences between these trials that likely<br />
led <strong>to</strong> this discrepancy. First, in both of these studies, the diagnosis<br />
of depression was very subjective; no validated <strong>to</strong>ols were<br />
used. Second, in the peginterferon alfa-2a registration trials,<br />
26% of patients discontinued therapy at 12 weeks, so only 74%<br />
of the patients in the trial par<strong>to</strong>ok of the full year of therapy; this<br />
contrasts with a 14% discontinuation rate among patients in the<br />
peginterferon alfa-2b trial. It is likely that the rates of depression<br />
would have been different if the entire population in the peginterferon<br />
alfa-2a trial had been treated for the full 48 weeks. Finally,<br />
there are geographic differences in diagnosed depression<br />
rates. The registration study of peginterferon alfa-2b was conducted<br />
at predominantly North American sites, whereas the<br />
majority of sites in the peginterferon alfa-2a registration study<br />
were European.<br />
Treatment Options<br />
There is emerging evidence that SSRIs may be the agents of<br />
choice for treating interferon-associated depression in patients<br />
with hepatitis C. 17,18 In a small study, Kraus et al treated 14<br />
patients with HCV and depression using paroxetine 20 mg per<br />
day. The study results found that depression scores declined in<br />
all the patients, and 11 patients were able <strong>to</strong> complete interferon<br />
therapy. 16<br />
In patients with liver disease, SSRIs have been shown <strong>to</strong> be<br />
safe and well <strong>to</strong>lerated. 19 The choice of which SSRI agent <strong>to</strong> prescribe<br />
should be based on patient symp<strong>to</strong>ms (ie, in patients with<br />
fatigue or cognitive slowing, the more activating agents [fluoxetine<br />
and sertraline] may be preferred <strong>to</strong> the less activating agents<br />
[paroxetine and fluvoxamine]). 20 Other first-line antidepressants<br />
(eg, venlafaxine, bupropion, and nefazodone) may have efficacy<br />
similar <strong>to</strong> that of the more activating SSRIs, but they have not<br />
been as well studied in HCV-infected patients. 15 Tricyclic antidepressants,<br />
which have an anticholinergic effect and may cause<br />
sedation, should be avoided in this population, particularly if pronounced<br />
fatigue and cognitive slowing are present. 15<br />
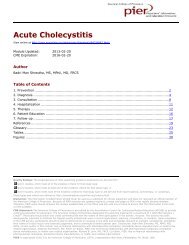
Hema<strong>to</strong>logic Side Effects<br />
Hema<strong>to</strong>logic side effects—anemia, neutropenia, and thrombocy<strong>to</strong>penia—frequently<br />
necessitate dosage modifications or<br />
discontinuation in HCV-infected patients taking peginterferon–ribavirin<br />
combination therapy, and such dose reductions<br />
adversely affect the ability <strong>to</strong> achieve SVR. 1,2 Regardless of the<br />
peginterferon product used, the rate of achieving SVR will<br />
decrease by a significant 17% <strong>to</strong> 29% if the patients receive<br />
16%<br />
14%<br />
12%<br />
10%<br />
8%<br />
6%<br />
14.2: 1.7 g/dL<br />
11.2: 1.3 g/dL<br />
EPO<br />
SOC<br />
4%<br />
2%<br />
0%<br />
N=62<br />
EPO<br />
SOC<br />
Study<br />
Entry<br />
34<br />
28<br />
Week<br />
2<br />
31<br />
23<br />
Week<br />
4<br />
34<br />
21<br />
Week<br />
8<br />
33<br />
21<br />
Week<br />
12<br />
29<br />
15<br />
Week<br />
16<br />
21<br />
14<br />
Figure 3. <strong>Pegylated</strong> interferons: anemia.<br />
Based on references 21 and 22.<br />
levels in this population. In one study, Dieterich and Spivak<br />
randomly assigned 62 patients <strong>to</strong> receive either the standard of<br />
care (dose reduction) or treatment with erythropoietin if they<br />
became anemic (Figure 3). 21,22 Although the baseline ribavirin<br />
doses were similar (approximately 1,000 mg per day), the mean<br />
reduction in ribavirin dose was significantly less for the group<br />
that received erythropoietin. In addition, there was a 3-g/dL<br />
difference in the hemoglobin level measured at 3 months in the<br />
group receiving erythropoietin from that of the standard-of-care<br />
treatment group. The erythropoietin-treated patients also had<br />
higher quality-of-life scores.<br />
If the hemoglobin level falls below 12 g/dL and the patient<br />
has symp<strong>to</strong>ms of anemia, or if the hemoglobin level falls below<br />
10 g/dL, once-weekly erythropoietin treatment can be beneficial.<br />
If the patient is iron depleted, iron should be given as well.<br />
Neutropenia<br />
Neutropenia occurs more commonly among patients treated<br />
with pegylated interferons than nonpegylated interferons. Granulocyte<br />
colony–stimulating fac<strong>to</strong>r (G-CSF) has become widely<br />
used in this setting <strong>to</strong> treat neutropenia and thereby reduce the<br />
need for dose reduction and the discontinuation of antiviral<br />
therapy. This growth fac<strong>to</strong>r serves <strong>to</strong> bolster neutrophil counts,<br />
allowing higher doses of interferon <strong>to</strong> be administered. One<br />
approach <strong>to</strong> neutropenia management in this patient population<br />
is <strong>to</strong> institute G-CSF therapy when the absolute neutrophil<br />
count (ANC) falls below 500/mm 3 , although some have advocated<br />
starting at an ANC of 1,000/mm 3 . G-CSF is generally<br />
administered at a dose of 300 mcg 1 <strong>to</strong> 3 times weekly, then<br />
titrated <strong>to</strong> maintain an ANC above 750/mm 3 . Although the use<br />
of this supportive agent has been shown <strong>to</strong> allow increased<br />
interferon dosing, more studies are needed <strong>to</strong> determine<br />
whether this translates in<strong>to</strong> an increase in SVR. Importantly,<br />
there have been no studies in this treatment population correlating<br />
low ANC with infections.<br />
Conclusion<br />
In summary, advances in the treatment of HCV infection with<br />
peginterferon–ribavirin combination therapy offer patients a<br />
good chance of achieving an SVR, but clinicians need <strong>to</strong> closely<br />
moni<strong>to</strong>r patients for the development of side effects, particularly<br />
depression, anemia, and neutropenia. Depression occurs<br />
with all classes of interferon, and can be treated wirh antidepressant<br />
agents. The development of hema<strong>to</strong>logic side effects<br />
should also be anticipated when one is treating patients with<br />
peginterferon–ribavirin combination therapy, and managed with<br />
available supportive agents. Careful management of these<br />
potential side effects can improve therapeutic outcomes.<br />
6<br />
References<br />
1. Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alfa-2b plus<br />
ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment<br />
of chronic hepatitis C: a randomised trial. Lancet. 2001;358:959-965.<br />
2. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin<br />
for chronic hepatitis C virus infection. N Engl J Med. 2002;347:<br />
975-982.<br />
3. National Institutes of Health Consensus Development Conference<br />
Statement: Management of hepatitis C 2002. Gastroenterology. 2002;<br />
123:2082-2099.<br />
4. Poynard T, Bedossa P, Opolon P. Natural his<strong>to</strong>ry of liver fibrosis progression<br />
in patients with chronic hepatitis C. The OBSVIRC, METAVIR, CLIN-<br />
IVIR, and DOSVIRC groups. Lancet. 1997;349:825-832.<br />
5. Yano M, Kumada H, Kage M, et al. The long-term pathological evolution of<br />
chronic hepatitis C. Hepa<strong>to</strong>logy. 1996;23:1334-1340.<br />
6. Mathurin P, Moussalli J, Cadranel JF, et al. Slow progression rate of fibrosis<br />
in hepatitis C virus patient with persistently normal alanine transaminase<br />
activity. Hepa<strong>to</strong>logy. 1998;27:868-872.<br />
7. Davis GL, Wong JB, McHutchison JG, Manns MP, Harvey J, Albrecht J.<br />
Early virologic response <strong>to</strong> treatment with peginterferon alfa-2b plus ribavirin<br />
in patients with chronic hepatitis C. Hepa<strong>to</strong>logy. 2003;38:645-652.
References (continued)<br />
8. Ferenci P, Fried MW, Chaneac M. A dynamic model <strong>to</strong> predict sustained<br />
virological response <strong>to</strong> combination peginterferon alfa-2a and ribavirin<br />
therapy in patients with chronic hepatitis C. Hepa<strong>to</strong>logy. 2003;38(Oct<br />
suppl):635A. Abstract #995.<br />
9. Buti M, Valdes A, Sanchez-Avila F, Esteban R, Lurie Y. Extending combination<br />
therapy with peginterferon alfa-2b plus ribavirin for genotype 1<br />
chronic hepatitis C late responders: a report of 9 cases. Hepa<strong>to</strong>logy.<br />
2003;37:1226-1227.<br />
10. Berg T, Hinrichsen H, Heintges T, et al. Comparison of 48 or 72 weeks of<br />
treatment with peginterferon alfa-2a plus ribavirin in treatment-naïve<br />
patients with chronic hepatitis C infected with HCV genotype 1. Hepa<strong>to</strong>logy.<br />
2003;38(Oct suppl):317A. Abstract #328.<br />
11. Poynard T, McHutchison JG, Manns MP, et al. Impact of pegylated interferon<br />
alfa-2b and ribavirin on liver fibrosis in patients with chronic hepatitis<br />
C. Gastroenterology. 2002;122:1303-1313.<br />
12. Shiffman ML, Hofmann CM, Con<strong>to</strong>s MJ, et al. A randomized, controlled<br />
trial of maintenance interferon therapy for patients with chronic hepatitis C<br />
virus and persistent viremia. Gastroenterology. 1999;117:1164-1172.<br />
13. Afdhal NH, Freilich B, Black M, et al. Comparison of therapy with PEG-<br />
Intron 0.5 mcg/kg versus colchicine 0.6 mg bid in 250 patients with cirrhosis<br />
and HCV: interim data from COPILOT. Hepa<strong>to</strong>logy. 2002;36:312A.<br />
14. McHutchison JG, Manns MP, Patel K, et al. Adherence <strong>to</strong> combination<br />
therapy enhances sustained response in genotype-1–infected patients<br />
with chronic hepatitis C. Gastroenterology. 2002;123:1061-1069.<br />
15. Zdilar D, Franco-Bronson K, Buchler N, Locala JA, Younossi ZM. <strong>Hepatitis</strong><br />
C, interferon alfa, and depression. Hepa<strong>to</strong>logy. 2000;31:1207-1211.<br />
16. Kraus MR, Schafer A, Faller H, Csef H, Scheurlen M. Paroxetine for the<br />
treatment of interferon-alpha–induced depression in chronic hepatitis C.<br />
Aliment Pharmacol Ther. 2002;16:1091-1099.<br />
17. Hauser P, Khosla J, Aurora H, et al. A prospective study of the incidence<br />
and open-label treatment of interferon-induced major depressive disorder<br />
in patients with hepatitis C. Mol Psychiatry. 2002;7:942-947.<br />
18. Epstein SA. Psychotropic medications in gastrointestinal and hepatic disease.<br />
Adv Psychosom Med. 1994;21:49-60.<br />
19. Edwards JG, Anderson I. Systematic review and guide <strong>to</strong> selection of<br />
selective sero<strong>to</strong>nin reuptake inhibi<strong>to</strong>rs. Drugs. 1999;57:507-533.<br />
20. Russo MW, Fried MW. Side effects of therapy for chronic hepatitis C. Gastroenterology.<br />
2003;124:1711-1719.<br />
21. Dieterich DT, Spivak JL. Hema<strong>to</strong>logic disorders associated with hepatitis<br />
C virus infection and their management. Clin Infect Dis. 2003;37:533-541.<br />
22. Dieterich DT. Once-weekly recombinant human erythropoietin (epoetin<br />
alfa) facilitates optimal ribavirin (RBV) dosing in hepatitis C virus (HCV)-<br />
infected patients receiving interferon alfa-2 (INF)/RBV combination therapy.<br />
Presented at Digestive Disease Week; May 20-23, 2001; Atlanta, Ga.<br />
Abstract #340.<br />
CME Post-test<br />
Select the single-letter response that best answers the question or completes the sentence.<br />
1. All but which of the following risk fac<strong>to</strong>rs put HCVinfected<br />
patients at higher risk for liver fibrosis and<br />
further progression of liver disease<br />
a. Male sex<br />
b. Long duration of infection<br />
c. Hypercholesterolemia<br />
d. His<strong>to</strong>ry of alcoholism<br />
2. In general, genotype 1 patients should be treated for:<br />
a. 12 weeks<br />
b. 24 weeks<br />
c. 48 weeks<br />
d. 72 weeks<br />
3. Based on Davis et al’s evaluation of the Manns et al<br />
data, the best definition and time point <strong>to</strong> measure<br />
EVR are:<br />
a. ≥1 log10 drop in viral load at 4 weeks<br />
b. ≥1 log10 drop in viral load at 12 weeks<br />
c. ≥2 log10 drop in viral load at 4 weeks<br />
d. ≥2 log10 drop in viral load at 12 weeks<br />
4. What was the negative predictive value when EVR was<br />
defined as ≥2 log10 drop in viral load at 12 weeks<br />
a. 0%<br />
b. 20%<br />
c. 50%<br />
d. 100%<br />
5. Evaluating the Manns et al trial data, Davis et al found<br />
that early discontinuation or interruptions of therapy<br />
longer than 2 weeks reduced SVR:<br />
a. from 82% <strong>to</strong> 70%<br />
b. from 72% <strong>to</strong> 50%<br />
c. from 62% <strong>to</strong> 40%<br />
d. from 45% <strong>to</strong> 25%<br />
6. The COPILOT maintenance trial is evaluating the<br />
efficacy of lower than standard-dose peginterferon<br />
alfa-2b compared with:<br />
a. calci<strong>to</strong>nin<br />
b. colchicine<br />
c. erythropoietin<br />
d. G-CSF<br />
7. Interferon-related depression is thought <strong>to</strong> occur<br />
through sero<strong>to</strong>nin depletion via depletion of:<br />
a. vitamin A<br />
b. vitamin B<br />
c. dimethylglycine<br />
d. tryp<strong>to</strong>phan<br />
8. The more activating SSRIs include:<br />
a. fluoxetine and paroxetine<br />
b. paroxetine and fluvoxamine<br />
c. fluoxetine and sertraline<br />
d. sertraline and paroxetine<br />
9. Tricyclic antidepressants should be avoided in HCVinfected<br />
patients with depression because of potential:<br />
a. anticholinergic side effects<br />
b. sexual side effects<br />
c. cholinergic effects<br />
d. weight gain<br />
10. In the treatment of peginterferon-related neutropenia,<br />
G-CSF is generally started at a dose of:<br />
a. 300 mcg 1 <strong>to</strong> 3 times weekly<br />
b. 300 mcg 1 <strong>to</strong> 3 times daily<br />
c. 500 mg 1 <strong>to</strong> 3 times weekly<br />
d. 500 mcg 1 <strong>to</strong> 3 times weekly<br />
7
ANSWER SHEET & EVALUATION FORM<br />
<strong>Guide</strong> <strong>to</strong> <strong>Managing</strong> <strong>Hepatitis</strong> C <strong>With</strong> <strong>Pegylated</strong> <strong>Interferons</strong><br />
Release Date: April 2004 Expiration Date: April 30, 2005<br />
✄<br />
A passing score of 70% or higher on the post-test awards the participant one (1) AMA PRA Category 1 credit. To claim<br />
continuing education credit, individuals must complete the self-study activity, post-test and evaluation. Please submit your<br />
answers only once through one of the methods listed below.<br />
Mail <strong>to</strong>: Attn: Distance Education or Participate online at: Test Code: MDEMHC03<br />
Continuing Education Office<br />
www.gastroendonews.com<br />
Colleges of Pharmacy and Medicine<br />
University of Kentucky<br />
One Quality Street, 6th Floor<br />
Lexing<strong>to</strong>n, KY 40507-1428<br />
Must be postmarked by April 30, 2005<br />
Participant Information: (Please print)<br />
Name:<br />
Credentials: Soc. Sec. #:<br />
Address:<br />
City: State: Zip:<br />
Daytime Phone:<br />
Fax:<br />
E-mail:<br />
Signature:<br />
1. a b c d<br />
2. a b c d<br />
3. a b c d<br />
4. a b c d<br />
5. a b c d<br />
Post-Test Answers:<br />
6. a b c d<br />
7. a b c d<br />
8. a b c d<br />
9. a b c d<br />
10. a b c d<br />
Evaluation:<br />
Ratings: 1=Poor 3=Satisfac<strong>to</strong>ry 5=Excellent<br />
1. Extent <strong>to</strong> which the objectives were achieved: 1 2 3 4 5<br />
2. Potential impact on your practice: 1 2 3 4 5<br />
3. Detail of information presented: 1 2 3 4 5<br />
4. Overall evaluation of this CE activity: 1 2 3 4 5<br />
5. Suggestions for future CE <strong>to</strong>pics:<br />
SR326<br />
8