Improving Code Blue Response Through the Use of Simulation
Improving Code Blue Response Through the Use of Simulation
Improving Code Blue Response Through the Use of Simulation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Improving</strong> <strong>Code</strong> <strong>Blue</strong> <strong>Response</strong><br />
<strong>Through</strong> <strong>the</strong> <strong>Use</strong> <strong>of</strong> <strong>Simulation</strong><br />
Kelley F. Huseman, MSN, RN-BC, CCRN<br />
Ephrata Community Hospital<br />
Ephrata, PA
OBJECTIVES<br />
• list <strong>the</strong> AHA benchmarks <strong>of</strong> best practice<br />
for resuscitation<br />
• list problems with current resuscitation<br />
training<br />
• name advantages <strong>of</strong> simulation in<br />
resuscitation training<br />
• discuss <strong>the</strong> research project and results<br />
<strong>of</strong> project relating to improving response<br />
time for a cardiac arrest
Overview <strong>of</strong> <strong>the</strong> Research Project<br />
Project Choice:<br />
Requested by Executive Management to<br />
improve code blue response<br />
Various approaches tried and failed<br />
Given gift <strong>of</strong> high fidelity patient simulator<br />
(iStan)<br />
Initiated code blue drills in hospital<br />
Needed to assess effectiveness
Overview<br />
Research Question:<br />
Will participation in simulated code blue<br />
drills improve code blue response times<br />
and will <strong>the</strong> improvements be sustained
Literature Review<br />
Stressors <strong>of</strong> Resuscitation<br />
Best Practices<br />
Importance <strong>of</strong> Timely <strong>Response</strong><br />
Issues with Current Training<br />
Effects <strong>of</strong> <strong>Simulation</strong> on Practice<br />
Barriers to <strong>the</strong> <strong>Use</strong> <strong>of</strong> <strong>Simulation</strong>
Stressors <strong>of</strong> Resuscitation<br />
• High Risk-Low Volume<br />
• Team must function effectively and<br />
quickly in order to have a good outcome<br />
• Nurses report feeling incompetent in<br />
performing in a code blue situation<br />
• Many are uncertain as to <strong>the</strong>ir role in a<br />
code blue
AHA Best Practices<br />
• Chest compressions start within one<br />
minute<br />
• Defibrillation performed within three<br />
minutes<br />
• Epinephrine administered within five<br />
minutes
Importance <strong>of</strong> Timely <strong>Response</strong><br />
• Average survival rate 10%<br />
• Delays in treatment increase <strong>the</strong><br />
likelihood <strong>of</strong> death 1.1 times per minute <strong>of</strong><br />
delay<br />
• For every minute defibrillation delayed,<br />
survival rates decrease by 10%<br />
• The shorter <strong>the</strong> time between arrest and<br />
intervention, <strong>the</strong> better <strong>the</strong> chance for<br />
survival
Issues with Current Training<br />
• Majority <strong>of</strong> healthcare workers cannot<br />
perform appropriately in an arrest<br />
situation<br />
• Skills erode within <strong>the</strong> first three months<br />
after training<br />
• Structured classes are unrealistic<br />
• Scheduled classes cannot replicate <strong>the</strong><br />
anxiety <strong>of</strong> a true arrest situation
Effects <strong>of</strong> <strong>Simulation</strong> on Practice<br />
• IOM has recommended simulation<br />
training to reduce errors<br />
• Skills and clinical decision making can be<br />
practiced in a nonthreatening<br />
environment<br />
• Less stressful than real life<br />
• More realistic than traditional training<br />
• Remediation and debriefing can be done<br />
immediately<br />
• Enjoyed by participants
Barriers to <strong>the</strong> <strong>Use</strong> <strong>of</strong> <strong>Simulation</strong><br />
• Expense<br />
• Expertise<br />
• Facilitator availability<br />
• Staff and physician buy-in
Overview <strong>of</strong> <strong>the</strong> Project<br />
Quasi-experimental, single sample<br />
Cannot predict who, where or when<br />
code will occur<br />
Cannot manipulate variables<br />
Cannot predict staff responders
Overview <strong>of</strong> <strong>the</strong> Project<br />
Setting<br />
Small Community Hospital<br />
Participants<br />
All patients/staff involved in code blue<br />
Procedure<br />
Conducted Mock <strong>Code</strong> Drills<br />
Measured code response times pre and posttraining
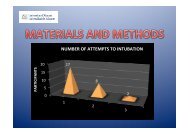
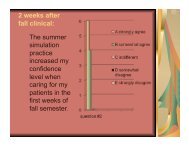
Results & Discussion<br />
Improvement in mean times for:<br />
Chest compressions<br />
Epinephrine dose<br />
Defibrillation<br />
Pretraining<br />
Post -<br />
training<br />
Q 2, 2010<br />
Chest<br />
Compressions<br />
0.867 min 0.214 min 0.375 min<br />
Epinephrine 4 min 0.929 min 0.05 min<br />
Defibrillation 3.286 min 1 min 1 min
Results & Discussion<br />
Mean <strong>Response</strong> Times<br />
6<br />
5<br />
Minutes<br />
4<br />
3<br />
2<br />
Benchmark<br />
Pre-training<br />
Post-training<br />
Maintenance<br />
1<br />
0<br />
Compressions Epinephrine Defibrillation
Results & Discussion<br />
t- tests<br />
Chest Compressions<br />
Pre to post training t = 2.8717 (p = 0.0079)*<br />
Post-training to Q 2 t = 0.5517 (p = 0.5983)#<br />
Epinephrine<br />
Pre to post training t = 4.6602 (p = 0.0001)*<br />
Post-training to Q 2 t = 0.5517 (p = 0.5517)#<br />
Defibrillation<br />
Pre to post training t = 1.7778 (p = 0.1008)<br />
Post-training to Q 2 t = 0.0000 (p = 1.000)<br />
*Statistically significant<br />
#Sustained improvement
Conclusions<br />
The use <strong>of</strong> simulation appears to have a<br />
positive impact on code blue response<br />
times.<br />
These results were sustained through <strong>the</strong><br />
second quarter <strong>of</strong> 2012.
Implications & Suggested Changes<br />
Retention <strong>of</strong> resuscitation skills declines<br />
rapidly after BLS and ACLS training.<br />
These training classes occur formally<br />
every 2 years.<br />
In order to maintain skills, staff needs to<br />
participate in practice sessions.<br />
Unannounced code blue drills appear to<br />
assist with skill retention<br />
<strong>Code</strong> blue drills should continue to be<br />
conducted on at least a monthly basis
Limitations<br />
Small number <strong>of</strong> actual patient codes<br />
It is possible that response did not<br />
change, but documentation improved<br />
Confidence levels were not directly<br />
measured, fur<strong>the</strong>r study should be<br />
conducted relative to confidence levels
Bibliography<br />
Adams, D., Dobbs, J., Greene, M., MacGillis, P., & Stockhausen, P. (2002). A model to enhance staff response in<br />
cardiopulmonary arrest. Journal <strong>of</strong> Nursing Care Quality, 17(1), 43-50.<br />
Ali, B., & Zafari, A. (2007). Narrative review: cardiopulmonary resuscitation and emergency cardiovascular care:<br />
review <strong>of</strong> <strong>the</strong> current guidelines [corrected] [published erratum appears in ANN INTERN MED 2007 Oct 16;147<br />
(8):592].<br />
American Heart Association. (2005). American Heart Association Guidelines for Cardiopulmonary Resuscitation and<br />
Emergency Cardiovascular Care. Circulation 2005, 112: IV-1 – IV-211.<br />
Asselin, M., & Cullen, H. (2002). Staff development special. A new beat for BLS and ACLS guidelines. Nursing<br />
Management, 33(2), 31-38.<br />
Beyea, S. (2004). Human patient simulation: a teaching strategy. AORN Journal, 80(4), 738.<br />
Brannan, J., White, A., & Bezanson, J. (2008). Simulator effects on cognitive skills and confidence levels. Journal <strong>of</strong><br />
Nursing Education, 47(11), 495-500.<br />
Broomfield, R. (1996). A quasi-experimental research to investigate <strong>the</strong> retention <strong>of</strong> basic cardiopulmonary<br />
resuscitation skills and knowledge by qualified nurses following a course in pr<strong>of</strong>essional development. Journal<br />
<strong>of</strong> Advanced Nursing, 23(5), 1016-1023.<br />
Broussard, L. (2008). <strong>Simulation</strong>-based learning: how simulators help nurses improve clinical skills and preserve<br />
patient safety. Nursing for Womens Health, 12(6), 521-524.<br />
Chan, P. (2009). Hospital variation in time to defibrillation after in-hospital cardiac arrest. Archives <strong>of</strong> Internal<br />
Medicine, 169(14): 1265-1273.<br />
Davies, N., & Gould, D. (2000). Updating cardiopulmonary resuscitation skills: a study to examine <strong>the</strong> efficacy <strong>of</strong><br />
self-instruction on nurses' competence. Journal <strong>of</strong> Clinical Nursing, 9(3), 400-410.<br />
Dichtwald, S., Matot, I., & Einav, S. (2009). <strong>Improving</strong> <strong>the</strong> Outcome <strong>of</strong> In-Hospital Cardiac Arrest: The Importance <strong>of</strong><br />
Being EARNEST. Seminars in Cardiothoracic & Vascular Anes<strong>the</strong>sia, 13(1), 19-30.<br />
Donovan, D., & Abella, B. (2009). Are your CPR skills up to speed <strong>Improving</strong> CPR and resuscitation care in <strong>the</strong><br />
field. EMS Magazine, 38(2), 33.<br />
Futterman, L., & Lemberg, L. (2005). Cardiology casebook. Cardiopulmonary resuscitation review: critical role <strong>of</strong><br />
chest compressions. American Journal <strong>of</strong> Critical Care, 14(1), 81-84.<br />
Good, M. (2005). Patient simulation for training basic and advanced clinical skills. Medical Education, 37: 14-21<br />
Hamilton, R. (2005). Nurses' knowledge and skill retention following cardiopulmonary resuscitation training: a review<br />
<strong>of</strong> <strong>the</strong> literature. Journal <strong>of</strong> Advanced Nursing, 51(3), 288-297.
Bibliography<br />
Institute <strong>of</strong> Medicine, (2000). To Err is Human: Building a Safer Health System. Washington, DC: National Academy<br />
Press.<br />
Keys, V., Malone, P., Brim, C., Schoonover, H., Nordstrom, C., & Selzler, M. (2009). <strong>Code</strong> carnivals: resuscitating<br />
<strong>Code</strong> <strong>Blue</strong> training with accelerated learning.Journal <strong>of</strong> Continuing Education in Nursing, 40(12), 560-564.<br />
Kiat, T., Mei, T., Nagammal, S., & Jonnie, A. (2007). A review <strong>of</strong> learners' experience with simulation based training in<br />
nursing. Singapore Nursing Journal, 34(4), 37-43.<br />
Krumholtz, H. (2008). Delayed time to defibrillation. New England Journal <strong>of</strong> Medicine, 358: 9-17.<br />
Lockey, A., & Nolan, J. (2001). Cardiopulmonary resuscitation in adults: revised guidelines are more evidence based.<br />
BMJ: British Medical Journal, 323(7317), 819-820.<br />
Lurie, K., & Lindner, K. (1997). Recent advances in cardiopulmonary resuscitation. Journal <strong>of</strong> Cardiovascular<br />
Electrophysiology, 8(5), 584-600.<br />
McGaghie, W. (2006). Effect <strong>of</strong> practice on standardized learning outcomes in simulation-based medical education.<br />
Medical Education 2006, 40: 792-797.<br />
Meaney, P. (2009). Rhythms and outcomes <strong>of</strong> adult in-hospital cardiac arrest. Critical Care Medicine, 38(1), 3054-61.<br />
Meerabeau, L., & Page, S. (1999). I'm sorry if I panicked you: nurses' accounts <strong>of</strong> teamwork in cardiopulmonary<br />
resuscitation. Journal <strong>of</strong> Interpr<strong>of</strong>essional Care, 13(1), 29-40.<br />
Morgan, P., Cleave-Hogg, D., DeSousa, S., & Lam-McCulloch, J. (2006). Applying <strong>the</strong>ory to practice in undergraduate<br />
education using high fidelity simulation. Medical Teacher, 28(1), e10-5.<br />
Morrison, R. (2006). The new adult resuscitation guidelines. Practice Nurse, 31(7), 30.<br />
Nehring, W., & Lashley, F. (2004). Current use and opinions regarding human patient simulators in nursing education:<br />
an international survey. Nursing Education Perspectives, 25(5), 244-248.<br />
Neumar, R. (2009). Variation in time to defibrillation after arrest. Critical Care Medicine, 38(1), 3042-46.<br />
ODonnell, C. (1990). A survey <strong>of</strong> opinion amongst trained nurses and junior medical staff on current practices in<br />
resuscitation. Journal <strong>of</strong> Advanced Nursing, 15, 1175 1180.<br />
Page, S., & Meerabeau, L. (1996). Nurses' accounts <strong>of</strong> cardiopulmonary resuscitation. Journal <strong>of</strong> Advanced Nursing,<br />
24(2), 317-325.
Bibliography<br />
Radhakrishnan, K., Roche, J., & Cunningham, H. (2007). Measuring clinical practice parameters with human<br />
patient simulation: a pilot study. International Journal <strong>of</strong> Nursing Education Scholarship, 4(1), 1-11.<br />
Ramsay, P., & Maxwell, R. (2009). Advancements in cardiopulmonary resuscitation: increasing circulation and<br />
improving survival. American Surgeon, 75(5), 359-362.<br />
Seropian, M., Brown, K., Gavilanes, J. & Driggers, B. (2004). <strong>Simulation</strong>: not just a manikin. Journal <strong>of</strong> Nursing<br />
Education, 43(4), 164-169.<br />
Sullivan, B. (2008). Cardiac arrest management: part 2. EMS Magazine, 37(4), 56.<br />
Swartz, M. (2008). Standardized patients: <strong>the</strong> "o<strong>the</strong>r" simulation. Journal <strong>of</strong> Critical Care, 23(2), 179-184.<br />
Taber's cyclopedic medical dictionary, 21st edition. (2009). Philadelphia, PA: F A Davis Co.<br />
Wallin, C., Meurling, L., Hedman, L., Hedegård, J., & Felländer-Tsai, L. (2007). Target-focused medical<br />
emergency team training using a human patient simulator: effects on behavior and attitude. Medical<br />
Education, 41(2), 173-180.<br />
Webb, D. (2002). Performance Improvement. Conversations in nursing pr<strong>of</strong>essional development. Pensacola,<br />
FL: Pohl Publishing.<br />
Whitcomb, J., & Blackman, V. (2007). Cardiopulmonary resuscitation: how far have we come. Dimensions <strong>of</strong><br />
Critical Care Nursing, 26(1), 1-8.<br />
White, R. (2006). 2005 American Heart Association Guidelines for CardiopulmonaryResuscitation: physiologic<br />
and educational rationale for changes. Mayo Clinic Proceedings, 81(6), 736-740.<br />
Zed, P., Abu-Laban, R., Shuster, M., Green, R., Slavik, R., & Travers, A. (2008). Update on cardiopulmonary<br />
resuscitation and emergency cardiovascular care guidelines. American Journal <strong>of</strong> Health-System<br />
Pharmacy, 65(24), 2337-2346.