Manual for Male Circumcision under Local Anaesthesia
Manual for Male Circumcision under Local Anaesthesia Manual for Male Circumcision under Local Anaesthesia
Male circumcision under local anaesthesia Version 3.1 (Dec09) coitus uncomfortable. Instead, close the V-shaped defect by placing the frenular suture 1–2 cm (depending on age and penis size) back from the apex of the V, taking both sides of the defect (Fig. 5.43C). The V incision is thus converted into an inverted T. Suture the rest of the skin as in a normal circumcision (Fig. 5.43D). Fig. 5.43 Variation in technique if the frenulum is tight or scarred Surgical procedures for adults and adolescents Chapter 5-34
Male circumcision under local anaesthesia Version 3.1 (Dec09) Chapter 6 Circumcision of infants and children SUMMARY This chapter gives step-by-step instructions for performing a circumcision on an infant or young child. Four surgical techniques are described: • the dorsal slit method; • the Plastibell method; • the Mogen clamp method; • the Gomco clamp method. Four widely-used surgical techniques for paediatric circumcision are described in this chapter. The recommended techniques are shown in detail so that they can be referred to in the context of a training course. After the initial training, they can be used to reinforce what has been learnt. Surgeons should become expert in the technique most suited to the circumstances of their practice. It is not recommended that a nursing, clinical or medical officer learn all the techniques. It is best to become a master of one. This will produce the best results with the least complications. Circumcision of infants and pre-pubertal boys is simpler than circumcision of older boys and adults, because the penis is relatively underdeveloped and the foreskin less vascular. Healing is quick and complication rates are low. A major disadvantage is that the child cannot give consent for the procedure. In addition, the primary health benefit – reduced risk of HIV infection – is not realized until many years later when he becomes sexually active. Circumcision can be delayed to an older age, when the boy can understand the risks and benefits of circumcision and consent to the procedure himself. Programmes that promote circumcision of young children are likely to have lower morbidity rates and lower cost than programmes targeting adolescents and adults. However, this must be balanced by concerns about consent. SCREENING MALE BABIES AND YOUNG BOYS FOR CIRCUMCISION The screening procedures for infants and young children are similar to those for adolescents and adults, and are aimed at ensuring that the client is suitable for surgery at the clinic. If there is any doubt, surgery should be deferred or the client Infant and paediatric circumcision Chapter 6 - 1
- Page 63 and 64: Male circumcision under local anaes
- Page 65 and 66: Male circumcision under local anaes
- Page 67 and 68: Male circumcision under local anaes
- Page 69 and 70: Male circumcision under local anaes
- Page 71 and 72: Male circumcision under local anaes
- Page 73 and 74: Male circumcision under local anaes
- Page 75 and 76: Male circumcision under local anaes
- Page 77 and 78: Male circumcision under local anaes
- Page 79 and 80: Male circumcision under local anaes
- Page 81 and 82: Male circumcision under local anaes
- Page 83 and 84: Male circumcision under local anaes
- Page 85 and 86: Male circumcision under local anaes
- Page 87 and 88: Male circumcision under local anaes
- Page 89 and 90: Male circumcision under local anaes
- Page 91 and 92: Male circumcision under local anaes
- Page 93 and 94: Male circumcision under local anaes
- Page 95 and 96: Male circumcision under local anaes
- Page 97 and 98: Male circumcision under local anaes
- Page 99 and 100: Male circumcision under local anaes
- Page 101 and 102: Male circumcision under local anaes
- Page 103 and 104: Male circumcision under local anaes
- Page 105 and 106: Male circumcision under local anaes
- Page 107 and 108: Male circumcision under local anaes
- Page 109 and 110: Male circumcision under local anaes
- Page 111 and 112: Male circumcision under local anaes
- Page 113: Male circumcision under local anaes
- Page 117 and 118: Male circumcision under local anaes
- Page 119 and 120: Male circumcision under local anaes
- Page 121 and 122: Male circumcision under local anaes
- Page 123 and 124: Male circumcision under local anaes
- Page 125 and 126: Male circumcision under local anaes
- Page 127 and 128: Male circumcision under local anaes
- Page 129 and 130: Male circumcision under local anaes
- Page 131 and 132: Male circumcision under local anaes
- Page 133 and 134: Male circumcision under local anaes
- Page 135 and 136: Male circumcision under local anaes
- Page 137 and 138: Male circumcision under local anaes
- Page 139 and 140: Male circumcision under local anaes
- Page 141 and 142: Male circumcision under local anaes
- Page 143 and 144: Male circumcision under local anaes
- Page 145 and 146: Male circumcision under local anaes
- Page 147 and 148: Male circumcision under local anaes
- Page 149 and 150: Male circumcision under local anaes
- Page 151 and 152: Male circumcision under local anaes
- Page 153 and 154: Male circumcision under local anaes
- Page 155 and 156: Male circumcision under local anaes
- Page 157 and 158: Male circumcision under local anaes
- Page 159 and 160: Male circumcision under local anaes
- Page 161 and 162: Male circumcision under local anaes
- Page 163 and 164: Male circumcision under local anaes
<strong>Male</strong> circumcision <strong>under</strong> local anaesthesia<br />
Version 3.1 (Dec09)<br />
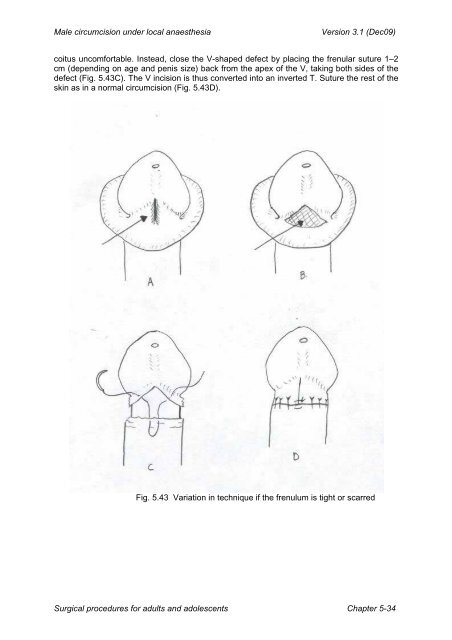
coitus uncom<strong>for</strong>table. Instead, close the V-shaped defect by placing the frenular suture 1–2<br />
cm (depending on age and penis size) back from the apex of the V, taking both sides of the<br />
defect (Fig. 5.43C). The V incision is thus converted into an inverted T. Suture the rest of the<br />
skin as in a normal circumcision (Fig. 5.43D).<br />
Fig. 5.43 Variation in technique if the frenulum is tight or scarred<br />
Surgical procedures <strong>for</strong> adults and adolescents Chapter 5-34


