indications and complications of capener technique (costo
indications and complications of capener technique (costo
indications and complications of capener technique (costo

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
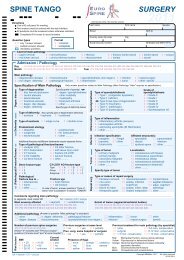
SURGICAL INDICATIONS AND<br />
COMPLICATIONS OF<br />
CAPENER TECHNIQUE<br />
(COSTO-TRANSVERSECTOMY).<br />
TRANSVERSECTOMY).<br />
Patricia Álvarez González,<br />
Javier Pizones Arce, Felisa SánchezS<br />
nchez-Mariscal,<br />
Lorenzo ZúñZ<br />
úñiga Gómez, G<br />
Enrique Izquierdo NúñN<br />
úñez.<br />
HOSPITAL UNIVERSITARIO DE GETAFE,<br />
MADRID. SPAIN.<br />
docalvarez@gmail.com
Objective <strong>and</strong> Background data<br />
• The objective <strong>of</strong> this study is to describe surgical <strong>indications</strong> <strong>and</strong><br />
<strong>complications</strong> <strong>of</strong> <strong>costo</strong>-transversectomy<br />
transversectomy.<br />
•This <strong>technique</strong> was described<br />
by Capener in 1954, it was<br />
called “lateral<br />
rhachotomy” . It<br />
was performed to drain<br />
tuberculous abscess.<br />
Methods<br />
N.Capener.<br />
JBJS 1954; 36 B: 173-9.<br />
• Retrospective case series <strong>of</strong> 24 patients operated from 2005 to<br />
2009. Mean age 60 years (17-84). There were 13 women <strong>and</strong> 11<br />
men. Most <strong>of</strong> the patients had severe co-morbidities (table 1).
SURGICAL TECHNIQUE: Posterior midline exposure two to three<br />
levels above <strong>and</strong> below lesion, dissection at level <strong>of</strong> lesion exposing<br />
transverse process, <strong>costo</strong>transverse articulation <strong>and</strong> medial 5 cm <strong>of</strong> ribs.<br />
Placement <strong>of</strong> pedicle screws at proximal <strong>and</strong> distal levels. Bilateral or<br />
unilateral <strong>costo</strong>transversectomy <strong>and</strong> rhacothomy at one or more levels.<br />
After temporary rod stabilization, laminectomy <strong>and</strong> discectomy/<br />
corpectomy are performed to permit circumferential decompression.
Reconstruction <strong>of</strong><br />
the anterior thoracic<br />
spine with cage <strong>and</strong><br />
graft. After that,<br />
posterior<br />
reconstruction with<br />
two rods.
Results<br />
• There were 11 cases <strong>of</strong> spondylodiscitis, , 7 spinal<br />
tumours, 4 kyphosis/kyphoscoliosis, , 1 acute fracture<br />
with spinal cord compression, 1 thoracic disk<br />
herniation (table 1).<br />
• There were 17 patients with spinal cord compression<br />
<strong>and</strong> neurological impairment before surgery.<br />
Neurological improvement <strong>of</strong> at least 1 Frankel grade<br />
was achieved in 9 cases. There were no cases <strong>of</strong><br />
neurological deterioration after surgery (table 1).<br />
• All <strong>of</strong> the patients received posterior instrumentation<br />
with two titanium rods. The average <strong>of</strong> fused levels was<br />
8 (4-15).<br />
Titanium mesh or PEEK cages were used as<br />
an anterior support in 19 cases, <strong>and</strong> tricortical iliac<br />
autograft in 2 (table 2).
Results<br />
• Bilateral <strong>costo</strong>-transversectomy<br />
transversectomy was done in 7 cases,<br />
right approach in 10 <strong>and</strong> left in 7. Costo-<br />
transversectomy was performed at one level in 4 cases,<br />
two levels in 10, <strong>and</strong> three levels in 10 (table 2).<br />
• 10 cases were located in the upper-thoracic spine (T1-<br />
T4), 5 in mid-thoracic (T5-T8) T8) <strong>and</strong> 9 in low-thoracic<br />
(T9-T12) T12) (table 2).<br />
• Pedicle subtraction osteotomy (PSO) was done in 2<br />
cases, corpectomy in 17 cases, thoracic discectomies in<br />
4, <strong>and</strong> 1 spinal cord decompression in vertebral rotatory<br />
subluxation (case 23).<br />
• None <strong>of</strong> the patients requiered a chest tube in<br />
inmediate postoperative (except<br />
case 19).<br />
• Blood loss averaged 2430 ml (900-4500). Mean surgical<br />
time 6.3 hours (4-10).<br />
Hospital length <strong>of</strong> stay 36,8 days<br />
(10-100).<br />
100).
Results. Complications.<br />
• There were postoperative <strong>complications</strong> in 15 patients (62.5%)<br />
(see table 3):<br />
• Pleural effusion in 6 cases (all(<br />
<strong>of</strong> them requiered chest tube<br />
insertion).<br />
• 5 patients required Intensive Care Unit (ICU) admission due to<br />
postoperative <strong>complications</strong>.<br />
• 7 patients required surgical intervention: 5 debridement <strong>and</strong><br />
closure due to wound dehiscence or infection <strong>and</strong> 2 proximal<br />
extension <strong>of</strong> fusion due to pull-out <strong>of</strong> instrumentation. Patients<br />
#20 <strong>and</strong> #23, needed a third operation: debridement <strong>and</strong><br />
removal <strong>of</strong> material due to infection. Patient #23 suffered from<br />
sepsis.<br />
• There were 2 acute atrial fibrillation, patient #14 had a<br />
cardiopulmonary arrest but she recovered after cardiopulmonary<br />
resuscitation.<br />
• Patient #3 <strong>and</strong> #13 had pneumonic sepsis; patient #13 (with<br />
severe chronic obstructive pulmonary disease), died.
n. Age Comorbidity Diagnosis Frankel pre Frankel pos<br />
1 75, F Hypothyroidism, metastases in long bones Metastatic renal cell carcinoma D D<br />
2 77, M Vertebral metastases, aortic insufficiency, hypertension Metastatic prostate cancer D D<br />
3 52, M Chronic liver disease, syphilis Thoracic disk herniation A D<br />
4 22, F - Giant cell tumour D D<br />
5 59, M Arterial hypertension Metastatic lung carcinoma E E<br />
6 33, M Ankle <strong>and</strong> scrotal tuberculous abcess Pott disease <strong>and</strong> epidural abcess C C<br />
7 44, F - Metastatic breast cancer E E<br />
8 47, M Obesity Unknown tumour metastases B B<br />
9 64, F Hypertension, severe osteoporosis Postraumatic kyphosis E E<br />
10 33, M Kniest syndrome, complete postraumatic paraplegia Congenital kyphosis A A<br />
11 71, F Cerebrovascular disease, hypertension, osteoporosis Pyogenic spondylodiscitis E E<br />
12 78, F Parkinson disease, severe osteoporosis Pyogenic spondylodiscitis E E<br />
13 61, M Obstructive pulmonar disease, diabetes, hypertension Thoracic fracture, cord compression C C<br />
14 78, F Cerebrovascular disease, dementia Pyogenic spondylodiscitis B C<br />
15 17, M asthma Congenital kyphoscoliosis E E<br />
16 84, F Myocardiopathy, arterial hypertension Pyogenic spondylodiscitis E E<br />
17 59, M Acute myeloid leukemia Fungal spondylodiscitis D E<br />
18 61, F Arterial hypertension Pott disease D E<br />
19 67, F Arterial hypertension Pott disease D E<br />
20 74, F Coronary heart disease, hypertension Pyogenic spondylodiscitis D E<br />
21 68, F Parkinson disease, hypertension Pott disease C E<br />
22 71, M Aortic aneurysm, arrythmia, pulmonar disease, renal failure Pyogenic spondylodiscitis A A<br />
23 45, M Restrictive pulmonary disease, neur<strong>of</strong>ibromatosis Kyphoscoliosis, rotatory subluxation B D<br />
24 69, F Multiple myeloma Myeloma A B
n. Approach Costotransversectomy level Corpectomy level Discectomy level Fusion levels Anterior support<br />
1 bilateral T11-T12 T12 T11-L1 T9-L3 Titanium mesh<br />
2 left T3-T4-T5 T4 T5 T3-T6 C7-L4 Titanium mesh<br />
3 left T9-T10-T11 - T9-T11 T8-L1 -<br />
4 bilateral T1 T1 Anterior approach C4-T4 Titanium mesh<br />
5 bilateral T1-T2-T3 T2 T1-T3 C7-T4 Titanium mesh<br />
6 right T8-T9 T8 T9 T7-T10 T6-L1 Tricortical iliac<br />
7 bilateral T2-T3 T2 T1-T3 C7-T5 Titanium mesh<br />
8 left T2-T3-T4 T3 T2-T4 C7-L1 Titanium mesh<br />
9 bilateral T12 PSO T12 - T10-L2 -<br />
10 right T12 PSO T12 T11-T12 T8-L2 PEEK cage<br />
11 left T11-T12 - T11-T12 T7-S1 (prev.T12-S1) Titanium mesh<br />
12 left T11-T12 T11 T10-T12 T8-L3 Titanium mesh<br />
13 left T4-T5 T4 T5 T3-T6 T1-T9 Titanium mesh<br />
14 left T5-T6-T7 T6 T7 T5-T8 T3-T10 Titanium mesh<br />
15 bilateral T9-T10-T11 T11 T10-T12 T7-L3 PEEK cage<br />
16 left T12 - T12-L1 T10-L3 PEEK cage<br />
17 right T6-T7-T8 T7 T6-T8 T3-T12 Titanium mesh<br />
18 right T2-T3 T2 T3 T1-T4 C6-T8 Titanium mesh<br />
19 right T1-T2 T1 T2 C7-T3 C6-T7 Tricortical iliac<br />
20 left T9-T10 - T9-T10 T1-L1 Titanium mesh<br />
21 right T2-T3-T4 T2 T1T3 C6-T12 Titanium mesh<br />
22 left T7-T8-T9 T8 T7-T9 T4-L2 Titanium mesh<br />
23 right T5-T6-T7 parcial T5 T6 T7 parcial T4-T8 T2-T11 -<br />
24 bilateral T2-T3 T2 T1-T3 C6-T6 Titanium mesh
n. Intraop complic. Postop <strong>complications</strong> Medical interv. Surgical intervention<br />
1 Dural tear Pleural Effusion (PE), wound infection Chest tube Debridement<br />
2 - Pleural effusion (PE), respiratory failure Chest tube, ICU -<br />
3 - PE, hepatic encephalopathy, neumonia, sepsis Chest tube, ICU -<br />
4 - PE, septic thromb<strong>of</strong>lebitis <strong>of</strong> central venous catheter Chest tube -<br />
5 - PE Chest tube -<br />
6 Neuromonitoring - - -<br />
7 - Wound seroma - -<br />
8 - Wound infection - Debridement<br />
9 Pleural tear Acute atrial fibrillation Cardioversion -<br />
10 - - - -<br />
11 - Pull-out <strong>of</strong> instrumentation, urinary tract infection - Proximal Extension <strong>of</strong> Fusion (PEF)<br />
12 - Wound dehiscence - Debridement <strong>and</strong> closure<br />
13 - Neumonia, sepsis, respiratory failure, death ICU -<br />
14 - PE, acute atrial fibrillation, cardiopulmonary arrest Chest tube, ICU -<br />
15 - - - -<br />
16 - - - -<br />
17 - - - -<br />
18 - - - -<br />
19 Pleural tear (tube) Wound dehiscence - Debridement <strong>and</strong> closure<br />
20 - Pull-out <strong>of</strong> instrumentation, wound infection - PEF, debridement.<strong>and</strong> parcial removal <strong>of</strong> material<br />
21 - - - -<br />
22 - - - -<br />
23 - Pull-out, wound infection, heart failure, sepsis ICU Debridement <strong>and</strong> closure, removal <strong>of</strong> material<br />
24 - - - -
E<br />
45-year old patient (#23) developed neurological impairment Frankel B, after performing a hyperextension movement <strong>of</strong> his<br />
arms. Past medical history: Neur<strong>of</strong>ibromatosis type 1, scoliosis operated at the age <strong>of</strong> 12, restrictive pulmonary disfunction.<br />
Paraplegia was due to vertebral rotatory subluxation in severe dystrophic kyphoscoliosis (Images A, B, C). Right <strong>costo</strong>transversectomies<br />
<strong>and</strong> instrumentation were performed, <strong>and</strong> spinal cord decompression was achieved (Image D). Protrusion <strong>of</strong><br />
instrumentation caused wound dehiscence <strong>and</strong> the patient needed plastic surgery closure 15 days after first surgery. 15 days later,<br />
the patient suffered from sepsis <strong>and</strong> required ICU admission <strong>and</strong> a third operation (debridement <strong>and</strong> removal <strong>of</strong> material) due to<br />
deep wound infection (Images E, F). The patient improved his neurological impairment after surgery, Frankel D, <strong>and</strong> he is able<br />
to walk with orthotic devices <strong>and</strong> crutches.<br />
A B C D
Conclusions<br />
• Thoracic corpectomies or discectomies have tradicionally been<br />
performed through an anterior approach or a combined anterior-<br />
posterior approach.<br />
• Patients who cannot tolerate anterior thoracic procedures with<br />
significant pulmonary comorbidity or those in whom a salvage<br />
procedure is the only palliative alternative, this <strong>technique</strong> may<br />
serve as a preferred option.<br />
• Costo-transversectomy<br />
transversectomy is a dem<strong>and</strong>ing <strong>technique</strong>, it leads to<br />
sufficient exposition <strong>of</strong> the anterior aspect <strong>of</strong> the spinal canal<br />
avoiding an anterior approach. Indications: Kyphotic<br />
deformities, thoracic disc herniation, , infective, traumatic or<br />
neoplastic lesions <strong>of</strong> the vertebral body that lead to vertebral<br />
body destruction, instability <strong>and</strong> neurologic deficit. But it is not<br />
free <strong>of</strong> <strong>complications</strong>, particularly in patients who have severe<br />
co-morbidity.