the tweed profile - The Charles H. Tweed International Foundation
the tweed profile - The Charles H. Tweed International Foundation
the tweed profile - The Charles H. Tweed International Foundation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
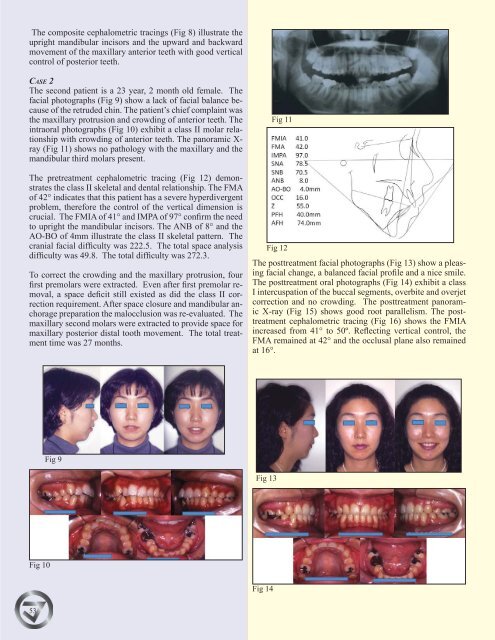
<strong>The</strong> composite cephalometric tracings (Fig 8) illustrate <strong>the</strong><br />
upright mandibular incisors and <strong>the</strong> upward and backward<br />
movement of <strong>the</strong> maxillary anterior teeth with good vertical<br />
control of posterior teeth.<br />
CASE 2<br />
<strong>The</strong> second patient is a 23 year, 2 month old female. <strong>The</strong><br />
facial photographs (Fig 9) show a lack of facial balance because<br />
of <strong>the</strong> retruded chin. <strong>The</strong> patient’s chief complaint was<br />
<strong>the</strong> maxillary protrusion and crowding of anterior teeth. <strong>The</strong><br />
intraoral photographs (Fig 10) exhibit a class II molar relationship<br />
with crowding of anterior teeth. <strong>The</strong> panoramic X-<br />
ray (Fig 11) shows no pathology with <strong>the</strong> maxillary and <strong>the</strong><br />
mandibular third molars present.<br />
<strong>The</strong> pretreatment cephalometric tracing (Fig 12) demonstrates<br />
<strong>the</strong> class II skeletal and dental relationship. <strong>The</strong> FMA<br />
of 42° indicates that this patient has a severe hyperdivergent<br />
problem, <strong>the</strong>refore <strong>the</strong> control of <strong>the</strong> vertical dimension is<br />
crucial. <strong>The</strong> FMIA of 41° and IMPA of 97° confirm <strong>the</strong> need<br />
to upright <strong>the</strong> mandibular incisors. <strong>The</strong> ANB of 8° and <strong>the</strong><br />
AO-BO of 4mm illustrate <strong>the</strong> class II skeletal pattern. <strong>The</strong><br />
cranial facial difficulty was 222.5. <strong>The</strong> total space analysis<br />
difficulty was 49.8. <strong>The</strong> total difficulty was 272.3.<br />
To correct <strong>the</strong> crowding and <strong>the</strong> maxillary protrusion, four<br />
first premolars were extracted. Even after first premolar removal,<br />
a space deficit still existed as did <strong>the</strong> class II correction<br />
requirement. After space closure and mandibular anchorage<br />
preparation <strong>the</strong> malocclusion was re-evaluated. <strong>The</strong><br />
maxillary second molars were extracted to provide space for<br />
maxillary posterior distal tooth movement. <strong>The</strong> total treatment<br />
time was 27 months.<br />
Fig 11<br />
Fig 12<br />
<strong>The</strong> posttreatment facial photographs (Fig 13) show a pleasing<br />
facial change, a balanced facial <strong>profile</strong> and a nice smile.<br />
<strong>The</strong> posttreatment oral photographs (Fig 14) exhibit a class<br />
I intercuspation of <strong>the</strong> buccal segments, overbite and overjet<br />
correction and no crowding. <strong>The</strong> posttreatment panoramic<br />
X-ray (Fig 15) shows good root parallelism. <strong>The</strong> posttreatment<br />
cephalometric tracing (Fig 16) shows <strong>the</strong> FMIA<br />
increased from 41° to 50º. Reflecting vertical control, <strong>the</strong><br />
FMA remained at 42° and <strong>the</strong> occlusal plane also remained<br />
at 16°.<br />
Fig 9<br />
Fig 13<br />
Fig 10<br />
Fig 14<br />
53