Health History Form
Health History Form
Health History Form

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
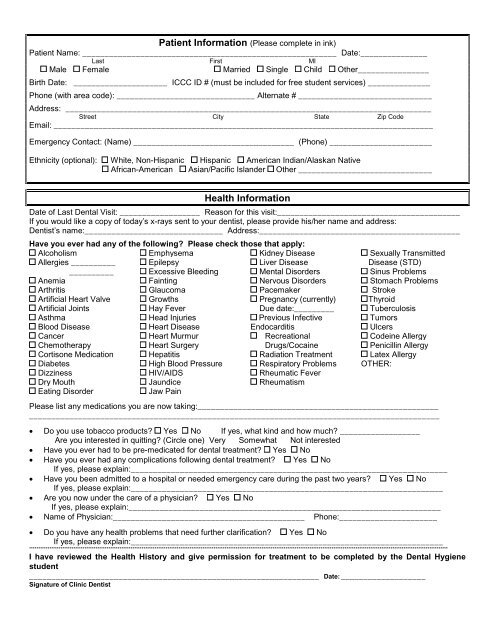
Patient Information (Please complete in ink)<br />
Patient Name: _________________________________________________________ Date:_______________<br />
Last First MI<br />
Male Female Married Single Child Other________________<br />
Birth Date: _____________________ ICCC ID # (must be included for free student services) ______________<br />
Phone (with area code): _______________________________ Alternate # ______________________________<br />
Address: __________________________________________________________________________________<br />
Street City State Zip Code<br />
Email: _____________________________________________________________________________________<br />
Emergency Contact: (Name) ____________________________________ (Phone) _______________________<br />
Ethnicity (optional): White, Non-Hispanic Hispanic American Indian/Alaskan Native<br />
African-American Asian/Pacific Islander Other ______________________________<br />
<strong>Health</strong> Information<br />
Date of Last Dental Visit: __________________ Reason for this visit:_________________________________________<br />
If you would like a copy of today’s x-rays sent to your dentist, please provide his/her name and address:<br />
Dentist’s name:_______________________________ Address:_____________________________________________<br />
Have you ever had any of the following? Please check those that apply:<br />
Alcoholism<br />
Allergies __________<br />
__________<br />
Anemia<br />
Arthritis<br />
Artificial Heart Valve<br />
Artificial Joints<br />
Asthma<br />
Blood Disease<br />
Cancer<br />
Chemotherapy<br />
Cortisone Medication<br />
Diabetes<br />
Dizziness<br />
Dry Mouth<br />
Eating Disorder<br />
Emphysema<br />
Epilepsy<br />
Excessive Bleeding<br />
Fainting<br />
Glaucoma<br />
Growths<br />
Hay Fever<br />
Head Injuries<br />
Heart Disease<br />
Heart Murmur<br />
Heart Surgery<br />
Hepatitis<br />
High Blood Pressure<br />
HIV/AIDS<br />
Jaundice<br />
Jaw Pain<br />
Kidney Disease<br />
Liver Disease<br />
Mental Disorders<br />
Nervous Disorders<br />
Pacemaker<br />
Pregnancy (currently)<br />
Due date:_________<br />
Previous Infective<br />
Endocarditis<br />
Recreational<br />
Drugs/Cocaine<br />
Radiation Treatment<br />
Respiratory Problems<br />
Rheumatic Fever<br />
Rheumatism<br />
Sexually Transmitted<br />
Disease (STD)<br />
Sinus Problems<br />
Stomach Problems<br />
Stroke<br />
Thyroid<br />
Tuberculosis<br />
Tumors<br />
Ulcers<br />
Codeine Allergy<br />
Penicillin Allergy<br />
Latex Allergy<br />
OTHER:<br />
Please list any medications you are now taking:______________________________________________________<br />
____________________________________________________________________________________________<br />
• Do you use tobacco products? Yes No If yes, what kind and how much? __________________<br />
Are you interested in quitting? (Circle one) Very Somewhat Not interested<br />
• Have you ever had to be pre-medicated for dental treatment? Yes No<br />
• Have you ever had any complications following dental treatment? Yes No<br />
If yes, please explain:_______________________________________________________________________<br />
• Have you been admitted to a hospital or needed emergency care during the past two years? Yes No<br />
If yes, please explain:______________________________________________________________________<br />
• Are you now under the care of a physician? Yes No<br />
If yes, please explain:______________________________________________________________________<br />
• Name of Physician:___________________________________________ Phone:______________________<br />
• Do you have any health problems that need further clarification? Yes No<br />
If yes, please explain:______________________________________________________________________<br />
***********************************************************************************************************************************************************************************************************************************<br />
I have reviewed the <strong>Health</strong> <strong>History</strong> and give permission for treatment to be completed by the Dental Hygiene<br />
student<br />
_________________________________________________________________ Date: ___________________<br />
Signature of Clinic Dentist
Responsible Party Information<br />
(Complete this section if patient is under 18 or someone other than the patient is responsible for payment)<br />
The following is for: the patient's spouse the person responsible for payment the patient’s parent/guardian<br />
Name:<br />
Male Female Married Single Child Other<br />
Birth Date: ______________________________<br />
Phone (with area code): _____________________________Alternate#:<br />
Mailing Address:<br />
Street City State Zip Code<br />
Insurance Information<br />
Name of Insured: _______________________________________________ Is insured a patient? Yes No<br />
Last First MI<br />
Insured's Birth Date: _________________ ID #: _____________________ Group #:<br />
Insured's Address:<br />
Street City State Zip Code<br />
Insured's Employer Name and Address<br />
Patient's relationship to insured: Self Spouse Child Other___________________<br />
Insurance Plan Name:_______________________________________________________________________<br />
Address:<br />
Street City State Zip Code<br />
Dental Insurance: It is your responsibility to consult with your insurance company for details on your covered or non-covered services, service<br />
limitations or restrictions, and yearly maximums. Medical coverage does not pay for dental hygiene services. You will receive a “super bill” that you can<br />
send in for reimbursement from your insurance company.<br />
Consent for Services<br />
As a condition of your treatment by the Iowa Central Community College Dental Hygiene Student Clinic, financial arrangements must be made in<br />
advance. The clinic depends upon reimbursement from the patients for the costs incurred in their care and financial responsibility on the part of each<br />
patient must be determined before treatment. Payment for dental hygiene treatment is required at each visit. We accept cash, check, and credit cards<br />
for payment of services.<br />
Patients who carry dental insurance understand that all dental services furnished are charged directly to the patient and that he or she is personally<br />
responsible for payment of all dental services. The Iowa Central Community College Dental Hygiene Student Clinic will help prepare the patients<br />
insurance forms or assist in making collections from insurance companies and will credit any such collections to the patient's account. However, this<br />
Dental Hygiene clinic cannot render services on the assumption that our charges will be paid by an insurance company.<br />
I understand that the fee estimate listed for this dental care can only be extended for a period of six months from the date of the patient examination.<br />
In consideration for the professional services rendered to me, or at my request, by the Doctor, I agree to pay therefore the reasonable value of said<br />
services to said Doctor, or his assignee, at the time said services are rendered. I further agree that a waiver of any breach of any time or condition<br />
hereunder shall not constitute a waiver of any further term or condition and I further agree to pay all costs and reasonable attorney fees if suit be<br />
instituted hereunder.<br />
I grant my permission to you or your assignee, to telephone me at home or at my work to discuss matters related to this form.<br />
I have read the above conditions of treatment and payment and agree to their content.<br />
To the best of my knowledge, all of the preceding answers and information provided are true and correct. If I ever<br />
have any change in my health, I will inform the clinic at the next appointment without fail.<br />
I am able to read and speak English.<br />
I have received a copy of the privacy practices of the Iowa Central Dental Hygiene Clinic.<br />
____________________________________________________<br />
Signature of patient, parent or guardian, or guarantor of payment<br />
Date: __________<br />
Relationship to Patient:
Iowa Central Community College<br />
Dental Hygiene Student Clinic<br />
This is a teaching clinic. All treatment is provided by dental hygiene students. Dental hygiene students<br />
are supervised by licensed dental hygiene faculty and a licensed dentist. Services performed are limited<br />
to preventive treatment and not intended to take the place of restorative dental treatment. Our teaching<br />
clinics strive to provide the best care for you; however there are some treatments that our students<br />
cannot provide. You may need to see a private dental office for further treatment.<br />
Fees will be charged for all dental hygiene services performed, however, they are greatly reduced from<br />
those in private practices, and payment is due at time of service. You will be responsible for paying the<br />
costs of the dental hygiene services provided.<br />
Payment must be submitted at each appointment for the treatment received. The clinic will accept cash,<br />
check, debit or credit card.<br />
If you have dental insurance coverage, you will be given a form to submit to your insurance company<br />
for reimbursement.<br />
Please be aware that your dental insurance may not reimburse you for all your treatment costs.<br />
Unattended children are not allowed in the reception area. Persons who are not patients are not allowed<br />
on the clinic floor. This may be waived if there are extenuating circumstances.<br />
Patient Eligibility<br />
Iowa Central Community College Dental Hygiene Clinic is an educational institution and provides<br />
preventative and oral hygiene patient treatment. In general, all persons who are able to afford the time<br />
and the cost will be treated at the school. Furthermore, patients whose medical or emotional<br />
management would be beyond the ability of the student in a school setting may not be accepted for<br />
treatment.<br />
New Patients<br />
Appointments for new patients for consultations, radiographs, or hygiene services are usually<br />
scheduled by the Dental Hygiene student. Appointments may be scheduled by contacting the clinic<br />
receptionist.<br />
Patient Assignment Procedures<br />
All patients are screened by the student and faculty and categorized according to the complexity of<br />
their dental hygiene needs. Student assignment may be made by the clinic instructors and is closely<br />
linked to the need of providing appropriate clinical experience to students based on their need to<br />
achieve and maintain clinical competency.<br />
Last modified 08-28-09
Procedures<br />
The following is a list of dental hygiene services and functions taught to clinical competency and<br />
performed by dental hygiene students in the Dental Hygiene Clinic. Treatment is prescribed by<br />
licensed dentists employed by the college to supervise clinic sessions. Licensed dental hygienists are<br />
employed in the clinic to instruct, evaluate, and enhance the students’ clinical learning experiences.<br />
1. Clinical infection control procedures<br />
2. Social, medical and dental history data collection<br />
3. Blood pressure and pulse measurements, temperature and respiration rates<br />
4. Extra-oral and intraoral examinations (Cancer Screening)<br />
5. Dental charting<br />
6. Periodontal charting and assessment<br />
7. Patient oral health education<br />
8. Dental hygiene assessment, treatment planning, and evaluation<br />
9. Oral radiographs – exposing, processing and interpreting<br />
• Bitewing x-ray<br />
• Full mouth x-rays<br />
• Panographic x-rays<br />
10. Calculus detection<br />
11. Ultrasonic scaling<br />
12. Periodontal scaling<br />
13. Root (planing) debridement<br />
14. Polishing<br />
15. Application of topical fluoride<br />
16. Application of dental sealants<br />
17. Application of tooth desensitization<br />
18. Application of topical anesthetic agents, including transoral delivery system<br />
19. Local anesthesia as needed<br />
20. Removal of interproximal overhangs<br />
21. Application of chemotherapeutic agents including subgingival irrigation<br />
22. Nutritional counseling<br />
23. Alginate impressions and study models<br />
24. Cleaning of removable prosthetic appliances<br />
The following procedures are taught to laboratory competency*<br />
1. Placement and removal of rubber dams<br />
2. Maintenance of dental implants<br />
3. Finishing and polishing amalgam restorations<br />
4. Suture removal<br />
5. Pulp vitality<br />
6. Placement and removal of periodontal dressings<br />
7. Soft tissue curettage<br />
*Procedures taught to laboratory competence are delegable to a licensed dental hygienist in the state of Iowa by a licensed dentist. The theory and process<br />
pertaining to these procedures are presented to students in dental hygiene courses. Students practice the procedures on student partners or manikins under<br />
direct faculty supervision. These procedures may be prescribed and provided to a community patient when such need has been determined during the<br />
assessment process; however, since adequate pool of patients is not always available, students are not required to achieve clinic competence prior to<br />
graduation.<br />
Last modified 08-28-09
NOTICE OF PRIVACY PRACTICES<br />
THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED<br />
AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.<br />
PLEASE REVIEW THIS NOTICE CAREFULLY.<br />
Each time you visit the Iowa Central Community College Dental Clinic, a record of your visit is made.<br />
This record includes information about your symptoms, examinations, medications you take, your<br />
allergies, your medical and dental histories and the plan for your care. This information we refer to as<br />
your health or dental record and is an essential part of the dental care we provide for you. Your dental<br />
record contains personal health information and there are state and federal laws to protect the privacy<br />
of your health information.<br />
In this notice we will tell you how we may use and disclose protected health information about you.<br />
Protected health information means any health information about you that could identify you (for<br />
example, your date of birth or social security number). In this notice, we will refer to protected health<br />
information as your health information.<br />
This notice will tell you about our privacy practices in accordance with the laws and will tell you<br />
about your rights and duties in regard to your health information. Also, it will describe how you<br />
can complain to us if you think we have violated your privacy rights.<br />
We are required by law to:<br />
a. maintain the privacy of your health information;<br />
b. provide you with notice of our legal duties and privacy practices; and<br />
c. abide by the terms of this Notice of Privacy Practices.<br />
HOW WE MAY USE AND DISCLOSE HEALTH INFORMATION ABOUT YOU<br />
For Treatment. All student dental hygienists, clinical staff, and supervisors involved in your care will read<br />
and document in your dental record about your examinations, the care plan for you, the care that you received<br />
and the results of that care. Your health information may be used and disclosed by those who are involved in<br />
your care for the purpose of providing, coordinating, or managing services and supports. This includes<br />
consultation with supervisors or other team members.<br />
If you were referred to us by another provider, your Iowa Central Community College Dental Clinic provider<br />
may send copies of your dental record to the provider who referred you to us so your provider will have updated<br />
treatment information about your care. We may share or disclose your health information with other health care<br />
providers so that the services you receive related to your health will be able to work together. For example, we<br />
may refer you to professionals for services we cannot provide so as to obtain new services for you. When we do<br />
this we need to tell them about you and your needs.<br />
We may also use information from your dental record to call you or send you a letter or postcard to remind you<br />
about an appointment, to follow up with diagnostic test results, to advise you of your treatment status, or to<br />
provide you with information about treatment and care that can benefit your health.<br />
For Payment. We may use and disclose health information about you so that we can receive payment for the<br />
services we provide to you. Examples of such activities are billing a third party payor, such as Medicaid or your<br />
insurance company. We may need, for example, to provide the Medicaid program with information about the<br />
services we provide to you so that we will be paid for those services. Also, we may need to provide the<br />
Medicaid program with information to make sure you are eligible for the medical assistance program.<br />
Last modified 08-28-09
For <strong>Health</strong> Care Operations. There are a few other ways we may use or disclose your health information for<br />
what are called health care operations. For example, we may use your health information to see where we can<br />
make improvements in the services we provide. We may use the information to explore ways to more<br />
efficiently manage our business, for licensing or accreditation activities, or for our compliance program.<br />
Iowa Central Community College Dental Clinic is a teaching facility so it is also probable that we will use<br />
your dental record in the process of educating and training students.<br />
You have the right to request a restriction on the above uses and disclosures of your protected health<br />
information for treatment, payment and health care operations; however, we are not required to agree to your<br />
request. If we do agree, we will comply with your request unless the information is needed to provide you<br />
emergency treatment. We may, however, also end the agreement at any time after informing you of such.<br />
OTHER USES AND DISCLOSURES OF YOUR HEALTH INFORMATION<br />
Disclosures to individuals involved in your care or payment for your care: We may disclose to a<br />
guardian/parent, personal representative, family member, or any other person identified by you, health<br />
information that is relevant to that person’s involvement with the support s and service s you receive or<br />
payment for that service and support. For example, if there is a health emergency, we may need to notify<br />
one of the above identified persons of your health situation. If there is a family member or other relative<br />
that you do not want us to disclose health information about you, please notify us via mail Renee Piper 303<br />
Avenue M, Fort Dodge Iowa 50501<br />
Verbal Permission: We may use or disclose your information to family members that are directly involved in<br />
your treatment with your verbal permission.<br />
Appointment Reminders: We may use and disclose health information to reschedule or remind you of<br />
appointments or meetings regarding your treatment.<br />
How We Will Contact You: If you want us to call or write to you only at your home or work or prefer<br />
some other way to reach you, we can usually arrange that. If you want to request that we communicate<br />
with you in a certain way or at a certain place, see “Right to Request Confidential Communications” in this<br />
Notice. Unless you tell us otherwise, we may contact you either by telephone or by mail at either your<br />
home or work. At either location, we may leave messages for you on the answering machine or voice mail<br />
concerning health information.<br />
Treatment and Service Alternatives: We may use or disclose your health information to tell you about or<br />
suggest possible treatments or services that may be of interest to you.<br />
Business Associates: Certain aspects and components of our services are performed through contracts with<br />
outside persons or organizations, such as auditing, accreditation, legal services, etc. At times it may be<br />
necessary for us to provide certain of your personal health information to one or more of these outside<br />
persons or organizations who assist us with our payment/billing activities and health care operations. In<br />
such cases, we require these business associates to appropriately safeguard the privacy of your information.<br />
Public <strong>Health</strong>: We may disclose health information about you for public health activities. These activities<br />
may include disclosures<br />
a. to a public health authority authorized by law to collect or receive such information for the purpose<br />
of preventing or controlling disease, injury, or disability;<br />
b. to appropriate authorities to receive reports of abuse and neglect;<br />
c. to FDA-regulated entities for purposes of monitoring or reporting the quality, safety, or<br />
effectiveness of FDA-regulated products; or<br />
Last modified 08-28-09
d. to notify a person who may have been exposed to a disease or may be at risk for contracting or<br />
spreading a disease or condition.<br />
For Law Enforcement Purposes: We may disclose health information about you to a law enforcement<br />
official as required by law, in response to a court, grand jury or administrative order, subpoena or warrant.<br />
We may also disclose health information to identify or locate a suspect, material witness, missing person or<br />
fugitive or about an actual or suspected crime victim if that person agrees to the disclosure. In limited<br />
circumstances, if we are unable to obtain that person’s agreement the information may still be disclosed.<br />
Threats to <strong>Health</strong> or Safety: We may use or disclose protected health information about you if we believe<br />
the disclosure or use is necessary to prevent or lessen an imminent or serious threat to the health or safety<br />
of a person or the public. We may also release information if we believe it is necessary for law enforcement<br />
to apprehend or identify a person who admitted participation in a violent crime or who is an escapee from a<br />
correctional institution or from lawful custody.<br />
Community <strong>Health</strong> Center Fort Dodge: Because Iowa Central Dental Hygiene and Community <strong>Health</strong><br />
Center Fort Dodge share an electronic record keeping system, your health information may be accessed by<br />
CHCFD employees for healthcare purposes.<br />
For Specific Government Functions: We may disclose the health information of military personnel and<br />
veterans to government benefit programs relating to eligibility and enrollment. We may disclose your<br />
health information to Worker’s Compensation and Disability programs, to correctional facilities if you are<br />
an inmate, and for national security reasons.<br />
We will not use information in your records for marketing purposes.<br />
Other uses and disclosures from your dental record will be made only with your written authorization or<br />
approval.<br />
YOUR RIGHTS REGARDING YOUR HEALTH INFORMATION<br />
You have the following rights regarding the health information we maintain about you. To exercise any of these<br />
rights, please submit your request in writing to us via mail, Renee Piper 303 Avenue M, Fort Dodge Iowa<br />
50501 or via phone at (800) 362-2793 ext.2335, or tell the student who is providing services to you and the<br />
student will provide to you a form for you to record your request.<br />
• Right of Access to Inspect and Copy Your Dental Records. You have the right, which may be<br />
restricted only in exceptional circumstances, to inspect and copy health information that may be used to<br />
make decisions about your care. Your right to inspect and copy health information will be restricted<br />
only in those situations where there is compelling evidence that access would cause serious harm to you.<br />
We may charge a reasonable, cost-based fee for copies. We will act on your request within thirty (30)<br />
calendar days after we receive your written request. If we deny the request, we will inform you of the<br />
reasons for the denial in writing, how you can have the denial reviewed, and how you may complain.<br />
• Right to Request an Amendment to Your Dental Records. If you feel that the health information we<br />
have about you is incorrect or incomplete, you may ask us in writing to amend the information although<br />
we are not required to agree to the amendment. We will act on your request within 60 (sixty) calendar<br />
days after we receive your request.<br />
• Right to an Accounting of Disclosures. You have the right to request in writing an accounting of<br />
certain of the disclosures that we make of your health information. This accounting may be for up to six<br />
years prior to the date on which you request the accounting but not before April 14, 2003. We may<br />
Last modified 08-28-09
charge you a reasonable fee if you request more than one accounting in any 12-month period. We will<br />
act on your request within sixty (60) calendar days after we receive your request.<br />
• Right to Request Restrictions on Use or Disclosure of Your <strong>Health</strong> Information. You have the<br />
right to request in writing a restriction or limitation on the use or disclosure of your health information<br />
for treatment, payment, or health care operations at any time. You also have the right to request that we<br />
restrict the use s or disclosure s we make to a family member or any other person you identify or to<br />
public/private entities for disaster relief. For example, you could ask that we not disclose your<br />
information to your sister or brother. We are not required to agree to any requested restriction.<br />
• Right to Request Confidential Communication. You have the right to request that we communicate<br />
with you about health matters in a certain way or at a certain location. For example, you may ask that<br />
we only contact you at home or by mail. You do not have to tell us why you are choosing this way of<br />
communicating confidential information. We may require an alternate method or address to contact<br />
you.<br />
• Right to a Copy of this Notice. You have the right to a paper copy of this Notice of Privacy Practices.<br />
To obtain a paper copy of this notice, please let us know.<br />
• The Dental Hygiene Program is in compliance with the Iowa Dental Practice Act, Occupational Safety<br />
Hazards Act (OSHA) and Center for Disease Control and Prevention (CDC), universal precautions and<br />
guidelines for preventing transmission of blood-borne pathogens as well as hazards control measures.<br />
There is potential risk even utilization of the above control measures.<br />
Iowa Central Community College reserves the right to change this Notice of Privacy Practices and its<br />
policies and procedures for privacy practices at any time and to make the changes effective for all<br />
protected health information created or received prior to the new effective date and then currently<br />
maintained by Iowa Central Community College’s Dental Clinic. The revised Notice will be posted in the<br />
College’s Dental Clinic lobby. You may also obtain a copy of the revised Notice from the Dental Clinic<br />
office.<br />
COMPLAINTS<br />
If you believe we have violated your privacy rights, you have the right to file a complaint in writing with us.<br />
To file a complaint, contact us via mail Renee Piper 303 Avenue M, Fort Dodge Iowa 50501 or via phone at<br />
(800) 362-2793 ext. 2335. You may complain to the Secretary of <strong>Health</strong> and Human Services at 200<br />
Independence Avenue, S.W. Washington, D.C. 20201 or by calling (202) 619-0257.<br />
You will not be retaliated against or treated differently for filing a complaint.<br />
If you have questions or problems:<br />
If you need more information or have questions about the privacy practices described above, please contact<br />
Renee Piper, 303 Avenue M, Fort Dodge Iowa 50501 or via phone at (800) 362-2793 ext. 2335.<br />
Effective Date: August 1, 2006<br />
Last modified 08-28-09
Consent for Use and Disclosure of <strong>Health</strong> Information<br />
Purpose: To obtain a client’s consent to use and disclosure of the client’s protected health information to carry out<br />
treatment, payment activities, and healthcare operations, as described more fully in Iowa Central Community<br />
College’s Notice of Privacy Practices.<br />
Client’s Name: ______________________________________________________________<br />
Address: ___________________________________________________________________<br />
Telephone: _______________________<br />
Purpose of Consent: By signing this form, you will consent to our use and disclosure of your protected health<br />
information to carry out treatment, payment activities, and health care operations.<br />
Notice of Privacy Practices: You have the right to read our Notice of Privacy Practices before you decide whether<br />
to sign this Consent. Our Notice provides a description of our treatment, payment activities, and healthcare<br />
operations, of the uses and disclosures we may make of your protected health information, and of other important<br />
matters about your protected health information. A copy of our Notice accompanies this Consent. We encourage you<br />
to read it carefully and completely before signing this Consent.<br />
We reserve the right to change our privacy practices as described in our Notice of Privacy Practices. If we change<br />
our privacy practices, we will issue a revised Notice of Privacy Practices, which will contain the changes. Those<br />
changes may apply to any of your protected health information that we maintain.<br />
You may obtain a copy of our Notice of Privacy Practices, including any revisions of our Notice, at any time by<br />
contacting: Iowa Central Dental Hygiene Clinic, One Triton Circle, Fort Dodge, Iowa 50501, 1-800-362-2793,<br />
extension 1327.<br />
Right to Revoke: You will have the right to revoke this Consent at any time by giving us written notice of your<br />
revocation submitted to the contact information listed above. Please understand that revocation of this Consent will<br />
not affect any action we took in reliance on this Consent before we received your revocation, and that we may<br />
decline to treat you or to continue treating you if you revoke this Consent.<br />
I have had full opportunity to read and consider the contents of this Consent form and your Notice of Privacy<br />
Practices. I understand that by, by signing this Consent form, I am giving my consent to your use and disclosure of<br />
my protected health information to carry out treatment, payment activities and health care operations.<br />
Client’s Signature: __________________________________________<br />
Date: _____________<br />
If the Consent is signed by a parent or personal representative on behalf of the client, complete<br />
the following:<br />
Personal Representative’s Name: __________________________________________________<br />
Relationship to Client: __________________________________________________________<br />
YOU ARE ENTITLED TO A COPY OF THIS CONSENT AFTER YOU SIGN IT