

2006 medical lecture - Addison's Disease Self Help Group
2006 medical lecture - Addison's Disease Self Help Group
2006 medical lecture - Addison's Disease Self Help Group

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
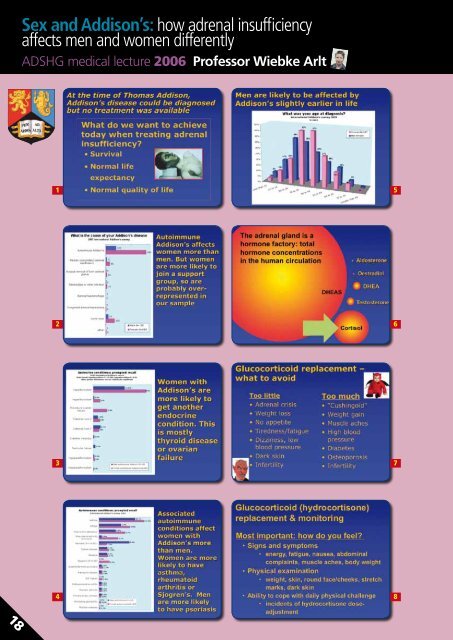
Sex and Addison’s: how adrenal insufficiency<br />
affects men and women differently<br />
ADSHG <strong>medical</strong> <strong>lecture</strong> <strong>2006</strong> Professor Wiebke Arlt<br />
1<br />
5<br />
2<br />
6<br />
3<br />
7<br />
4<br />
8<br />
18
9<br />
13<br />
10<br />
14<br />
11<br />
15<br />
12<br />
16<br />
19
Sex and Addison’s: how adrenal insufficiency<br />
affects men and women differently<br />
ADSHG <strong>medical</strong> <strong>lecture</strong> <strong>2006</strong><br />
Professor Wiebke Arlt (continued)<br />
17<br />
21<br />
18<br />
22<br />
19<br />
23<br />
20<br />
24<br />
20
25<br />
29<br />
26<br />
30<br />
27<br />
31<br />
28<br />
21
Sex and Addison’s: how adrenal insufficiency<br />
affects men and women differently<br />
ADSHG <strong>medical</strong> <strong>lecture</strong> <strong>2006</strong><br />
Professor Wiebke Arlt (continued)<br />
Despite pressing family commitments and a struggle with the<br />
tube, I was determined to attend the <strong>medical</strong> <strong>lecture</strong> to see some<br />
friendly faces and hear some juicy pointers on Addison’s and sex – I<br />
had somehow ignored the subtitle in my excitement. Professor<br />
Arlt opened her talk with the history of Dr Thomas Addison and<br />
the discovery of Addison’s in the 1850s. She made the interesting<br />
observation that four times more women than men develop<br />
Addison’s disease, and that women are more likely to develop<br />
a second endocrine condition, most often a thyroid condition<br />
or ovarian failure. Asthma and psoriasis are high contenders for<br />
accompanying (nonendocrine) autoimmune conditions, with asthma<br />
more common in women and psoriasis in men.<br />
Age also became a significant difference between the sexes, with<br />
men most likely to be diagnosed with Addison’s disease between<br />
20-29 and women between 30-50 years. Professor Arlt then<br />
illustrated the problems with diagnosis by comparing two hospital<br />
admissions. Typically, it is the tan that initially hinders diagnosis –<br />
because patient looks so well – while its association with extreme<br />
fatigue then achieves it.<br />
Looking at replacement therapy, Professor Arlt ‘asked the audience’<br />
and found the majority on hydrocortisone, with a few people<br />
taking prednisolone or cortisone acetate. The question on many<br />
lips was the usefulness of day curves. Professor Arlt explained that<br />
day curves are useful to track how serum cortisol is used by the<br />
body, but stressed they are only helpful if there is a record of the<br />
time the replacement hydrocortisone is taken. She then explained<br />
why mineralcorticoid replacement – the drug fludrocortisone - is<br />
required. Quite simply put, it is a blood pressure assistant. If the<br />
individual is on too little fludrocortisone, they will usually experience<br />
dizziness when standing up, and muscle cramps are also common.<br />
Hydrocortisone exerts a small amount of fludrocortisone activity in<br />
the body, therefore if there is a change in the type of replacement<br />
or the amount of hydrocortisone taken, it can affect fludrocortisone<br />
levels. At last I understand why I get cramps in hospital when I get<br />
put onto dexamethasone for emergency treatment!<br />
This was further explored by looking at the extra hydrocortisone<br />
requirements during surgery and in times of infection. When the<br />
hydrocortisone is increased to more than 50mg for illness or surgery,<br />
this has a fludrocortisone activity equivalent to 100mcg. So anyone<br />
whose normal fludrocortisone dose is 100mcg can probably safely<br />
stop taking it until they taper their hydrocortisone to less than<br />
50mg.<br />
Plasma renin is the most sensitive test of whether an individual is<br />
getting enough fludrocortisone, but it is not always reliable. It is not<br />
accurate during pregnancy, because of the additional pregnancy<br />
hormones in circulation, and it is likely to give a misleadingly low<br />
reading for anyone who also has diabetes or who is taking NSAIDs.<br />
In these circumstances it is best to rely on the broader indicators:<br />
blood pressure, sodium and potassium. Professor Arlt then<br />
tackled the management of Addison’s during pregnancy, with the<br />
observation that both fludrocortisone and hydrocortisone may need<br />
to be increased as the pregnancy advances, while high doses of<br />
intramuscular hydrocortisone are needed during delivery.<br />
Professor Arlt closed her presentation with a look at DHEA. The<br />
question of whether people with Addison’s need DHEA seems to<br />
be answered with a resounding yes. Tests are continuing to study<br />
whether immune function is improved on DHEA, and Professor<br />
Arlt has some results in the pipeline here. Studies show that people<br />
with Addison’s subjects report fatigue, dry skin and low libido as<br />
significant problems while on standard steroid replacement therapy;<br />
these symptoms are improved by DHEA. Women with Addison’s are<br />
noticeably more affected by low libido than men and report more<br />
improvement on DHEA replacement. In clinical trials conducted by<br />
Professor Arlt, four months of DHEA replacement therapy restored<br />
androgens to normal levels, which boosted sexuality. And this<br />
improvement has been observed and reported by the spouses of<br />
women taking part in clinical trials as well. Now that’s the juicy bit I<br />
was waiting for!<br />
Claire Allen<br />
22




