

Download a PDF of this issue - Field Exchange - Emergency ...
Download a PDF of this issue - Field Exchange - Emergency ...
Download a PDF of this issue - Field Exchange - Emergency ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Field</strong> article<br />
The implementation <strong>of</strong> the revised M&E system for<br />
the PRN has been halted due to delays in the printing<br />
and distribution <strong>of</strong> instruments required to collect<br />
health centre-level data. It is expected that final<br />
approved versions <strong>of</strong> the instruments will be printed<br />
and distributed by the end <strong>of</strong> 2011, with collection <strong>of</strong><br />
data starting in earnest from January 2012.<br />
Supplies and supply chain management<br />
The primary supplies for the PRN are therapeutic<br />
milks (F75 and F100), RUTF, CSB Plus, ReSoMal,<br />
routine drugs (e.g. antibiotics, vitamin A, deworming<br />
drugs, malaria prophylaxis, etc) and anthropometric<br />
equipment (including MUAC tapes, weighing scales<br />
and height/ length boards).<br />
The MoH receives support from several partners to<br />
procure the products required to treat acute malnutrition,<br />
including F75, F100, RUTF and ReSoMal. As<br />
mentioned, UNICEF and CHAI have been purchasing<br />
imported RUTF for the programme, although <strong>this</strong><br />
support was phased out in 2010.<br />
The WFP supplies CSB Plus to selected health<br />
centres in the southern and central parts <strong>of</strong> the country.<br />
Initially, <strong>this</strong> was done via NGOs but it is now<br />
supplied directly to the provincial health directorates<br />
(with financial support from WFP).<br />
Supply chain management capacity at different<br />
levels is limited. Stock-outs <strong>of</strong> RUTF, ReSoMal and<br />
therapeutic milks are <strong>of</strong>ten reported. In most cases, it<br />
is due to inadequate forecasting and communication<br />
between the different levels (health facility-districtprovince-central<br />
level). The weak and <strong>of</strong>ten late<br />
reporting <strong>of</strong> numbers <strong>of</strong> children treated is a major<br />
contributor to the forecasting challenges.<br />
Community involvement<br />
The community components <strong>of</strong> PRN in Mozambique<br />
were initiated as part <strong>of</strong> the pilot in Nampula Province<br />
in 2008 (see earlier). The pilot showed that the strategy<br />
<strong>of</strong> encouraging active community involvement quickly<br />
produced results. Health centres in the districts where<br />
community activities were being implemented<br />
(Memba, Eráti and Ribáué districts) experienced an<br />
increase in the number <strong>of</strong> referrals. However, requirements<br />
for RUTF resulting from the subsequent increase<br />
in caseloads had not been properly forecasted. When<br />
screening <strong>of</strong> acute malnutrition was integrated into<br />
activities <strong>of</strong> the monthly health day at provincial level,<br />
there were further increases in caseloads.<br />
Following the success <strong>of</strong> the pilot, the programme<br />
was expanded to other provinces including S<strong>of</strong>ala,<br />
Zambézia and Gaza. Save the Children (the main<br />
provider <strong>of</strong> technical assistance to MoH in <strong>this</strong> area)<br />
partnered with other community-based programmes to<br />
strengthen staff capacity. These staff have, in turn,<br />
Table 2: Individual and programme level monitoring forms<br />
Monitoring forms<br />
1 Referral form (MUAC, oedema, other signs) used<br />
by CHWs to refer cases to the health centres<br />
2 Inpatient individual health card, called the<br />
‘Multicard’ or Multicartão<br />
3 Monthly reporting form (admissions,<br />
discharges, mortality rates performance) for<br />
inpatient care; from facility to district and<br />
provincial health <strong>of</strong>fices<br />
4 PRN register book for outpatient care; SAM<br />
and MAM<br />
5 Malnutrition treatment card (Cartão do Doente<br />
Desnutrido) given to the caretaker to keep<br />
track <strong>of</strong> treatment and informing next<br />
appointment date<br />
6 Monthly reporting form (admissions,<br />
discharges, performance) for outpatient care;<br />
from facility to district and provincial health<br />
<strong>of</strong>fices<br />
Level used<br />
Community<br />
Inpatient<br />
Inpatient<br />
Outpatient<br />
Outpatient<br />
Outpatient<br />
supported the provincial and district health<br />
services in the implementation <strong>of</strong> the<br />
community strategies included in PRN.<br />
Partner support has included training <strong>of</strong><br />
trainers on community mobilisation in the<br />
context <strong>of</strong> PRN and home-based nutrition<br />
care for people living with HIV/AIDS in<br />
several provinces during 2011.<br />
The experience <strong>of</strong> Nampula Province<br />
showed that it is possible to develop a close<br />
link between health pr<strong>of</strong>essionals and<br />
community groups. Monthly meetings were<br />
conducted involving health pr<strong>of</strong>essionals<br />
and community groups, to discuss relevant<br />
health <strong>issue</strong>s. Health pr<strong>of</strong>essionals now<br />
recognise the importance <strong>of</strong> active community<br />
involvement for wide dissemination <strong>of</strong><br />
health messages and <strong>of</strong> community sensitisation<br />
to ensure early referrals, when the<br />
disease process is at a less advanced state<br />
and still relatively easy to treat. Many traditional<br />
healers now also recognise that the<br />
treatment <strong>of</strong> malnutrition is complex and<br />
requires referral <strong>of</strong> the child to the health<br />
centre for appropriate rehabilitation.<br />
However, it has still proven to be challenging<br />
to roll-out the community activities,<br />
in part because the focus so far has been at<br />
health facility level. There are a limited<br />
number <strong>of</strong> experienced staff who can<br />
provide technical assistance to the MoH’s<br />
efforts at community level. This will<br />
continue to be a problem unless additional<br />
efforts and funding are geared toward <strong>this</strong><br />
gap. The delay in printing and distribution<br />
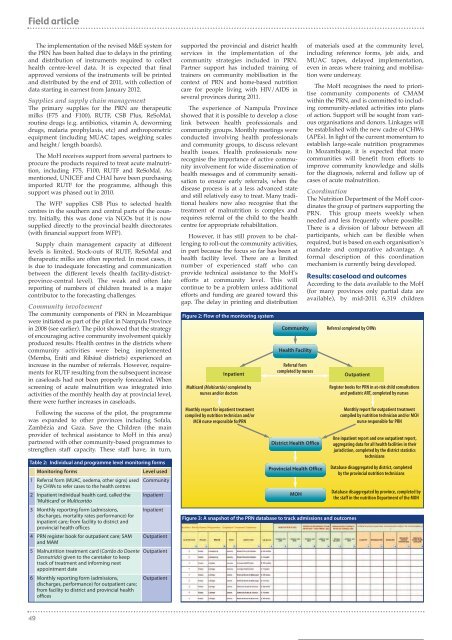
Figure 2: Flow <strong>of</strong> the monitoring system<br />
Inpatient<br />
Multicard (Multicartão) completed by<br />
nurses and/or doctors<br />
Monthly report for inpatient treatment<br />
compiled by nutrition technician and/or<br />
MCH nurse responsible forPRN<br />
Community<br />
Health Facility<br />
Referral form<br />
completed by nurses<br />
District Health Office<br />
Provincial Health Office<br />
MOH<br />
Referral completed by CHWs<br />
Figure 3: A snapshot <strong>of</strong> the PRN database to track admissions and outcomes<br />
<strong>of</strong> materials used at the community level,<br />
including reference forms, job aids, and<br />
MUAC tapes, delayed implementation,<br />
even in areas where training and mobilisation<br />
were underway.<br />
The MoH recognises the need to prioritise<br />
community components <strong>of</strong> CMAM<br />
within the PRN, and is committed to including<br />
community-related activities into plans<br />
<strong>of</strong> action. Support will be sought from various<br />
organisations and donors. Linkages will<br />
be established with the new cadre <strong>of</strong> CHWs<br />
(APEs). In light <strong>of</strong> the current momentum to<br />
establish large-scale nutrition programmes<br />
in Mozambique, it is expected that more<br />
communities will benefit from efforts to<br />
improve community knowledge and skills<br />
for the diagnosis, referral and follow up <strong>of</strong><br />
cases <strong>of</strong> acute malnutrition.<br />
Coordination<br />
The Nutrition Department <strong>of</strong> the MoH coordinates<br />
the group <strong>of</strong> partners supporting the<br />
PRN. This group meets weekly when<br />
needed and less frequently where possible.<br />
There is a division <strong>of</strong> labour between all<br />
participants, which can be flexible when<br />
required, but is based on each organisation’s<br />
mandate and comparative advantage. A<br />
formal description <strong>of</strong> <strong>this</strong> coordination<br />
mechanism is currently being developed.<br />
Results: caseload and outcomes<br />
According to the data available to the MoH<br />
(for many provinces only partial data are<br />
available), by mid-2011 6,319 children<br />
Outpatient<br />
Register books for PRN in at-risk child consultations<br />
and pediatric ART, completed by nurses<br />
Monthly report for outpatient treatment<br />
compiled by nutrition technician and/or MCH<br />
nurse responsible for PRN<br />
One inpatient report and one outpatient report,<br />
aggregating data for all health facilities in their<br />
jurisdiction, completed by the district statistics<br />
technicians<br />
Database disaggregated by district, completed<br />
by the provincial nutrition technicians<br />
Database disaggregated by province, completed by<br />
the staff in the nutrition Department <strong>of</strong> the MOH<br />
49














