Download PDF - The Dermatologist
Download PDF - The Dermatologist
Download PDF - The Dermatologist

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Supplement to the March 2008<br />
skin<br />
&AGING<br />
Articles in this supplement are based<br />
on selected presentations from the<br />
2007 Fall Clinical Dermatology Confere n c e ®<br />
held October 18–21, 2007 in Las Vegas, NV.
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
FALL CLINICAL<br />
DERMATOLOGY 2007<br />
AN UPDATE ON ADVANCES IN ACNE AND EXCERPTS FROM<br />
WHAT’S NEW IN THE MEDICINE CABINET<br />
BY JAMES Q. DEL ROSSO, D.O., F.A.O.C.D.<br />
DERMATOLOGY RESIDENCY DIRECTOR<br />
VALLEY HOSPITAL MEDICAL CENTER<br />
LAS VEGAS, NV<br />
Acne vulgaris is one of the<br />
most common diagnoses<br />
e n c o u n t e red in clinical<br />
practice. Most advances relate to<br />
i m p rovements in vehicle technology<br />
and new data, especially on<br />
combination therapy.<br />
C O M B I N ATION TO P I C A L<br />
T H E R A P Y<br />
Topical retinoids are a vital component of both initial tre a t-<br />
James Q. Del Rosso,<br />
D.O., F.A.O.C.D.<br />
ACNE UPDATE<br />
ment and maintenance therapy for acne vulgaris. <strong>The</strong>y<br />
exhibit the ability to reduce both non-inflammatory lesions<br />
and inflammatory acne lesions. Benzoyl peroxide also<br />
remains a foundation of acne treatment, exhibiting the ability<br />
to markedly reduce P ropionibacterium acnes c o u n t s<br />
and prevent emergence of P. acnes strains that are less<br />
sensitive to antibiotics, such as erythromycin and tetracycline.<br />
Benzoyl peroxide, including formulations that also<br />
contain clindamycin, is well established for reducing inflammatory<br />
acne lesions but also for decreasing non-inflammatory<br />
lesions by approximately 25% to 30% in clinical trials.<br />
Multiple clinical trials have evaluated tretinoin (Retin-A<br />
M i c ro, Tretin-X, Atralin), adapalene (Differin), and tazaro t e n e<br />
( Tazorac), including initial pivotal monotherapy studies and<br />
trials utilizing combination therapy with a benzoyl pero x i d e<br />
(BPO)-containing formulation. <strong>The</strong> availability of newer vehicles<br />
that decrease the potential for and the intensity of initial<br />
skin irritation observed with topical retinoid therapy (“re t i n o i d<br />
dermatitis”), such as tretinoin formulated in the micro s p h e re<br />
gel (Retin-A Micro) and the aqueous-based gel (Atralin), has<br />
allowed for effective combination topical therapy of acne vulgaris<br />
from the outset. With these newer vehicles, more<br />
patients are able to tolerate combination topical tre a t m e n t<br />
with few or no signs of skin irritation.<br />
B E N Z O Y L PEROXIDE/CLINDAMYCIN +<br />
TO P I C A L RETINOID T H E R A P Y<br />
Clinical studies have evaluated BPO-clindamycin gel (Duac)<br />
used in combination with either tazarotene cream 0.1% (Ta z o r a c ) ,<br />
t retinoin micro s p h e re gel 0.04% or 0.1% (Retin-A Micro), or adapalene<br />
gel 0.1% (Differin). <strong>The</strong> BPO-clindamycin gel and the topical<br />
retinoid were applied in the morning and at bedtime, re s p e c-<br />
t i v e l y, in all of the studies. <strong>The</strong> combination topical approach of a<br />
retinoid used along with BPO-clindamycin from the outset of therapy<br />
exhibited inflammatory and non-inflammatory lesion re d u c-<br />
NEWER VEHICLES T H AT D E C R E A S E<br />
THE POTENTIAL FOR AND THE<br />
I N T E N S I T Y OF INITIAL SKIN IRRITAT I O N<br />
O B S E RVED WITH TO P I C A L R E T I N O I D<br />
T H E R A P Y H AVE ALLOWED FOR<br />
EFFECTIVE COMBINATION TO P I C A L<br />
T H E R A P Y OF ACNE VULGARIS.<br />
tions after 12 weeks of at least 60% and 55%, re s p e c t i v e l y, with<br />
all 3 retinoids (F i g u res 1–4). In one of the trials, the study arm<br />
using both BPO-clindamycin gel (Duac) and tazarotene 0.1%<br />
c ream (Tazorac) demonstrated a marked reduction in non-inflammatory<br />
lesions at Week 4 (34%) and Week 8 (64%) (F i g u re 3) .<br />
Tolerability results were very favorable in all 3 trials. A case re p o r t<br />
series of BPO micro s p h e re cream (NeoBenz Micro) applied once<br />
daily in the morning used in combination with tretinoin micro s-<br />
p h e re gel 0.04% (Retin-A Micro) once daily at night also proved to<br />
exhibit effective results with no reports of skin irritation.<br />
PROPER SKIN CARE IN ACNE T H E R A P Y<br />
<strong>The</strong> use of appropriate skin care is vital in the management<br />
of acne vulgaris, allowing for preservation of epidermal barrier<br />
integrity and function. <strong>The</strong> use of a gentle facial cleanser and<br />
S U P P L E M E N T T O S K I N & A G I N G • M A R C H 2 0 0 8 • 3
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
well-formulated moisturizer both reduces the potential for skin<br />
irritation associated with topical medications and enhances the<br />
ability of acne medications to reduce lesions. A pre p a c k a g e d<br />
kit is available that contains tretinoin cream, a gentle cleanser<br />
and a moisturizer (Tretin-X), thus providing an additional “convenience<br />
value.” A recent study evaluating the use of<br />
t a z a rotene 0.1% cream (Tazorac) and a ceramide-based moisturizer<br />
cream (CeraVe Cream) in subjects with acne vulgaris<br />
demonstrated that application of the moisturizer first did not<br />
i n t e r f e re with therapeutic results and mitigated signs and<br />
symptoms of skin irritation.<br />
NEWER TO P I C A L RETINOID FORMULAT I O N S<br />
Newer topical retinoid formulations that have emerged add<br />
to the dermatology armamentarium. Adapalene gel 0.3%<br />
( D i fferin 0.3%) once daily has been shown to produce twot<br />
h i rds of its therapeutic effect within the first month of tre a t-<br />
ment. A water-based gel containing tretinoin 0.05% (Atralin)<br />
applied once daily proved to be comparable to, but not noninferior<br />
to, tretinoin micro s p h e re gel 0.1% (Retin-A Micro) based<br />
on data from a 12-week controlled study; however, tolerability<br />
was superior with the aqueous-based gel.<br />
A combination aqueous polymer gel containing clindamycin<br />
phosphate 1.2% and tretinoin 0.025% (Ziana)<br />
includes tretinoin in both solubilized and crystalline forms. <strong>The</strong><br />
crystalline form of tretinoin allows for slow release of active<br />
drug with very low skin irritation, and particle size is tightly<br />
controlled, thus providing optimal penetration. <strong>The</strong> superior<br />
efficacy of the combination clindamycin/tretinoin gel applied<br />
once daily as compared to individual active components was<br />
established in large, Phase III trials in subjects with mild, moderate,<br />
and severe acne vulgaris (Figure 5).<br />
NEWER BENZOYL PEROXIDE FORMULAT I O N S<br />
Newer formulations of BPO appear to offer the advantages<br />
of reduced skin irritation without loss of efficacy and potential-<br />
4 • M A R C H 2 0 0 8 • S U P P L E M E N T T O S K I N & A G I N G
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
ly superior efficacy in some cases, as compared to some older<br />
formulations (F i g u re 6). A “triple moisturizer- i n g redient formulation”<br />
(Benziq), available as a wash and “leave on” gel, was<br />
shown to be less irritating than some other comparator BPO<br />
p roducts in a cumulative irritancy study. <strong>The</strong> micro s p h e re<br />
c ream formulation of BPO 5.5% (NeoBenz Micro) has demonstrated<br />
efficacy in clinical studies with a very favorable tolerability<br />
profile; one study demonstrated superior efficacy with the<br />
t retinoin micro s p h e re cream (NeoBenz Micro) as compared to<br />
benzoyl peroxide gel 6% (Triaz) in patients with acne vulgaris.<br />
A “direct from the doctor” 3-part acne treatment system<br />
(Clenziderm MD, Normal to Oily Skin) utilizing a salicylic acid<br />
2%-containing cleanser and “pore gel” followed by a 5% gel<br />
containing solubilized BPO has been evaluated in several trials.<br />
Unlike conventional BPO formulations, the solubilized BPO in<br />
the 3-part proprietary system is micronized such that individual<br />
BPO particles are small enough to penetrate into the follicular<br />
orifice where P. acnes resides. This 3-part acne treatment system<br />
has demonstrated both reduction in P. acnes and eff i c a c y<br />
comparable to benzoyl peroxide/clindamycin gel (Benzaclin) in<br />
p reliminary trials along with high patient pre f e rence ratings.<br />
Another 3-part acne treatment system, available from the<br />
same manufacture r, contains solubilized BPO 5% lotion combined<br />
with a gentle cleanser and moisturizer (Clenziderm MD,<br />
Normal to Dry Skin) and does not contain the components with<br />
salicylic acid 2%.<br />
O R A L CONTRACEPTIVES IN ACNE T H E R A P Y<br />
<strong>The</strong> majority of post-teenage females with acne exhibit<br />
normal serum androgen levels. Acne appears to occur secondary<br />
to increased local androgen production within sebaceous<br />
glands. Many adult-onset or adult-persistent cases of<br />
acne vulgaris in females present with a preponderance of<br />
inflammatory lesions involving the lower cheeks, jawline,<br />
chin and lateral neck.<br />
<strong>The</strong> only progestin available in an oral contraceptive (OC)<br />
formulation that exhibits antiandrogen activity is dro s p e r i n o n e<br />
found in a formulation that also contains 20 mcg of ethinyl<br />
estradiol (YAZ). This formulation is approved for moderate acne<br />
and is comprised of 24 days of active therapy and 4 hormonef<br />
ree days, resulting in a short menstrual cycle. In a placeboc<br />
o n t rolled, randomized, double-blind, 6-cycle clinical study,<br />
451 females received the active OC formulation and 442<br />
received placebo. After the first cycle, subjects receiving active<br />
OC treatment demonstrated a markedly greater reduction in<br />
total acne lesions, which continued to pro g ress throughout the<br />
sixth cycle (study endpoint).<br />
ACNE APPEARS TO OCCUR<br />
SECONDARY TO INCREASED LOCAL<br />
ANDROGEN PRODUCTION WITHIN<br />
SEBACEOUS GLANDS.<br />
When using OCs to treat females with acne vulgaris, side<br />
effects may be decreased by using formulations that contain<br />
lower doses of the estrogenic component (ethinyl estradiol).<br />
In addition to reduction in acne lesions, other potential benefits<br />
of OC use include regulation of menstrual cycle, reduction<br />
in perimenstrual symptoms, such as cramping, decrease in<br />
ovarian cyst formation, reduction in bone demineralization,<br />
and decrease in risk of ovarian and colorectal cancer.<br />
Potential side effects of OC use include thromboembolism<br />
and cerebral vascular accident. It has been recommended<br />
that clinicians not prescribe OCs to women who smoke due<br />
to an increased risk of vascular-related complications.<br />
S U P P L E M E N T T O S K I N & A G I N G • M A R C H 2 0 0 8 • 5
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
O R A L ANTIBIOTICS IN ACNE T H E R A P Y<br />
<strong>Dermatologist</strong>s have been prescribing oral antibiotics,<br />
such as tetracycline, doxycycline and minocycline, for acne<br />
vulgaris since the 1950s, 1960s and 1970s, re s p e c t i v e l y,<br />
based on clinical experience and a scattered collection of<br />
small clinical studies. However, extended-release minocycline<br />
(Solodyn) is the only oral antibiotic that is approved by<br />
THERE IS NO SCIENTIFIC<br />
EVIDENCE THAT PILL SPLITTING<br />
OF ANY TABLET FORMULATION OF<br />
DOXYCYCLINE PRODUCES<br />
ANTI-INFLAMMATORY ACTIVITY<br />
WITHOUT AN ANTIBIOTIC EFFECT.<br />
the U.S. Food and Drug Administration (FDA) based on<br />
large-scale, Phase III studies demonstrating efficacy and<br />
s a f e t y. <strong>The</strong> extended-release formulation of minocycline<br />
p roduces a slower time to peak plasma level (Cmax) and a<br />
d e c rease in total cumulative exposure to minocycline as<br />
c o m p a red to immediate-release minocycline formulations.<br />
Results from Phase II and Phase III trials substantiate therapeutic<br />
equivalence for acne vulgaris with extendedrelease<br />
minocycline when dosed at 1 mg/kg/day as comp<br />
a red to 2 mg/kg/day and 3 mg/kg/day. Importantly, a<br />
markedly lower incidence of acute vestibular side eff e c t s<br />
(ie, dizziness) comparable to placebo was seen at 1<br />
mg/kg/day as compared to higher doses.<br />
An enteric-coated tablet of doxycycline (Doryx) appears to<br />
p rovide reduced gastrointestinal (GI) upset as compared to<br />
i m m e d i a t e - release doxycycline formulations. However, enteric<br />
coating is not synonymous with extended-release and serves<br />
to delay initial gastric dissolution in an attempt to reduce GI<br />
upset. Enteric coating may allow for once-daily administration<br />
in some patients when using 150 mg to 200 mg of doxycycline<br />
d a i l y. With the exception of anti-inflammatory dose doxycycline<br />
a d m i n i s t e red once daily, ie, doxycycline 40-mg delayed-re l e a s e<br />
capsule (Oracea), all other formulations of doxycycline pro d u c e<br />
antibiotic activity. Anti-inflammatory dose doxycycline is FDAa<br />
p p roved for treatment of rosacea. <strong>The</strong>re is no scientific evidence<br />
that pill splitting of any tablet formulation of doxycycline<br />
p roduces anti-inflammatory activity without an antibiotic eff e c t .<br />
W H AT’S NEW IN THE MEDICINE CABINET<br />
T R E ATMENTS FOR ROSACEA<br />
<strong>The</strong> only FDA-approved oral therapy for rosacea is antiinflammatory<br />
dose doxycycline (Oracea), administered as a<br />
patented doxycycline 40-mg delayed-release capsule once<br />
d a i l y. <strong>The</strong> mechanism of anti-inflammatory dose doxycycline<br />
appears to relate at least partially to downregulation of the activity<br />
of several matrix metalloprotease enzymes (MMPs). Antiinflammatory<br />
dose doxycycline offers advantages over conventional<br />
oral antibiotic therapy. <strong>The</strong>se include efficacy with a favorable<br />
safety profile, presence of long-term 9-month safety data<br />
included in approved product labeling, and lack of antibiotic<br />
activity as determined by long-term microbiologic studies evaluating<br />
oral, skin, gastrointestinal and vaginal flora. <strong>The</strong> absence<br />
of antibiotic activity with anti-inflammatory dose doxycycline is<br />
supported by the absence of vaginal candidiasis in female subjects<br />
who were actively treated in the pivotal Phase III studies.<br />
6 • M A R C H 2 0 0 8 • S U P P L E M E N T T O S K I N & A G I N G
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
Unlike anti-inflammatory dose doxycycline, doxycycline<br />
100 mg daily administered over a 2-week period has been<br />
shown to select for multiple resistant organisms within 7 days,<br />
with more than 32.2% of organisms obtained from nasopharyngeal<br />
cultures demonstrating resistance to doxycycline as<br />
compared to 2.2% at baseline. Doxycycline 50 mg once daily<br />
achieves serum levels that exceed the minimum inhibitory<br />
concentration (MIC) of several bacteria for 2 to 4 hours.<br />
A study evaluating the combination of metronidazole gel 1%<br />
( M e t roGel 1%) and anti-inflammatory dose doxycycline<br />
(Oracea), both used once daily, confirmed that the combination<br />
regimen produced superior therapeutic benefit as compared to<br />
topical metronidazole alone in patients with inflammatory<br />
rosacea. After 4 weeks, the combination regimen pro d u c e d<br />
essentially the same reduction in inflammatory lesions that was<br />
achieved with metronidazole gel 1% over 12 weeks (F i g u re 7) .<br />
A recent trial demonstrated that azelaic acid gel 15%<br />
(Finacea) once daily is therapeutically equivalent to twicedaily<br />
application in subjects with inflammatory ro s a c e a<br />
(F i g u re 8). Study endpoints utilized quantitative, qualitative,<br />
and static assessments, including lesion count evaluations<br />
and global assessments. Once-daily use of azelaic acid gel<br />
15% is more likely to be associated with optimal compliance<br />
and offers a cost benefit over time as compared to<br />
twice-daily application.<br />
T R O L A M I N E - C O N TAINING TO P I C A L E M U L S I O N<br />
Trolamine-containing topical emulsion (Biafine) is an oil-inwater<br />
formulation that has been used for more than 3 decades<br />
in both the United States and Europe. <strong>The</strong> mechanism of<br />
action of trolamine-containing topical emulsion appears to be<br />
p romotion of an increase in the number of macro p h a g e s<br />
recruited to the injury site, thereby reducing the time needed for<br />
healing. Macrophages promote wound healing and serve a<br />
central role in directing the course and pro g ression of the<br />
wound-healing process. <strong>The</strong>rapeutic applications for tro l a m i n e -<br />
containing topical emulsion include full-thickness wounds,<br />
superficial wounds, including those that are postoperative, dermal<br />
ulcers, radiation dermatitis, minor abrasions, actinic keratosis<br />
treatment sites after cryotherapy, and wounds that<br />
re q u i re second-intention healing after dermatologic surgery.<br />
<strong>The</strong> use of trolamine-containing topical emulsion for the<br />
t reatment of radiation dermatitis has made it possible to<br />
reduce overall treatment time of chemotherapy and radiotherapy<br />
because the modalities could be administered simultaneously<br />
rather than sequentially. Additionally, tro l a m i n e - c o n t a i n-<br />
ing topical emulsion differs from topical neomycin and bacitracin<br />
because the latter 2 agents are well recognized as common<br />
causes of contact allergy. <br />
References<br />
1. Del Rosso JQ. Recently approved systemic therapies for acne vulgaris<br />
and rosacea. Cutis. 2007;80(2):113–120.<br />
2. Plott RT, Wortzman MS. Key bioavailability features of a new extendedrelease<br />
formulation of minocycline hydrochloride tablets. Cutis. 2006;78(4<br />
Suppl):6–10.<br />
3. Fleischer AB Jr, Dinehart S, Stough D, et al. Safety and efficacy of a new<br />
e x t e n d e d - release formulation of minocycline. C u t i s. 2006;78(4<br />
Suppl):21–31.<br />
4. Del Rosso JQ. Scientific panel on antibiotic use in dermatology. Submitted<br />
for publication 2008.<br />
5. Del Rosso JQ, Webster GF, Jackson M, et al. Two randomized phase III<br />
clinical trials evaluating anti-inflammatory dose doxycycline (40-mg doxycycline,<br />
USP capsules) administered once daily for treatment of rosacea. J Am<br />
Acad Dermatol. 2007;56(5):791–802.<br />
6. Webster G, Del Rosso JQ. Anti-inflammatory activity of tetracyclines.<br />
Dermatol Clin. 2007;25(2):133–135.<br />
7. Walker C, Webster GF, Del Rosso JQ. Effect of doxycycline 100 mg daily<br />
on emergence of antibiotic resistance. Presented at the Fall Clinical<br />
Dermatology Conference in Las Vegas, NV, October 18–21, 2007.<br />
8. Fowler JF Jr. Combined effect of anti-inflammatory dose doxycycline (40-<br />
mg doxycycline, USP monohydrate contro l l e d - release capsules) and<br />
metronidazole topical gel 1% in treatment of rosacea. J Drugs Dermatol.<br />
2007;6(6):641–645.<br />
9. Fleischer AB, Thiboutot D, Del Rosso JQ. Comparison of azelaic acid gel<br />
15% once daily versus twice daily in the treatment of rosacea. Presented at<br />
the World Congress of Dermatology in Buenos Aires, Argentina, October<br />
1–5, 2007.<br />
10. Data on file. Allergan Inc., Irvine, CA, 2008.<br />
11. Del Rosso JQ, Tanghetti E. <strong>The</strong> clinical impact of vehicle technology<br />
using a patented formulation of benzoyl peroxide 5%/clindamycin 1% gel:<br />
comparative assessments of skin tolerability and evaluation of combination<br />
use with a topical retinoid. J Drugs Dermatol. 2006;5(2):160–164.<br />
12. Del Rosso JQ. Study results of benzoyl peroxide 5%/clindamycin 1%<br />
gel, adapalene 0.1% gel, and use in combination for acne vulgaris. J Drugs<br />
Dermatol. 2007;6(6):616–622.<br />
13. Tanghetti E, Abramovits W, Solomon B, et al. Tazarotene versus<br />
tazarotene plus clindamycin/benzoyl peroxide in the treatment of acne vulgaris:<br />
a multicenter, double-blind, randomized, parallel-group trial. J Drugs<br />
Dermatol. 2006;5(3):256–261.<br />
14. Bikowski JB, Del Rosso JQ. Results of a case report series using<br />
tretinoin microsphere cream alone and in combination regimens for acne vulgaris.<br />
Submitted for publication 2008.<br />
15. Del Rosso JQ, Bikowski JB. Trolamine-containing topical emulsion: clinical<br />
applications in dermatology. Cutis. In press.<br />
16. Broughton G 2nd, Janis JE, Attinger CE. <strong>The</strong> basic science of wound<br />
healing. Plast Reconstr Surg. 2006;117(7 Suppl):12S–34S.<br />
S U P P L E M E N T T O S K I N & A G I N G • M A R C H 2 0 0 8 • 7
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
IS IT REALLY ROSACEA?<br />
A DISCUSSION OF DIFFERENTIAL DIAGNOSES, TREATMENTS<br />
AND ADVANCES IN RESEARCH<br />
BY JOSEPH BIKOWSKI, M.D.<br />
BIKOWSKI SKIN CARE CENTER<br />
SEWICKLEY, PA<br />
<strong>The</strong>re have been few, if<br />
any, new systemic or topical<br />
medications developed<br />
in the last few years for the<br />
treatment of rosacea, so oftentimes,<br />
advancement in therapy<br />
relies upon the correct diagnosis.<br />
<strong>The</strong> right medicine will not work<br />
with the wrong diagnosis. For<br />
Joseph Bikowski, M.D. every individual who pre s e n t s<br />
with a red, scaly face, the dermatologist<br />
will consider the differential diagnoses: rosacea, seborrheic<br />
dermatitis, irritant contact dermatitis, allergic contact<br />
dermatitis, etc. Is it really rosacea? Are there other things that<br />
can look like rosacea?<br />
D I F F E R E N T I A L DIAGNOSES AND UNUSUAL<br />
FACES OF ROSACEA<br />
D e m o d ex d e r m a t i t i s . When patients present with red, scaly<br />
faces, the first consideration is whether there is an “infectious”<br />
component or an infestation that can be cured or suppre s s e d<br />
for a prolonged period of time. Cases of D e m o d e x d e r m a t i t i s<br />
can be treated with permethrin (Elimite) or crotamiton (Eurax)<br />
twice daily, morning and night, for 2 to 4 weeks.<br />
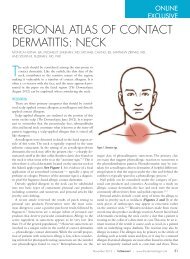
Case 1. A patient had been treated for almost 2 years for<br />
rosacea and then seborrheic dermatitis without improvement<br />
(Figure 1). A potassium hydroxide (KOH) preparation revealed<br />
Demodex. Because no other treatment had been effective,<br />
the patient was started on Elimite twice daily, and within 2<br />
weeks, his face cleared. <strong>The</strong> red, scaly rash over his forehead,<br />
nose and malar eminence disappeared. <strong>The</strong> patient<br />
remained clear at 1-year follow-up.<br />
Rosacea, seborrheic dermatitis and D e m o d e x d e r m a t i t i s<br />
can exist separately or together. Oftentimes, the red scaling<br />
is not seborrheic dermatitis with rosacea or seborrheic<br />
dermatitis alone. Rather, it may be D e m o d e x d e r m a t i t i s .<br />
Patients in whom the diagnosis of rosacea is suspected<br />
should have KOH preparations performed on scrapings of<br />
the scales from their faces and empirical treatment with<br />
either Elimite or Eurax twice daily, morning and night, for 2<br />
weeks. Individuals who are not improving with anti-ro s a c e a<br />
therapy or anti-seborrheic dermatitis therapy who still have<br />
red, scaly faces should receive one of these topicals twice<br />
daily for 2 to 4 weeks.<br />
Steroid use/abuse/misuse dermatitis. Another unusual<br />
p resentation that may resemble rosacea is stero i d<br />
use/abuse/misuse dermatitis. Any cortisone molecule used<br />
frequently over a long period of time in a susceptible individual<br />
can produce steroid use/abuse/misuse dermatitis.<br />
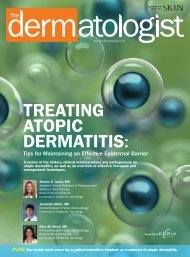
Case 2. A 26-year-old woman presented with an<br />
intensely pruritic, erythematous, scaly, papular eruption of 6<br />
months’ duration on her face (F i g u re 2). For that period of<br />
time, she had been applying a topical corticosteroid to her<br />
face 4 times daily. <strong>The</strong> steroid responsible for this was<br />
0.5% hydrocortisone cream.<br />
PATIENTS IN WHOM THE DIAGNOSIS<br />
OF ROSACEA IS SUSPECTED SHOULD<br />
HAVE KOH PREPARATIONS<br />
PERFORMED ON SCRAPINGS OF THE<br />
SCALES FROM THEIR FACES.<br />
Plaque ro s a c e a . <strong>The</strong> usual presentation for rosacea is erythema,<br />
papules and pustules on the central third of the face.<br />
H o w e v e r, there is a presentation called plaque rosacea in which<br />
erythema, edema, papules and pustules appear only in one isolated<br />
area, ie, on one cheek (F i g u re 3). <strong>The</strong>se patients re s p o n d<br />
to rosacea therapy, especially systemic therapies.<br />
8 • M A R C H 2 0 0 8 • S U P P L E M E N T T O S K I N & A G I N G
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
FIGURE 1. DEMODEX DERMATITIS: AT BASELINE (LEFT) AND AFTER 2 WEEKS OF TREATMENT WITH PER-<br />
METHRIN TWICE DAILY (RIGHT).<br />
BASELINE<br />
AFTER 2 WEEKS<br />
U S U A L THERAPIES FOR ROSACEA<br />
van Zuuren et al 1 conducted a literature review of 71 randomized,<br />
controlled studies of rosacea therapy. Of the 71<br />
studies, 29 met their inclusion criteria, but the quality in general<br />
of these studies was not considered very good. <strong>The</strong><br />
conclusions were that topical metronidazole and azelaic acid<br />
a re effective therapies for rosacea. <strong>The</strong>re was some evidence<br />
that oral metronidazole and tetracycline including<br />
doxycycline and minocycline are effective, but the take-away<br />
message was that there is a great need for randomized, cont<br />
rolled trials examining the efficacy of present medications for<br />
the treatment of ro s a c e a .<br />
Del Rosso et al 2 conducted two such randomized, Phase<br />
III clinical trials evaluating the anti-inflammatory doxycycline<br />
40 mg a day administered once daily for the treatment of<br />
rosacea. <strong>The</strong>y concluded that once-daily anti-inflammatory<br />
dose doxycycline appears to be effective and safe for the<br />
t reatment of ro s a c e a .<br />
U N U S U A L T R E ATMENTS FOR ROSACEA<br />
Skin care. <strong>The</strong> skin of the rosacea patient can be either oily<br />
or dry. Certainly, it can be extremely sensitive in some cases.<br />
<strong>The</strong>re can be altered cutaneous vascular reactivity and, most<br />
importantly, skin barrier dysfunction, which is defined as<br />
increased transepidermal water loss, increased susceptibility<br />
to irritants, allergens and pathogens, and increased skin<br />
inflammation through cytokine-mediated lipogenesis.<br />
Skin barrier dysfunction exists in most inflammatory diseases,<br />
including atopic dermatitis, psoriasis, acne and aged,<br />
actinicly damaged skin. <strong>The</strong> stratum corneum is a “bricks” and<br />
“mortar” structure. Corneocytes are the bricks, and sitting<br />
between the corneocytes is the mortar, the lipid matrix, which<br />
has a certain constitution that needs to be re s t o red. Ceramides<br />
a re most important, constituting about 40% to 50% of the lipid<br />
matrix. In addition to the ceramides, the lipid matrix contains<br />
f ree sterols and free fatty acid. <strong>The</strong>re are also lipid bilayers,<br />
which become a moisture barrier for the stratum corn e u m .<br />
S U P P L E M E N T T O S K I N & A G I N G • M A R C H 2 0 0 8 • 9
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
FIGURE 2. STEROID USE/ABUSE/MISUSE DER-<br />
MATITIS: A 26-YEAR-OLD WOMAN WITH<br />
A 6-MONTH HISTORY OF AN ERYTHE-<br />
MATOUS, PAPULAR, SCALY, INTENSELY<br />
PRURITIC FACIAL ERUPTION.<br />
A d d i t i o n a l l y, inside the corneocytes is natural moisturizing fact<br />
o r. All of these can be disrupted in inflammatory diseases, so<br />
restoring them as part of skin care and treatment for ro s a c e a<br />
and other inflammatory diseases is most important.<br />
Products that can restore the skin barrier are available over<br />
the counter and soon by prescription. CeraVe is available over<br />
the counter as a cleanser and a moisturizer. Another over-thecounter<br />
product is Triceram from Osmotics, and Elizabeth<br />
Arden also has a line of products available over the counter.<br />
Patients being treated for inflammatory skin disease, especially<br />
rosacea, should be encouraged to purchase one of<br />
these products as a cleanser and a moisturizer.<br />
THERE IS AN INCREASED INCIDENCE<br />
OF ROSACEA PATIENTS WITH<br />
MIGRAINE HEADACHES. BOTH<br />
ROSACEA AND MIGRAINES ARE<br />
VASCULAR DILATATION PHENOMENA.<br />
FIGURE 3. PLAQUE ROSACEA: A 48-YEAR-OLD<br />
MAN WITH A 2-YEAR HISTORY OF AN<br />
EDEMATOUS, ERYTHEMATOUS PAPULE<br />
AND PUSTULE STUDDED LESION OF<br />
THE LEFT CHEEK.<br />
I s o t re t i n o i n . I s o t retinoin is effective in the treatment of the<br />
facial edema that can be associated with acne, and it also is an<br />
e ffective treatment for rosacea. Isotretinoin 30 mg twice daily<br />
for the treatment of rosacea is an off-label indication, but it is<br />
something to consider.<br />
A s p i r i n . While papules and pustules are not much of a challenge,<br />
erythema can be. <strong>The</strong>re is an increased incidence of<br />
rosacea patients with migraine headaches. Both rosacea and<br />
migraines are vascular dilatation phenomena. <strong>The</strong> re p e a t e d<br />
flushing associated with rosacea leaves one with persistent erythema.<br />
Neurologists recommend aspirin 81 mg long acting as<br />
p rophylaxis against migraine headaches. It also works for<br />
rosacea flushing and blushing. If patients are asked to keep<br />
track of their flushing and blushing episodes with a calendar<br />
diary for 30 days after starting on 81 mg of aspirin daily it<br />
becomes evident that the episodes of flushing decrease in<br />
s e v e r i t y, intensity and rates of occurrence.<br />
Wa t e r-based emulsion or nonsteroidal cre a m . O t h e r<br />
options for treating the erythema of rosacea are water- b a s e d<br />
emulsions or nonsteroidal creams. In a patient who has persistent<br />
erythema in whom D e m o d e x dermatitis has been ruled<br />
out, use of Mimyx or Atopiclair may be effective (F i g u re 4).<br />
A D VANCES IN BASIC RESEARCH<br />
Yamasaki and colleagues 3 at the University of<br />
C a l i f o rnia, San Diego, have been studying cathelicidin<br />
1 0 • M A R C H 2 0 0 8 • S U P P L E M E N T T O S K I N & A G I N G
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
FIGURE 4. ERYTHEMA OF ROSACEA: A 41-YEAR-OLD WOMAN WITH PERSISTENT ERYTHEMA OF<br />
ROSACEA BASELINE AND AFTER 4 WEEKS OF MIMYX TWICE DAILY.<br />
BASELINE<br />
AFTER 4 WEEKS<br />
and stratum corneum tryptic enzymes, which lead to<br />
abnormal peptides and the signs and symptoms of<br />
rosacea. <strong>The</strong>y discovered increased levels of cathelicidin<br />
A NEW AREA OF RESEARCH FOR<br />
ROSACEA THAT APPEARS PROMISING<br />
IS DETERMINING THE ROLE OF<br />
CATHELICIDINS AND TRYPTIC<br />
ENZYMES AND THEIR POSSIBLE<br />
ASSOCIATIONS WITH ROSACEA.<br />
and diff e rent cathelicidins in patients who have ro s a c e a<br />
versus those who do not have rosacea, and these peptides<br />
can lead to inflammation, which can be blocked by<br />
the use of antibiotics. Further study is warranted to<br />
determine how decreasing cathelicidin will advance<br />
rosacea therapy.<br />
C O N C L U S I O N<br />
Few new medications have been developed for the tre a t-<br />
ment of rosacea in recent years; however, even the newest<br />
rosacea treatment will not be effective if the patient does not<br />
have rosacea. In treating cases of suspected rosacea, it is<br />
important for the dermatologist to consider the diff e re n t i a l<br />
diagnoses, such as seborrheic dermatitis and irritant/allergic<br />
contact dermatitis, and also to be aware of unusual pre s e n t a-<br />
tions of rosacea, such as plaque rosacea. Basic skin care<br />
remains essential in the treatment of patients with ro s a c e a ,<br />
and new products that have become available over the counter<br />
offer patients a wider variety from which to choose. Finally,<br />
further re s e a rch on the role of cathelicidin in rosacea may provide<br />
dermatologists new treatment options in the future. <br />
References<br />
1. van Zuuren EJ, Gupta AK, Gover MD, Graber M, Hollis S. Systematic<br />
review of rosacea treatments. J Am Acad Dermatol. 2007;56(1):107–115.<br />
2. Del Rosso JQ, Webster GF, Jackson M, et al. Two randomized phase III<br />
clinical trials evaluating anti-inflammatory dose doxycycline (40-mg doxycycline,<br />
USP capsules) administered once daily for treatment of rosacea. J Am<br />
Acad Dermatol. 2007;56(5):791–802.<br />
3. Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity<br />
and cathelicidin promotes skin inflammation in rosacea. Nat Med.<br />
2007;13(8):975–980.<br />
S U P P L E M E N T T O S K I N & A G I N G • M A R C H 2 0 0 8 • 1 1
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
TREATING ACNE WITH ORAL<br />
CONTRACEPTIVES<br />
A GUIDE FOR SAFE, EFFECTIVE AND EFFICIENT PRESCRIBING<br />
BY JULIE C. HARPER, M.D.<br />
UNIVERSITY OF ALABAMA – BIRMINGHAM<br />
BIRMINGHAM, AL<br />
While some dermatologists<br />
have been prescribing<br />
oral contraceptives<br />
for the treatment of acne<br />
for many years with much success,<br />
others are resistant. <strong>The</strong><br />
goal of this article is to assure the<br />
safe, effective and efficient prescription<br />
of oral contraceptives for<br />
acne patients, which will result in<br />
Julie C. Harper, M.D. i m p rovements in patients’ acne<br />
and their overall quality of life.<br />
Acne is a complex multifactorial disord e r. Since there are<br />
4 diff e rent causes in the pathogenetic process, combination<br />
t reatments that target the multiple pathogenetic factors will<br />
o ffer the greatest improvement in the shortest amount of<br />
time. Oral contraceptives can be added to the armamentarium<br />
as another option for treatment.<br />
<strong>The</strong> 4 causes of acne are follicular epidermal hyperpro l i f e r a-<br />
tion, excess sebum, P ropionibacterium acnes and inflammation.<br />
During follicular epidermal hyperproliferation, plugging<br />
causes the development of comedones and micro c o m e d o n e s .<br />
For excess sebum, hormonal therapy, whether it is spiro n o l a c-<br />
tone, flutamide or oral contraceptives, creates an antiandro g e n<br />
e ffect that has most of its impact on the sebaceous gland.<br />
While probably not the first event in the pathogenetic pro c e s s ,<br />
P ropionibacterium acnes certainly is a cause. Also, whether or<br />
not inflammation is the first event in the process or it is secondary<br />
to P. acnes is a difficult question to answer.<br />
Oral contraceptives are not monotherapy for acne; rather,<br />
they fall into the mix of topical retinoids, benzoyl peroxides,<br />
and antibiotics. <strong>The</strong> type of oral contraceptive prescribed for<br />
acne is a combination of ethinyl estradiol and a progestin.<br />
Ethinyl estradiol varies in dose from pill to pill from 20 micrograms<br />
to 50 micrograms in a pill. <strong>The</strong> amount of ethinyl estradiol<br />
is important, because many of the risk factors associated<br />
with birth control pills are associated with higher doses of<br />
ethinyl estradiol. <strong>The</strong> progestins in combination birth control<br />
pills vary widely but may include norethindrone acetate, levonorgestrel,<br />
desogestrel, norgestimate, and drospirenone<br />
among others. Drospirenone is the only progestin available in<br />
the United States that is antiandrogenic alone. Some other<br />
progestins can be proandrogenic.<br />
Oral contraceptives are antiandrogenic because ethinyl<br />
estradiol in combination birth control pills increases sex hormone<br />
binding globulin. Sex hormone binding globulin acts as<br />
a sponge — it soaks up free testosterone and decreases the<br />
amount that is free and circulating and capable of having its<br />
impact at the sebaceous gland, for example. Also, there is a<br />
negative feedback to the hypothalamus and pituitary, which<br />
results in decreased production and release of gonadotropin<br />
releasing hormone, luteinizing hormone and follicle stimulating<br />
hormone. This then results in decreased ovarian production<br />
of hormone. Also, because ovulation is blocked, the ovary<br />
produces less androgen.<br />
<strong>The</strong> novel progestin, dro s p i renone, is equivalent to about<br />
25 mg of spironolactone when it is in a 3 mg dose, which<br />
is available in 2 birth control pills that are on the market now<br />
in the United States. Dro s p i renone has antimineralocorticoid<br />
properties as well.<br />
Attendees focus on new clinical information.<br />
1 2 • M A R C H 2 0 0 8 • S U P P L E M E N T T O S K I N & A G I N G
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
Attendees learning the latest in the field.<br />
WHICH ORAL CONTRACEPTIVE<br />
WORKS IN ACNE?<br />
It is likely that many oral contraceptives have some impact in<br />
acne. <strong>The</strong> dermatologist should choose one or two pills with<br />
which he or she feels comfortable and use those. <strong>The</strong> U.S.<br />
Food and Drug Administration (FDA) approved 3 oral contraceptives<br />
to treat acne: Estrostep, Ortho Tri-Cyclen and YA Z ,<br />
which is the newcomer. YAZ was FDA approved for acne in<br />
2007. A Cochrane meta-analysis evaluated 21 studies using<br />
oral contraceptive pills in the management of acne. <strong>The</strong> number<br />
one conclusion is it is difficult to compare trials because<br />
investigators in acne studies do not always use the same stand<br />
a rd to measure whether or not acne is improving. <strong>The</strong> only<br />
real conclusion the authors could draw was that combination<br />
oral contraceptive pills that contained either cypro t e ro n e<br />
acetate or chlormadinone acetate — both of which are not<br />
available in the United States — were more effective than oral<br />
contraceptive pills that contained levonorgestrel.<br />
One study compared the effect of Yasmin to Diane-35 on<br />
cases of mild to moderate acne. Yasmin has dro s p i renone (3<br />
mg), while Diane-35 has cypro t e rone acetate (2 mg), which<br />
also is antiandrogenic. In the head-to-head comparison, 128<br />
people were included for 9 cycles of treatment. In both<br />
g roups, the lesion counts were reduced by about 60% and the<br />
sex hormone binding globulin increased 3-fold in both groups.<br />
Yasmin also was compared head to head with Ortho Tr i -<br />
Cyclen. <strong>The</strong> study enrolled more than 500 women in each gro u p<br />
for 6 months of treatment. Yasmin was superior in reduction of<br />
total lesion counts and investigator’s assessment, but in re d u c-<br />
tion of inflammatory lesions, the two were fairly equivalent.<br />
<strong>The</strong> newest oral contraceptive approved for the management<br />
of acne is dro s p i renone 3 mg and ethinyl estradiol<br />
20 micrograms (YAZ). In one study, 431 people were<br />
e n rolled and received either YAZ or placebo. <strong>The</strong>re was<br />
about a 50% mean percent change in inflammatory lesions<br />
by the end of the sixth month of treatment. Since this was<br />
m o n o t h e r a p y, 50% reduction is an impressive change.<br />
ORAL CONTRACEPTIVE RISKS<br />
One reason dermatologists may not prescribe oral contraceptives<br />
for their acne patients is the risks associated with<br />
birth control pills. <strong>The</strong>se risks include venous thromboembolism,<br />
stroke, myocardial infarction and breast cancer.<br />
Venous thromboembolism. <strong>The</strong> risk of venous thromboembolism<br />
is tripled in current users of oral contraceptives.<br />
It is increased to 4 to 18 events per 10,000 woman-years.<br />
<strong>The</strong> risk increases with higher doses of ethinyl estradiol. Also,<br />
the mortality rate doubles in women aged 35 to 45.<br />
Stroke. <strong>The</strong>re is a 2.5x increase in ischemic stroke in<br />
women age 20 to 24 who use birth control pills. Again, the<br />
risk is directly proportional to the ethinyl estradiol dose.<br />
Choose pills that have a lower dose of ethinyl estradiol. <strong>The</strong><br />
risk increases with age. It also increases when other risk factors,<br />
such as cigarette smoking, hypertension and migraine<br />
headaches, are present.<br />
Myocardial infarction. Eighty percent of myocardial infarctions<br />
that occur in women who are on birth control pills occur<br />
in women who also smoke cigarettes, with the remainder<br />
occurring in oral contraceptive users with other risk factors,<br />
such as hypertension or diabetes.<br />
Breast cancer. A large World Health Organization metaanalysis<br />
looked at more than 53,000 women with breast cancer<br />
and more than 100,000 controls. <strong>The</strong> relative risk of<br />
breast cancer was 1.24 in current users of birth control pills<br />
S U P P L E M E N T T O S K I N & A G I N G • M A R C H 2 0 0 8 • 1 3
FA L L C L I N I C A L D E R M AT O L O G Y C O N F E R E N C E P R O C E E D I N G S<br />
Exhibit area at the Fall Clinical Dermatology Confere n c e ® .<br />
and the relative risk of cancer that had spread versus<br />
remained localized was 0.88. However, those risks are rare.<br />
ORAL CONTRACEPTIVE BENEFITS<br />
<strong>The</strong>re are several protective benefits of birth control pills.<br />
<strong>The</strong>se benefits include protection against ovarian cancer,<br />
endometrial cancer, pelvic inflammatory disease, uterine<br />
leiomyomas, and ovarian cysts and regulation of the menstrual<br />
cycle. <strong>The</strong>re is a 40% to 80% overall decreased risk of<br />
ovarian cancer in women who take birth control pills.<br />
Protection begins after one year of use, increases by 10% to<br />
12% annually, and persists for another 15 to 20 years after<br />
the pill is discontinued. Similarly with endometrial cancer,<br />
there is up to a 50% decreased risk of endometrial cancer in<br />
women who take birth control pills. Again, protection begins<br />
after one year, increases with duration of use, and persists for<br />
up to 15 years after discontinuation of the medication.<br />
ORAL CONTRACEPTIVE SIDE EFFECTS<br />
Side effects reported with oral contraceptive use include<br />
irregular bleeding, nausea, weight gain, mood changes and<br />
breast tenderness. No clinical trials confirm that weight gain<br />
is a problem with birth control pills. <strong>The</strong> thought is the ethinyl<br />
estradiol causes water retention and associated weight gain.<br />
Drospirenone, which has some antimineralocorticoid properties,<br />
also has a diuretic effect. Using drospirenone may offset<br />
water retention and weight gain. Irregular bleeding is most<br />
common in the first 3 months of treatment. Spotting is normal<br />
during the first 3 months and does not require stopping treatment<br />
or changing the pill. After the third month, it may be<br />
necessary to increase the ethinyl estradiol dose and prescribe<br />
a different pill. Irregular bleeding is one side effect that worsens<br />
with lower ethinyl estradiol doses. Most other side effects<br />
improve with lower ethinyl estradiol doses.<br />
PRESCRIBING ORAL CONTRACEPTIVES<br />
FOR ACNE<br />
Prior to prescribing oral contraceptives for acne patients,<br />
performing a pelvic exam is not necessary; however, taking a<br />
history is necessary. Much of the pertinent information already<br />
will be readily available in the patient’s chart, but it may be<br />
necessary to spend a few extra moments talking with patients<br />
about contraindications. Contraindications include pregnancy;<br />
current breast cancer; breast feeding; age over 35 and<br />
heavy smoker (more than 15 cigarettes a day); hypertension;<br />
diabetes with nephropathy, retinopathy, neuropathy, and vascular<br />
disease; deep vein thrombosis, history or current; history<br />
of heart disease; history of stroke; and migraine headaches<br />
with focal neurological symptoms at any age or without neurological<br />
symptoms in patients > 35 years of age.<br />
When prescribing oral contraceptives, give patients re a s o n-<br />
able expectations. Improvement in acne is not expected until<br />
the patient has been taking the oral contraceptive for 3 months<br />
or longer. Consider combination therapy early in the tre a t m e n t<br />
of acne. Many topical and systemic acne treatments will have<br />
a positive impact on acne as early as 4 to 8 weeks. Discuss<br />
potential side effects, namely irregular bleeding, and assure the<br />
patient that it is not a sign of anything gone wrong if she spots<br />
during the first 3 months of treatment.<br />
<strong>The</strong>re are several options for starting a birth control pill. One<br />
is the Sunday of the next menstrual period. <strong>The</strong> next is the<br />
first day of the next menstrual period. <strong>The</strong> last option is immediately<br />
upon obtaining a negative pregnancy test.<br />
Some combination therapies include antibiotics. Antibiotics<br />
and birth control pills can be used safely; however, of all the<br />
interactions that have been reported, 76% involve rifampin.<br />
Rifampin is a potent inducer of cytochrome p450, which<br />
increases metabolism of oral contraceptives and other medications.<br />
<strong>The</strong> hypothesis with antibiotic use is antibiotics<br />
decrease the gut flora that are needed to further degrade<br />
inactive metabolites of the oral contraceptives to active drug<br />
during enterohepatic recirculation. This theory has never been<br />
substantiated. Two studies in the dermatology literature look<br />
at pregnancy rate in women who are on birth control pills and<br />
antibiotics. <strong>The</strong> pregnancy rate was not statistically different<br />
between women who were on both versus women who were<br />
on a birth control pill alone (1.6% versus 0.96%).<br />
CONCLUSION<br />
Oral contraceptives prescribed eff e c t i v e l y, safely and eff i c i e n t l y<br />
will greatly impact the quality of life of women with acne. <br />
References<br />
1. Hersh EV. Adverse drug interactions in dental practice: interactions involving<br />
antibiotics: part II of a series. J Am Dental Assoc. 1999;130(2):236–251.<br />
2. London BM, Lookingbill DP. Frequency of pregnancy in acne patients taking<br />
oral antibiotics and oral contraceptives. A rch Derm a t o l.<br />
1994;130(3):392–393.<br />
1 4 • M A R C H 2 0 0 8 • S U P P L E M E N T T O S K I N & A G I N G