Download - Yemen Humanitarian Response | YEMEN
Download - Yemen Humanitarian Response | YEMEN
Download - Yemen Humanitarian Response | YEMEN

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Nutrition Cluster Coordination (NCC)<br />
Meeting Minutes<br />
10 th June, 2012 - Sanaa - WFP office<br />
Participants:<br />
Name Agency Email Address<br />
Mr.Nagib Abdulbaqi UNICEF nabdulbaqi@unicef.org<br />
Mr.Abdulkarim Al-Hubaishi WFP abdulkarim.al-hubaishi@wfp.org<br />
Ms.Latifa Beltaifa WFP latifa.beltaaiefa@wfp.org<br />
Dr. Isam –AlDeenAwad CSSW info@csswyemen.org,<br />
Dr Hisham Musleh IOM artols2002@yahoo.com<br />
halqubati2@gmail.com<br />
Dr Wafa AlSaedi MDM-F sanaa.mdm.assisstant@gmail.com<br />
Dr Wisam Al Timimi UNICEF waltimimi@unicef.org<br />
Mr.Jean Pierce ICRC jnezeyalagabo@icrc.org<br />
Mr.Mubarak Ahmad ICRC muahmad@icrc.org<br />
Ms.Lenna Abdullah MOPH eryan_7@yahoo.com<br />
Mr. Farouk Al Salihi IFAD f.al-salihi@ifad.org<br />
Ms. Marie Thomes Vision-Hope Marie.thomas@vision-hpoe.org<br />
Mr.Rene.de Vnies ECHO Rene.de-vnies@echofield.eu<br />
Mr.Beka Teshome RI bekates@yahoo.com<br />
Dr AbdulKarim Nasser YRC Nasr.196.@hotmail.com<br />
Mohammed Nayef Intersos Harad.yemen@intersos.com<br />
Dr. Agostinno Munyiri UNICEF amunyiri@unicef.org<br />
Dr. Mohammed Al-Emad WHO alemadm@yem.emro.who.int<br />
Dr. Fekri Dureab WHO fekridureab@yahoo.com<br />
Ms. Nashwa Hazaa WFP Nashwa.Hazaa@wfp.org<br />
Mr. Ahmed Al Garbani MSFE Msfe.sanaa-med@@barcelona.msf.org<br />
Michiko Kyokan MSFE Msfe.sanaa-med-dep@@barcelona.msf.org<br />
Dr Lodesani Cuodia MSFF Msff-sanaa-medco@paris.msff.org<br />
Dr. Nader Makki IMC nadermakki@yahoo.com
Purpose of the meeting: This is an extra ordinary cluster meeting to present the results of<br />
Hajjah SMART survey and discuss with partners the recommendations and the way forward:<br />
The meeting chaired by Dr. Agostino Munyiri :<br />
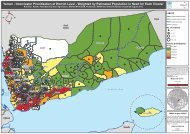
Mr Nagib Abd Al Baqi presented the finding as per the attached , it was updated that Hajja<br />
governorate nutrition surveys have been conducted through the collaboration of Nutrition<br />
Cluster, MoPH , UNICEF and local authorities across the low land, mountains areas and IDP<br />
camps of the governorate. The main purposes of the surveys are to assess the Nutrition<br />
Situation of the Low Land, Mountains areas and IDP camps of the Hajja Population and<br />
assessment of Infant and Young Child Feeding practices, Morbidity,Mortality and Water,<br />
Sanitation and Hygiene practices to make recommendations for interventions.<br />
A brief outline was presented on the methodology, geographical location where the surveys<br />
were conducted and samples size used for the survey. It was also indicated that the quality<br />
control measures were taken during the survey implementation to ensure appropriate<br />
sampling procedures, anthropometric measurements, representativeness and reliability of<br />
findings. The overall quality of each survey was presented and all the key characteristics of<br />
the WHZ curve were found within the plausible range for all surveys and were in line with<br />
the quality standards.<br />
It was noted that the Hajja governorate Nutrition Survey results revealed a critical nutrition<br />
situation in the IDP camps and in Lowland Ecological Zone, exceeding the emergency<br />
threshold of >15% GAM rate while the rate in the Mountainous zone indicate that the<br />
nutrition situation is poor. Global Acute Malnutrition rate of 15.7 % and Severe Acute<br />
Malnutrition rates of 3.0 % are recorded in the IDP camps. GAM rate of 21.6% and<br />
SAM rate of 3.7% are recorded in Lowland Ecological Zone. GAM and SAM rates in<br />
the Mountainous Ecological Zone were 9.3% and 0.9%, respectively. These results<br />
indicate a very worrying and critical situation with high risk of malnutrition related death if<br />
emergency response is not delivered or if it’s interrupted. The prevailing aggravating factors<br />
like high morbidity, inadequate sanitation conditions and poor feeding practice are just likely<br />
to depress this critical nutritional condition.<br />
Discussion around recommendations:<br />
As a result, continuation/expansion of the existing nutrition interventions including the<br />
CMAM programme and district level humanitarian needs micro planning were<br />
recommended. Improving access to safe water and sanitation, promoting key child feeding<br />
and hygiene practices and health education at the community level were also found a concern<br />
to the surveyed areas. The recommendations were provided to participants for their feedback,<br />
but later it was agreed that (Action point) :the whole survey reports to be circulated in an e-<br />
mail for participants feedback and inputs within one week , Mr Nagib will be the focal point<br />
for compilation .<br />
Next step, the chairman opened the floor for discussion and invited the participants to ask<br />
questions and provide feedbacks.<br />
MSFE reported implementing rapid nutrition assessments in their operational areas and found<br />
low prevalence of malnutrition by MUAC and it was requested for explanation why there is a<br />
difference in the prevalence of malnutrition between the MSF survey and the current SMART<br />
survey. It was pointed out that the results of the rapid assessments using MUAC screening<br />
and standard nutrition survey by SMART are not comparable because of completely different<br />
methodological approach. It was also further elaborated that SMART methodology is an<br />
international golden standard method to provide the necessary information on nutrition and
elated factors, to help inform decision makers and stakeholders of the nature and scale of the<br />
nutrition situation and for the purposes of guiding the design and implementation of an<br />
appropriate response. On its part, MSFE acknowledged that their rapid assessment results<br />
using MUAC screening and the standard nutrition assessment result using SMART<br />
methodology are not comparable and requested UNICEF to share the MUAC results in the<br />
SMART assessment. Nagib Abdulbaqi revealed that in the Hajja governorate survey, the<br />
team have also taken MUAC measurements from the study subjects and will share the finding<br />
to the interested partners.<br />
Recommendation: The head of Nutrition in the Ministry of Public Health emphasized that<br />
future nutrition assessments/Surveys should be planned in consultation with the MOPH so<br />
that the government is aware of what was going on and ensure that all assessments in the<br />
country are conducted according to agreed standard SMART methodology.<br />
Explanation why there was low death rate reported despite the prevalence of acute<br />
malnutrition is above the emergency threshold. It was explained that the relationship between<br />
mortality and acute malnutrition as measured by Weight-for-Height (W/H) is a complicated<br />
scenario and still the global debate. However, mortality is usually estimated as an average<br />
over the previous several months and GAM with W/H is a cross-sectional snapshot.<br />
Secondly, the analysis is ecological (i.e. we are not looking at the risk of death in wasted<br />
individuals but the correlation between a previous mortality rate and a current GAM<br />
prevalence in a population). Thirdly, W/H may only be weakly associated with mortality so<br />
GAM by W/H may be weakly correlated with mortality. Finally, an important thing to<br />
consider is that the relationship between malnutrition and mortality is not a fixed relationship.<br />
Most deaths among malnourished children are attributable to disease/infection rather than<br />
simply a lack of nutrients. A major factor in the association is the amount of exposure to<br />
infection the malnourished children face. Malnutrition makes people vulnerable to infection<br />
(and therefore to death), so the higher their exposure, the more likely they will be to contract<br />
some infection their bodies would have difficulty in fending off because of their poor<br />
nutritional status. The high GAM rate but low mortality in <strong>Yemen</strong> could be due to a number<br />
of factors like; a very recent, rapid rise in malnutrition; or low exposure to infection or even<br />
the timely intervention and health services to treat infections as they arise. The fact that the<br />
prevalence of oedema was ‘zero’ could also give some explanation to this complicated<br />
scenario. It’s also worth arguing that the situation of high GAM by W/H with low mortality<br />
could be as simple as "lots of death coming quite soon" if lifesaving intervention are not in<br />
place to salvage the situation.<br />
In conclusion, interpreting mortality and GAM assessed at the same time needs to be treated<br />
with caution since the mortality estimate is (usually) for the period before the GAM estimate.<br />
The SMART method cannot distinguish between rising and falling mortality and it must be<br />
noted that a typical mortality survey reports on what has happened on average in the past not<br />
what is happening now.<br />
Recommendation: A stand-alone prospective study is required to fully understand this<br />
scenario.<br />
Participants also asked about the source of mortality data as well as the recall period. It was<br />
explained that the mortality data was gathered from mother’s recall and the recall period was<br />
90 days. It was also described that in <strong>Yemen</strong>, there was poor record in birth registration as<br />
well as death certificate.<br />
MSF also raised a question why there were less deaths in the therapeutic feeding centers of<br />
their operational areas. The chairman recommended a bilateral discussion between MSF and<br />
UNICEF experts to further discussion on this topic, and get clarity on the MUAC versus
anthropometric measurements, to have only one clear message going out on the prevalence of<br />
malnutrition in the surveyed areas. See Addendum.<br />
Comparison with the previous survey in July 2011: The overall nutrition situation after the<br />
survey in July 2011 was discussed. Although the results of the July 2011 and the current<br />
survey are not directly comparable due to seasonality, it was noted that there was a decrease<br />
(not an improvement as the current magnitude also showed the level is still above WHO<br />
emergency threshold) in the prevalence of acute malnutrition .The change in the level of<br />
acute malnutrition in the IDP population over the past 10 months could be attributed to the<br />
various interventions going on. These includes expansion of the service coverage to 12 OTP<br />
as well as 6 SFP, health and hygiene promotion activities, water supply and sanitation<br />
interventions and extensive capacity building of the service providers.<br />
A comment was raised, why Hayran district was not included in the assessment? It was<br />
explained that the Hayran district was included in the sampling frame together with Khayran,<br />
Harad, Abs and Mustaba districts.<br />
A participant also asked if it’s possible to see the correlation between the feeding practice<br />
indicators and acute malnutrition. It was explained that the proportion of 6-24 months in the<br />
sample is not adequate to conduct the causal relationship analysis and separate study are<br />
required to fully understand such relationship.<br />
It was also commented why the sanitation practice among the IDP population was low while<br />
there was a hygiene promotion campaign undergoing since 2009 in the camps . It was<br />
explained that outside the camp the sanitation condition is poor as indicated by lack of latrine<br />
(as an example).<br />
It was also suggested that information sharing on the capacity building activities should be<br />
available for partners.<br />
AOB<br />
UNICEF informed partners that the Rayma survey was also completed and the results of the<br />
mentioned survey will be shared with partners during the next Cluster meeting.<br />
UNICEF also updated partners on the upcoming planned nutrition surveys that will be<br />
commenced in the various governorates in the coming weeks. As per the CFSS, it was<br />
mentioned that Lahj, Ibb, Sanna rural and Aden are the priorities in the next round of<br />
SMART surveys.<br />
Action point: (1) UNICEF bilaterally discuss with MSF after the meeting<br />
(2) NCC to circulate the Hajja SMART survey report to cluster members to<br />
submit their comments/feedback with in 1 week (late by Monday, 18 th July<br />
2012).<br />
The meeting was adjourned at 10:30 AM.
Addendum -1-<br />
Side meeting UNICEF, MSF, WHO:<br />
The bilateral discussion between UNICEF and MSF was conducted immediately after the<br />
meeting. The WHO representative was also presented during the discussion. As per MSF<br />
request, the IDP MUAC results of the Hajja governorate was shared with them. Accordingly,<br />
the MUAC results for proxy SAM was 1.4% and the proxy GAM was 7.9%. During the<br />
discussion, it was mentioned that the interpretation of the MUAC should be made with<br />
caution in the <strong>Yemen</strong>i context. As an example, the Somalia scenario was raised where the<br />
proxy SAM >1.0% is considered as a reference indicator for critical and very critical nutrition<br />
situation. During the bilateral discussion, MSF also raised a question as to why there was low<br />
death in the TFC where they are implementing the therapeutic programme. It was described<br />
that it could be due to sub-optimal progarmme coverage, where poor families in rural villages<br />
couldn’t access the TFC service (for e.g., could be because unable to afford the transport cost,<br />
or the awareness within the community regarding the programme). It was pointed out that<br />
well designed and intensive community mobilization and outreach service complimented by<br />
effective mobile team is useful to increase the service coverage. It was also described that the<br />
low death in the TFC where MSF is working cannot fully described in the meeting as there<br />
are different factors contributed to that. Finally, MSF assured not to provide press release in<br />
regards of the nutrition situation based on the MUAC findings to ensure that similar message<br />
send out among cluster partners, donors and the global community at large.